
Abstract
Background:
Ethics education is essential to the education of all healthcare professionals. The purpose of this study was to evaluate an interprofessional approach to ethics education to all students across an academic health science center.
Research objectives:
The objectives were to (1) compare student perception of ethics education before and after the implementation of the campus-wide ethics program and (2) determine changes in student ethical decision-making skills following implementation of a campus-wide ethics program.
Research design:
This study was a quasi-experimental design with seniors graduating prior to the intervention serving as the control group.
Participants and research context:
The setting was a comprehensive health science center in the southwestern United States. All students enrolled in the university participated in the intervention; however, 976 graduating students were used for evaluation of the intervention.
Ethical considerations:
Study materials for each survey were submitted to the university’s IRB, and the project was approved as exempt by the Committee for the Protection of Human Subjects. Student participation in the surveys was voluntary. No names or other identifying information were collected, and responses to the survey questions were kept confidential.
Findings:
Students’ perception of the adequacy of time spent on the ethics content in course instruction and practical training decreased from the baseline to the fifth-year survey. Students’ overall comfort level with their abilities to deal with ethical issues increased from the baseline to the fifth year. Student ethical decision-making skills were higher at the third-year evaluation for all indicators. For the fifth-year survey, responses were also higher scoring on all four indicators.
Discussion:
After participation in an interprofessional campus-wide effort on health professions ethics, students demonstrated higher ethical decision-making scores according to the Health Professional Ethics Rubric. However, their scores still did not reach the proficiency level identified in the rubric.
Conclusion:
Examination of the effectiveness of each part of the intervention is needed.
Keywords
Introduction
Ethics education is essential to the education of all healthcare professionals. 1 Improvements in technology have led to new issues and dilemmas that previously existed only in science fiction films. Nurses are daily facing issues regarding conflict over end-of-life care, allocation of scarce resources, patient privacy versus the benefits to another, and the use of genetics in prevention and treatment of diseases. While healthcare educators have instructed students in their profession about ethics and ethical decision-making, few institutions have attempted an interprofessional approach to teaching ethics across the campus. The majority of those who have done so have only evaluated knowledge gains instead of the application of ethical decision-making skills. 1 –6 The purpose of this study was to evaluate an interprofessional approach to ethics education to all students across an academic health science center, which includes six health professional schools in bioinformatics, biomedical sciences, dentistry, medicine, nursing, and public health. The specific aims were to (1) compare student perception of ethics education before and after the implementation of the campus-wide ethics program and (2) determine changes in student ethical decision-making skills following implementation of the campus-wide ethics program.
Literature review
Today there is a general consensus that instruction in ethics and professionalism is essential in the education of all healthcare professionals. 1 However, this consensus was not always the case. Certain scandals, perhaps most notably the Tuskegee Syphilis Study, 7 indicated a need for greater oversight and more systematic thinking with regard to the ethics of research and clinical practice. During the 1960s and 1970s theologians, philosophers, lawyers, and others, who have been called “strangers at the bedside” of patients, 8 helped to create, along with physicians such as Edmund Pellegrino, a field that became known as bioethics.
A core text was written—Principles of Biomedical Ethics 9 —that offered a method of inquiry in bioethics and, in time, various subfields of ethics emerged within medicine, such as psychiatric ethics. 10 Other health professions also developed their own ethics, such as dental ethics, 11 nursing ethics, 12 and public health ethics. 13 Often, but not always, these texts followed in the footsteps of Principles of Biomedical Ethics.
But the basis of bioethics was not grounded only in scandal. Confusion played a part as well. As has been documented in various histories of bioethics, 14 improvements in biotechnology created new dilemmas. Some of these dilemmas have been around for decades now: If someone is put on a ventilator, when is it acceptable to turn off such life support? If access to medical procedures—such as dialysis—is limited, who should receive it? Is it ethical to do research on embryos? Recent advances and potential breakthroughs push these dilemmas even further: How long should human beings live? Should the cloning of human beings be pursued? Is gene editing ethical? These issues make for good academic debates in college classrooms and in editorials.
In terms of the education of clinicians, ethics instruction is usually more concrete and less grand than these issues because decisions really do need to be made, often in real time. That is, the core questions of clinical ethics in various professions and specialties are not merely intellectual or academic—action must be taken. As noted, nurses face conflicts over end-of-life care, allocation of scarce resources, and patient privacy every day. For example, in hospice care, patients may receive inadequate pain medication because there is a disagreement between a physician and a nurse regarding proper dosage to manage pain. Such disagreements become harder to manage if clear data do not exist. Allocating scarce resources could refer to something as mundane as a nurse’s time, for if a clinic is being run with too few nurses (so as to maximize profits) patients may suffer as a result. Finally, regarding patient privacy, where one stores one’s laptop as well as what one posts on social media are moral matters. While such issues may not be as “sexy” as the grand debates of bioethics (e.g. When does life begin? How is death defined and determined?), they are nevertheless a part of everyday nursing. It is likely that there is a moral dimension to every aspect of clinical care.
Like ethics education for health professions students, the importance of interprofessional education in the health professions has also become increasingly recognized over the past few decades. 15 Caring for patients has become increasingly complex, with various team members caring for individual patients. It has become obvious that more coordinated efforts are needed. Sometimes, for example, patients receive bad news in haphazard ways because different teams think that the other team has already broken the bad news, as when the internal medicine team thinks that oncology team broke the news about a patient’s cancer diagnosis (because they are the specialists), but the oncology team thinks that internal medicine team did so (because they are supposedly overseeing all aspects of the patient’s care). Learning how to communicate effectively with all team members is an important aspect of interprofessional education in today’s healthcare environment.
The teaching of nursing ethics in nursing schools has been discussed for decades. 16 –18 While some uncertainty remains regarding the degree to which this teaching is effective, and which methods are best, 19,20 empirical studies in the scholarship of teaching and learning regarding nursing ethics in nursing schools show that nursing students and practitioners tend to feel more confident regarding their moral judgments if they have had some formal ethics education. 21,22 Traditional models of nursing ethics education involve the use of cases 13 as well as codes. 23 Recent trends in nursing ethics education have involved interprofessional education 24 as well as problem-based learning. 25
Our approach to interprofessional ethics education
Even though interprofessional education has gained ground in principle, common barriers nevertheless remain at many institutions, often involving logistics relating to time and space. 26,27 How to grant credit is also sometimes an issue that needs to be worked out. One solution has been to offer classes and activities over the lunch hour, in the evenings, on the weekends, and online. Such strategies work in the short term, with modest success. A truly interprofessional approach would rethink and rebuild various curricula at the same time with concrete goals in mind.
As a part of our Quality Enhancement Plan (QEP) for the Southern Association of Colleges and Schools Commission on Colleges (SACSCOC), our institution developed a plan for the teaching of interprofessional ethics. An interprofessional team from all six schools in the university led the development of core materials and evaluated activities that were based in each school. A key part of this plan included developing core materials to be used across our campus in all of our schools—most notably, we wrote The Brewsters, 28 a choose-your-own-adventure novel with didactic materials that introduces a common vocabulary and key concepts for the teaching of ethics and professionalism in an academic health science center. Assessment findings have indicated that The Brewsters has been effective with regard to knowledge gain. 29 The implementation of our QEP also led to school-specific activities, assessments, and publications. 30,31 Table 1 includes major activities and the number of student participants. The programs and activities were implemented in a variety of settings. While the majority of activities were in classrooms, such as ethics courses and interprofessional electives or seminars, another five activities were clinically based (e.g. Adopt-a-Resident Program, Palliative Care Rotation). The remaining programs involved both classroom and clinical components, including Clinical Applications and the Postdoctoral Fellowship Program.
Major activities and participation by school.
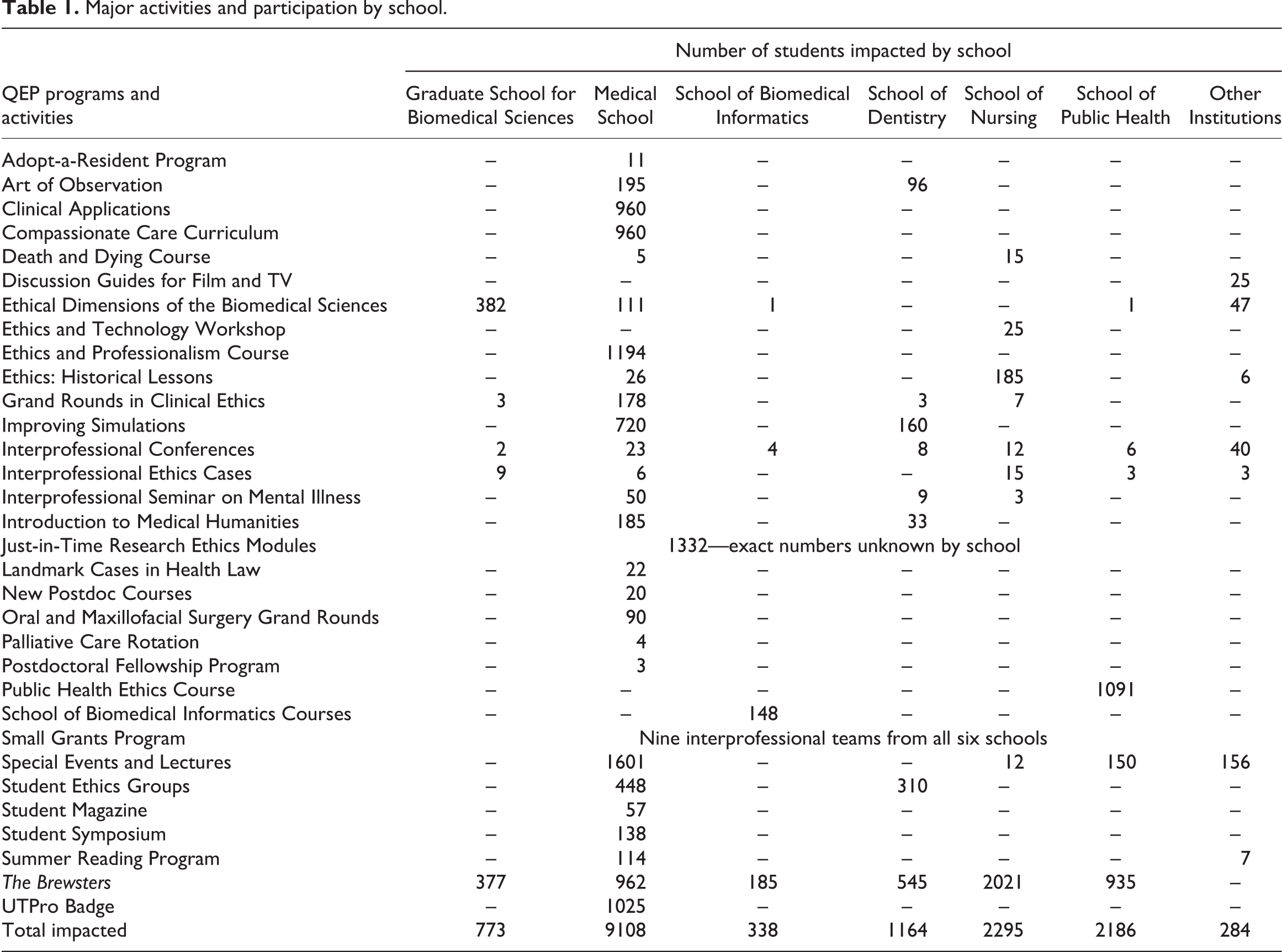
While educators in the health professions have attempted to teach students about their profession regarding ethics and ethical decision-making, few institutions have attempted an interprofessional approach to teaching ethics across the campus. The majority of those who have done so only evaluated knowledge gains instead of skills assessment in ethics education. 1–6 We have also evaluated knowledge gains, but we have gone beyond the assessment of knowledge gains to analyzing ethical decision-making skills. A key part of our initiative in this regard included developing a rubric for practical assessment of ethical decision-making skills in health professional schools, 32 which we used for a baseline assessment as well as for this current study. 29
Activities in the School of Nursing included requiring all entering nursing students to read The Brewsters, including taking a pretest and posttest. At the orientation for each degree program in the nursing school, a bioethicist introduced The Brewsters and a nursing faculty member of the core university interprofessional team led a discussion on ethics and professionalism in nursing. Ethics content was integrated throughout the nursing program in the clinical and research courses. Some graduate programs had core courses with a major emphasis on ethics. The integrated content throughout the curricula of the nursing degree programs was not new. The final new activity included an elective interprofessional ethics course developed by a School of Nursing faculty member. This course discussed ethics in the context of historical case studies, such as the Holocaust, the Tuskegee Syphilis Study, the Vipeholm Study, Hansen’s disease in the United States, Hurricane Katrina, and the emergence of HIV/AIDS. This course was taught in both a face-to-face format and in an online format. Course lecturers presented the case studies and students watched related movies after each case study. Medical, dental, and nursing (BSN, MSN, DNP, and PhD) students took the course and lectures were done by an interprofessional team including a bioethicist, a medical social worker, nurses, a physician, a dentist, and a theologian.
Methods
The study was conducted at a health science center located in a large urban medical center in the southwestern United States. The institution has a population of more than 5000 students across six health professional schools for bioinformatics, biomedical sciences, dentistry, medicine, nursing, and public health. Using a nonequivalent control group quasi-experimental approach, graduating students who did not receive the intervention served as the control group and the intervention group comprised students enrolled for the next 5 years. Graduating student participants responded to evaluation surveys before the interventions were implemented and again at the third- and fifth-year intervals. The university’s Committee for the Protection of Human Subjects granted exemption for the study.
Participants
Over 5 years, all university students participated in the intervention, amounting to nearly 18,000 students. A total of 976 students from the six health professional schools participated in the evaluation. Of these students, 437 were in the control group. From the intervention group, 288 students participated in the third year and 251 students participated in the fifth year evaluations. During each evaluation phase of the study, participants were graduating seniors.
Instrument
The evaluation survey was composed of two sections. The first portion asked students to self-assess the amount of time spent on ethics and professionalism content in university courses and practical training. They were also asked to self-assess their level of comfort in dealing with ethical issues. The first two questions regarding the amount of time spent on ethics education used a four-point Likert-type scale of “no time,” “too little time,” “the right amount of time,” and “too much time.” A four-point Likert-type scale was also used for responding to the question of comfort, which ranged from “very uncomfortable” to “very comfortable.” Several other questions in the first section included asking students demographic questions and to offer an opinion as to whether they believe ethics teaching is needed at the university.
The second section of the survey included four open-ended questions asking students about an ethical dilemma they have faced while at the university. Students identified an ethical dilemma, outlined options for addressing the situation, presented their personal action taken to resolve the issue, and offered professional codes or values relevant to the situation. Participants’ responses were evaluated by raters using the Health Professional Ethics Rubric, 32 which provides guidelines for scoring the four outcomes using a three-point scale of “insufficient” (1), “acceptable” (2), and “proficient” (3). To ensure consistency among the scores, inter-rater reliability was computed for each survey; all three scorings were above .90.
Procedures
Students in the control group completed primarily paper surveys, which were distributed during classes at five of the six schools. Courses at the end of each academic program were identified to recruit survey participants. At least one class per the five schools received paper surveys. A member of the interprofessional team introduced the survey, which was distributed during the classes. Students who chose to participate turned in the surveys at the end of class. The exception was the School of Public Health, at which a web survey was conducted using Zoomerang. Graduating students of public health received an email containing the survey invitation and link from the school’s academic affairs office. The web survey mode was used for public health because many of the students attend remotely. Data from the paper surveys were entered into SPSS and combined with web survey data.
Data collection later shifted online for subsequent surveys using Qualtrics to host the survey. The survey link was distributed to graduating students of each school by their school’s respective academic affairs offices. Students received reminder emails to complete the survey about 2 weeks after receiving the initial survey invitation. All participation was voluntary across the two survey modes for all three surveys. Participants did not receive incentives for opting to participate. Despite conducting the paper surveys in classroom settings, neither extra credit nor grades were given to students who participated.
Response rates varied among the control group and subsequent surveys. Table 2 demonstrates the return rate for the surveys. Of note, response rates in the control group for participants who completed paper surveys (84.7%) were higher than those participants who completed web surveys (19.9%). The response rate for web surveys in the control group was lower, but similar to response rates for web surveys conducted in years three and five. Despite declining response among the surveys, rates remained consistent with expected ranges of 20%–30% in university-based surveys with students. 33
Response rates by survey.

Data analysis
Survey data were analyzed using descriptive statistics. Analysis of variance was selected to compare the control and interventional groups. Testing for the assumptions indicated homogeneity of variances was violated, thus Welch’s ANOVA with Games–Howell post hoc testing was used. Differences were considered statistically significant if p < .05. Effect sizes were determined using adjusted omega squared.
Ethical considerations
Study materials for each survey were submitted to the university’s IRB, and we were granted exemption by the Committee for the Protection of Human Subjects. Student participation in the surveys was voluntary. For all three surveys, students invited to participate in the paper or web surveys received informed consent and were notified they could choose to participate, opt out of participating, or stop participating at any time. Students were also informed of our efforts to maintain their anonymity and confidentiality. Participants were anonymous as no names or other identifying information were collected. For the two online surveys, we also disabled any tracking features in Qualtrics. Students’ responses to the survey questions were kept confidential. Only the scorers of the four open-ended questions, which included the authors, saw the responses. Further, survey findings were previously reported internally only in aggregate.
Findings
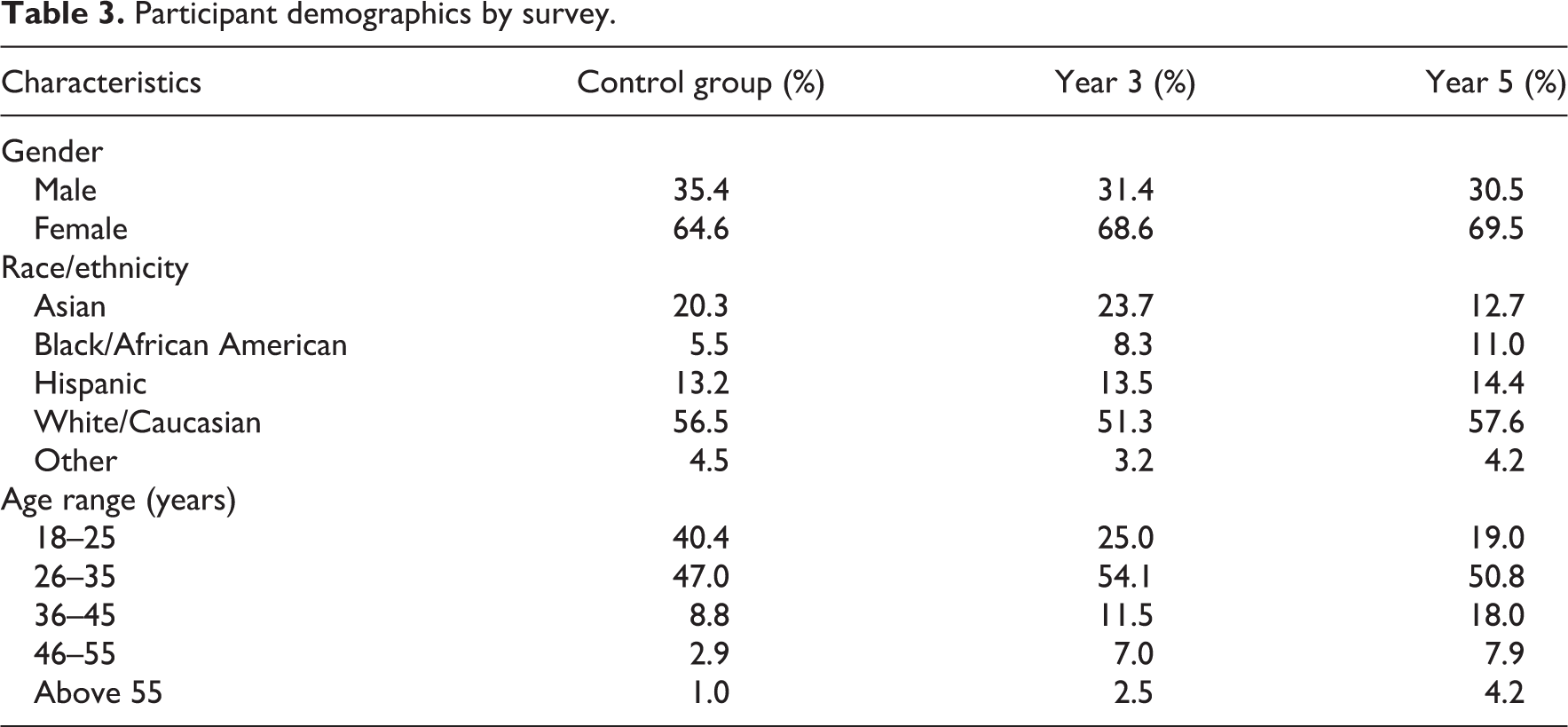
Of the 976 students who completed the survey, 42 were bioinformatics students, 96 were biomedical sciences students, 139 were students of dentistry, 148 were medical students, 175 were nursing students, and 278 were students of public health. An additional 98 students did not identify their school. Demographics of the student participants in the survey are in Table 3.
Participant demographics by survey.
Perception of ethics education
Students in the control group reported that ethics content was addressed in coursework between too little and the right amount of time (M = 2.70, SD = .49) as well as in practical training (M = 2.64, SD = .52). The students rated themselves as comfortable in dealing with ethical and professional issues (M = 2.97, SD = .53). Medical students reported the greatest amount of time spent on ethics content in coursework (M = 2.95, SD = .43), while bioinformatics students reported the least time (M = 2.17, SD = .64). In practical training, dentistry students (M = 2.74, SD = .44) reported the most time and bioinformatics students (M = 2.31, SD = .89) again reported the least time spent on ethics content. With regard to students’ comfort in dealing with ethical issues, biomedical sciences students reported they were most comfortable (M = 3.18, SD = .32), while public health students felt least comfortable (M = 2.76, SD = .60).
Students who participated in the third-year evaluation of the intervention reported the time spent on ethics coursework was, on average, between “too little time” and “the right amount of time” (M = 2.66, SD = .55). Similarly, students reported that ethics content in practical training was between too little and the right amount of time (M = 2.56, SD = .63). They also reported feeling comfortable (M = 2.94, SD = .67) dealing with ethical and professional issues. Students’ ratings of the questions varied by their particular schools. Bioinformatics students reported spending the least amount of time on ethics content in both coursework (M = 2.36, SD = .69) and practical training (M = 2.23, SD = .85). Conversely, medical students reported the most time spent on ethics content in coursework (M = 2.92, SD = .38) and students of dentistry reported the most time spent on ethics content in practical training (M = 2.82, SD = .33). Public health students assessed themselves with the lowest level of comfort (M = 2.83, SD = .73), while dentistry students self-assessed as having the highest level of comfort (M = 3.30, SD = .47) dealing with ethical and professional issues.
At the fifth-year evaluation of the intervention, students reported similar ratings. They reported the time spent on ethics content was between too little and the right amount of time in coursework (M = 2.57, SD = .54) and in practical training (M = 2.48, SD = .60). Their level of comfort was rated as “comfortable” (M = 3.09, SD = .55). By school, the ratings varied somewhat from the overall averages. For instance, biomedical sciences students reported that greater amounts of time were spent on ethics and professionalism content in courses (M = 2.81, SD = .40) and practical training (M = 2.67, SD = .72), while public health students reported, on average, the least amount of time spent on this content in both courses (M = 2.40, SD = .55) and practical training (M = 2.29, SD = .61). Regarding their comfort level in dealing with ethical issues, biomedical sciences students assessed their level of comfort as highest (M = 3.31, SD = .61), while dentistry students reported feeling the least comfortable (M = 2.92, SD = .44).
All three items—estimation of time spent on ethics content in coursework (Welch’s F(2, 545.23) = 4.83, p = .008, estimated ω2 = .008) and in practical training (Welch’s F(2, 452.27) = 5.54, p = .004, estimated ω2 = .013), and students’ comfort level dealing with ethical issues (Welch’s F(2, 491.24) = 4.30, p = .012, estimated ω2 = .009)—were statistically significantly different between the three groups. Post hoc testing indicated that students’ estimation of time spent on ethics content in coursework (p = .006) and practical training (p = .003) was significantly lower between the control group and the fifth year of the intervention. Despite this reported decrease in students’ perceptions of time spent on ethics education, their comfort level significantly increased (p = .035) from the pre-intervention to the fifth-year evaluation of the intervention. Students also reported significantly higher levels of comfort in the fifth year compared to the third year (p = .026). Effect sizes of the statistically significant differences, however, were small for all three areas.
Ethical decision-making skills
To evaluate students’ skills in making ethical decisions, students were asked four questions relative to the ethical decision-making process. The qualitative responses were scored by raters using a three-point rubric. The first question required students to provide an example of an ethical or professional dilemma they have encountered while a student of the university. Students were asked to outline possible options for addressing the situation in the second question and to share what option they chose in the third question. The final question requested the student to list any professional codes or values they used to inform their decision.
Survey participants prior to the intervention earned mean scores on each of the four outcomes ranging from “insufficient” (1) to “acceptable” (2): identification of the ethical issue (M = 1.38, SD = .61), outlining possible options (M = 1.39, SD = .64), personal action (M = 1.27, SD = .58), and identification of professional codes or values (M = 1.13, SD = .43). At both the third- and fifth-year evaluations, students of all six schools earned higher scores on the four outcomes (see Table 4).
Mean scores by evaluation year.

Within the control group, medical students earned higher mean scores overall for the four outcomes of ethical decision-making (M = 1.52, SD = .53), while bioinformatics students scored lowest (M = 1.10, SD = .13). In the third year of the intervention, nursing students scored highest (M = 1.85, SD = .60) and biomedical sciences students scored lowest (M = 1.32, SD = .38). In the fifth year of the intervention, biomedical sciences students scored highest (M = 2.60, SD = .34) and bioinformatics students scored lowest (M = 1.50, SD = .54).
Welch’s ANOVA indicated that students’ mean scores on the four outcomes were statistically significantly different between the evaluation groups: identification of the ethical issue (Welch’s F(2, 193.74) = 31.16, p < .001, estimated ω2 = .099), outlining possible options (Welch’s F(2, 196.94) = 13.12, p < .001, estimated ω2 = .042), personal action (Welch’s F(2, 191.89) = 21.39, p < .001, estimated ω2 = .069), and identification of professional codes or values (Welch’s F(2, 198.80) = 3.38, p = .036, estimated ω2 = .009). The effect sizes of these differences were small for two outcomes–outlining options and identifying codes or values–and medium for identifying the ethical issue and personal action. Post hoc testing identified the specific outcomes and intervention years between which the statistically significant differences occurred.
At the third-year evaluation, participants’ scores statistically significantly improved on two outcomes compared to the control group: identification of the ethical issue (p < .001) and personal action (p = .009). At the fifth-year evaluation, students scored statistically significantly higher on all four outcomes when compared to the pre-intervention: identification of the ethical issue (p < .001), outlining possible options (p < .001), personal action (p < .001), and identification of professional codes or values (p = .030). This finding was similar when comparing the third-year evaluation to the fifth-year evaluation: identification of the ethical issue (p = .020), outlining possible options (p = .003), personal action (p = .001), and identification of professional codes or values (p = .047).
Discussion
Students who participated in the intervention, which included multiple activities on ethics, reported a higher need for more ethics education than students in the control group did. While this finding may seem counterintuitive, once students were exposed to more ethics education, they were more aware of the need for information and educational experiences in dealing with ethical issues in healthcare and healthcare research. Students who participated in the program have anecdotally reported an increased awareness of ethical issues and an increased desire for more educational experiences on making ethical decisions. However, the intervention group also reported more comfort in their abilities to deal with ethical issues.
After participation in an interprofessional campus-wide effort on health professions ethics, students demonstrated higher ethical decision-making scores according to the Health Professional Ethics Rubric. 32 However, their scores still did not reach the proficiency level identified in the rubric. Examination of the effectiveness of each part of the intervention is needed to determine what is most helpful in enhancing students’ ethical decision-making skills. For example, 100% of students in the interprofessional ethics and history course were able to score proficient using the rubric on a course assignment similar to the questionnaire used in the program evaluation.
Students had the most difficulty relating the options for addressing the ethical issue to professional values or an ethical framework. This item most likely indicates the highest level of critical thinking. The other three items only require self-awareness of issues and options to address the issue while thinking through the options from an ethical framework requires a more objective and critical review of the situation and options.
Barriers to interprofessional education were similar to previous reports—students were on different schedules and in different locations. Online courses appeared to be the most effective in reducing these barriers. One advantage of an online format is that students do not necessarily know the profession of the students they are interacting with in the discussion, thus eliminating some of the biases of professional stereotyping.
Further research is also needed to determine the most effective interventions and the number and timing of interventions. This approach was broad-based and used a variety of methodologies in an attempt to reach all students on campus. While there is evidence that The Brewsters was effective in increasing knowledge, 29 more research is needed on the impact of other strategies on improving ethical decision-making skills. Future study could also illuminate the differences in students’ perceptions of ethics education and decision-making skills in relation to their respective schools and professions.
Ethics education is essential for nursing education at all degree levels, because each day nurses face ethical dilemmas. Again, these include issues related to changes in technology, such as gene manipulation, as well as complex end-of-life decisions and allocation of resources. Thus, education needs to not only address basic knowledge in clinical ethics but also enable the student to obtain operational skills for dealing with these issues. They need to be able to identify that there is an ethical issue, analyze the issue and its possible solutions and outcomes, and then navigate the complex social process of working with other providers, patients, and families in implementing appropriate responses. Educators should strive to continue to develop new methods for helping students to obtain these skills, and they should rigorously evaluate their educational methodology in an ongoing manner.