
Abstract
Background:
Informed consent is essential for the ethical conduct of clinical research and is a culturally sensitive issue. But, a measurable Chinese version of the scale to evaluate the informed consent process has not yet been explored in the existing literature.
Research objectives:
This study aimed to develop and psychometrically test the Chinese version of the Informed Consent Process Scale.
Research design:
Back-translation was conducted to develop the Chinese version of the questionnaire. A cross-sectional survey was administered, after which an exploratory factor analysis was conducted.
Participants:
We recruited a total of 375 participants who had experience in signing an informed consent form within the previous 3 years in Taiwan.
Ethical considerations:
This study was approved by two Institutional Review Boards and the autonomy of the participants was respected.
Findings:
The Chinese version of the Informed Consent Process Scale is composed of three factors with 23 items showing evidence of acceptable reliability and validity. Three major factors were extracted and labeled: Factor 1 – ‘Understanding of the research’, Factor 2 – ‘Trust and confidence’ and Factor 3 – ‘Doubt and uncertainty’. The three factors accounted for is 52.954 of the total variance with Cronbach’s α of .917.
Discussion and conclusion:
The finding corroborates previous studies showing that participants had too little understanding on the informed consent forms they signed and implied the need to clarify the critical points in clinical research. The psychometric results indicated good internal consistency and validity for this newly constructed instrument, and it was found worthy of conducting further testing and application.
Keywords
Introduction
Informed consent is essential for the ethical conduct of clinical research. An extensive search of the literature has catalogued the many known influencing factors in the consent process. The core value lies in the insistence that people who can potentially become subjects of a study should not be treated as defenceless objects. Before initiating any research, it is a necessary step for any participant to consent to be subjects of any studies. An adequate and valued informed consent form (ICF) specifies the objectives, procedures, implications and potential benefits as well as risks of the research, whereby the potential research subjects have the freedom to participate in the study or to withdraw at any point and choose other available alternatives.
The tendency in recent years has been towards human rights and autonomy; yet, more examined clinical trials have revealed that inadequate information was provided especially on certain procedures that have proved to influence patients’ decisions to participate in the study. In the informed consent process, a systematic search of PubMed (1961–2006) conducted by Falagas et al., 1 specified that only 50% of participants understood the research procedures of the ICF in their surgical and clinical trials. Tam et al. 2 further reviewed studies based on meta-analysis until 2013 and found that 75% of participants had understood the process of the ICF but were not aware of the risks of the research they participated in. On the other hand, Sanchini et al. 3 explored the comprehension of the ICF in 77 cancer patients and found that only 62% of them understood the purpose and the nature of the trial survey, but only 44% understood the study procedures indicating less than half of the patients were aware of the study procedures. Therefore, research participants’ understanding on the content of the ICF remains unclear. The study showed 4,5 that there are 44% of patients who signed the consent forms for certain surgery had no idea what purpose was in the consent forms and there are 60%–70% of patients who did not read thoroughly or did not understand the content of the consent forms. More specifically, among the participants in the clinical trials of malaria vaccines in West Africa, 90% of the respondents ‘did not understand the exit conditions’, 93% ‘did not understand the test risk’ and 74% ‘did not understand that they may not receive treatment after the trial’. Another study involving informed consent for the Brazilian tuberculosis trial found that 51% of the respondents did not remember whether the HIV test was necessary or not, and 70% did not know they can withdraw from the trial. 6 In addition, there were a total of 40 valid questionnaires in a clinical trial conducted by the National Taiwan University Hospital. Although up to 80.27% of the respondents were found to have a general understanding regarding the consent forms, there are about 47.5% and 60.0% of patients who were not very clear on the ‘compensation for injury’ and ‘processes for participants to submit concerns, complaints or requests for information’, respectively. Another study also found that one subject was completely unaware that he was participating in a clinical trial, and 17.47% of the respondents felt that the consent forms of the study were too lengthy. 7 Therefore, existing literature revealed that patients might not necessarily understand the content of consent forms completely, though they signed the consent forms.
The study
Research objectives
Our purpose was to develop and test the psychometric properties of an informed consent measure scale for the clinical participants and to understand their levels of perception and various experiences involved.
Translation process of the Chinese version of Informed Consent Process Scale
Back-translation was conducted to develop the Chinese version of the informed consent questionnaire. This was a cross-sectional survey study. Dr Bob Anderson, professor emeritus of the University of Michigan Medical School, granted permission. To convey the conceptual meaning of the target language, the original consent questionnaire was translated into Mandarin using a stringent four-step back-translation that included the following: (a) translating the questionnaire into the target language, (b) back-translation, (c) pretesting the items and (d) validating the items. 8 The questionnaire was first translated by the third author (C-C.L.), who is fluent in both English and Chinese, and then back-translated blindly by another research team member, who is also fluent in these two languages. Afterwards, the back-translated questionnaire was sent via email to a monolingual English-speaking team member to check whether the first translation accurately contained the original meaning of each item. The background of the research members involved in the translation process is in nursing field. In order to resolve problems that arose from the first translation or the back-translation, inaccurate expression or unclear English terms or verb tenses were discussed via email. Some modifications were made based on the attempt to improve the expression of the questionnaire and to adapt some of the items for contextual differences in Taiwan and Hong Kong. Any change made for the English content then went through the full first- and back-translation process until consensus on the concept and wording was reached, and the versions of both languages were confirmed. Back-translation was conducted to develop 23 items from the Mandarin version of the questionnaire.
Research design
The cross-sectional survey was administered to the participants, and exploratory factor analysis (EFA) was conducted. More specifically, in the medical field, white lab coat represents the professional image of health providers. In Chinese culture, the majority of doctors are males and the majority of nurses are females. We would like to see whether there is any potential influence of gender and attire representing professional images on how participants respond to the ICFs. Although the existing literature showed that there is no gender preference for the more ‘instrumental’ health professions (e.g. surgeons, anaesthetists), gender preferences are more related to the health professions who engage in intimate and psychosocial health problems (e.g. gynaecologists and general practitioners (GPs)). 9 Since our intervention is related to psychometric evaluation, the participants may also have their gender preference while giving the responses on the consent forms depending on which gender of the researcher (health professions) they were with. How health professions’ gender influences patients’ responses on consent forms seems to be scant in the literature; hence, it is worth exploring on the perspective of gender influence in this study.
In addition, the attire of doctors and nurses may influence how participants respond to their consent forms. According to previous study conducted by Caldow et al.,10 patients mainly perceived differences between doctors and nurses based on academic ability and qualifications. Most respondents thought nurses could deal with relatively minor problems compared with doctors who are mainly in charge of diagnosis and treatment. As the attire represents different professional images and authority, participants may differ in their responses while interacting with these two different health providers.
Participants
The criteria included in the study were the following: (a) the participants had experience of having signed a research ICF within the previous 3 years, (b) their age was over 20 years and (c) they were able to communicate in Chinese. Exclusion criteria were as follows: (a) inability to independently consent and (b) inability to read or sign the study’s ICF. In order to keep the heterogeneity high, we tried to reach institutions in three different regions (north, middle and south) of Taiwan. Finally, we recruited 375 participants who had previous experience of signing an ICF within the past 3 years. While filling in the questionnaires of informed consent, the participants were free to ask the researchers if they had any inquiry regarding the study.
Data collection and ethical considerations
The institutional review boards of two selected hospitals approved this research (KMUHIRB-E-20150016; CCHIRB:150416) and the autonomy of the participants was respected as they voluntarily agreed to fill in the questionnaire anonymously. The process of data collection was first through communicating with principal investigator, co-investigators and research staffs who had conducted clinical trials within the previous 3 years and seeking the potential participants from their studies. After their verbal explanation to the potential participants, some agreed to participate in and were referred to the researchers of this study for further explanation. After receiving the explanation of the study, these participants completed the informed consent questionnaires. If the participants were not able to complete the questionnaires themselves, the researchers would assist them in interviewing them in order to collect the data. The interview took about 10 min at a quiet area such as a meeting room. The participants would be reimbursed with a gift worth of US$3 approximately.
The researcher kept personal privacy information as confidential and replaced an individual information with a code and the above data would not be available to other researchers. The completed questionnaires would be locked and kept cautiously. The contents of the questionnaires were only for academic research purposes. In addition to the relevant agencies to investigate according to law, the research team would carefully keep the confidentiality and privacy of the respondents.
Findings
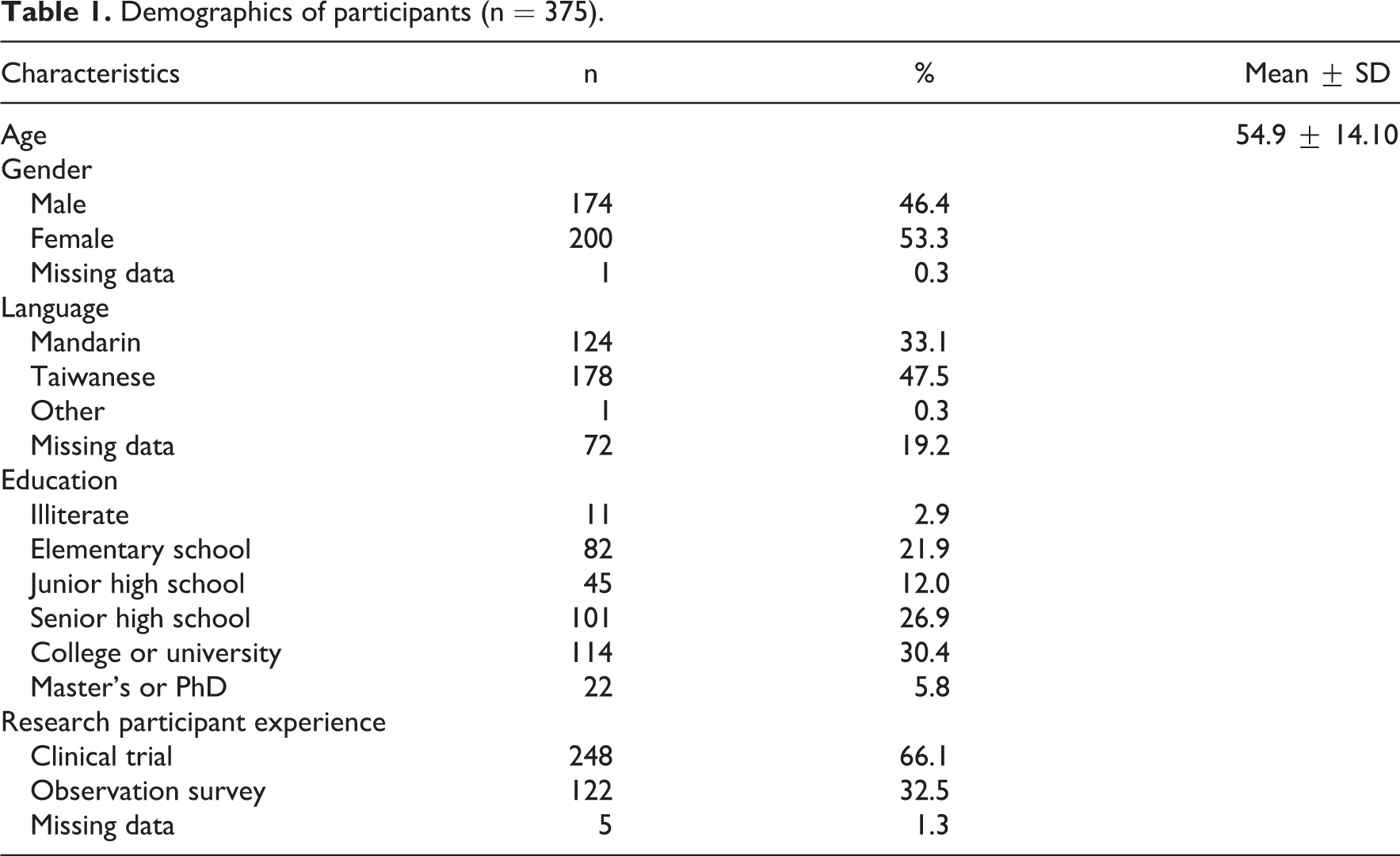
Data were analysed using SPSS 14.0. Descriptive statistics were generated for demographic variables and individual item scores. A total of 375 participants participated in the study. Their mean age was 54. 9 (standard deviation (SD) = 14. 10 ) years. More than half of the participants were female (53.3%) and married (77.9%), of which 66.1% had previously enrolled in a clinical trial involving informed consent and 32.5% had enrolled in an observation survey. Most of the participants had senior high school (26.9%) or elementary school education (21.9%), a few were self-directed learners without formal education background yet were able to read the questionnaires (2.9%) and 5.8% held a master’s degree or higher. Most were Taiwanese (87.2%), and their language was Taiwanese (47.5%). The total family income of the majority was NTD 40,000 to 59,999 (23.2%) and 60,000 to 99,999 (23.5%) (see Table 1).
Demographics of participants (n = 375).
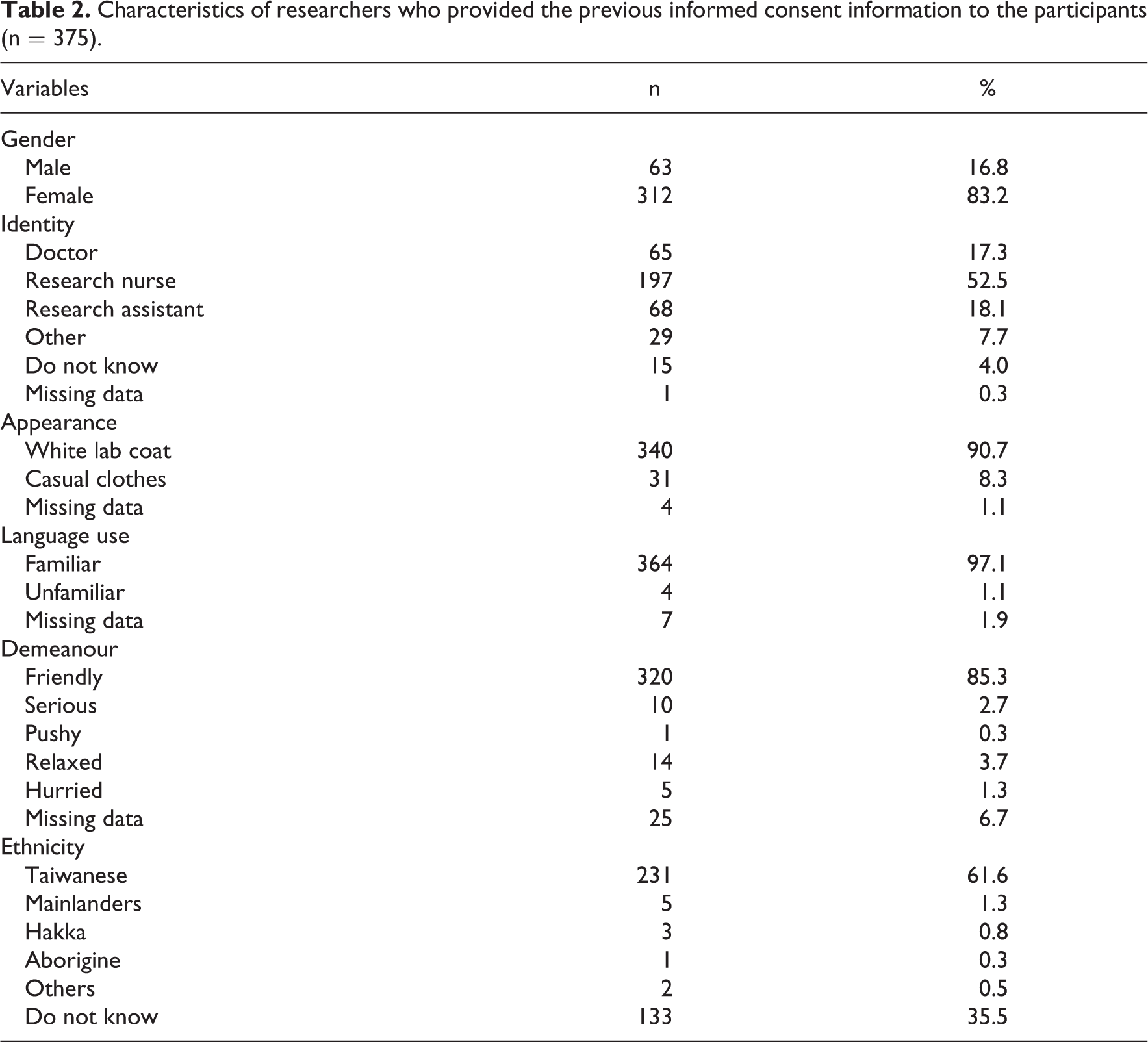
In this study, 83.2% (n = 312) of the participants reported that they had received most informed consent explanations, that 90.7% (n = 340) of the information providers who gave explanations wore a white lab coat, 85.3% were friendly (n = 320) and 97.1% (n = 364) explained information with familiar language. Information from a doctor was received by 17.3% (n = 65) of the participants, while 70.7% (n = 265) received information from a research nurse or research assistant (see Table 2).
Characteristics of researchers who provided the previous informed consent information to the participants (n = 375).
Item analyses were used to decide which items on the instrument should be eliminated and which ones should be kept. 11 EFA using principal component analysis was used to assess the factor structure. The factor structure of the 23-item scale was analysed with a sample of 375 adults using principal components to extract factors. The Kaiser–Meyer–Olkin (KMO) test of sampling adequacy and Bartlett’s test of sphericity were performed. The number of factors to be retained was determined by a convergence of criteria including eigenvalues >1, the scree plot and theoretical interpretability of the resulting factor structure. The number of factors to be retained was determined by parallel analysis, one of the most accurate methods of deciding the appropriate number of factors to retain. 12 Items were selected according to the following criteria: (a) factor loading above 0.5 and (b) minimum factor membership of three items.
The distributions of each item and subscale were generally symmetrical. Based on the criteria for dropping items and using upper and lower groups’ analysis, all items were kept after the item analysis. The item-total correlation test was checked if any item in the set of tests was inconsistent with the averaged behaviour of the others. Items that met any of the following criteria were eliminated: (a) the means of the items were extreme or the variances were zero, (b) items with skewness >3 or kurtosis >10, (c) the corrected item-total correlation was <.3 and (d) the critical ratio value of an item was found to be insignificant (see Table 3).
Results of item analysis (n = 375).
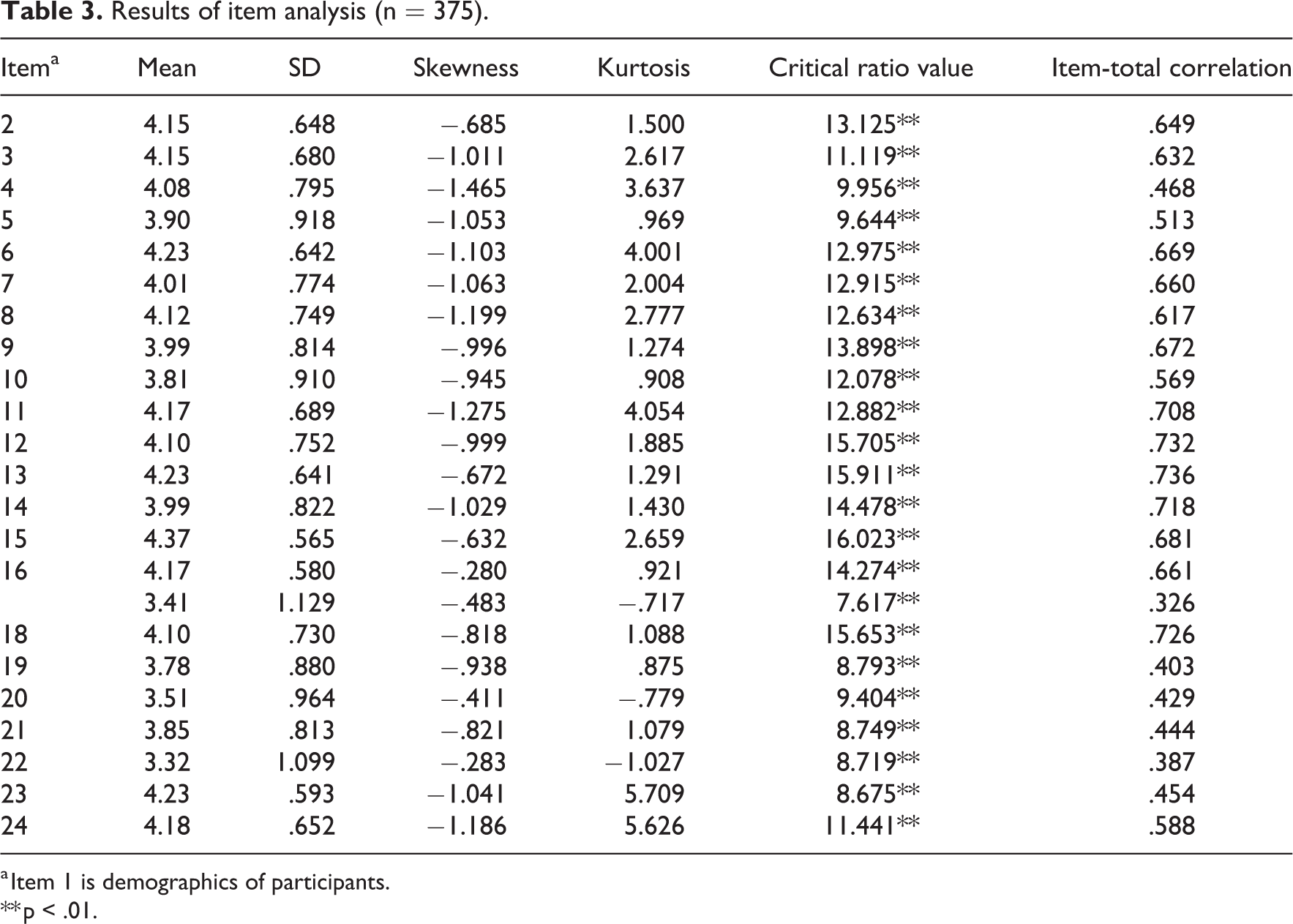
a Item 1 is demographics of participants.
** p < .01.
According to the item analysis results, no items were eliminated from the original scale. The KMO value was .937, indicating excellent sampling adequacy and relatively compact patterns of correlation; such factor analysis should produce distinct and reliable factors. 13 Bartlett’s test of sphericity was significant (χ2 = 4185.925, df = 190, p < .0001), indicating that some relationships existed between the variables. 8 Orthogonal rotation procedures were used to rotate the factors.
After examining the various factor solutions, the investigators found that a three-factor solution provided the most meaningful factor pattern. Factor 1 is ‘Understanding of the research’, with factor loading from .581 to .759, variance 26.763%, Cronbach’s α of .925. Factor 2 is ‘Trust and confidence’, with factor loading from .538 to .658, variance 16.817%, Cronbach’s α of .865. Factor 3 is ‘Doubt and uncertainty’, with factor loading from .531 to .707, variance 9.74%, Cronbach’s α of .713. The total variance is 52.954 and Cronbach’s α is .917 (see Table 4).
Factors and item loadings in ICPS-CV (n = 375).

ICPS-CV: Chinese version of the Informed Consent Process Scale.
a Items 25–28 were different question types, not included in the factor analysis.
Discussion
Chinese version instrument
The informed consent process is culturally different and culturally sensitive. 14 In the previous literature, there is no published Chinese version. The main goal of the study, after creating a Chinese version of the scale, was to evaluate the psychometrics of the Chinese version of Informed Consent Process Scale (ICPS-CV) in an effort to help managers address the informed consent process in clinical research and properly apply interventions to facilitate the process. We included participants who had the experience in signing a research ICF within the previous 3 years, were 20–80 years old and could communicate with Chinese. To help broaden the future application of the scale, we tried to keep the heterogeneity high with regard to sample size, age, gender, total family monthly income, language, education and research participant experience. The psychometric evaluation evidence had acceptable results, with an adequate factorial analysis, a high internal consistency. The ICPS-CV is composed of three factors and 23 items in total. This includes Factor 1 – ‘Understanding of the research’, Factor 2 – ‘Trust and confidence’ and Factor 3 – ‘Doubt and uncertainty’. The specific 23 items are shown in Tables 3 and 4.
Understanding of the research
According to previous studies, patients’ understanding of clinical informed consent seemed to be an important factor that might affect their decision-making while signing an ICF. Schenker et al. 15 indicated that patient understanding in clinical informed consent is often poor. Sanchini et al.3 found that only 62% of patients understood the purpose and the nature of their trial survey and only 44% understood the study procedures. Wade et al. 16 indicated that evaluation of recruiter–patient interaction should focus on evidence of (a) patient views of the trial, randomisation and treatments; (b) improved patient understanding; and (c) patients’ understanding of clinical equipoise. Farrell et al. 17 noted in 2014 that for patients, poor information delivery can impair their understanding of recommended treatment, reduce their satisfaction with care delivery and have a detrimental impact on their treatment adherence. Our results also showed that only 47.2% of the participants completely understood the research study when they joined it. But ‘Understanding of the research’ is not the only factor; ‘Trust and confidence’ and ‘Doubt and uncertainty’ are also factors that affect their decision. Among 375 respondents in this study, majority of the respondents had ‘the ability to understand the content of the consent form of the subject’, but had scant responses in ‘I have enough time to read the subject’s consent’, the ‘risk of research’ and the ‘benefit of research’. This corresponds to the research on the West African malaria vaccine trial, of which 93% ‘did not understand the test risk’. 18 In addition, a systematic review conducted by Tam et al.2 found that only 74.0% did not understand potential benefits, and 67.0% did not understand potential risks and side effects. Therefore, the above two results correspond to each other. It is clear that the risks and benefits of research should be the focus while interpreting the research process and it is necessary to give the participants sufficient time to read the consent forms for their readiness to participate in the study.
Trust and confidence
Our results also showed that 40.8% of the participants when making decisions regarding their medical care would prefer to make those decisions equally with the doctor, and 20.8% of the participants would let the doctor make most of the decisions. In the previous research, culture has been addressed in varied issues related to healthcare ad hoc the communication or educational intervention between patients and health providers. Informed consent is different by culture. Beach et al. 19 addressed the importance of cultural competency as it could be considered a strategy for improving the knowledge, attitudes and skills of health professionals. Maybe, in the Taiwanese culture, our participants hesitate to express their doubts and discuss their uncertainties. However, evidence on this perspective on health outcomes is still lacking in the existing literature. Thus, future research should focus on cultural significance and, more specifically, investigate on the cultural differences among different regions with the same informed consent tool. As Somnath 20 suggested that culture is considered multifaceted and dynamic. Individuals are more likely employ different perspectives for different issues or even for the same issue at different points in time. Cultural contexts are essential in the field of healthcare as certain cultural competence creates trust between the health professions and patients. 21
In our Taiwanese culture, the doctor–patient relationship and trust can affect the participant’s decision, and the review of Halkoaho et al. 14 noted that taking cultural aspects into account during the whole research process improves the quality of the research. But, in our study, 52.5% of those who provided the information to the participants were research nurses (Table 2) and, similar to the two studies of Susilo and colleagues, 22,23 inter-professional education is needed to promote inter-professional collaboration, and informed consent practice should be tailored and improved. 23
Doubt and uncertainty
In the 2014 study of Sherlock and Brownie, 24 patients’ recollection and understanding of the medical procedure, its risks and complications, was often low, particularly among older individuals. For discretionary tests and procedures, complete information about expected benefits and risks may lead many individuals to choose alternative strategies or to be more confident in the recommended choice. 25
Limitations
The main goal of our study was to conduct an EFA, not to verify correlations. And our results may be specific to the Taiwanese population; further testing may be needed in other areas where people speak the same language, although their cultures are different. The study also did not discuss how the role of participants’ memory was over the 3 years and how many might not have remembered certain specific information on the ICFs they signed. The above points could be considered the limitations of the study.
Conclusion
The purpose of this study was to develop a Chinese version of the Informed Consent Process Scale (ICPS-CV) and to then evaluate its psychometrics. The 23-item ICPS-CV, with its three factors labeled ‘Understanding of the research’, ‘Trust and confidence’ and ‘Doubt and uncertainty’, with Cronbach’s α of .917, shows evidence of sound reliability and validity. The study indicated good internal consistency for this new instrument, finding it worthy of further testing and application.
Footnotes
Authors’ note
Shu Yu Chen and Shu-Chen Susan Chang have contributed equally to this article.
Acknowledgements
The authors thank all participants for their support and involvement in the study.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.