
Abstract
Background:
Patients and their caregivers are expected to take joint responsibility for reporting symptoms and seeking medical assistance, for example, by calling oncology emergency telephones or other helplines during a cancer trajectory.
Research objective:
The aim was to explore the meaning of responsibility as it appeared in patients’ or caregivers’ experiences of calling an oncological emergency telephone.
Design, participants and context:
Inspired by qualitative description and qualitative content analysis, a secondary analysis of data from interviews with 12 participants calling the oncological emergency telephone at a Danish university hospital was performed.
Ethical considerations:
The project observes demands for safekeeping data and all regulations concerning research ethics in agreement with the Nordic Nurses Federation and the Danish Health Act.
Findings:
Two main themes emerged: (1) to act responsibly as a patient or caregiver was to ‘be watchful and alert’, ‘report symptoms the right way’ and ‘do crosschecking’ and (2) to deal with the burden of responsibility was to ‘feel safe when dealing with the burden of responsibility’ and ‘be relieved from the burden of responsibility’.
Discussion:
Too much responsibility and a potential imbalance between healthcare professionals’ expectations and callers’ knowledge and capacity to act may place additional burdens on the callers, which may be eased by person-centred care.
Conclusion:
The meaning of responsibility appeared in the participants’ capacity to act, where they observed, assessed and reported symptoms and controlled prescribed treatments as well as shared or handed over the responsibility to the healthcare providers. Thus, the analysis provided essential knowledge for healthcare professionals on how patients and caregivers handle this responsibility when faced with a cancer disease that is treated on an outpatient basis.
Keywords
Introduction
Multiple signs of responsibility appeared in an analysis of interviews aiming to explore patients’ and caregivers’ experience of calling the oncological emergency telephone (OET) at a Danish university hospital (unpublished material; the paper is in review at Cancer Nursing but not yet accepted.). Patients and caregivers were encouraged to call the OET in case of severe symptoms from the disease or side effects from the treatment. From a qualitative approach, the analysis revealed patients’ and caregivers’ deliberations about when to call and what to report and illustrated how the telephone was perceived as a lifeline. They rather called ‘one time too many than one time too few’ when the patient’s condition changed. During this primary analysis, responsibility appeared as an underlying pattern that made additional demands on patients and caregivers. This insight urged us to undertake a secondary analysis of the data focusing on how responsibility appeared between the lines in the interviews.
Background
Given the trend towards shorter hospital stays and the increase in outpatient care, patients are increasingly left to self-manage their illness. 1,2 For cancer patients, this may involve handling serious symptoms of the disease and side effects from the treatment given when they are at home between their outpatient treatments. In order to prevent life-threatening side effects, patients are expected to perform self-assessment and report side effects from cancer treatment to their healthcare providers (HCPs). 3 –5 Staying at home during these conditions, patients are encouraged to call the OET to gain support in their self-management and to avoid unnecessary admission.
In accordance with national and international policies on partnership and involvement of patients in the healthcare systems, 6 –8 person-oriented care 9,10 and participation in one’s own care is highly valued. 11 Respecting patients’ individuality and values are essential, and support independent decision-making and feelings of being in control. 7 However, the increasing responsibility placed on patients makes the role of the caregiver in supporting patients more important and burdensome. 12,13 The caregiver is a person, defined by the patient, who provides unpaid assistance with physical care and psychosocial needs, 14 including cancer-specific care like complex symptom management related to the cancer disease or side effects from cancer treatment. 12,15
The cancer experience affects not only the patient but also the caregiver as symptoms of the cancer patients and the caregivers’ well-being may be associated. 16 For example, Valeberg and Grov 17 demonstrated that troubled sleeping in the patient had impact on the caregivers’ mental health regardless if the patient being in curative or palliative phase. Northouse et al. 18 found a reciprocal relationship between patients’ and caregivers’ emotional distress that varied by phases of illness. Moreover, testing the feasibility of using the Edmonton Symptom Assessment System to assess caregiver burden, Tanco et al. 19 found a statistical significant association between patients’ and caregivers’ experiences of fatigue, depression, anxiety and lack of sleep. Thus, given the responsibility for providing care, suffering may appear evident in patients as well as in their caregivers as the caregiver burden may increase alongside the degree of patients’ symptoms and suffering. Moreover, the caregiver burden may depend on whether the caregiving role is subjected to free choice or constraints. Carried out as a free choice, a positive association with the caregivers’ well-being was found, opposed to feeling constrained related to duty, lack of social support and financial resources. 20 Based on the above-mentioned conditions, taking care of oneself or others requires a high degree of responsibility performed in a complex context that may be demanding for patients and caregivers.
Responsibility
Personal responsibility rests on values inherent in the Western culture and is influenced and governed especially by the ethical principle ‘autonomy’ 21 that is a synonym for self-governance, self-determinism and self-rule. i The notion of autonomy ultimately perceives a person as one able to act competently and free of internal and external constraints 22,23 and guides the professionals in decision-making in their everyday practice. 21 The principle of autonomy runs through the goal of nursing, that is, to provide care and comfort to the patients while treating them as unique and valuable individuals, respecting their autonomy and integrity and ensuring the safety of the vulnerable human being. 24,25
Referring to Beauchamp and Childress’ definition of autonomy, Greaney et al. 23 quote autonomy as ‘self-rule that is free from both controlling interference by others and from personal limitations, such as inadequate understanding, that prevent meaningful choice’. In addition, regarded as a competent person, being autonomous entails the responsibility of providing self-care and self-management. 26 This also implies the responsibility to keep healthy and take care of oneself and being blameable if health turns into a serious condition. 21 Possessing adequate knowledge and being free for constraints, a responsible moral agent is consequently one who possesses the capacity to reflect upon his or her own actions, to act and to take an active role in decision-making.
However, the idea of ‘self-rule’ may be influenced by whether the person in focus is an ‘independent rational decision-makers’ or a vulnerable and deteriorated person. 27 In addition, Greaney et al. 23 discuss the idea of being free from internal and external constraints and introduce the notion of relational autonomy. In this perspective, one’s sense of responsibility to others is an integral component of the decisions-making process. This means that patients’ and caregivers’ autonomy and responsible actions must be seen in the light of the interdependent nature of life, and patients’ and caregivers’ commitment towards each other.
The responsibility for complex symptom management performed by patients and caregivers in a context of increasing outpatient care may be a challenge that needs attention from professionals. Given the responsibility for assessing when to call the OET among patients and caregivers, HCPs must understand and act on the meaning of responsibility when patients are at home during the cancer trajectory and experience symptoms that can be potentially life threatening. Although studies have described burdens of patients and caregivers, there is a lack of knowledge of what responsibility means for patients and caregivers when they are at home with potential life-threatening symptoms between their outpatient treatments. Exploring this in a profound way may provide HCPs with a deeper understanding of how users of the health system look at themselves as responsible agents and whether or when they need additional help from HCPs.
Hence, adopting a new objective, the aim of this study was to explore the meaning of responsibility as it appears among patients or caregivers calling the Danish OET.
Design
Methodology
To understand the meaning of responsibility, this study applies a qualitative descriptive design 28,29 and uses steps from qualitative content analysis to organise and interpret data from semi-structured interviews. A qualitative descriptive approach lies within the naturalistic research tradition and seeks to describe a phenomenon through the meanings the participants ascribe to them. From a qualitative point of view, knowledge about a phenomenon is created in interaction between the interviewee and the interviewer in the interview and between the transcribed text and the researcher in the analysis. 28 –31 Although qualitative description emphasises literal descriptions, it moves beyond the literal description of data in the attempt to interpret the findings. 28,29 As a text contains multiple meanings, it always contains more than one interpretation. 28,30,31 The interpretation of the interviews takes place in an iterative process between part of the text and the whole part, in a hermeneutical circle where the researchers’ preunderstanding is in interplay with the text. 32 However, applying analytical steps from qualitative content analysis, it is possible to stay close to the text and describe the manifest content of the interviews as well as interpret the latent content – the underlying meaning of responsibility appearing between the lines, still close to the participants’ experiences. 30 To levitate the findings into a more abstract level, the findings are finally discussed in interplay with theory and other research findings.
Participants
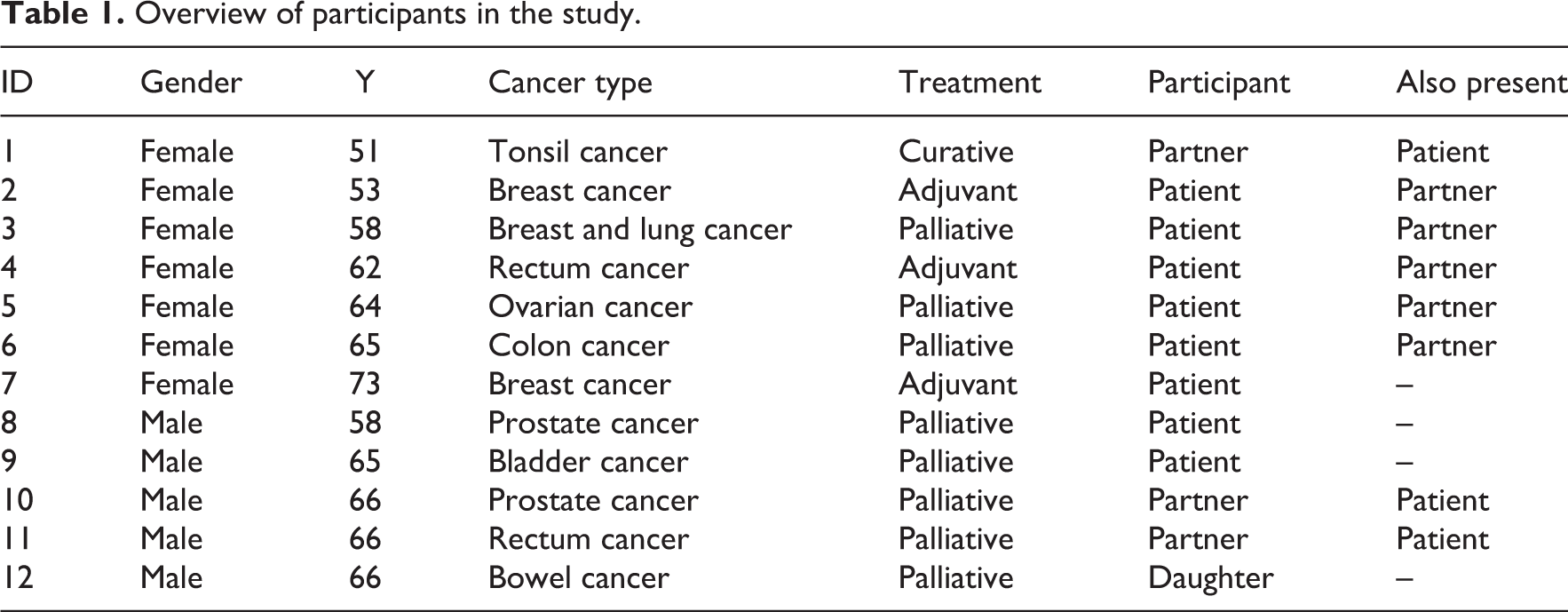
A total of 12 participants from a group of patients and caregivers who had called the OET within the last 2 months were purposively enrolled in the study (Table 1). Variation was obtained with regard to age, gender, diagnosis and whether the main participant was a patient or a caregiver. In eight interviews, the patient acted as the primary interview person, whereas in four interviews, the caregiver was the main interviewee. Patients with psychiatric diseases, brain tumours or brain metastases as well as patients unable to speak and understand Danish were not suitable for inclusion.
Overview of participants in the study.
Data collection
Initially, we conducted and transcribed verbatim semi-structured interviews with open-ended questions. The interviews aimed to answer three research questions about what initiated the call, reflections before the call and the participant’s experience of the telephone consultation. The interview guide contained no questions about responsibility. However, when analysing the participants’ experiences of the original questions, responsibility appeared as an underlying pattern during the preliminary analysis. As the interviews aimed to describe experiences from short telephone calls, the interviews were short and lasted between 15 and 33 min.
Data analysis
Content analysis is a means to structure data in qualitative studies with the core features to reveal meanings illustrated in themes that elucidate threads of underlying meanings and the expression of the latent content of the text. 30,31 Thus, the text was re-analysed through an open-minded inductive process that was built on analytical steps from qualitative content analysis, in accordance with qualitative description. 28,30,31
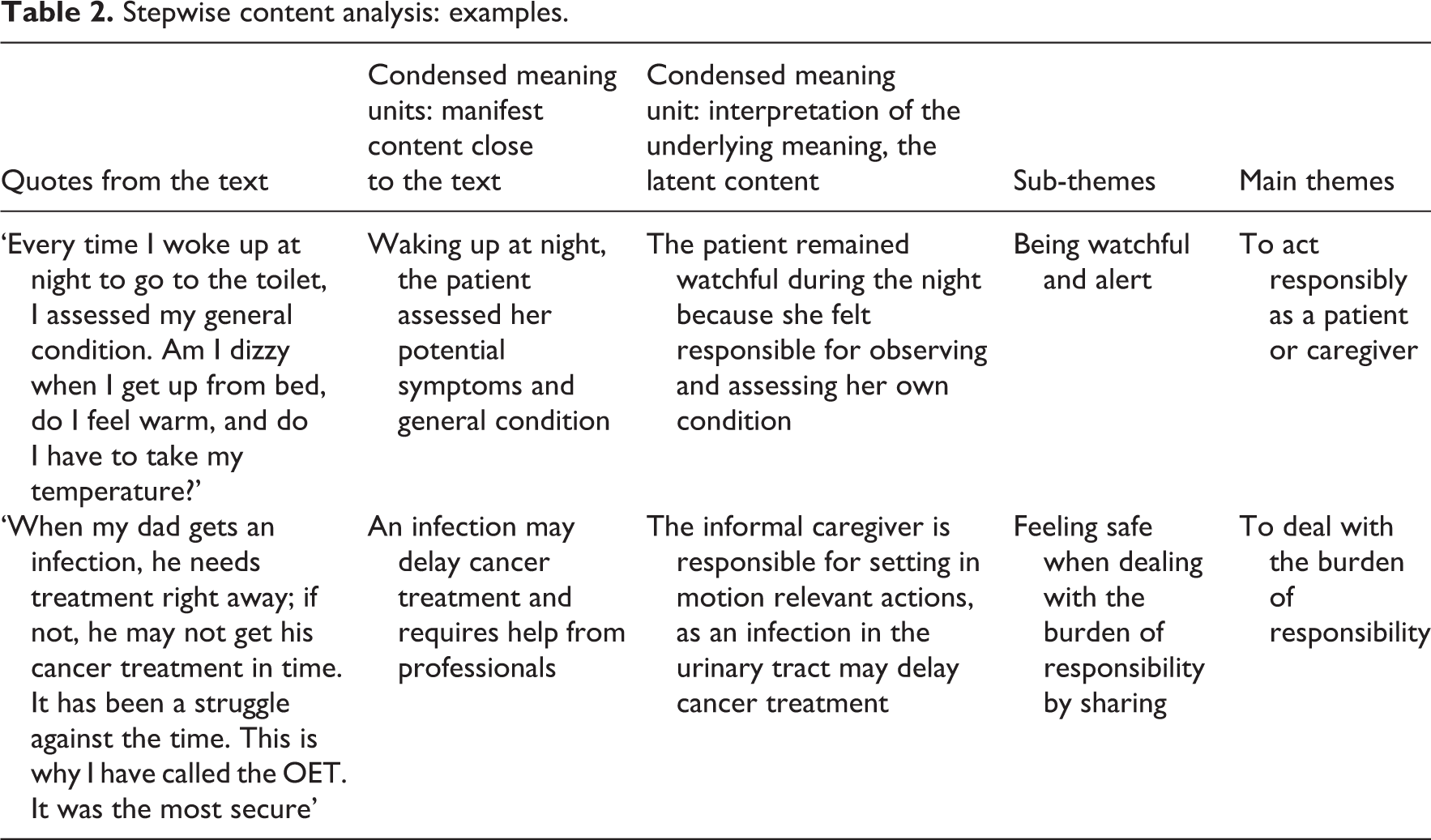
Based on the new objective, we reread the text several times, coded and separated the text that indicated the experience of responsibility. Looking for recurring themes, we organised and condensed the text in manifest and latent content. The analysis went on in a hermeneutical process in an interplay between the researchers and data in an iterative process of reading, analysing and rereading, 32 reflections and discussions of the text until consensus of main and sub-themes was obtained in the group of researchers (Table 2). In addition to providing the themes and sub-themes, the process continuously was a means to take into account our different preunderstandings and to ensure rigour in the analysis.
Stepwise content analysis: examples.
Ethical considerations
The Danish Data Protection Agency (ID number 2016-153) has been notified of the project. After having been informed orally and in writing about the project, the participants signed an informed consent form before being interviewed. 33,34 Participation was voluntary, and the participants were informed of their right to withdraw from the study at any time without any consequences. We gained the participants’ trust by replacing their names with numbers. The ethical dimensions regarding reuse of data collected for a different purpose were deliberated. 35 The secondary analysis was not contradictory with regard to the primary aim of the study, as it provided a supplementary view on essential elements regarding the use of the OET.
Findings
The participants expressed responsibility through different actions, which were revealed in two main themes, each unfolded in sub-themes: (1) to act responsibly as a patient or caregiver was to ‘be watchful and alert’, ‘report symptoms the right way’ and ‘do crosschecking’ and (2) to deal with the burden of responsibility was to ‘feel safe when dealing with the burden of responsibility’ and ‘be relieved from the burden of responsibility’.
To act responsibly as a patient or caregiver
It seemed essential for the patients and caregivers to take, or share, responsibility for (self-) observations, (self-) assessments and decision-making alone or in cooperation with HCPs. Responsibility showed up when the patients and caregivers were alert to and observant of changes in the physical condition. Furthermore, it appeared when they endeavoured to report symptoms sufficiently to ensure that the HCPs understood the nature hereof and when they crosschecked that the medicine and treatment administered was the right one.
To be observant and alert
To act responsibly and to take care of oneself or one’s relative meant that the patients and caregivers had to be observant and alert day and night. This required balancing between symptoms of the disease or side effects from treatment and knowing when and how to act. One patient remained watchful at night, as she felt responsible for monitoring her own condition before calling the OET. She had called the OET in the afternoon because she was worried about infection signs relating to her central intravenous catheter. At the time, the HCP believed that a red area on her skin had been caused by a plaster. Afterwards, the participant told us, Every time I woke up at night to go to the toilet, I assessed my general condition. Am I dizzy when I get up from bed, do I feel warm, and do I have to take my temperature? (Informant 2)
Being watchful and alert helped the patient complete her chemotherapy as prescribed. This participant had experience with home-based chemotherapy and discovered late in the evening that the infusion of chemotherapy had not been opened. Calling the OET, she corrected the error together with a HCP. She said, I turned on the infusion…I could do it myself without difficulty. (Informant 6)
Reporting symptoms
Reporting symptoms sufficiently and in an understandable way became a central issue that placed responsibility on both patients and caregivers. In some cases, the callers prepared themselves before calling the OET, reflecting on how they should report the incidence in question, because, as one participant said, The nurse was not right beside me […]. She can only react on the basis of what I tell her, so she depends on what I tell her and sees things as they are. (Informant 2) I think it would have been better if they had seen the rash, because before the next treatment it had disappeared. They offered me a consultation, but I declined, so in this case it was my own fault. If it happens again, I will go. I should have been there, so they could have taken a photo of the rash as a basis for further decision-making. (Informant 9)
Crosschecking
To act responsibly included a final sub-theme: crosschecking. In addition to monitoring symptoms, patients and caregivers performed a kind of crosschecking. Crosschecking was a way of taking responsibility by confirming one’s own presumptions, ensuring prescriptions and assessing whether or not the doctor who made the recommendations was reliable. This was qualified by experiences from previous treatment, prescriptions and healthcare support.
The need to have one’s presumptions confirmed was strong in the case where a patient contacted the OET following an incidence of haemoptysis. She wanted to be certain and said, I was not in panic, but wanted to be sure that nothing was very wrong. After consulting with a doctor, she (the nurse) called back. I should calm down. The blood sputum would disappear in three days. If not, she urged me to call again. Then I asked ‘what doctor’ she had talked to, because I do not trust all of them…but this one was okay, and then I calmed down. (Informant 3) I thought it was strange what one doctor told us about the medication. Afterwards we did as we used to, and the next day I called and talked to a different doctor. They could not recall what the first one had written in the record. This was odd. Then I wondered whether they thought I had done something wrong or was lying. (Informant 11)
To deal with the burden of responsibility
To successfully deal with the burden of responsibility seems to require balancing between the capacity to be able to perform (self-) care and recognise one’s own limits of knowledge and the capacity to act. In the interviews, the patients and their caregivers demonstrated an awareness of not transcending this balance. To deal with the burden and to feel safe, they sometimes needed to share their responsibility with the HCPs. In other situations, they reached their limit and needed to be relieved from the burden of responsibility.
Feel safe when dealing with the burden of responsibility by sharing
Confidence in one’s own ability to observe and assess symptoms or make the decision to contact the OET for help made the participants feel safe. With these options available to them, the participants remained calm and had the courage to wait and see in which direction the health condition would develop. Trusting oneself could also help prevent incidents. A caregiver who worked as a nurse’s assistant shared her observation of an infection in the urinary tract with an HCP in order not to risk delayed treatment. She said, When my dad gets an infection, he needs treatment right away; if not, he may not get his cancer treatment in time. It has been a struggle against the time. This is why I have called the OET. It was the most secure. (Informant 12) Last time I called the OET, was because my blood magnesium was too low and I had been given some new medication. During the night I got diarrhoea…I was not prepared…but my husband had heard that this could be a side effect and when I called them, they told me the same thing. (Informant 5) I was feeling unsure…first of all I worried for you (the husband). Next, I worried: Is this problem of a minor concern? Okay, but he did not eat for six days nor did he have any elimination for six days. This was definitely wrong. (Informant 10)
Handing over the responsibility to be relieved from the burden
Some patients and caregivers were challenged extensively with anxiety, uncertainty, doubt and specific or general concerns. When they found the situation unmanageable and acknowledged lack of knowledge and capacity to act, they needed to hand over the responsibility to the HCPs as illustrated in this quote: My husband was very ill and I called and asked them what to do. Then I was guided…‘You tell your husband this and that’. He was so sick, and I was afraid to drive. They said: ‘We will call for an ambulance’. They did not ask a lot of questions, they just said come in…That works. (Informant 12) When my wife is feeling well, she usually is very active. She acts like a person suffering from ADHD (Attention Deficit Hyperactivity Disorder), moving around from here to there. When I see her just sitting in the chair, sleeping all the time, falling apart, then I realize something is very wrong. Then I call the oncology department and ask ‘WHAT SHOULD WE DO? (Informant 1)
Although the burden of responsibility may be eased by the nurse, when he or she examines/asks questions about fever, nutrition, weight and so on, during the consultation, acknowledging the patients’ or caregivers’ worries and inviting them to attend the OET, further relieves them of their responsibility. Calling the OET when the patient’s condition became life threatening and subsequently going to the hospital could relieve some of the burdens of responsibility on relatives when the patient’s temperature substantially surpassed the limits of infection risk, as expressed by this informant: His temperature was higher than 40oC. I did not like this condition because we need to call the OET as soon as the temperature exceeds 38.5. I think they could hear how nervous I was. (Informant 11)
Discussion
The expectation of being responsible for caring for oneself or one’s sick relative in a healthcare system with increasing outpatient treatment has been investigated in other scientific studies. 12,15,36 The aim of this secondary analysis, however, was to explore the meaning of responsibility as it appeared in calls to an OET. We found that both patients and their relatives expressed their responsibility through actions, which fell within the main themes ‘To act responsibly as a patient or IC’ and ‘To deal with the burden of responsibility’.
To act responsibly as a patient or caregiver
The aim of knowledge exchange and partnerships between patients/caregivers and HCPs is to monitor the patients’ treatment and safety 4,11 as well as to keep them safe from life-threatening side effects. 3,4 The aim is to also support decision-making and feelings of being in control. 7 The participants in our study tried to maintain control by being watchful and alert day and night, and this required self-governance, self-care and self-management performed by competent autonomous persons. 26
McKenzie et al. 36 found that caregivers were watchful and alert, but felt they were given too much responsibility. This was especially true of novices or anyone who was ‘new’ to the supporting role. In addition, taking responsibility for oneself, one’s actions and one’s mistakes as an autonomous person 26 can make the person vulnerable to self-blame and guilt. 21,37 In their efforts to minimise adverse events, patients and caregivers in our study continuously observed and assessed the health condition of the patient. This suggests that they were afraid of overlooking serious signs and wanted to minimise the risk of self-blame and guilt. Consequently, too much responsibility and a potential imbalance between the callers’ knowledge and capacity to act and the HCPs’ expectations may place additional burdens on patients and caregivers. To relieve their potential suffering related to personal limitations such as inadequate knowledge associated to the situation, 23 it is essential that HCP explore whether patients or caregivers can be perceived as independent rational decision makers or as vulnerable and deteriorated persons. 27
We found that reporting symptoms could be challenging for patients and caregivers, who used a different terminology than HCPs to describe problems. Besides learning the language of cancer and chemotherapy, McKenzie et al. 36 have described the demands of detailed knowledge of medication and their side effects and knowing what to do or who to call in critical situations. In their study, reporting observations thus tended to demand advanced skills and knowledge at a ‘professional level’, including reporting in a specific professional language and consequently translating everyday language into medical vocabulary. These requirements underscore an additional risk of inducing self-blame and fear of not having accessed and reported the symptoms appropriately, as shown in our study. Furthermore, calling the OET could be a means to cover fundamental needs and to balance between dependence and independence, essential for well-being, safety and recovery. 38 As such, it seems urgent to identify the latent gap between expected competences and actual competences, which the participants tried to bridge when asking HCPs for help via the OET.
Although the participants needed advice, they also displayed self-confidence and competencies when they were able to connect former experiences with the present situation. Our study showed awareness of regulating the discomforting or deleterious effects of medical care when participants took responsibility and demonstrated courage by validating, for example, prescriptions and recommendations through crosschecking. Thus, the callers in our study demonstrated the ability to understand and use healthcare information to make appropriate decisions – a degree of health literacy that is presented as an important predictor of successful self-management and autonomous actions. 1 However, the ability to take responsibility as an ‘independent decision-maker’ 27 may be limited regardless of being patient or caregiver due to the association between patients’ symptoms and caregiver burden. 4,16,18,19 Interfering each other in their interdependent relationship may thus be a restraint in the caregiving process that needs acknowledgement from HCPs. Moreover, the notion of relational autonomy 23 requires HCPs to be attentive on the risk for caregivers to exceed their strengths in their obligation for the sick patient.
To deal with the burden of responsibility
The theme ‘To deal with the burden of responsibility’ revealed important knowledge about prerequisites for performing self-care. Performing self-care requires self-management, which is an individual’s ability to manage symptoms and consequences of living with a chronic condition. 39 Perceiving cancer as a chronic condition, 40 self-management involves long-term challenges and demands power and a surplus of resources, which may be difficult to find in an acute distressing situation. We found that dealing with the burden of responsibility stressed the need for patients and caregivers to balance between performing (self-) care safely and acknowledging the limits of one’s own capacity to act and dependence on healthcare support. In addition, perceived as autonomous persons, patients and caregivers risk being held accountable and blamed for inappropriate actions and exposed to demands of self-management that may appear unmanageable. 21,37
A person-centred perspective may ease the burden on patients and ICs, as it would involve listening to their personal accounts of the illness, symptoms and impact on everyday life. This includes sharing information, deliberations and decision-making. 9,41 When patients or caregivers in our study needed confirmation, advice or attendance, they called the OET to share their responsibility with an HCP and to feel safe in further decision-making. In other situations, patients or caregivers wanted to hand over the responsibility to the HCP. Thus, they moved from shared decision-making to welcomed paternalism. 26 In these cases, the callers’ capacity to act autonomously seemed to be limited.
Failure to understand the connection between treatments and subsequent side effects is reported to increase anxiety, insecurity and loss of control. 42 Welcomed paternalism – handing over the responsibility to HCPs – can therefore be a sign of side effects and symptoms exceeding the participants’ understanding and competences. McKenzie et al. have reported that caregivers developed from frightened novices characterised by fear, uncertainty, apprehension and lack of knowledge to reassuring experts during the cancer trajectory. Although they had difficulties reaching the expert level in general, the participants in their study felt confident in their subtle observation of the person they were caring for and about. 36 Besides showing signs of being a novice when the health conditions became unmanageable, participants in our study demonstrated clinical skills and medical knowledge that belong to a higher level of competence; in some cases, they showed an intuitive grasp of the situation that belongs at the expert level. 43 However, as stated by a caregiver who saw his wife fall apart, this intuitive grasp was directed towards deviations in the patient’s condition and not towards ensuring sufficient nutrition himself. Thus, expecting the patients and caregivers to act as experts may be restricted, although they may be experts in sensing psychological and physical changes in their own or the sick person’s condition.
In our study, caregivers played an important role as a preliminary source of support for patients in their efforts to manage their illness. To enhance caregivers’ coping opportunities, Hazelwood et al. 44 suggest a problem-solving approach, involving the ability to define problems, identify their need for professional help and possible barriers to their caregiving focus, implementing and adjusting care plans. However, both patients and caregivers may suffer from psychological and emotional constraints and be unable to understand the information given. 4,16,18,19 In this case, we must consider whether a problem-solving approach would increase their capacity to act or whether it would place an additional burden on the patients and caregivers, as requirements concerning self-care and self-management may demand strength and a surplus of resources. Even though Hazelwood et al. 44 have found that caregivers became more confident in their own capacity to act, the training did not affect the patients’ well-being and physical symptoms. Therefore, this intervention was unable to provide patients with care and comfort, which is one of the main goals in nursing. 24,25 Although the problem-solving approach involved the caregivers, it seemed that the request for involving the patient in person-centred care and shared decision-making was lacking. According to our findings, caring for vulnerable patients or caregivers and balancing requirements in nursing ethics, HCPs had to find a way to respect patients’ and caregivers’ autonomy. However, not to overlook the burden of responsibility, it requires balancing shared autonomy and welcomed paternalism and taking into consideration the option of relational autonomy.
Conclusion
Patients and caregivers calling the OET painted a complex picture of the meaning of responsibility, evident from the participants’ capacity to act. Their actions displayed responsibility to observe, assess and report symptoms and to control prescribed treatments as well as to share or hand over responsibility to an HCP. Thus, the analysis provides HCPs with essential knowledge of how patients and caregivers handle responsibility in their everyday life with cancer, treated on an outpatient basis. On the basis on the Fundamentals of Care’s framework, 38 HCPs may help patients and caregivers to manage this responsibility without making them feel responsible for problems over which they have no control.
Adopting a person-centred approach to these callers – in accordance with the values of the nursing profession – may support the balance between dependence and independence and autonomy and welcomed paternalism. From this stance, the HCP must acknowledge that even though the callers may be experts in their own lives, they may be novices when it comes to self-care in a vulnerable situation. This contributes to establishing and maintaining a trustful relationship through which it is possible to determine what patients and caregivers can do on their own and when they need further support.
Our study may have some limitations. Using data from a previous study to conduct a secondary analysis on the meaning of responsibility may be at methodological challenge. Data collected with the aim to cover a different topic requires the data interpretation to be executed with caution not to exceed the latent meaning expressed by the participants but revealed by the researchers. However, the iterative process and the request for consensus contributed to being faithful to the data, with a low level of interpretation and abstraction. Still, the findings and subsequent discussion point at what might be at stake regarding responsibility experienced by patients and caregivers, which can be transferred into similar contexts.
We did not distinguish between patients and caregivers, which also may be a limitation. The increasing number of cancer patients who receive treatment on an outpatient basis implies that we need to focus attention on patients’ responsibility regarding self-management and health literacy in a primary study, as not all patients have caregivers who are able to support them during their illness. Furthermore, taking into consideration the association between patients and caregivers suffering and the underlying reason for caretaking among caregivers, the meaning of responsibility related to caregiver burden may be a topic for further investigations.
Patients have a legal and ethical right to be involved in their own care, 6,7 a right that contains a responsibility as well as a duty to perform self-care. Increasingly, caregivers are expected to provide cancer-related care in the healthcare system. How this responsibility and duty are fulfilled in an interplay between autonomy and welcomed paternalism may be influenced by many factors that require further exploration.
Footnotes
Acknowledgements
The authors would like to thank the participants for their valuable contribution, providing knowledge of their experiences of calling the oncological emergency telephone.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.