
Abstract
Background:
Individualized care is closely related to the fulfillment of nurses’ ethical responsibilities regarding the provision of healthcare as well as having a strong foundation in the philosophy of nursing.
Objective:
This study aimed to determine the association of job satisfaction and burnout with individualized care perceptions in nurses working at a university hospital located in the Central Black Sea region of northern Turkey.
Research design:
A cross-sectional correlational survey design.
Participants and research context:
The study was conducted between 15 February 2017 and 15 August 2017 with 419 nurses working at a public university hospital located in Samsun. Data were collected using an information form, the Individualized Care Scale-Nurse Version, the Minnesota Job Satisfaction Scale, and the Maslach Burnout Inventory. The Mann–Whitney U test, Kruskal–Wallis test and Spearman Correlation were used.
Ethical considerations:
Ethical approval for the study was obtained from the Ondokuz Mayıs University Clinical Studies Board of Ethics. Oral informed consent was taken from the participants.
Findings:
There was a significant positive relationship between the total Individualized Care Scale-A Nurse Version score and the General Satisfaction subscale score of the Minnesota Job Satisfaction Scale (r = 0.121, p < 0.05). The total Individualized Care Scale-A Nurse Version score increased as the General Satisfaction subscale score of the Minnesota Job Satisfaction Scale increased. There was a significant negative relationship between the total Individualized Care Scale-B Nurse Version score and the Desensitization (r = –0.143, p < 0.01) and Personal Achievement subscale scores of the Maslach Burnout Inventory (r = –0.182, p < 0.01). The Desensitization and Personal Achievement subscale scores of the Maslach Burnout Inventory increased as the total Individualized Care Scale-B Nurse Version score decreased.
Discussion:
Factors associated with the individualized care perceptions of nurses, such as job satisfaction and burnout levels and factors related to personal life and worklife should be taken into consideration. Also in order to increase job satisfaction and motivation in nurses, personal preferences regarding the service they want to work at should be taken into account.
Conclusion:
Nurses with lower burnout and higher job satisfaction were found to have higher individualized care perceptions and to support the individuality of patients in care applications. It is important to consider work-related factors associated with individualized care perceptions, job satisfaction, and burnout in nurses.
Introduction
Healthcare ethics, clinical ethics, and nursing ethics underscore the importance and value of every patient as individuals. 1 International Council of Nurses (ICN) stated that the fundamental responsibility of a nurse is to preserve life, alleviate pain and suffering, and promote health and that respect for people, human rights, and appreciation of people are inherent to nursing. 2 Good clinical practice requires nurses to have adequate knowledge regarding ethical issues such as informed consent, autonomy, truthfulness, honor, patient rights, and individuality. 3 The right to be respected as an individual is among the cornerstones of nursing ethics. 3 Accordingly individualized care, which is about fulfilling ethical responsibilities in health services, has a strong foundation in the philosophy of nursing. 1 Nurses can plan the best and most effective care for every patient by supporting the patient’s individuality. 4 They can also protect the honor and uniqueness of every patient. 3,5 It is of utmost importance that nurses provide individualized care focused on specific patient problems and needs in accordance with the profession’s ethical responsibilities. 3
Individualized care, which is shaped according to multiple factors including culture, religion, and life experiences of an individual, stresses that individuals have different personal values and beliefs which should be respected. 6 Individualized care takes into account that each individual is in a dynamic interaction with the environment he or she lives in Amaral et al. 7 Individualized care focuses on the individual and his or her health problem. 5 According to individualized care, each individual is unique and different applications need to be performed in order to meet their needs. 8,9
Individualized care encompasses care applications emerging during the interaction between the nurse and the patient.
10
It is the application of nursing care according to the emotions, thoughts, experiences, and perceptions of the individual.
1,4,5,8
Suhonen et al.
1,4
have defined individualized care as how nursing care is adapted for the specific health condition of the individual, his/her characteristics, needs, and preferences, as well as being a form of nursing care applied according to the views of the patient on how the patient perceives the reflection of the individuality of the patient in the applications of nurses.
Individualized care was found to increase patient satisfaction, 12,13 strengthen the ability of individuals to manage their own care at home after discharge, 13 and increase quality of life. 14,15 At the same time, it has been underscored that developing an individual centered approach and attitude was closely related to the worklife of nurses, increasing their job satisfaction and motivation. 14,16 –18
Job satisfaction is a very important factor as it enables working happily, productively, and efficiently. 19 The job satisfaction of nurses can be affected by several factors including age, marital status, willingly choosing the profession, employment duration, the working environment and its conditions, relations to managers and colleagues, uncertainties regarding professional roles, and employment statuses. 19 In this context, many individual and organizational factors can decrease the job performance and efficiencies of nurses, causing them to experience burnout. 20
Burnout in nurses can cause various problems in nurses including insomnia, fatigue, short temper, decreased self-esteem, anxiety, alienation to the institution, reduced work motivation, and communication problems with the health team members, patients, and their relatives. 20,21 In worklife, burnout can lead to decreased productivity, difficulties in realizing professional responsibilities, and decreases in the efficiency of the institution and the quality of care. 22,23 At the same time, burnout may negatively affect the ability of nurses to understand the individual they care for and his or her family, interpret verbal and non-verbal behavior, and meet their needs. 24
Provision of high-quality healthcare is dependent upon nurses’ satisfaction with the institution and the workplace. Accordingly nurses with high job satisfaction and low burnout can provide individualized care at optimal levels. 25 Previous studies indicated that little is known about the association of nurses’ individualized care perceptions with job satisfaction and burnout at healthcare settings. 26 –28 To our knowledge, this study is the first to examine the association of nurses’ individualized care perceptions with job satisfaction and burnout in Turkey. The current study will provide insights to the association of nurses’ individualized care perceptions with job satisfaction and burnout, which in turn can be used in developing appropriate strategies for increasing the quality of care provided to healthy/ill individuals.
Aim
This study was conducted in order to determine the association of job satisfaction and burnout with individualized care perceptions in nurses working at a university hospital located in the Central Black Sea region of northern Turkey.
This study aimed to answer the following questions: At what level are the individualized care perceptions of the nurses? At what level are the burnout and job satisfactions of the nurses? Are nurses’ burnout and job satisfaction levels associated with individualized care perceptions? Are factors related to nurses and the institution (age, gender, marital status, educational level, the service they worked at, employment duration, type of employment, employment status, number of patients cared for, loving the job, voluntary choice of the profession, satisfaction with the service they work at) associated with individualized care perceptions?
Methods
Study design and sampling method
The study was conducted between 15 February 2017 and 15 August 2017 at the public university hospital located in Samsun. This hospital has 1000 beds and is the largest and most developed university research hospital of the Central Black Sea region of northern Turkey. The majority of patients from Samsun and nearby cities are treated at this hospital. In Samsun, healthcare services are provided by public hospitals, public university hospitals, and private hospitals.
Data were collected from nurses working at the university hospital’s internal medicine units (Hematology, Oncology, Infectious Diseases, Physical Therapy, Dermatology, Chest Diseases, Cardiology, Neurology, Nephrology, Endocrine, Gastrology, and Psychiatry), surgical units (Neurosurgery, General Surgery, Chest Surgery, Obstetrics and Gynecology, Cardiovascular Surgery, Otorhinolaryngology, Ophthalmology, Orthopedics and Traumatology, Plastic Surgery, and Urology), and intensive care units (Internal medicine-intensive care, Cardiovascular Surgery intensive care, and general-intensive care unit).
In this study, the nurses were chosen using random sampling which is a probability sampling method. In random sampling, individuals can be chosen from the universe with equal probability. The sample size to represent the universe of the study was calculated as 397 based on a pool of 630 nurses working at the hospital with a 95% confidence interval and 3% margin of error. Thinking that there could be missing data, data collection was ended when 419 nurses were reached.
Nurses who (1) worked at internal medicine, surgery, and intensive care units; (2) directly provided patient care; (3) obtained the title “nurse” after completing basic education; and (4) volunteered to participate were recruited for the study at the study hospital. Nurses in Turkey can be categorized into four groups according to their education: Nurses may graduate from attending a 4-year nursing degree at vocational high schools after 8 years of basic education. A large number of vocational high school graduates are working in the health sector. Nurses may also graduate from a 2-year degree at vocational schools and earn a pre-bachelor’s degree in nursing. At present, graduates from these schools are working in healthcare, but these schools no longer exist. Four-year nursing schools offer a bachelor’s degree in nursing. Nurses may also have a master’s degree or higher (PhD). All these nurses have the same title and the same level of autonomy and responsibilities, thus, all nurses have the same level of liability for actions that result in breaches of the standards of care. After 2014, vocational high school graduates gained the title “nurse associate.” However, nurse associates have not been commissioned to healthcare institutions by state exams yet.
In Turkey, nurses are employed as permanent staff or on contract (temporary employment). In order to become a permanent staff member, nurses need to take the nationwide public personnel selection exam and make preferences for hospitals to work at after reaching a certain score in this exam. Nurses who cannot achieve the required exam score can apply to hospitals in order to work on contract. Contracted personnel candidates are ranked according to the results of the public personnel selection exam and are interviewed for the job. Nurse candidates who pass the interview start working with a 1-year contract. This contract is renewed every year, but it can be nullified if deemed necessary by the hospital management. Unlike nurses on permanent staff, contracted nurses cannot transfer to other hospitals during employment. According to the code of hospital employment conditions issued by the Turkish Ministry of Health, nurses can work in 8-h shifts or they can work for 16 or 24 h depending on institutional policies.
In Turkey, nurses working at healthcare institutions comprise of young and middle-aged nurses. Public personnel’s age of retirement is calculated with a gradual system in Turkey. Accordingly, nurses who completed adequate years of service can prefer not to continue working and can retire early. In Turkey, a graduated pension system was put into effect since 30 April of the year 2008. In this system, the age of retirement for men is 60 years and 58 for women until the year 2036. From the year 2036, the age of retirement will increase gradually and become 65 for men in 2044 and 65 for women in 2048. On the other hand, gender discrimination in nursing was ended with the modifications made to the nursing law in 2007, enabling men to become nurses as well. Thus, the number of male nurses is very low compared to female nurses in the healthcare system.
Nurses who did not agree to participate in the study (n = 28), and those who were on leave between the dates when the study was conducted (n = 56) were not included in the sample. In addition, nurses working at the polyclinic and surgery services where inpatients were not treated and patients did not directly receive nursing care were excluded from the study (n = 127).
Data collection
Data were collected using an information form regarding the socio-demographic and employment characteristics of the nurses prepared by the researcher according to literature, 12,28,29 the Individualized Care Scale-Nurse version (ICS-Nurse), the Minnesota Job Satisfaction Scale, and the Maslach Burnout Inventory. The questionnaires were tested by a pilot study conducted with 10 nurses. The pilot study revealed that none of the questions or statements in the questionnaire was misunderstood or incomprehensible. The nurses in the pilot study were not included in the final sample. The information form and scales were completed by nurses in a quiet room during hours when their workload was less. Data collection took approximately 15–20 min per person.
Data collection tools
Nurse information form
The nurse information form consisted of 24 questions, 4 regarding socio-demographic characteristics and 20 regarding employment characteristics.
The Individualized Care Scale - Nurse Version
The ICS-Nurse is a scale developed by Suhonen et al. 14 to evaluate the views of nurses in the healthcare environment on individualized care. The Turkish adaptation of the scale was performed by Acaroğlu and Şendir. 28 The ICS-Nurse Version is a 5-point Likert-type scale consisting of two sections, A and B, with 17 items each. In the first section of the scale (ICSA-Nurse), how much the nurses support the individuality of patients during care applications is questioned, while in the second section (ICSB-Nurse), their perceptions on individualizing the care of patients is evaluated. In both sections of the scale, there are three sub-dimensions: Clinical Condition, Personal Life Condition, and Decision-Making Control.
The minimum score that can be obtained from each section and sub-dimension of the ICS-Nurse version is 1, while the maximum is 5. The mean scores of the sub-dimensions are calculated by summing the scores from the items included in each sub-dimension and dividing it by the number of items. Higher scores indicate that nurses support the individuality of the patient during the nursing applications that they generally apply (ICSA-Nurse) and that they have high perceptions regarding the individualization of patient care (ICSB-Nurse). 4,14
The ICS-Nurse is commonly used in many countries for determining nurses’ opinions on individualized care. Previous studies reported that the ICS-Nurse is valid and reliable, with Cronbach’s alpha coefficients ranging from 0.88 to 0.90. 27,30,31 Acaroğlu and Şendir, 28 found the Cronbach’s Alpha reliability coefficient of the ICS-Nurse to be 0.77 for the ICSA-Nurse and 0.88 for the ICSB-Nurse. In this study, the Cronbach’s alpha reliability coefficient of the ICS-Nurse was found to be 0.93 for the ICSA-Nurse and 0.95 for the ICSB-Nurse.
The Minnesota Job Satisfaction Scale
The Minnesota Job Satisfaction Scale is a scale developed by Weiss et al. 32 to measure job satisfaction, and was tested for validity and reliability in Turkish by Baycan. 33 The Minnesota Job Satisfaction Scale is a 5-point Likert-type scale with 20 items that show the internal and external satisfaction factors experienced by individuals regarding their job. The lowest score that can be obtained from the scale is 20, while the highest is 100. The Minnesota Job Satisfaction Scale has three sub-dimensions, namely General Satisfaction, Internal Satisfaction, and External Satisfaction.
Internal satisfaction consists of factors regarding the internal quality of the job such as success, recognition, approval, the job, responsibilities, and advancement options. The internal satisfaction score is calculated by dividing the total score from the internal factor items (1, 2, 3, 4, 7, 8, 9, 10, 11, 15, 16, and 20) by 12. The minimum score that can be attained from this sub-dimension of the scale is 12, while the maximum is 60. Higher scores indicate increased internal satisfaction. External satisfaction consists of factors related to the job such as institutional policy, management and supervision type, relations to colleagues and employees, working conditions, and pay. The external satisfaction score is calculated by dividing the total score from the external factor items (5, 6, 12, 13, 14, 17, 18, and 19) by 8. The minimum score that can be attained from this sub-dimension is 8, while the maximum is 40. Higher scores indicate increased external satisfaction. General satisfaction is calculated by dividing the total score from 20 items, which include the internal and external satisfaction factors, by 20.
The Minnesota Job Satisfaction Scale is commonly used in many countries for measuring employees’ job satisfaction. Previous studies reported that the Minnesota Job Satisfaction Scale is valid and reliable, with Cronbach’s alpha coefficients ranging from 0.88 to 0.91. 34 –36 Baycan 33 found the Cronbach’s alpha reliability coefficient of the Minnesota Job Satisfaction Scale to be 0.77. In this study, the Cronbach’s alpha reliability coefficient of the Minnesota Job Satisfaction Scale was found to be 0.89.
The Maslach Burnout Inventory
The Maslach Burnout Inventory is a scale developed by Maslach and Jackson, 37 and adapted to Turkish and tested for validity and reliability by Ergin. 38 The Maslach Burnout Inventory is a 5-point Likert-type scale with 22 items that evaluates job burnout of individuals and has three sub-dimensions, namely Emotional Burnout, Desensitization, and Personal Achievement. In this scale, scores obtained from each sub-dimension are evaluated separately.
The emotional burnout sub-dimension, which aims to indicate whether individuals feel fatigue and excessive emotional burnout, is calculated through the total of 9 items (1, 2, 3, 6, 8, 13, 14, 16, and 20). The minimum score that can be obtained from this sub-dimension is 0, while the maximum is 36. Higher scores indicate higher emotional burnout levels.
The desensitization sub-dimension, which was defined by Maslach as “distant, strict, or even inhumane responses to service receivers,” is calculated through the total of 5 items (5, 10, 11, 15, and 22). The minimum score that can be taken from this sub-dimension is 0, while the maximum is 20. Higher scores indicate higher desensitization levels.
The personal achievement sub-dimension, which terms lack of personal success, sufficiency of personal success, and problems being overcome through success, is calculated through the total of 8 items (4, 7, 9, 12, 17, 18, 19, and 21). The minimum score that can be obtained from this sub-dimension is 0, while the maximum is 32. Higher scores indicate lower personal achievement levels.
The Maslach Burnout Inventory is widely used throughout the world for measuring burnout among employees. Previous studies indicated that the Maslach Burnout Inventory is valid and reliable and that Cronbach’s alpha coefficients of the emotional burnout sub-dimension ranged from 0.86 to 0.90, 0.77 to 0.79 for Desensitization, and 0.71 to 0.78 for Personal Achievement. 39 –41 Ergin found the Cronbach’s alpha reliability coefficients of the sub-dimensions of the Maslach Burnout Inventory to be 0.83 for Emotional Burnout, 0.65 for Desensitization, and 0.72 for Personal Achievement. 38 In this study, the Cronbach’s alpha reliability coefficients of the sub-dimensions of the Maslach Burnout Inventory were found to be 0.84 for Emotional Burnout, 0.73 for Desensitization, and 0.67 for Personal Achievement.
Data analysis
The data were analyzed using the IBM SPSS V23 software. The normality of quantitative data was examined using the Shapiro–Wilk test. The Mann–Whitney U test and the Kruskal–Wallis test were used where normality of data could not be established. In the examination of the relationships between variables, the Spearman Correlation was used. The level of statistical significance was accepted as p < 0.05.
Ethical considerations
The study protocol was approved by the Ondokuz Mayıs University Clinical Studies Board of Ethics (13.02.2017/ number; B.30.2.ODM.0.20.08/682-749). Permission to conduct the study was granted by the study hospital’s chief doctor (15374210-929-E.4423). Data were collected by the researchers. Nurses who met the inclusion criteria were invited by the researchers to participate in the study. Nurses who participated in the study were informed about the study, and their oral informed consent was taken. They were explained that the decision to participate in the study was completely theirs, their names will not be written on the questionnaires, and data collected for the study will be used for scientific purposes only. Nurses received a written instruction on how to complete the questionnaires. The descriptive information form and the scales were completed by the nurses during hours of less workload. Service head nurses provided a quiet room for the participants to fill out the questionnaires. Necessary permissions were obtained in order to administer the three scales used in this study.
Findings
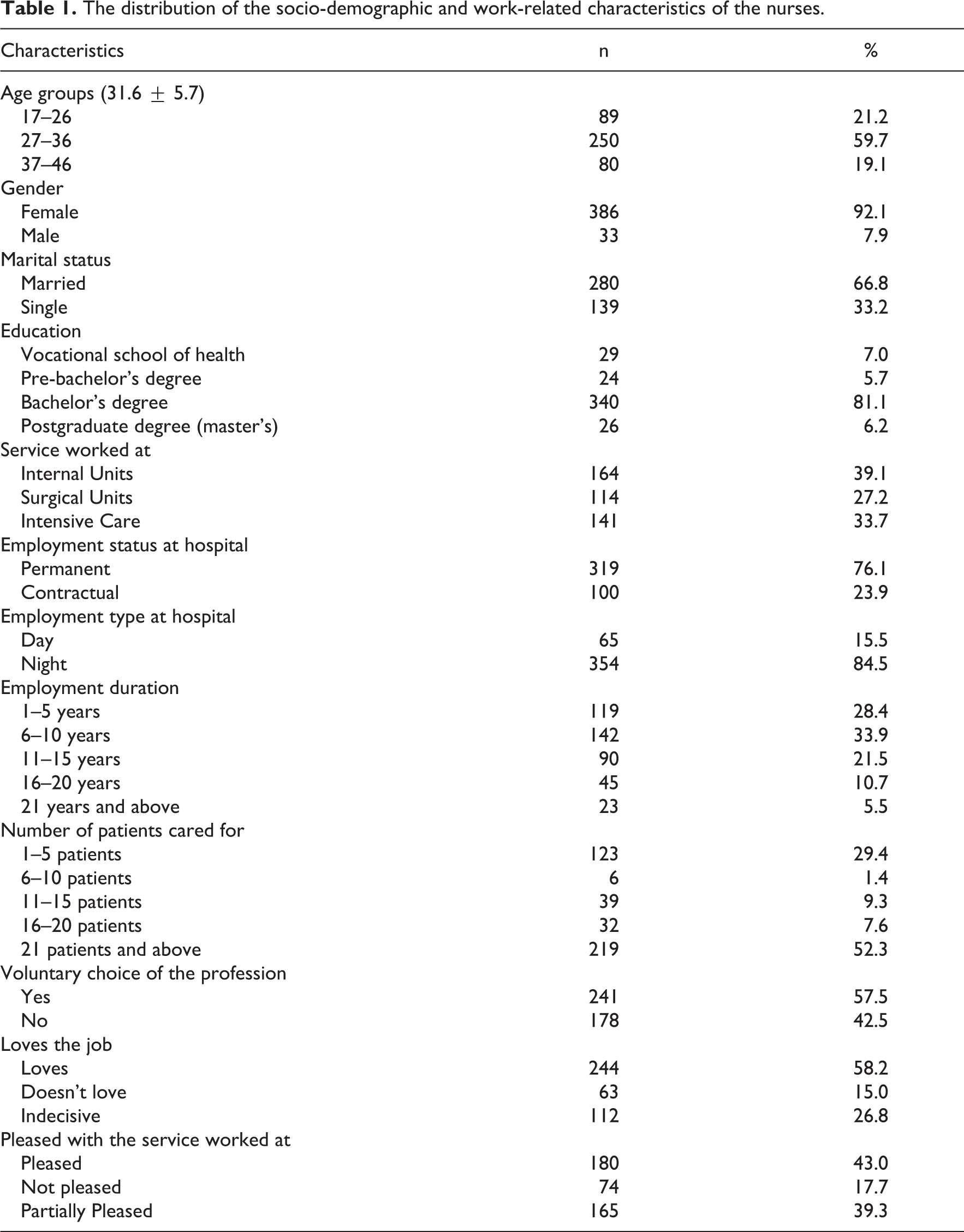
A total of 419 nurses participated in the study. It was determined that 21.2% of the nurses were aged 17–26 years, 59.7% were aged 27–36 years, and 19.1% were aged 37–46 years. Among the nurses, 92.1% were female, 7.9% were male, 66.8%were married, 33.2% were single, 7% graduated from a vocational school of health, 5.7% had a pre-bachelor’s degree, 81.1% had a bachelor’s degree, 6.2% had a postgraduate degree, 39.1% worked at the internal medicine unit, 27.2% worked at the surgical units, 33.7% worked at the intensive care units, 76.1% were permanent staff, 23.9% were on contract, 15.5% worked only during daytime, 84.5% worked only in night shifts, 33.9% worked as a nurse for 6–10 years, 52.3% had 21 and more patients, 57.5% voluntarily chose the nursing profession, 58.2% loved their job, and 43% were satisfied with the service they worked at (Table 1).
The distribution of the socio-demographic and work-related characteristics of the nurses.
The mean total ICSA-Nurse score was found to be 3.9 ± 0.7 with a median of 3.9. The median scores of the Clinical Condition, Personal Life Condition, and Decision Making Control sub-dimensions of the ICSA-Nurse were found to be 4.0, 3.5, and 4.0, respectively. The mean total ICSB-Nurse score was found to be 4.1 ± 0.6 with a median of 4.0. The median scores of the Clinical Condition, Personal Life Condition, and Decision Making Control sub-dimensions of the ICSB-Nurse were found to be, respectively, 4.3, 4.0, and 4.2. The mean General Satisfaction, Internal Satisfaction, and External Satisfaction sub-dimension scores of the Minnesota Job Satisfaction Scale were found to be respectively 56.9 ± 12.3, 37.8 ± 7.1, and 19.1 ± 6.5. The mean Emotional Burnout, Desensitization, and Personal Achievement sub-dimension scores of the Maslach Burnout Inventory were found to be 23.2 ± 6.7, 7.2 ± 4.3, and 11.0 ± 4.6, respectively (Table 2).
The Individualized Care Scale, Minnesota Job Satisfaction Scale, and Maslach Burnout Inventory scores of the nurses.

ICS-A: individualized care scale-A; ICS-B: individualized care scale-b;
The total ICSA-Nurse score had weak but significant positive relationships with the Internal Satisfaction (r = 0.183, p < 0.01) and General Satisfaction (r = 0.121, p < 0.05) sub-dimension scores of the Minnesota Job Satisfaction Scale. Also, the total ICSA-Nurse score had weak but significant correlations with the Desensitization (r = –0.115, p < 0.05) and Personal Achievement (r = –0.256, p < 0.01) sub-dimension scores of the Maslach Burnout Inventory (Table 3).
The relationship between the ICSA and ICSB Nurse versions, the Minnesota Job Satisfaction Scale and the Maslach Burnout Inventory.

r: spearman correlation coefficient.
*p
A weak but significant positive relationship was found between the total ICSB-Nurse score and the Internal Satisfaction (r = 0.125, p < 0.05) sub-dimension score of the Minnesota Job Satisfaction Scale, while a weak but significant negative relationship was found between the total ICSB-Nurse score and the External Satisfaction (r =–0.108, p < 0.05) sub-dimension score of the Minnesota Job Satisfaction Scale. The total ICSB-Nurse score had weak but significant negative relationships with the Desensitization (r = –0.143, p < 0.01) and Personal Achievement (r = –0.182, p < 0.01) sub-dimension scores of the Maslach Burnout Inventory (Table 3).
Discussion
In this study, the mean total ICSA-Nurse score, which evaluates how much the nurses support the individuality of the patients they care for, was found to be 3.9 ± 0.7, while the mean total ICSB-Nurse score, which evaluates the perceptions of nurses regarding the individualization of patient care, was found to be 4.1 ± 0.6. In a study performed by Suhonen et al. 11 which compared individualized care perceptions of nurses from different countries, the mean total ICSA-Nurse score of Turkish nurses was found to be 3.96 ± 0.48, while their mean total ICSB-Nurse score was found to be 3.93 ± 0.52. 11 In another study, the mean total ICSA-Nurse score was reported to be 3.80 ± 0.72. 29 In the current study, the ICSA-Nurse and ICSB-Nurse scores of the nurses, which implied that they supported patient individuality, were in line with previous study findings.
The mean total ICSA-Nurse and ICSB-Nurse scores were found to be higher in nurses who had bachelor’s and postgraduate degrees, worked during the day, were employed in surgical units, loved the job, were pleased with the service worked at, were female, and had an employment duration of 21 years or more. In parallel to our findings, Idvall et al. 30 found that nurses with postgraduate degrees supported individualized care. Despite the findings of our study, other studies reported that individualized care scores did not vary according to gender, 3,30 educational level, and employment type. 29
In the current study, it was determined that nurses with higher levels of education prioritized patients’ uniqueness during the provision of healthcare. Nurses are obliged to be sensitive toward patients’ physical and emotional needs and provide care accordingly. In this aspect, ethical sensitivity and responsibility are important for nurses who provide care based on their own moral values. 42 Ethical codes guide professionals in dealing with problems related to proper applications or acts. Moreover, nursing ethics compel nurses to act in a certain way during the provision of high-quality healthcare. 43
According to the findings of this study, the total ICSB-Nurse score was found to be higher in nurses who had an employment duration of 21 years or more. The higher individualized care perception in nurses with greater employment duration can be related to the improvement inexperienced nurses’ knowledge, skills, and attitudes in patient care as well as their problem-solving skills. Appreciation of one’s occupation is also strongly associated with the quality of the care provided. Effective provision of care requirements for the individual depends on nurses’ willingness to do their job. Nurses who chose their job willingly since they found the skills and abilities required by the job appropriate for themselves can adapt to their work environment easier, and thus experience increases in their dedication to their job and institution as well as their job satisfaction.
In the current study, nurses who worked as permanent staff had higher ICSA-Nurse and ICSB-Nurse scores compared to nurses who worked on contract. These findings may stem from the fact that contracted nurses experience stress and anxiety related to possible job loss, while nurses on permanent staff think they have job security in the future. 44
It is known that working in shifts may cause negative effects in terms of physical and psychological health and negatively affect the quality of the care provided by nurses. 45 Working in night shifts in particular may cause fatigue, attention and perception deficits, difficulties in decision-making, stress, burnout, reduced job satisfaction, loss of motivation, insufficiencies in patient care and monitoring, and communication problems with health team members in nurses. 20,45 The socio-demographic and work life–related characteristics of nurses associated with ICSA-Nurse and ICSB-Nurse scores vary according to the study settings, the working environment, working conditions, and care load of nurses.
In the current study, it was found that the nurses had moderate levels of job satisfaction and that ICSA-Nurse scores increased as the General satisfaction sub-dimension score of the Minnesota Job satisfaction Scale increased. Nurses regarding the internal (success, recognition, responsibilities, etc.) and the external characteristics of the job (institutional policy, relationships to colleagues and employees, working conditions, etc.) and nurses with high job satisfaction were found to support the individuality of the patients at very high rates. In a study by Edvardsson et al., 46 which was conducted with nurses who worked at retirement homes, it was reported that there was a significant relationship between the level of individualized care provision and job satisfaction.
It was determined that the nurses had high levels of emotional burnout and that the Desensitization and Personal Achievement sub-dimension scores of the Maslach Burnout Inventory decreased as ICSA-Nurse and ICSB-Nurse scores increased. Accordingly, nurses with high personal achievement and low desensitization were highly supportive of individualize care. Previous studies are in line with these findings as they indicated that factors including job satisfaction affected the care provided by nurses and set the ground for ethical problems. 47 –49
A variety of factors such as long working hours, heavy workload, working in shifts, dissatisfaction with the work environment, negative interactions between team members, role conflict, and role ambiguity can lead to burnout in nurses. Having a negative working environment in particular can precipitate moral distress. Jameton, 50 Hamric, 51 and Wilkinson 52 indicated that moral distress derives from limitations in units, the healthcare system, and the environment and people working at an ethically enhanced work environment experience significantly less moral distress. In this context, it is of paramount importance that managers pay attention to factors related to employee burnout and device a working environment which increases job satisfaction and motivation.
Although the individualized working environment forms the basis of individualized care, 53 the individualized care applications of nurses are highly related to a positive working environment and job satisfaction. 17,26,27 Indeed, it has been reported that the quality of the care provided in healthcare environments and positive perceptions regarding the work environment increase job satisfaction, 54 with nurses providing high-quality care being more satisfied with their job. 55 In this aspect, individualized care is an indicator of care quality. 56 Also, the quality of care is closely linked to job satisfaction and burnout. Although it is possible to mention an indirect relationship between job satisfaction, burnout, and individualized care, 16,26,27,54,55,57 it is important to examine this relation and develop appropriate strategies on the subject.
Strengths and limitations
This is the first study to examine the association of job satisfaction and burnout with individualized care perceptions in nurses working at a university hospital located in the Central Black Sea region of northern Turkey. One of the strengths of the study include revelation of factors, such as the work environment and conditions arranged by managers, associated with the provision of individualized care. A limitation of the study is that observations and evaluations regarding the effects of nurses’ job satisfaction and burnout on individualized care practices could not be undertaken. Future studies can employ qualitative research methods as well and conduct focus groups regarding the effects of nurses’ job satisfaction and burnout on individualized care perceptions.
Clinical and research impact of study
Work-related factors associated with nurses’ individualized care perceptions, job satisfaction, and burnout should be determined, and necessary precautions should be taken accordingly. Also, the number of patients nurses care for should be taken into consideration and human resources planning at healthcare institutions should be done properly. In order to increase nurses’ job satisfaction and motivation, their individual choices regarding the clinics they wish to work in should be considered. Training programs and seminars should be arranged for reinforcing care behaviors supportive of patient individuality. In addition, managers should use motivators that may affect nurses’ job satisfaction and provide routine feedback on nurses’ achievements. It is recommended to cross-cultural studies on the topic by examining different samples from different countries.
Conclusion
There was a weak but significant positive correlation between the total ICSA-Nurse score and the General Satisfaction sub-dimension score of the Minnesota Job Satisfaction Scale. It was determined that the total ICSA-Nurse score increased as the General Satisfaction sub-dimension score of the Minnesota Job Satisfaction Scale increased. The total ICSA-Nurse and the ICSB-Nurse scores were weakly but significantly and positively associated with the Desensitization and Personal Achievement sub-dimension scores of the Maslach Burnout Inventory. It was determined that the total ICSA-Nurse and the ICSB-Nurse scores increased as the Desensitization and Personal Achievement sub-dimension scores of the Maslach Burnout Inventory decreased. Accordingly, nurses with high job satisfaction and low burnout levels had higher individualized care perceptions, which is affected by various factors including culture, religion, and life experiences.
Footnotes
Acknowledgements
We thank the nurses who participated in our study.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ondokuz Mayıs University BAP Commission with the project number PYO.SBF.1904.17.002.
Ethical approval
Ethical approval for the study was obtained from the Ondokuz Mayıs University Clinical Studies Board of Ethics (13.02.2017/ no; B.30.2.ODM.0.20.08/682-749).