
Abstract
Background:
Informed consent can be obtained by various methods, by various people, and with use of various types of consent forms. Persistent effort is necessary to reveal the practical realities of informed consent to improve ethical and legal standards.
Objective:
To determine the ethical challenges of obtaining informed consent from surgical patients.
Methods:
The present study was a descriptive cross-sectional study using two researcher-made questionnaires and a checklist for data collection. Data were collected from nursing personnel (n = 95) and surgical patients (n = 203) on the surgical wards of three university hospitals in Isfahan, Iran. Data were analyzed using descriptive statistics, Spearman’s rank correlation, Pearson’s correlation coefficient, and the t-test.
Ethical considerations:
The study was approved by the Ethics Committee of Isfahan University of Medical Sciences (No: 396478).
Results:
The mean scores (maximum 100) of awareness, competency, and authority were 36.3, 67.7, and 57.6, respectively. The overall quality of the informed consent was poor (score 53.9 of 100). The higher educational level in patients was correlated with lower awareness of and less authority to give informed consent. Only 12.6% of the nurses stated that patients were given sufficient information to assure informed consent. In 89.2% of the consent forms, the risks of the treatment were mentioned. However, alternative methods and risks and advantages of rejecting the treatment were not mentioned in any of the forms.
Conclusion:
Ethical challenges to obtaining informed consent include patients’ poor awareness of their rights, a failure to provide adequate information to patients, absence of consideration of patients’ educational level, an unclear definition of who is responsible for obtaining informed consent from the patients, time constraints, and use of unclear language and medical jargon. Constructing an ethical framework may guide nursing staff in dealing with the ethical challenges involved in obtaining informed consent.
Introduction
Medical ethics is a set of acceptable rituals and behaviors that should be honored by everyone in the field of medicine. One of the most important issues in the field of medical ethics is obtaining informed consent. 1 Informed consent is a voluntarily, revocable acceptance of an eligible individual’s participation in medical decision-making after receiving information about nature, goals, and consequences of a proposed treatment or procedure. 2,3 Providing adequate information to a competent patient and emphasizing that the consent is voluntary are important prerequisites in the process of obtaining informed consent. 4 –6 Competency in decision-making is a concept that links autonomy and informed consent. 7 Voluntary decision-making is a patient’s right to freely choose medical care without any external influences.5 According to the independence or autonomy principle, the patients should be aware of what is best for them and have the right to decide for themselves. 8 Hence, the signature on the consent form must reflect a patient’s understanding of the medical choices, based on appropriate communication and the provision of sufficient information. 8,9
In Iran, a surgeon is responsible for obtaining informed consent from a patient before surgery. However, due to the heavy workload in university hospitals, other hospital staff also obtain informed consent, which may impair the quality of the obtained informed consent. Thus, there is need of a unified structure for obtaining informed consent. Moreover, sometimes consent is obtained from a person on behalf of a patient who cannot legally give consent. 10 The content of existing consent forms is confusing for the patients, and they are often anxious about making decisions that can have serious consequences for their health status. 10 –12 The ethical and legal standards of obtaining an informed consent need to be fully investigated in Iran. 10
Ethical challenges in surgical patients include obtaining an adequate informed consent from a patient, working with family members, and responding to requests from patients or family members regarding surgical interventions. 11 The communication of medical information to patients can also be challenging because of the need to explain medical interventions in plain language. 4 Due to the complexity of these challenges and their potential to result in conflict, 11 it is important for nurses to be aware of these ethical challenges and to develop their ethical decision-making skills to better tackle these challenges. 13 In this regard, it is imperative that nurses have a detailed understanding of the ethical challenges and are able to use strategies to meet them. 14 Correct ethical decisions by nurses may improve the patient’s recovery and the quality of healthcare services, and reduce healthcare costs. 13
A review of the studies on ethical challenges in surgical patients revealed widespread inconsistency and the many ethical issues involved in obtaining informed consent. Joolaee et al. 10 indicated that 48% of surgical patients who had signed a consent form had not even read it before signing. Among the patients who had read the consent form, 99.2% reported ambiguity in the technical, medical, and legal vocabulary. Only 12%–18% were satisfied with the consent form and had no fear and anxiety at the time of signing. Abolfotouh and Adlan 15 showed that most of the patients did not know their rights and that paternalism was common in hospitals. The quality of informed consent was poor, and two-thirds of the patients believed that they were forced to sign the consent form. Forty-eight percent of patients thought that if they refused the treatment plan, they would no longer be able to receive treatment.
Vučemilo and Borovečki 16 showed that the readability of informed consent forms was not appropriate for the general population. A systematic review study on surgical patients’ understanding of informed consent by Falagas et al. 4 indicated that only 29% of the patients had an adequate understanding of the information provided and of the risks related to surgery. Patients in 58% of the studies involving surgery and 80% involving clinical research were satisfied with the amount of information given.
These studies show that the quality of the obtained consent before surgery is not adequate and acceptable, and that the necessary information and awareness of risks are not communicated to many patients. In addition, ethical challenges regarding surgical patients varied from one clinical setting to another because of different structures of the consent forms, different types of surgical interventions, and different people being responsible for obtaining consent. Hence, ongoing persistent efforts to reveal the practical realities of informed consent are essential 1 to improve ethical and legal standards to promote nursing practice and research. In this regard, the present study was conducted to determine the ethical challenges for obtaining informed consent in surgical patients from the viewpoint of the surgical patients and nurses working in the surgical wards.
Methods
Design, setting, and participants
This study was a descriptive cross-sectional study conducted from May to June 2017. Participants consisted of surgical patients and nursing staff in the general surgery and orthopedic departments of three university hospitals affiliated with the Isfahan University of Medical Sciences, Isfahan, Iran. The inclusion criteria for patients were willingness to participate in the study, being at least 18 years old, being in a period of 1-7 days after surgery, being able to verbally answer the questions, and having a clinical condition with a level of pain and consciousness that did not prevent participation in the study. The inclusion criteria for nurses were willingness to participate in the study and having at least a bachelor’s degree in nursing.
The sample size for the patients was calculated to be 215 using the N = z2s2 / d2 formula and considering a 10% rate for sample loss. Samples were selected using non-randomized quota sampling (44%, 29%, and 27% of the sample size) method based on the number of the beds in the hospitals studied. All nurses (n = 104) met the inclusion criteria and were selected for participation in the study.
Instruments and data collection
Two questionnaires and a checklist were developed by the researchers based on a review of the literature 1,3,4,8,11,12,17 –26 and experts’ opinions on obtaining adequately qualified informed consent in surgical patients. After consulting the relevant literature, a primordial version of the instruments was developed and presented to 10 experts in medical ethics from the schools of nursing and midwifery and medicine for advice regarding the content validity of the instruments. Some semantic ambiguities and linguistic errors were revealed, and more appropriate words were identified, the questionnaires and checklist were revised accordingly. The internal reliability of the final version of the instruments was measured using Cronbach’s alpha. The results of the Cronbach’s alpha in the pilot study with a sample of 10 nurses, 10 patients, and 10 informed consent forms showed acceptable reliability: 0.88 for the questionnaire for evaluating the quality of obtained informed consent, 0.78 for the nurses’ attitude questionnaire, and 0.82 for the evaluation of the content of informed consent forms’ checklist.
The first questionnaire was designed to evaluate the quality of obtained informed consent in surgical patients and had two parts. The first part contained seven questions regarding demographic characteristics, including gender, age, educational level, priority of surgery, history of surgery, the place where the informed consent was obtained, and the person who obtained the informed consent. The second part consisted of 36 questions assessing the quality of the obtained informed consent in three dimensions of awareness (20 questions), competency (8 questions), and authority (8 questions). Awareness refers to adequate disclosure of the information to the patient with regard to understanding the nature and purpose of the treatment, its risks, potential benefits, and available alternatives. It also requires that the patient comprehend the information given and understand its relevance to his or her condition. Competency refers to the patient’s legal standing and ability to make healthcare decisions. Authority refers to the patient’s voluntary decision-making and the patient being free from inappropriate pressures or unfair persuasions from individuals or institutions. 3,26 This questionnaire was scored based on a 3-point Likert-type scale from 0 to 2, where no = 0, to some extent = 1, and yes = 2. Some of the questions (21, 22, 24, 25, 28, and 29) were scored from 2 to 0 due to their negative or reverse content. The total score of the questionnaire was equal to the sum of the scores of all the questions and the final score was calculated based on a maximum score of 100. The higher the score, the better the quality of obtained informed consent.
The checklist was designed to evaluate the content of the informed consent forms and consisted of 12 questions, indicating whether the following were mentioned in the forms: name of the hospital, patient, the risks of the treatment, alternative methods, risks, and benefits of the alternative methods and risks, and advantages of rejecting the treatment. The items in the checklist were answered with yes or no by the researcher (S.M.) based on the patient’s medical file, where yes = 1 and no = 0, and the total score was calculated out of 100 as a percentage. The higher the score, the better the standard of the content of informed consent form.
The second questionnaire was designed to evaluate the nurses’ attitudes toward obtaining informed consent and had two parts. The first part contained demographic characteristics (gender, age, educational level, work experience, place of work, and type of employment). The second part evaluated the nurses’ attitude through 20 questions in five dimensions (competency for obtaining the informed consent, competency for giving informed consent, right time for obtaining informed consent, making sure of understanding the provided information by the patient, and providing information about the alternative therapeutic methods). This questionnaire was answered with yes or no, where yes = 1 and no = 0. The questionnaire was scored from 0 to 20, and the frequency of yes answers to each item was determined.
To collect patient data, the first author, S.M., came to the general surgery and orthopedic departments every day at the beginning of the morning and evening shifts, and after introducing herself and providing an explanation of the goals of the study and obtaining informed consent from the patients who met the inclusion criteria, the quality of obtained informed consent’s questionnaires were given to the patients. The questionnaires were self-completed by patients or researcher-assisted self-completed. That is, if the patients could not read or write, the questions were read to them by the researcher and their responses were recorded. The completed questionnaires were collected by the researcher during the same shift.
Using the checklist, the researcher evaluated the quality of the content of the consent forms, in the medical files of the patients who completed the quality of obtained informed consent questionnaire.
To collect nurse data, after providing an explanation of the goals of the study and obtaining informed consent from the nurses, the second self-reported questionnaire on nurses’ attitudes toward obtaining informed consent was handed out by the researcher at the beginning of the morning and evening shifts and collected at the end of the shifts.
Ethical considerations
This study was approved by the Ethics Committee of Isfahan University of Medical Sciences (No: 396478). The required permissions were obtained from the hospital and ward adminstrators. All patients/nurses were informed about the aim of the study and were assured that their participation was voluntary. A written informed consent was obtained from all study participants. In addition, all the participants were assured about the confidentiality of their personal data.
Data analysis
All analyses were performed using the IBM SPSS Statistics (version 18). For all statistical analyses, the significance level was p < 0.05. Descriptive statistics (frequency, mean, standard deviation), Spearman’s rank correlation coefficient, Pearson’s correlation coefficient, and the t-test were used for data analysis.
Results
In the patient group, the response rate for the 215 distributed questionnaires was 94.4% (n = 203). The mean age of the patients was 39.8 ± 16.9, range 18–94 years, and 53.2% (n = 108) of them were female. Among patients, 52.2% (n = 106) had an elementary school education and 47.8% (n = 97) had a high school education or higher levels. Among those responsible for obtaining consent, 61.6% (n = 125) were physicians, 13.7% (n = 28) were nurses, 1.5% (n = 3) were receptionists, and 1% (n = 2) were ward secretaries. In 22.2% (n = 45) of the cases, patients were not aware of the position of the person to whom they gave consent. The mean scores of awareness, competency, and authority were 36.3, 67.7, and 57.6 out of 100, respectively. The overall quality of the obtained informed consent was 53.9 out of 100 (Table 1).
Mean scoresa of awareness, competency, authority, and overall quality of obtained informed consent in surgical patients (n = 203).

aMaximum score = 100.
Spearman’s rank correlation coefficient between the three dimensions of the quality of obtained informed consent in surgical patients and their educational levels showed a significant reverse correlation between the score of awareness (r = −0.169, p = 0.02) and authority (r = −0.156, p = 0.03). Thus, patients with a higher educational level indicated that they had a lower awareness of and less authority to give informed surgical consent. No significant relation was observed between the score of the competency and the educational level of the patients (r = −0.112, p = 0.11). Pearson’s correlation coefficient between the three dimensions of the quality of obtained informed consent in surgical patients and their ages showed a significant positive correlation between the score of awareness (r = 0.182, p = 0.009) and a significant reverse correlation between the score of the competency (r = −0.161, p = 0.02). That is, older patients indicated that they had a higher awareness and less competency to give informed surgical consent. No significant relation was observed between the score for the authority and the patient age (r = 0.109, p = 0.12). Furthermore, there was no significant difference between the mean scores for awareness (t = 0.65, p = 0.52), competency (t = 0.67, p = 0.50), and authority (t = 0.08, p = 0.94) in male and female surgical patients.
In the nurse group, the response rate to the 104 distributed questionnaires was 91.3% (n = 95). The mean age of the nurses was 34.1 ± 7.2, range 22–49 years, and the mean working experience was 10 ± 7.1 years. Among the nurses, 72.6% (n = 69) were female, 88.4% (n = 84) had a bachelor’s degree, 11.6% (n = 11) had a master’s or PhD degree, 68.4% (n = 65) were working on a general surgery ward, and 31.6% (n = 30) were working on an orthopedic surgery ward.
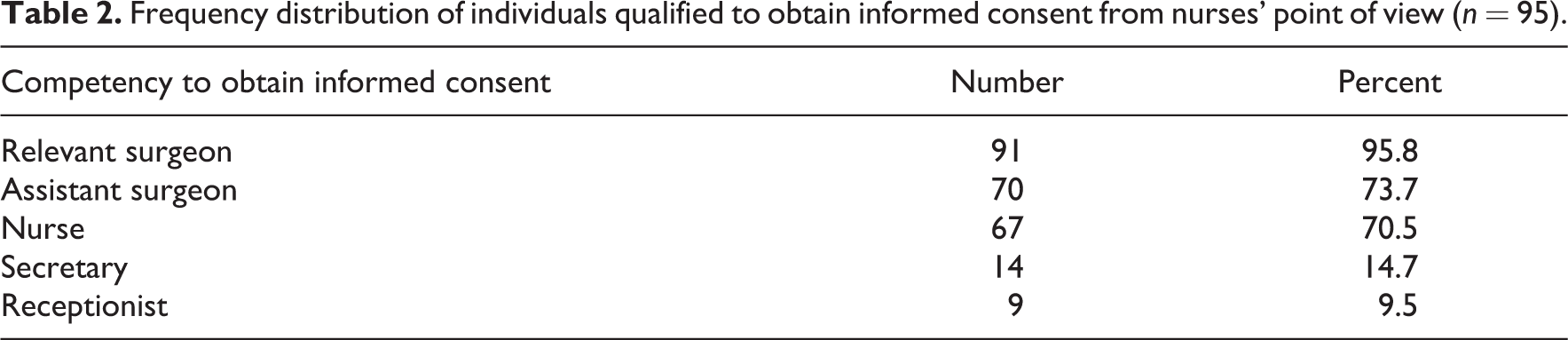
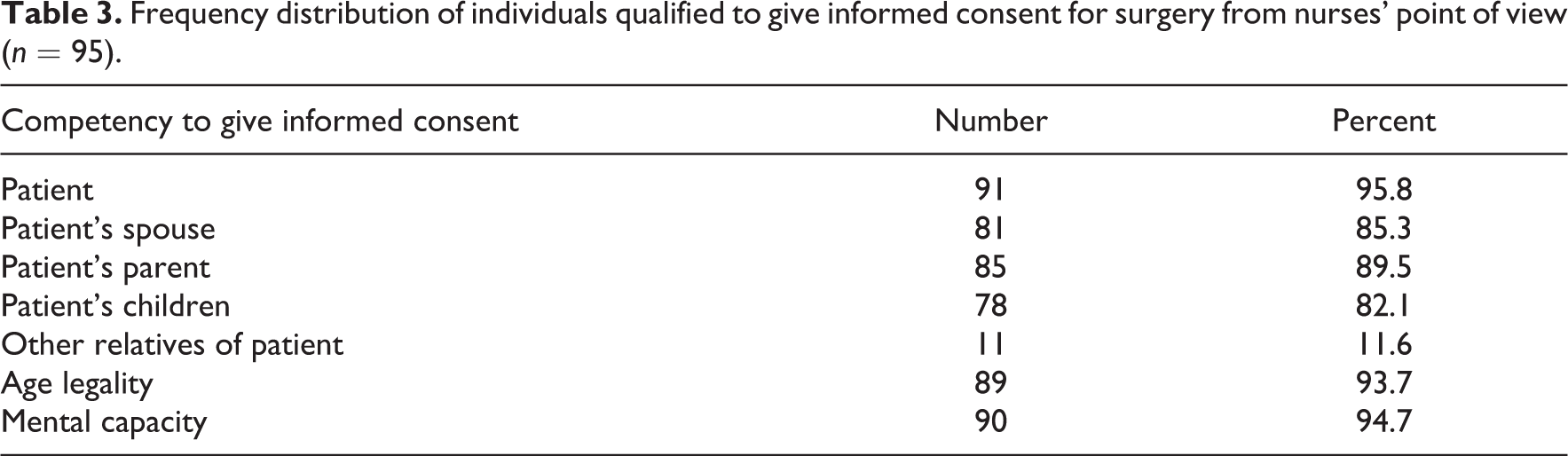
The majority of the nurses (95.8%) reported that the relevant surgeon had the competency for obtaining informed consent from the patient (Table 2). The majority of the nurses (95.8%) reported that the patients themselves had the competency to give informed consent for the surgery. The others who were considered competent to give informed consent from nurses’ point of view were patient’s spouse (85.3%), patient’s parents (89.5%), patient’s children (82.1%), and patient’s other relatives (11.6%). Furthermore, 93.7% of the nurses considered age and 94.7% considered mental capacity as a criterion for giving informed consent (Table 3).
Frequency distribution of individuals qualified to obtain informed consent from nurses’ point of view (n = 95).
Frequency distribution of individuals qualified to give informed consent for surgery from nurses’ point of view (n = 95).
Most of the nurses (69.5%) reported that the night before surgery was the right time to obtain informed consent. While 37.9% of them reported the day of admission and 32.6% reported the time right before the surgery as the right time to obtain informed consent. Most of the nurses (92.6%) considered receiving feedback from the patients, and 87.4% repeated the provided information for the patient as a way to assure that the information about the informed consent was understood correctly by the patients. Most of the nurses (88.4%) stated that the alternative treatment methods available at the center should also be explained to the patients. Only 12.6% of the nurses stated that the information given to the patients was satisfactory.
Results of evaluating the existing consent forms in the medical files of the patients showed that the name of the hospital was mentioned in 100% of the forms. In 93.1% of the forms, the name of the patient or their legal guardian, and in 89.2% of the forms the risks of the treatment or procedure were mentioned. Alternative methods (regardless of their costs or coverage by an insurance company), risks and benefits of the alternative methods, and risks and advantages of rejecting the treatment or procedures were not mentioned in any of the forms.
Discussion
The present study was conducted to determine the ethical challenges involved in obtaining informed consent in surgical patients from the viewpoints of patients and nurses. In the present study, the overall quality of the informed consent was poor (53.9 out of 100). In line with our results, Joolaee et al. 10 reported a poor quality of obtained surgical informed consent (17.1 out of 35). Abolfotouh and Adlan 15 also reported the poor quality of informed consent for invasive procedures (51%). The poorest quality of obtained informed consent in our study was in the domain of awareness. Similarly, Falagas et al. 4 reported that nearly two-thirds of the surgical patients had an insufficient understanding of the information provided and of the risks associated with the surgery. Cawich et al. 12 also reported that nearly half of the patients were unaware of the training status of the physician who obtained their informed consent. Chima 19 reported that the majority of physicians provided information on diagnosis (96.4%), the benefits of treatment (89.3%), treatment options (81%), and recommendations regarding a specific treatment (88.7%). An unproved justification about providing insufficient information is that patients may become anxious when an excessive amount of information is volunteered. 12
Patients’ rights charters and ethical codes state that patients have the right to receive appropriate information; otherwise, the consent should not be considered valid and informed. Accordingly, provision of insufficient and inaccurate information to the patient would be considered a breach of contract and consequently, the patient could file a lawsuit for any incurred damage. 12 However, there is no consensus on how much information is considered as sufficient. 25 Moreover, there are no clear guidelines on how to provide sufficient relevant and updated information to patients that would ensure an informed decision. 12
In the present study, two-thirds of the patients had the necessary competency, and more than a half of them stated that they had the authority to give informed consent. In line with our results, Abolfotouh and Adlan 15 reported that two-thirds of the patients had been given enough time to study the consent forms and ask questions, and half of the patients stated that their decision was not important with regard to the surgery and that it was the physician who had the responsibility to decide for them. Another study also reported that the risks and benefits of the alternative treatments were not explained to nearly half of the patients and that they did not have the chance to choose other treatment methods. In general, the quality of the voluntary dimension of giving consent was poor. 4
In this study, nearly one-third of the nurses stated that only the available surgical procedures in the hospital should be explained to the patient, which is in contrast with patients’ rights charters and professional ethics principles, while 88.4% of the nurses stated that the alternative treatment methods at other medical centers should also be explained to the patients. Moral performance and decision-making of the nurses can be affected by personal values, and economic, cultural, and environmental conditions. 2,27 For instance, the personal culture or even the organizational culture can hinder nurses from presenting the alternative treatment methods in the hospital. 1 Further attention should be paid to enhancing patients’ understanding regarding the authority to give informed consent for surgery, particularly in clinical settings, such as Iran, in which patients have diverse cultures and beliefs.
In the present study, a reverse correlation was observed between patients’ educational levels and the score of awareness and authority of the patients in the process of obtaining informed consent. That is, patients with higher educational levels believed that their awareness of and authority to give informed consent were insufficient. The higher the educational level of the patient, the more they would be willing to receive information, and provision of more information would bring more authority. Information to the patients should be based on their educational levels, and presenting the same information to all the patients is not appropriate.
In the present study, most of the nurses believed that the chief surgeon or the assistant surgeon was the competent person for obtaining informed consent and others had lower priorities. In Iran, nurses often obtained informed consent from the patients; however, it had to be approved by the surgeon in charge of the surgery. Although there is no legal prohibition against hospital personnel other than the surgeon obtaining informed consent, the necessary information may not be adequately communicated to the patient, and in any case, the final responsibility would rest on the surgeon responsible for the surgery. 11 Some surgeons avoid providing detailed information to the patients and state that it would make them anxious and disturb their decision-making process if they did. 12 It is the responsibility of the surgeon to spend sufficient time to obtain informed consent and provide patients with appropriate and sufficient information in such a way that it can provide the basis for them to make the correct decision. However, healthcare professionals do not always have an adequate understanding of the importance of informed consent. 21 Therefore, retraining sessions and continuing education regarding medical ethics and law might be considered appropriate undertakings among hospital personnel.
In the present study, the name of the hospital was mentioned in all the forms and none of the forms contained alternative treatment methods and their risks and benefits. In 89.2% of the cases, the risks of the intended procedure and only in 3.2% of the cases, the advantages of the procedure were mentioned. In nearly one-third of the cases, the content of the consent was understandable and clear and non-Latin and medical terms were used. Similarly, Joolaee et al. 10 reported that nearly two-thirds of surgical patients stated that the content of the consent form was unclear, and 94.2% stated that the technical, medical, and legal wording was difficult to understand. Rajesh et al. 20 also reported that in only one-third of the cases was the content of the consent understandable. A systematic review study on patients’ understanding of the informed consent process for surgery showed the overall understanding of the information provided in the consent forms was 29%, and in only one-third of the informed consent were the risks associated with the surgery mentioned. Based on the principles of professional ethics, appropriate and sufficient information about all the aspects of the intended procedure should be given to the patient so that the patient is consciously able to make the decision. However, when applying this principle, it appears that its legal aspect has received more consideration than its ethical aspect, and instead of obtaining informed consent from the patient, the main concern has been to exculpate the hospital and medical personnel. Therefore, there is a need to improve patients’ understanding of the informed consent for surgery as well as reevaluate the contents of existing consent forms.
Study limitations
This study has limitations because the sample size was small and it was conducted in university hospitals over a 2-month period. Future studies in private or other public hospitals may provide different results. Thus, the results of our study should be generalized with caution to other types of hospitals and clinical settings. Future studies with a larger sample size and longitudinal design may better address the ethical challenges and increase the generalizability of the results.
Conclusion
Results of the present study showed that the quality of the informed consent forms in patients undergoing surgery was poor. Ethical challenges with regard to obtaining informed consent include patients’ poor awareness of their rights, a failure to provide adequate information to patients, lack of clear guidelines on how to provide sufficient information to patients, absence of consideration of patients’ educational level, lack of clear designation of who is responsible for obtaining informed consent from the patients, time constraints, and use of unclear language and medical jargon. Based on our results, the current informed consent forms and processes of obtaining informed consent in the three surgical departments require reevaluation and improvement to adequately meet ethical and legal standards. Constructing an ethical framework may guide nursing staff in dealing with the ethical challenges involved in obtaining informed consent. Nurses can help the patient through decision-making by appropriate participation in the process of obtaining informed consent and maintaining the independence and rights of the patients.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Research Deputy of Isfahan University of Medical Sciences (Grant no: 396478).