
Abstract
Introduction:
Ethical conflict is a phenomenon that has been under study over the last three decades, especially the types moral dilemma and moral distress in the field of nursing care. However, ethical problems and their idiosyncrasies need to be further explored.
Aim:
The objectives of this study were, first, to obtain a transcultural Portuguese-language adaptation and validation of the Ethical Conflict Nursing Questionnaire–Critical Care Version and, second, to analyse Portuguese critical care nurses’ level of exposure to ethical conflict and its characteristics.
Methods:
A cross-cultural validation and descriptive, prospective and correlational study. The sample was made for 184 critical care nurses in 2016.
Ethical Considerations:
The study was authorised by Bioethics Commission of the University of Barcelona, the Associaçâo de Apoio ao Serviço de Cuidados Intensivos do Centro Hospitalar do Porto and the Sociedade Portuguesa de Enfermagem de Saúde Mental.
Findings:
The Portuguese version of the Ethical Conflict Nursing Questionnaire–Critical Care Version was a valid and reliable instrument to measure exposure to conflict. Moral outrage was the most common type of conflict. The most problematic situations were the ineffectiveness of analgesic treatments, the administration of treatments considered futile and the mismanagement of resources.
Introduction
Ethical conflict and how it emerges is a phenomenon that has been under study over the last three decades, especially in the field of nursing care. Most studies on the subject focus on the causes and consequences of a range of moral dilemmas and moral distress in nursing professionals. A moral dilemma is a moral state that arises when a professional must choose between two or more a priori morally correct options for a patient, that is, between two opposing, disjunctive propositions. Moral distress, a term coined by the philosopher Andrew Jameton, 1 is the moral state in which professionals find themselves when they feel they cannot carry out what they consider to be morally correct due to external third-party limitations or constraints. Both types of conflict imply having the moral sensitivity to detect them. They both make it difficult to adopt decisions in clinical contexts, having an impact on decision-making 2 –5 and quality of care. 3,6,7
In the case of moral distress, some recent reviews 5,8,9 have found that despite hundreds of qualitative and quantitative works, the use of the term is somewhat diffuse and there seems to be no unanimous application of Jameton’s expanded definition. 10,11 This implies that the term’s operationalization presents insufficiencies, leading us to question whether it is moral distress that is being accurately measured, 3,5 –12 or rather only the intensity of ethical problems, attributable to other types of conflict.
In this vein, to adjust the moral distress type of conflict to its original definition, Falcó-Pegueroles et al. 12 operationalized a conceptual model in which different types of ethical conflicts, such as moral uncertainty, moral dilemma, moral distress and moral outrage, were explicitly defined, as well as states such as moral indifference and moral well-being. Moral uncertainty, as Jameton 1 defined, occurs when a person intuits an ethical conflict but is unable to identify the ethical principles involved. On the other hand, moral outrage was defined by Wilkinson 13 as a type of conflict in which the persona or professional experiences a sense of impotence in the face of an immoral action performed by others.
In the Falcó-Pegueroles 14 conceptual model, all types were ordered, from lower to higher levels of exposure to ethical conflict, a variable that takes both temporal frequency and the intensity of perceived ethical problems into account. Based on this conception of ethical conflict, she designed the Ethical Conflict Nursing Questionnaire–Critical Care Version (ECNQ-CCV), containing 19 situations that potentially generate ethical conflict. The instrument showed a Cronbach’s α reliability of 0.88 and 0.92 in samples of intensive care unit (ICU) nursing professionals in Spain 15 and Iran, 16 respectively.
Other instruments in the literature dedicated to measuring ethical problems are also worthy of note for their reliability and broad applicability to different samples, such as Corley’s Moral Distress Scale, 17 Kälvermark’s Moral Distress Questionnaire 18 and the Stress of Conscience Questionnaire. 19 All of them have adequate metric properties, with Cronbach’s α values ranging from 0.78 to 0.97 depending on the instrument and study. 20 –22 They aim at measuring the intensity of ethical conflict or ethical problems, although they deal with a single type of ethical conflict.
Situations of ethical conflict in ICUs
A number of studies on ethical conflicts raise awareness about the fact that they constitute a barrier to ethical decision-making. Most of these studies have focused until now on situations that generate moral distress in the context of ICUs because of critical patients’ special vulnerability and ICUs’ specific choice of therapeutic options. 2,5,23 –28
Experts agree that sources of ethical conflict include certain situations linked to patients and their families’ care, treatments, relationships with the team and institutional characteristics. Regarding patients and their families, informed consent management raises the ethical issue of preserving critical patients’ confidentiality and defending their rights and interests. 18,23,29 –32 Regarding treatments, decisions on whether to apply them or not are linked to life support treatment limitations and therapeutic futility. 23,30,32 –34 Some studies bring to our attention, however, that checking whether analgesic treatment is insufficient to control patient’s pain is a very conflictive and relatively frequent situation in ICUs. 2,29,30 Finally, several studies have shown that some conflicting situations emerge from relationships between professionals and team dynamics, from resource management or burnout. 2,18,24,28 –31,33 –38
A number of studies have described the particular case of Portuguese-speaking nursing professionals from Portugal and Brazil and the ethical problems they face. They highlight how care is exercised with limitations to autonomy and emphasize the need to apply strategies to address the moral distress this causes. 39 –42 In this regard, using Corley’s Moral Distress Scale, Barlem et al. 43 verified that levels of moral distress in the Brazilian nurses under study were greater in terms of frequency and intensity than those found in most previous studies. They also found that the most conflictive situations were those relating to team members’ inadequate technical competence, insufficient resources and lack of respect for patient autonomy in decision-making. Recently, in their literature review, Schaefer et al. 44 identified a total of 53 moral distress risk factors from quantitative, qualitative and theoretical studies. They warned of the growing need to address this type of ethical conflict going beyond institutional constraints and using new instruments in the Portuguese language. Thus, ethical problems and their idiosyncrasies need to be further explored, and all the more so given that works on ethical conflict in this cultural context and in the specific field of intensive care are still scarce. To this end, the ethical conflict exposure model of Falcó-Pegueroles et al. 12 was used because it is based on the ethical conflict typology. Thus, the ECNQ-CCV was adapted to Portuguese. The two research questions were as follows: ‘What are the reliability and factor structures of the ECNQ-CCV in Portuguese language?’ and ‘What are the levels of exposure to ethical conflict and what are the characteristics of Portuguese critical care nurses?’
The objectives of this study were, first, to obtain a transcultural Portuguese-language adaptation and validation of the ECNQ-CCV from the original Spanish version and, second, to analyse Portuguese critical care nurses’ level of exposure to ethical conflict and its characteristics.
Methods
Design
A two-phase methodological approach was adopted consisting of translation, adaptation and cross-cultural validation followed by a descriptive, prospective and correlational study.
Sample
The study sample was made up of 186 critical care nurses who attended one of the three Medicine and Intensive Nursing Congresses held in Portugal between October 2015 and April 2016. The sampling technique was non-probability convenience sampling. The inclusion criteria were as follows: to be a nurse, to have worked for a minimum of 1 year in the ICU and to have given their informed consent to participate in the study. The exclusion criteria were as follows: to be a master’s student or an intern in an ICU service, or to have previously answered the questionnaire.
The recommendations of Nunnally and Bernstein 45 were followed to calculate the sample size, which suggests including between 5 and 20 participants for each questionnaire item, with an agreed value of 10, representing an ideal sample of 190 subjects.
Procedure
There were two phases. The first phase consisted in translating and adapting the Spanish version to the Portuguese version. An independent committee of bilingual Portuguese–Spanish, Spanish–Portuguese experts was formed. The translation and back-translation process by the expert committee was carried out following the Standards for Educational and Psychological Testing. 46 The committee consisted of two professors of ethics with advanced level language and accreditation of Spanish and Portuguese, a nurse with a PhD experience in intensive care, three intensive medicine service professionals who were members of a Hospital Ethical Committee, a representative of the Portuguese Intensive Care Society, two nurses from the intensive medicine service and a relative of a patient admitted to the ICU. They began by performing an individual and then joint translation of the original questionnaire, the attached sociodemographic data form and the participant informed consent form. There was a consensus that the questionnaire items in Portuguese matched the original version. Nevertheless, the experts suggested modifying the item categories ‘type of schedule’ and ‘type of training’ in the attached sociodemographic data form to adapt it to Portugal’s cultural and professional context. Subsequently, the questionnaire and the form were administered to a pilot sample consisting of 10 ICU nursing professionals to detect difficulties and estimate completion time. No difficulties were reported. The completion time ranged between 15 to 20 min.
In a second phase, the psychometric properties of the ECNQ-CCV-Portuguese and the levels of exposure to ethical conflict were analysed. The questionnaire was administered to the sample of nursing professionals attending medical and intensive nursing conferences. At each of the three scientific events, the research team presented the study, answered any questions raised and distributed the questionnaires among the attendees who gave their consent to participate. Participants returned the completed questionnaire and the sociodemographic data form in a box dedicated to this purpose, and were guaranteed privacy with respect to third parties.
Data collection and variables
The ECNQ-CCV-Portuguese version was administered as well as an ad hoc form to collect sociodemographic data. They are described below: Sociodemographic data form: contained 21 items related to socio-professional data, the clinical environment and decision-making dynamics in intensive care services. The variables were numerical for age and qualitative dichotomous and polytomous categorical for the rest. ECNQ-CCV-Portuguese version: As mentioned previously, this questionnaire was created and validated in Spain by Falcó-Pegueroles and colleagues.
14,15
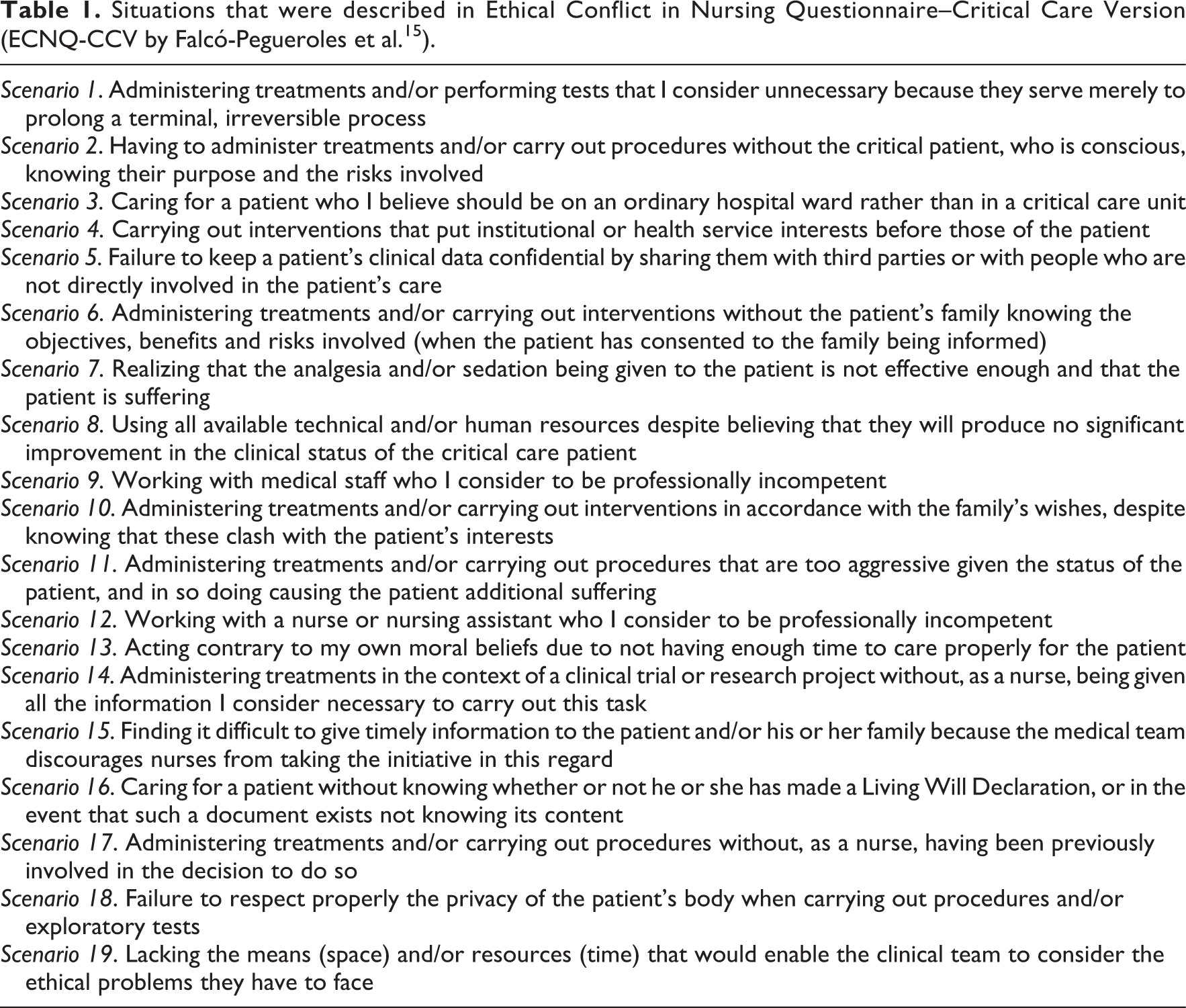
The questionnaire, which is self-administered and takes about 15 to 20 min, describes 19 situations that potentially give rise to ethical conflict (Table 1), classified into three areas: patient and family interpersonal relationships (P&F) (seven items); treatments and clinical procedures (T&CP) (five items); and to finish, the service dynamics and the work environment (DS&WE) (seven items). The questionnaire addresses the following points in each situation: (a) Temporary frequency of conflicting situations: answers have a Likert-type format with six options (never, almost never, at least once a year, at least once every 6 months, at least once a month, at least once a week) – if the answer is never, the participant moves on to the next situation; (b) intensity of ethical conflict: answers have a Likert-type format with five options (non-problematic, slightly problematic, somewhat problematic, moderately problematic and very problematic); (c) type of experienced ethical conflict: answers have a categorical format, with six options: four types of ethical conflict and two moral states. Each section includes a brief definition of each ethical type and moral state: moral indifference, because I do not feel involved in this situation; moral well-being, because I can act according to my ethical values and my convictions; moral uncertainty, because I sense there is an ethical problem but I cannot identify the values involved or the best actions; moral dilemma, because I perceive two ethically correct options and I have to choose one of them; moral distress, because I know which action is ethically correct but something prevents me from acting accordingly; moral outrage, because I am aware that an ethically incorrect action is being taken by others and I feel there is nothing I can do.
Situations that were described in Ethical Conflict in Nursing Questionnaire–Critical Care Version (ECNQ-CCV by Falcó-Pegueroles et al. 15 ).
A fourth variable, the index of exposure to ethical conflict, is obtained from the result of frequency and intensity variables for the 19 situations obtaining a range between 0 and 475.
Data analysis
For statistical analysis, the SPSS PASW-21 was used. A descriptive analysis was carried out using frequencies and percentages, measures of central tendency and dispersion.
The normality, reliability and construct validity test of the ECNQ-CCV-Portuguese was analysed based on the index of exposure to ethical conflict variable, following the original version’s method. The Kolmogorov–Smirnov (KS) and Shapiro–Wilks tests were applied to assess the goodness of fit of the distributions.
Cronbach’s α was determined considering a value greater than 0.7 as satisfactory to determine the instrument’s internal consistency. The Kaiser–Meyer–Olkin (KMO) test and the Bartlett’s test of sphericity were conducted to check the adequacy of data for factor analysis. The construct validity was analysed based on the factorial analysis of principal components with varimax rotation. To carry out this type of analysis, participants who had encountered this situation were taken into account (question a). Finally, the analysis of variance (ANOVA) test was performed to compare the groups’ means and to check whether the quantitative variable, the index of exposure to ethical conflict, was influenced by qualitative variables. The assumptions when applying the test were studied first, and the equality of variances was verified by performing Levene’s statistical test. Furthermore, the Pearson correlation coefficient was applied to compare the index of exposure to ethical conflict with the variables of age and years worked.
Ethical consideration
This study was authorized by the Bioethics Commission of the University of Barcelona (Spain), the Associação de Apoio ao Serviço de Cuidados Intensivos do Centro Hospitalar do Porto (Portugal) and the Sociedade Portuguesa de Enfermagem de Saúde Mental (Portugal). The guidelines of the Declaration of Helsinki and the legal regulations of both countries on personal data confidentiality were followed.
All subjects were informed about the voluntary nature of their participation in the study and about the absence of any financial reward for taking part. Participants were informed both orally upon distribution of the questionnaire and in writing about the confidentiality of data and research authorship. The research team assigned an external number to each delivered questionnaire. The fact of returning the completed questionnaire was regarded as the subjects’ written consent to participate in the study. Participants were given an email address in case they needed to ask any questions.
Results
Demographic characteristics
Two hundred and forty questionnaires were returned, of which 56 were discarded as incomplete, leaving a final sample of 184 participants.
A total of 70.1% (n = 129) were women, with an average age of 36.83 (±8.67) years and professional experience in critical patient care of 13.82 (±8.20) years. No statistically significant relationship was observed between index of exposure to conflict and sex (F = 0.69, p = 0.793) or age (p = 0.942). Participants’ districts of origin were situated mostly in the northern part of the country, specifically Porto (63.5%, n = 117) and Vila Real (15.1, n = 28). A total of 68.9% (n = 127) of professionals worked in intensive care, although some nurses worked in cardiology units (8.2%, n = 15), emergencies (8.2%, n = 15) and intermediate critical care (6.5%, n = 12), among others. The majority (83%, n = 157) had a rotating morning-afternoon-night shift, and a significant relationship was found between this latter variable and exposure to ethical conflict (F = 6.528, p < 0.001).
In relation to academic level and professional category, 62% (n = 114) were registered nurses and 25.5% (n = 47) were specialized in a field of critical care. A total of 57.6% (n = 106) of nurses had no postgraduate training in critical care and 94.6% (n = 74) had no training in bioethics. Table 2 shows the sociodemographic and professional characteristics of the sample.
Sample demographic and professional characteristics and IEEC correlation (n = 184).
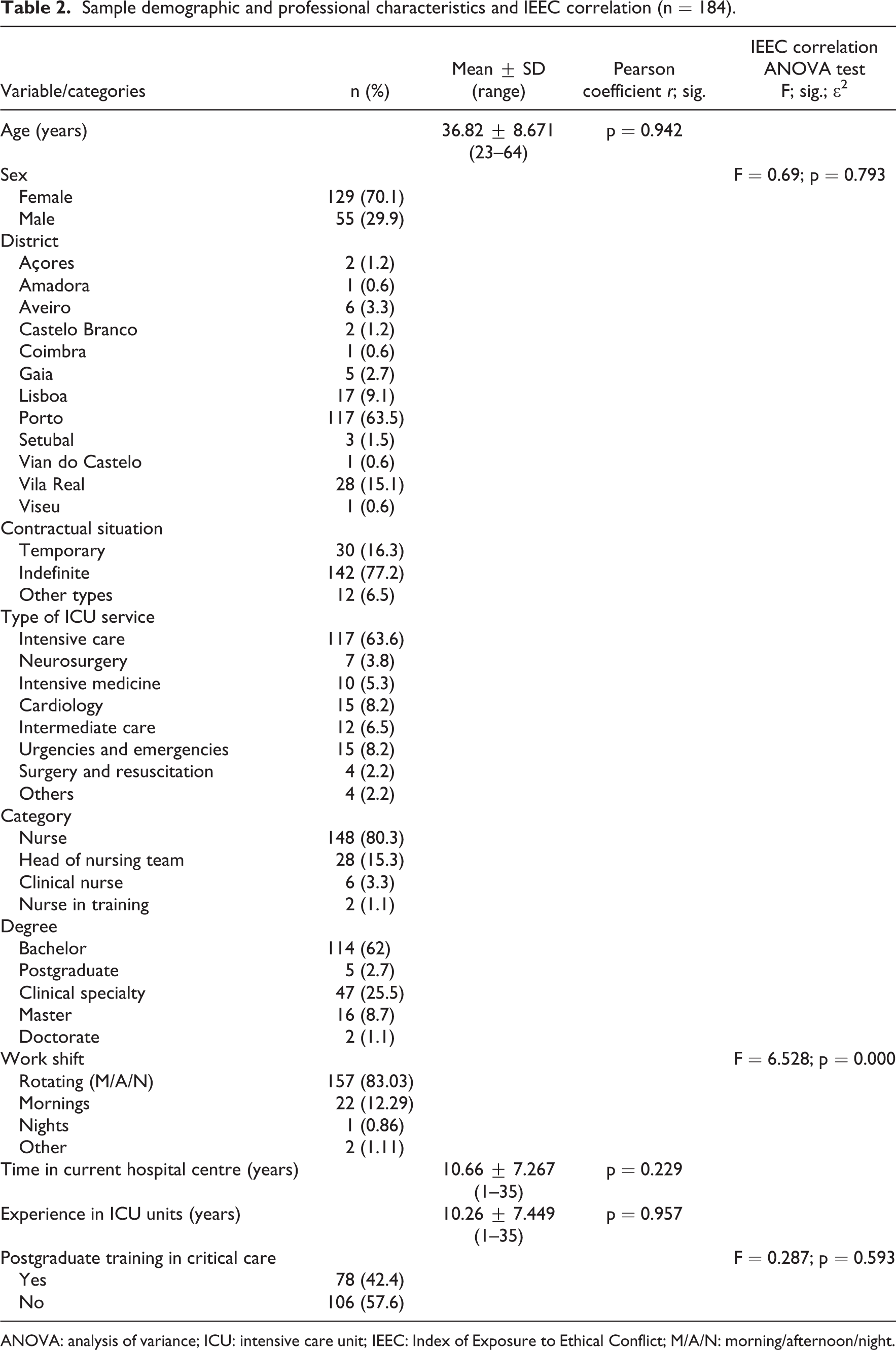
ANOVA: analysis of variance; ICU: intensive care unit; IEEC: Index of Exposure to Ethical Conflict; M/A/N: morning/afternoon/night.
Reliability and validity of the ECNQ-CCV-Portuguese version
The ECNQ-CCV-Portuguese version obtained a Cronbach’s α value of 0.886, all 19 items obtaining α values between 0.876 and 0.888 (Table 3).
Cronbach’s α and exposition ethical conflict index for each item (n = 179).
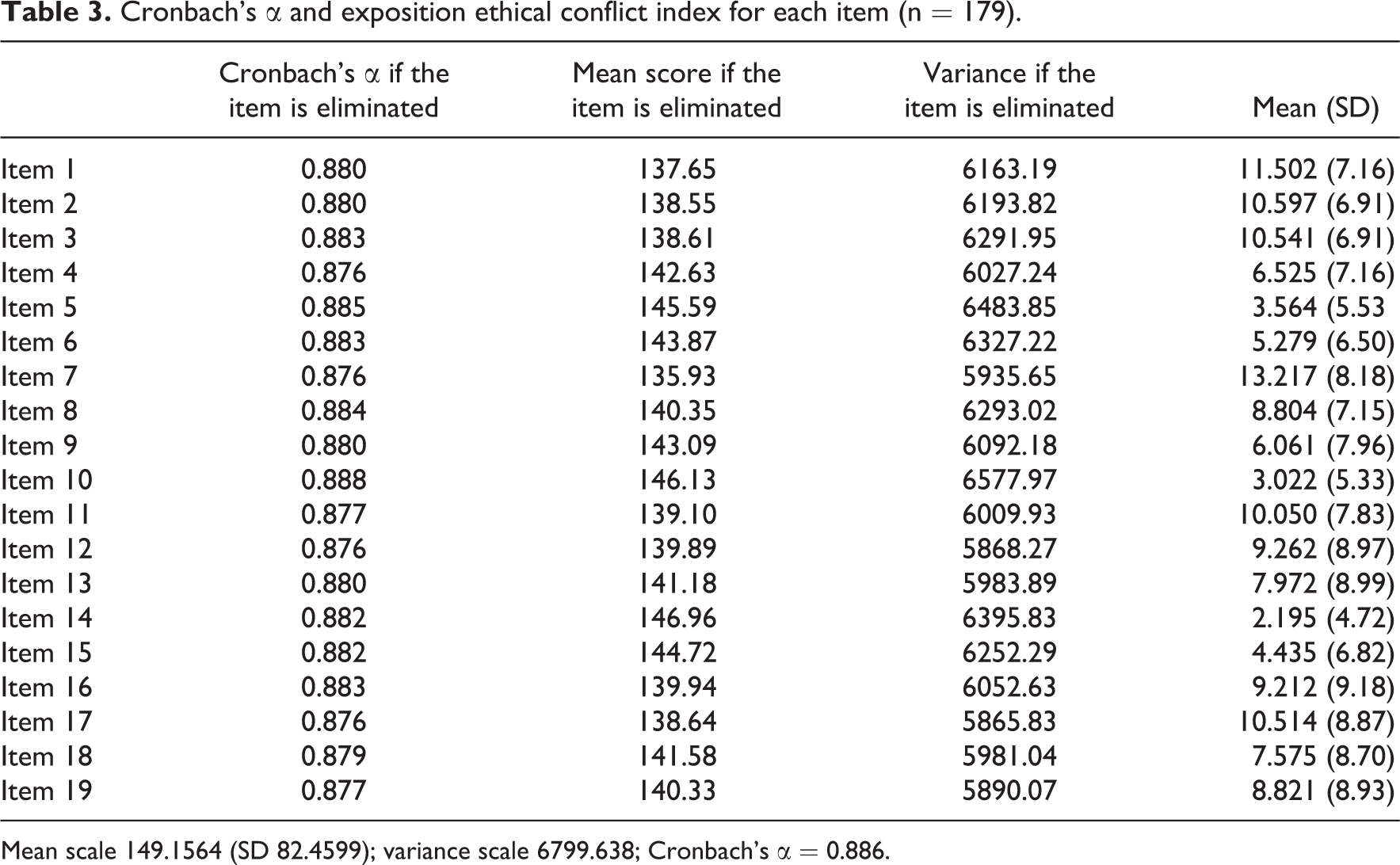
Mean scale 149.1564 (SD 82.4599); variance scale 6799.638; Cronbach’s α = 0.886.
The KMO test obtained a value of 0.817 (p < 0.001) and Bartlett’s sphericity test a χ2 value of 1541.288 (p < 0.001), which showed adequacy of data for factor analysis. Once the exploratory factorial analysis was carried out, a component capable of explaining 33.510% of the variance was identified, in line with the original instrument (Figure 1).

Sedimentation graph for ECNQ-CCV-Portuguese version.
Levels of exposure to ethical conflict and clinical context
A mean = 149.15 (SD 82.45) was obtained with a range of exposure to ethical conflict from 0 to 389. In relation to the normality tests, the results of the KS test (statistic = 0.085; df = 179; p = 0.003) and the Shapiro–Wilks test (statistic = 0.961; df = 179; p < 0.001) indicated that the phenomenon of exposure to ethical conflict analysed in the sample did not fit the normal curve.
Regarding the frequency of occurrence of ethically conflictive situations, without exploring the level of ethical conflict that may arise in professionals, the following situations occurred at least once a month or week: ‘S2. Having to administer treatments and/or carry out procedures without the critical patient, who is conscious, knowing their purpose and the risks involved’, with 62.5% (n = 115), and ‘S3. Caring for a patient who I believe should be on an ordinary hospital ward rather than in a critical care unit’, with 62% (n = 114) (Table 4).
Frequencies and percentages for ‘frequency with which ethically conflictive situations emerged’.
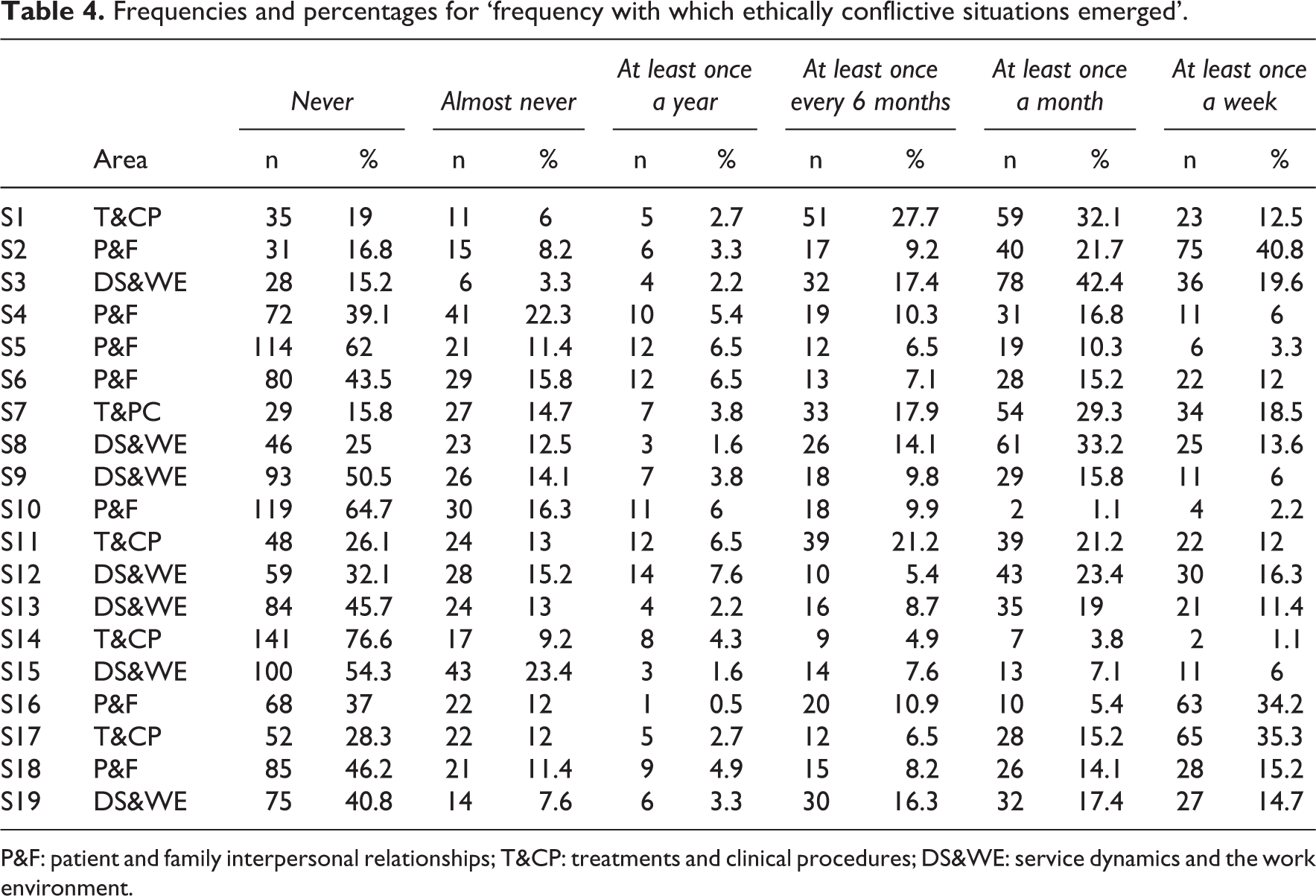
P&F: patient and family interpersonal relationships; T&CP: treatments and clinical procedures; DS&WE: service dynamics and the work environment.
Conversely, the situations that occurred less frequently, never or almost never were as follows: ‘S.10 Administering treatments and/or carrying out interventions in accordance with the family’s wishes, despite knowing that these clash with the patient’s interests’, with 81% (n = 149), and ‘S5. Failure to keep a patient’s clinical data confidential by sharing them with third parties or with people who are not directly involved in the patient’s care’, with 73.4% (n = 135).
The following situation was particularly interesting in this regard: ‘S.16 Caring for a patient without knowing whether or not he or she has made a Living Will Declaration, or in the event that such a document exists not knowing its content’, as the data revealed very similar percentages at the extremes of never (37%, n = 68) and at least once a week (34.2%, n = 63). This question raises the issue of diversity of opinion in relation to the management of guidelines given in ICUs.
On the other hand, in relation to perceived conflict intensity without considering its frequency, the situations ‘S7. Realizing that the analgesia and/or sedation being given to the patient is not effective and that the patient is suffering’ (78.8%, n = 134) and ‘S11. Administering treatments and/or carrying out procedures that are too aggressive given the status of the patient, and in so doing cause the patient additional suffering’ (60.9%, n = 112) were perceived as moderately to very problematic by Portuguese nurses (Table 5).
Frequencies and percentages for ‘degree of ethical conflicts experienced’.
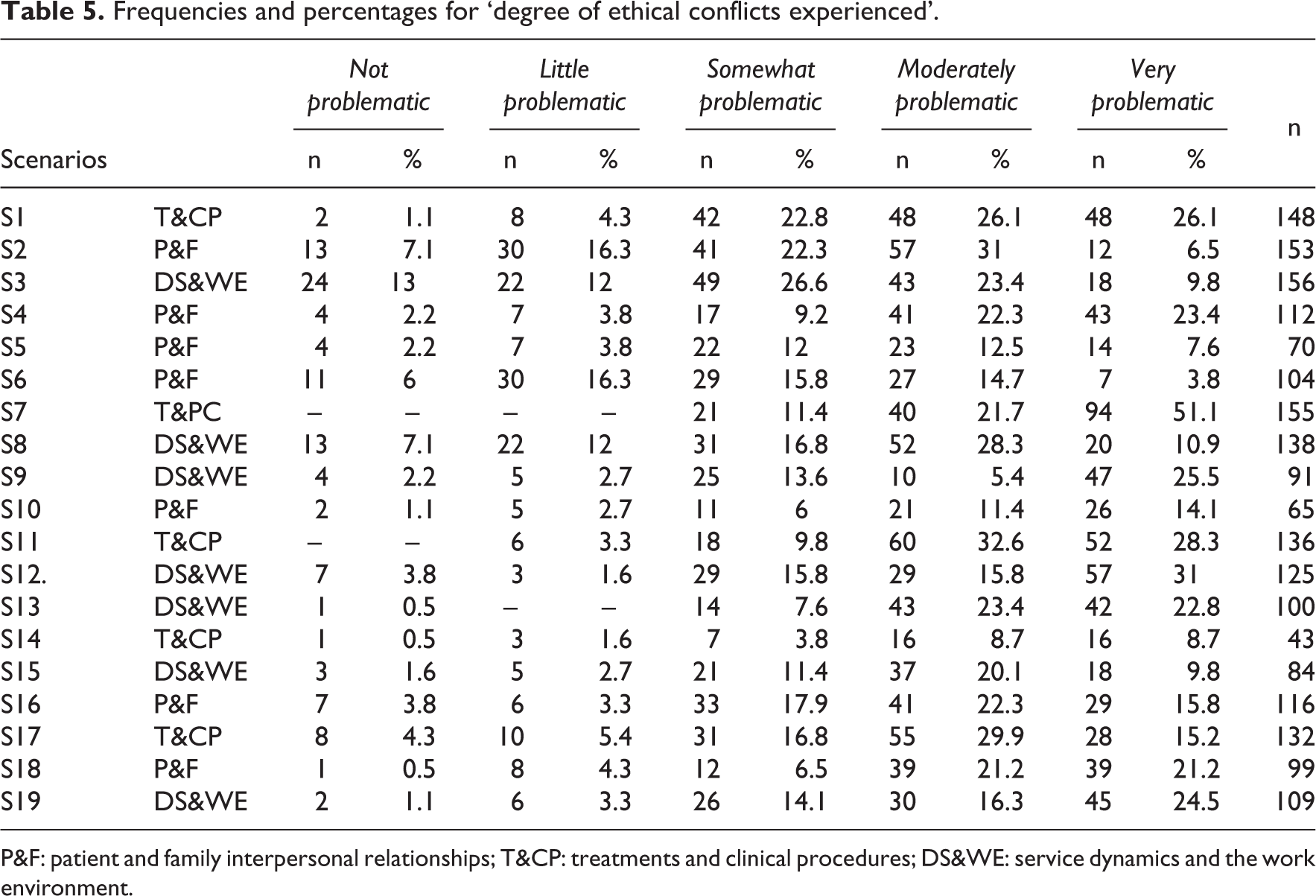
P&F: patient and family interpersonal relationships; T&CP: treatments and clinical procedures; DS&WE: service dynamics and the work environment.
When exploring the scenarios based on the exposure index variable which considered both conflict frequency and intensity, the realization that analgesia and/or sedation given to the patient was not effective and that the patient is suffering (S7) proved highly conflictive, with a = 13.217 ± 8.18 (Table 3).
Regarding the clinical environment, 92.4% (n = 170) of the professionals were aware of the existence of an Ethics Committee in their hospital, although only 45.1% (n = 84) knew how to ask for support from this Committee if necessary. A total of 44% (n = 81) said they did not know about the existence of any protocols to guide ethical decision-making in conflictive situations relating to critical patients’ care. However, 86.4% (n = 159) said that having such protocols, guides or multidisciplinary discussion sessions could be useful when having to face conflicting situations from an ethical perspective.
A total of 64.7% (n = 119) of the surveyed professionals reported having complex or conflicting situations in their service, and 51.1% (n = 95) would have thought at some time of changing service due to overload or stress, an issue that was significantly related to levels of exposure to ethical conflict (F = 3.056, p = 0.05). Similarly, 73.3% (n = 135) stated that they knew some ICU professional who had decided to change service due to overload or stress.
Concerning the dynamics within the services, the professionals stated that the environment was favourable to the discussion and resolution of ethical problems deriving from critical patient care (45.7%, n = 84) or that this environment was favourable at times (40.2%, n = 74). In the same way, only 46.2% (n = 85) said they took part in decision-making, representing a statistically significant relationship with level of exposure to ethical conflicts (F = 5.841, p = 0.001). Nevertheless, 71.7 % (n = 132) said they would like to participate more actively in decision-making regarding patients’ clinical aspects, and a significant correlation (F = 8.508, p = 0.05) was also found (Table 6).
Frequencies and percentages on the clinical environment and dynamics in the ICUs and correlations with the index of exposure to ethical conflict (n = 184).

ICU: intensive care unit; ANOVA: analysis of variance; IEEC: Index of Exposure to Ethical Conflict.
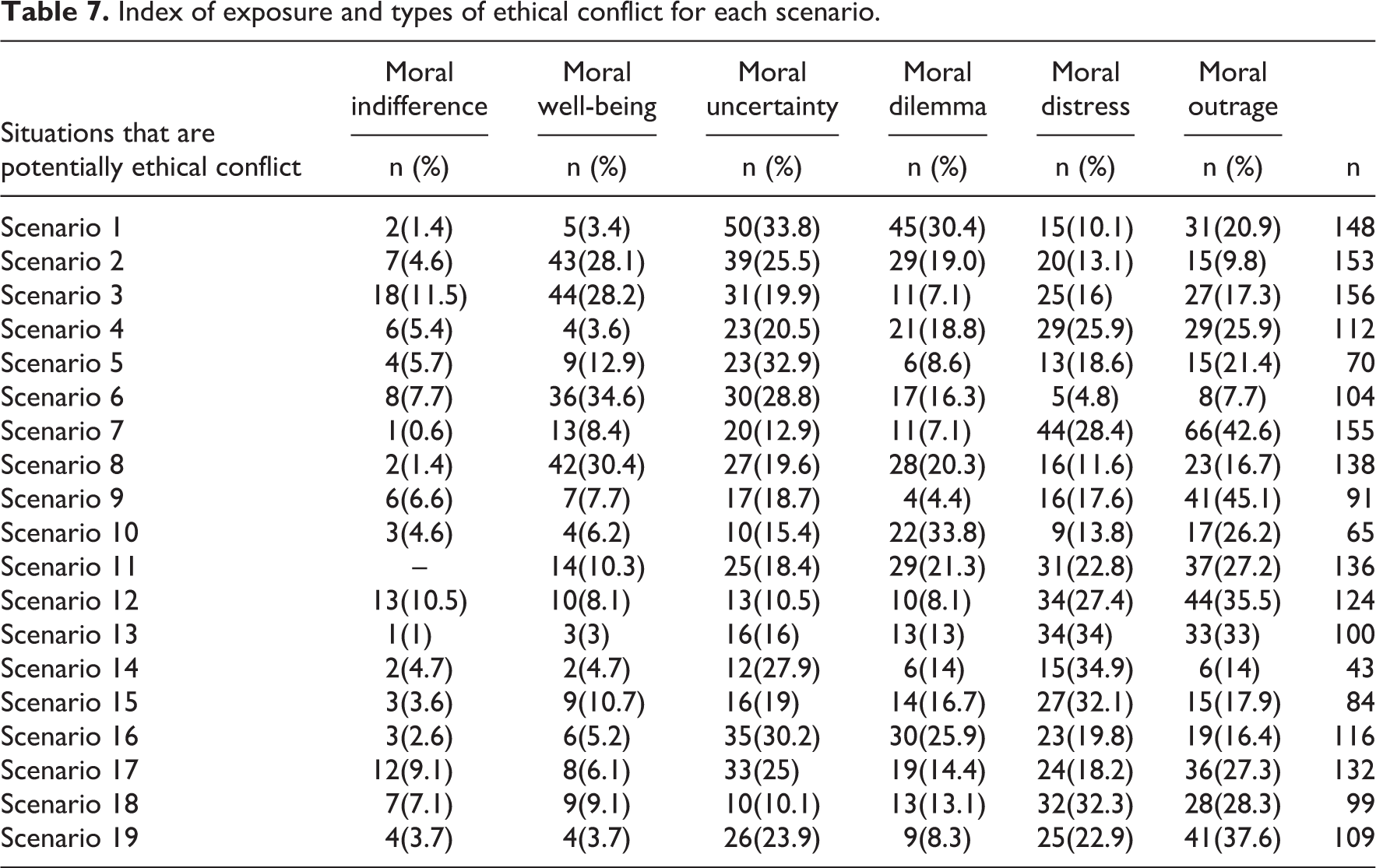
To finish, regarding the type of ethical conflict experienced by Portuguese nurses, moral outrage was the most common in seven of the 19 scenarios. It is worth noting that this type of conflict was also the most common in S7, relating to analgesic treatment inadequacy, and it was one of the most conflictive situations in terms of frequency and intensity. Situations of moral outrage involved care of patients and their families, treatments and procedures, and dynamics of the service and environment indistinctly (Table 7)
Index of exposure and types of ethical conflict for each scenario.
Discussion
The Portuguese version of the ECNQ-CCV was shown to be a valid and highly reliable instrument to measure exposure to ethical conflict in the context of the Portuguese-speaking population: it presented an α value above 0.85, 47 that is, equal to the value of the original Spanish version 15 and slightly below that of the version in Persian. 16 However, despite these positive results, it is necessary to consider some cultural differences between Portugal and Brazil that would justify complementary qualitative studies to capture specific and differentiating issues that may be introduced in a previous phase of adaptation according to the original study sample.
The underlying conceptual model allows exploring ethical conflict from different perspectives, offering a broader understanding of the phenomenon. Portuguese ICU nurses’ level of exposure was moderate, lower than the levels of nurses in Iran 28 and Spain. 12
In Portugal, the situations that generated the highest level of exposure to ethical conflict in ICUs were related to the ineffectiveness of analgesic pain control treatment in critical patients, the administration of treatments considered futile, and the problems generated by the management of resources. These findings are consistent with those of other authors. 2,12,23,26,28,38,48 The specific situation of witnessing the failure of analgesic treatment to control pain in critical patients revealed itself again as a frequent situation that generated high levels of conflict. However, few studies in nursing ethics and critical care nursing identify this specific situation; they place a greater emphasis on dilemmatic situations related to therapeutic futility, despite the latter not being common ICU context.
The data showed that neither the variables of gender, age, type or experience in ICUs nor professional category was associated with exposure to conflict, although the work shift variable was related. However, previous studies about moral distress have shown correlations between sex, 48 age 18 and type of ICUs 49 with high levels of moral distress. Consistent with other studies, 2,5,26,36,44,50 –52 the variables having ever thought about leaving the service due to overload or stress, being in an environment that is favourable to making ethical decisions and having the availability to participate more actively in these decisions correlated with exposure to types of ethical conflict. All the above show that ethical conflict, despite being an individual phenomenon, can be influenced by certain characteristics of the professionals’ working environment. This points to the possibility of intervening, for example, in the work dynamics adopted by the ICU team, in line with other studies that have taken the clinical environment into consideration. 2,5,7,22,23,36 –38 The fact that the type of ethical conflict most experienced in the sample under study was moral outrage is consistent with results obtained for the Spanish sample. 2 These results differ, however, from those obtained for the Iranian sample, 28 in which the most commonly experienced type of conflict was moral dilemma. More conclusive studies are now needed. Until then, this difference could be explained by the fact that levels of ethical conflict in Iran were lower than levels found in Portugal and would be in line with findings by Falcó-Pegueroles et al. 12 in which the conflict typology was structured from lesser to greater exposure to conflict. Naturally, cultural and religious factors may also play a part: Pishgooie et al. 28 relate these low to moderate levels of conflict to a form of resilience that is characteristic of the Islamic tradition, that is, the religious framework of Iranian critical care nurses.
As in the Spanish 15 and Iranian 16 samples, situations related to breaches of confidentiality, clashes of interests between families and patients, or instances in which medical teams tried to prevent nurses from giving information were infrequent and did not cause high levels of exposure to ethical conflict. This may have been because the professionals have these issues in mind and implement mechanisms to avoid these problems. This issue should also be useful to maintain the dynamics that have shown to protect against conflict, such as participating in decision-making.
To conclude, critical care nurses’ levels of exposure to ethical conflict in Portugal, though moderate, should stimulate initiatives to reduce these levels further. Actions aimed at increasing their participation in decision-making, ensuring that they know the purpose of treatments, and defined therapeutic strategies are important for them to feel broadly involved in critical patient care. To develop ample and autonomous responsibility regarding care also implies taking an active part in decision-making.
Implications for practice and limitations
Evaluating ethical conflict levels allows gaining a better understanding of problematic situations in ICUs. It is also necessary to implement specific measures aimed at reducing exposure to this problem and improving decision-making. In the specific case of analgesia control, despite services’ numerous clinical guidelines and protocols, urgent measures must be taken to improve patient quality and safety standards, in addition to reducing ethical conflict.
Regarding the study’s limitations, the fact that most respondents were women makes it difficult to examine the phenomenon from a gender perspective, an issue that should be considered in future work. The fact that the sample covered several health centres, though useful to extend the scope of the study, limited the possibility of analysing the specificities of each health centre or ICU. Regarding the methods we used, and considering some cultural differences between Portugal and Brazil, it could be required that future studies consider qualitative methods as a complementary in phase of adaptation. Finally, the size of our sample, despite being enough, is fair to raise a Confirmatory Factor Analysis (CFA). For this reason, future studies with long samples may consider to perform this type of analysis with the aim to find evidence about theoretical model operationalization.
Conclusion
The Portuguese version of the ECNQ-CCV is a valid and reliable instrument for measuring exposure to ethical conflict in Portuguese culture context. Moral outrage is the most frequently experienced type of ethical conflict among Portuguese critical care nurses, who presented moderate levels of conflict. The situations that produced the highest level of exposure to ethical conflict in our sample were related to the ineffectiveness of analgesic treatment to control pain, the administration of treatments considered futile and resource management problems. Consistent with previous studies, certain environmental factors and work dynamics had an impact on levels of ethical conflict, such as perception of overload, feeling of being in an environment favourable to ethical decision-making and wishing to participate more actively in decisions. These key factors should be borne in mind when designing strategies to prevent ethical conflicts and when seeking to foster ethical environments that improve decision-making in critical patients’ and their families’ care.
Footnotes
Acknowledgements
The authors would like to thank all the participants for their time and dedication to the questionnaire.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received a Research Support Grant from Department of Fundamental Care and Medical-Surgital Nursing and School of Nursing Faculty of Medicine and Health Sciences of the University of Barcelona (Spain).