
Abstract
Background:
Ethical and legal issues are increasingly being reported by health caregivers; however, little is known about the nature of these issues in geriatric care. These issues can improve work and care conditions in healthcare, and consequently, the health and welfare of older people.
Aim:
This literature review aims to identify research focusing on ethical and legal issues in geriatric care, in order to give nurses and other health care workers an overview of existing grievances and possible solutions to take care of old patients in a both ethical and legally correct way.
Methods:
Using a systematic approach based on Aveyard, a search of the PubMed, CINAHL, and Ethicshare databases was conducted to find out the articles published on ethical and legal issues in geriatric care.
Ethical considerations:
The approval for the study was obtained from UMIT-The Health and Life Sciences University, Austria.
Results:
Only 50 articles were included for systematic analysis reporting ethical and legal issues in the geriatric care. The results presented in this article showed that the main ethical issues were related to the older people’s autonomy, respect for their needs, wishes and values, and respect for their decision-making. The main legal issues were related to patients’ rights, advance directives, elderly rights, treatment nutrition dilemma, and autonomy.
Conclusion:
Further education for professional caregivers, elderly people, and their families is needed on following topics: care planning, directive and living wills, and caregiver-family member relationships to guide and support the elderly people within their decision-making processes and during the end-of-life care.
Introduction
Aging is not a disease, but a normal process. Nowadays, people are living longer worldwide. 1 The proportion of people over age 60 years is growing faster than any other age group as a result of longer life expectancy and declining fertility rates. According to the World Health Organization (WHO), 2 by 2050 the world’s population of people aged 60 years and older is expected to reach 2 billion, leaving behind a number of 900 million elderly people in 2015. 2 Today, 125 million people are 80 years or older. The population in the European region has the highest median age of elderly in the world. 3 In this study, “elderly” has been defined as a chronological age of 65 years or older, while those from 65 through 74 years old are referred to as “early elderly” and those over 75 years old as “late elderly.” 4 Elderly people have problems and needs that require attention and care from their family, health care practitioners, health care systems, and from the society. An organized effort of these institutions is needed in order to promote their health, well-being, recovery from illness or disability, and sustaining a healthy life. 1
It is the geriatric care that assesses the needs of older people, planning and implementing care, and assessing the effectiveness of care to achieve and maintain wellness and health. 1 Geriatric care is important to maximize the health and functional capacity of the aging population. 1 Aging is influenced by complex changes, such as biological losses that lead to an increased risk of disease, a decline in the capacity of the individual, and death. 1,2 The WHO 2 defines “aging” as “the course of gradual alteration in a person’s mind and body, and their relationships with others” Beyond these changes, older age involves other psychosocial changes that influence functional capacity, physical and mental health, and social involvement. 1,4 Due to these changes, when considering as a doubt of what ought to be done, health caregivers pose ethical and legal issues such as nonmaleficence “first do not harm” and autonomy. 1,4 As the health caregivers have the ethical and legal duty to protect patients, it is crucial for them to be well informed about ethical and legal issues. 1,4
Ethics are standard rules or principles that govern the right conduct and are designed to protect the rights of a human being. 1,5 In addition, principlism is a system of ethics that focuses on four important ethical principles, namely: autonomy, beneficence, nonmaleficence, and justice. 6 There is a set of ethics that is used by the nursing profession and mainly described in the code of ethics. The code of ethics is a list of principles intended to govern the behavior of those entrusted with providing care for the patients. 1,7 In the nursing profession, ethics provides the professional standards for nursing activities, which help to protect not only the nurse but also the patient. In 1973, the International Council for Nurses (ICN) adopted the code of ethics for the first time and implemented a rule that all nurses must follow this professional code. 1,5
Moreover, ethics helps to solve health care dilemmas and make the right decisions based on values that work in unison with the laws. 7,8 In contrast, laws are general rules of conduct that are enforced by a controlling authority. 7,8 They are designed to prevent harm to others while protecting the rights of individuals. Health caregivers have both a legal and ethical obligation to attend to their patients ‘needs. 1,7 Law and ethics intertwine in patient care. Compassion, trust, justice, and respect for patient privacy are all ethical principles which interact with the law (Figure 1 explains how law, ethics and principlism intertwine). Ethical and legal issues are usually closely related; however, ethical obligations exceed legal duties. 1,7
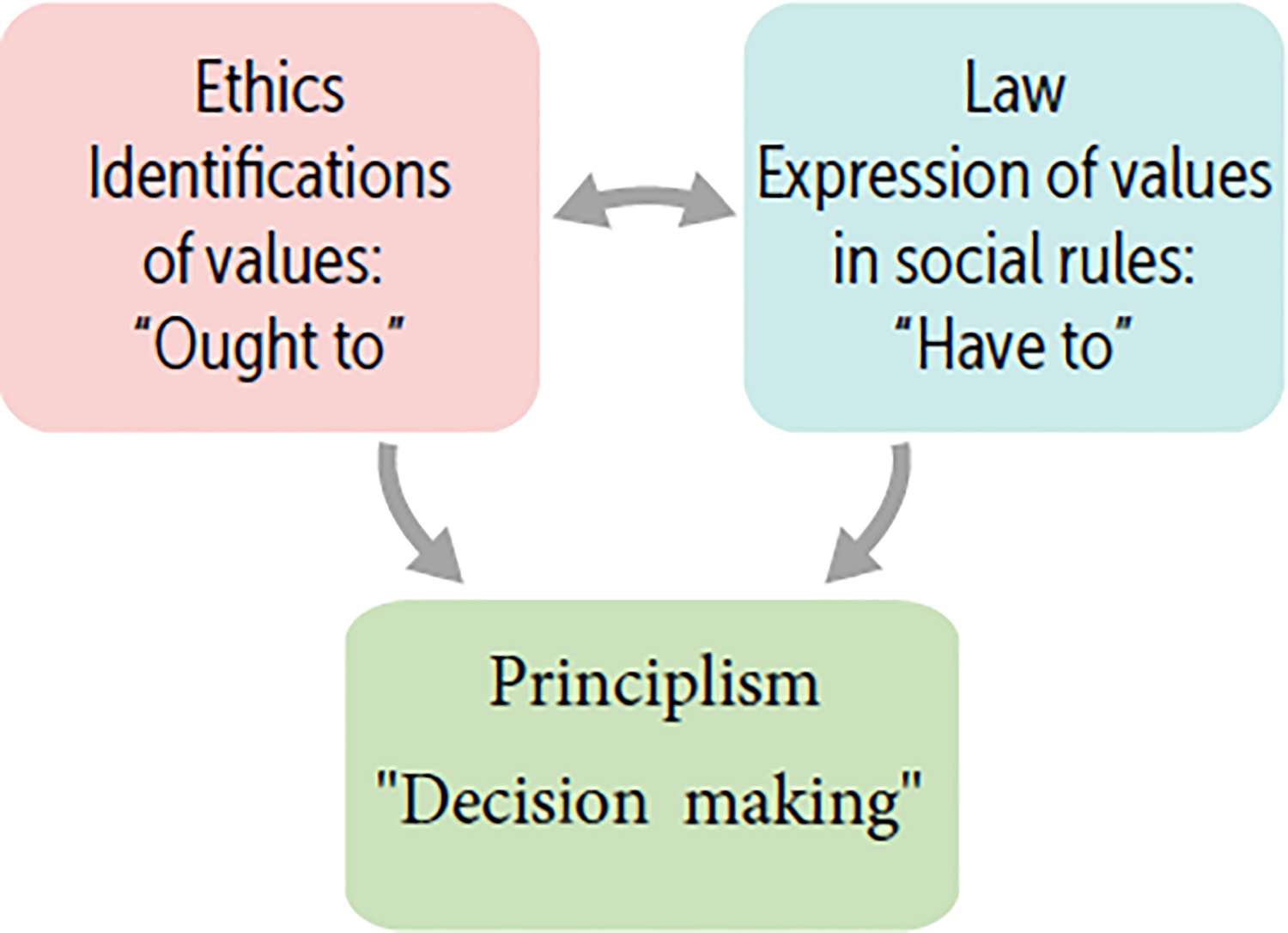
Law, ethics, and principlism intertwine.
Although nurses learn a lot about geriatric nursing and the problems of the elderly in theory, it is important in practice to rule out the possibility of the legal and ethical issues and protect the elderly by practicing the ethical principles of nursing care. Building knowledge of ethical and legal issues supports health care practitioners to function at the highest possible professional level, to avoid legal entanglements and litigation, and to be familiar with the rights, responsibilities, and concerns of the patients.
As a framework for assessing the ethical aspects of the elderly “Principlism” of Beauchamp and Childress 6 can be used; following four main principles of autonomy, beneficence, nonmaleficence, and justice. Moreover, to contrast and discuss the ethics-related results, the ICN Code of Ethics for Nurses can be used. 5 In addition, as a framework for the legal aspects of the review results, the human rights framework with its hard and soft laws on the international level, can be used to analyze the legal issues related to the care of elderly persons. Figure 2 shows a list of international and European sources to protect human rights of older people. Human rights are understood as the actions, terms, and liberties that all people are permitted to experience, which include political, municipal, financial, communal, and social rights. 9 Human rights are essential, absolute, symbiotic, and amalgamated, which means that they cannot be given nor taken. 9 Patients in geriatric care should enjoy universal human rights. Legal issues arise when there is violation of human rights. Health caregivers should be aware of all the rights of the older people, respect them, and help these people to get their rights implemented.

International and European main law sources in the field of human rights.
Aim of the study
This review aims to identify research focusing on ethical and legal issues in geriatric care; to give nurses and other health care workers an overview of existing grievances and possible solutions to take care of old patients in a both ethical and legally correct way.
Research questions
What are the ethical issues recognized by health care practitioners, elderly people, and relatives in geriatric care?
What are the legal issues recognized by health care practitioners, elderly people, and relatives in geriatric care?
What methods have been used in studying ethical and legal issues in geriatric care?
Materials and methods
Literature search
This article reports the results of a systematically conducted literature review guided by Aveyard. 10 Figure 3 illustrates the literature search process. We performed a systematic literature search during (November 2015—December 2015) using three electronic databases (PubMed/Medline, CINAHL and Ethicshare) and hand searching, using the following keywords: “ethic,” “bioethics in geriatric care,” “ethics in geriatric care,” “law in geriatric care,” “geriatric care,” “elderly care,” “health caregivers’’, “family,” “relatives,” and “older people.” Two reviewers (N.P., M.F.) independently screened the studies using the following inclusion criteria: (1) focus on ethical and/or legal issues in geriatric care, (2) published in English as full text, (3) focus on informants such as health care practitioners, elderly people, and/or their relatives, and (4) are published between January 2000—December 2015.
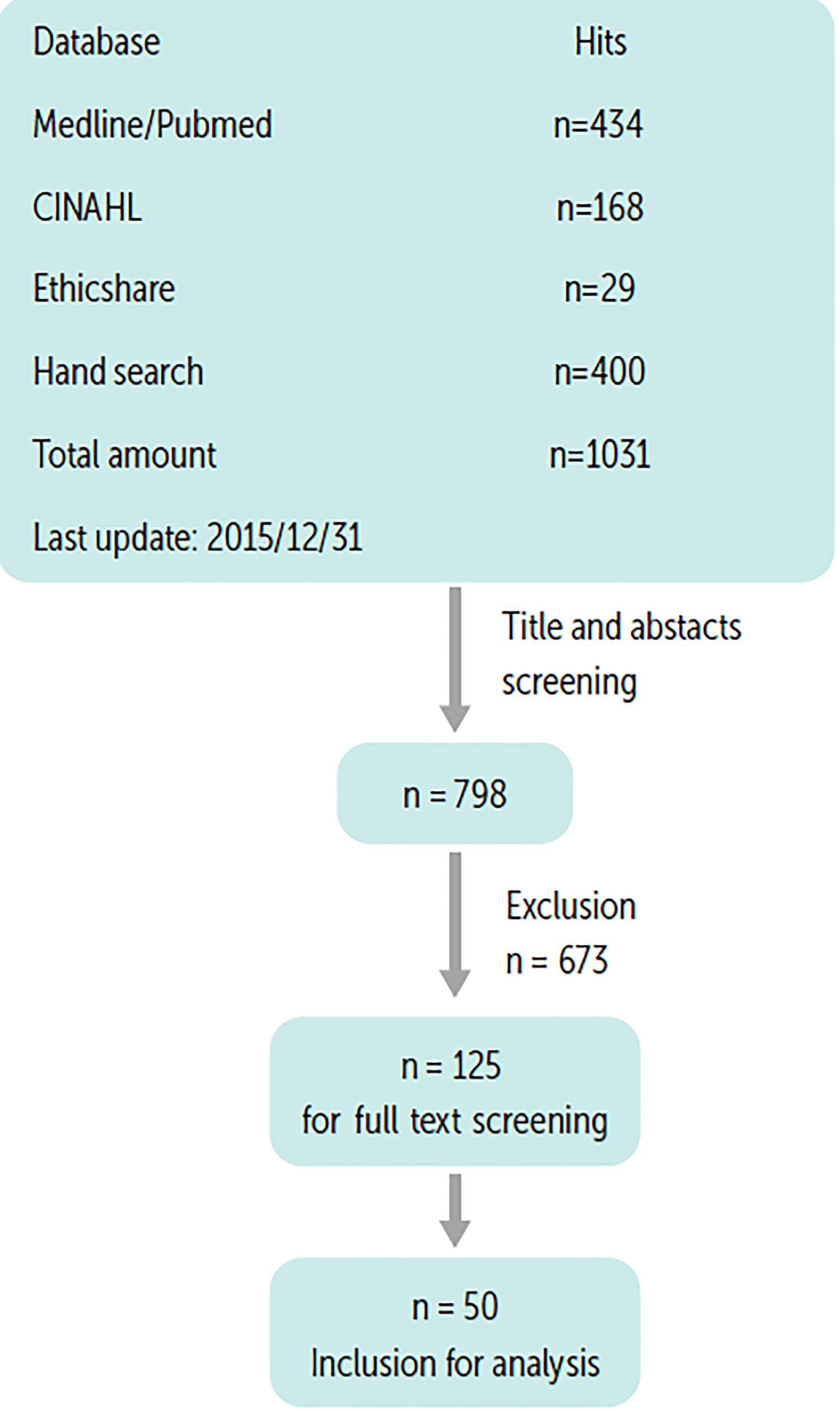
Flow diagram of the systematic search.
Search results
The retrieval process was conducted systematically in four phases. 10 The initial phase identified 1031 articles, which were examined following the inclusion/exclusion criteria by two researchers working independently, and when there were disagreements it was decided together which abstracts would be included in the further steps (Figure 3). A total of 798 studies were included based on title and abstracts screening. In the second phase of the review, the two researchers re-examined the abstracts and selected 125 studies and a total of 673 abstracts were excluded (300 did not focus on ethical and legal issues; 200 were editorials, letters, and dissertations; and 173 were not full-text in English language).
In the third phase, the full texts of the 125 articles were reviewed independently. At the end of this phase, 75 articles were excluded since 50 were not related to geriatric care, and 25 were not related to ethical and/or legal issues.
In the fourth and last phase, the 50 included articles were systematically analyzed using a data collection sheet. The results presented in this article are based on the synthesis of the information collected from this evaluation (for a detailed overview, see Supplemental Appendix 1).
Settings
These 50 studies were conducted in settings such as nursing homes and senior centers (18), hospitals (8), clinics (4), emergency and primary health care centers (3), other long-term care institutions, and continuing care institutions (3). Other studies used mixed settings such as hospitals and nursing homes (6), hospitals, and nursing homes, and other long-term care institutions (2), nursing homes, community centers, and long-term care institutions (1), and one study was conducted in a community center and long-term care institutions.
From the articles retrieved, 13 were conducted in the United States, 11 from the Nordic countries, 6 from the United Kingdom, and the remaining from Australia (3), Canada (1), Ireland (1), Czech Republic (1), Netherland (1), Belgium (1), Turkey (1), Israel (1), Austria (1), Saudi Arabia (1), China (1), and Germany (1). Five studies were conducted in (Finland, Spain, Greece, Germany, and the United Kingdom), and one was conducted in the European Union (EU) countries. From these studies, 24 were published between 2006 and 2010, and 17 were published between 2000 and 2005. Only nine studies were published within the period 2011–2015 (see Figure 4).
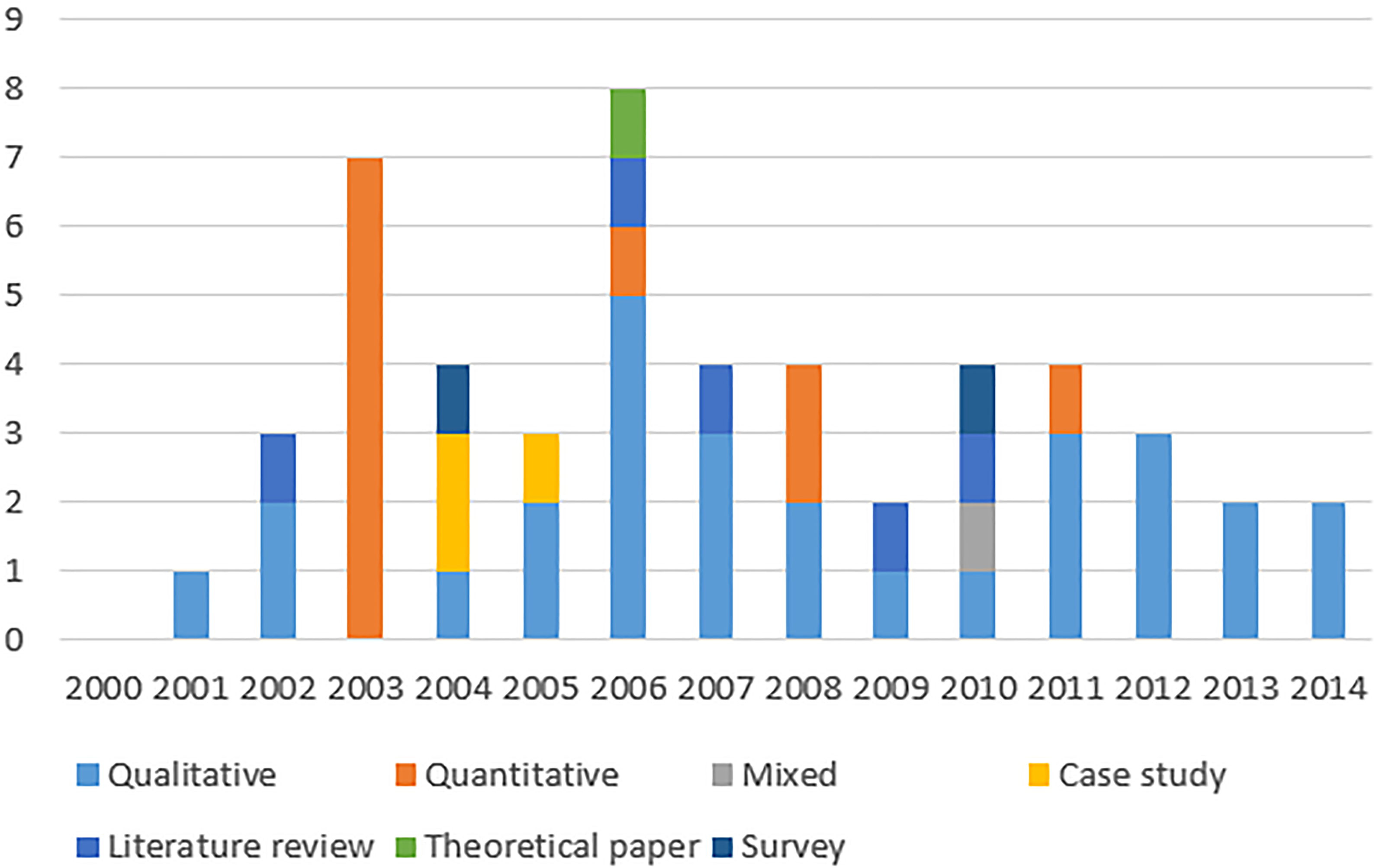
Study design—the year of publication.
Sample
Usually the study participants included were as follows: nurses and elderly people (10); all health care professionals and elderly people (9); only nurses (6); only health care professionals (5); only elderly people (5); physicians (2); elderly people, relatives, and all health care professionals (6); elderly people and relatives (1); nurses and relatives (1); and one study used as informants only relatives.
Methods used
A total of 29 articles used a qualitative approach, 13 were quantitative, 6 were literature reviews, one used mixed-method and one was theoretical paper (Table 1).
Overview of study design and data analysis approaches.

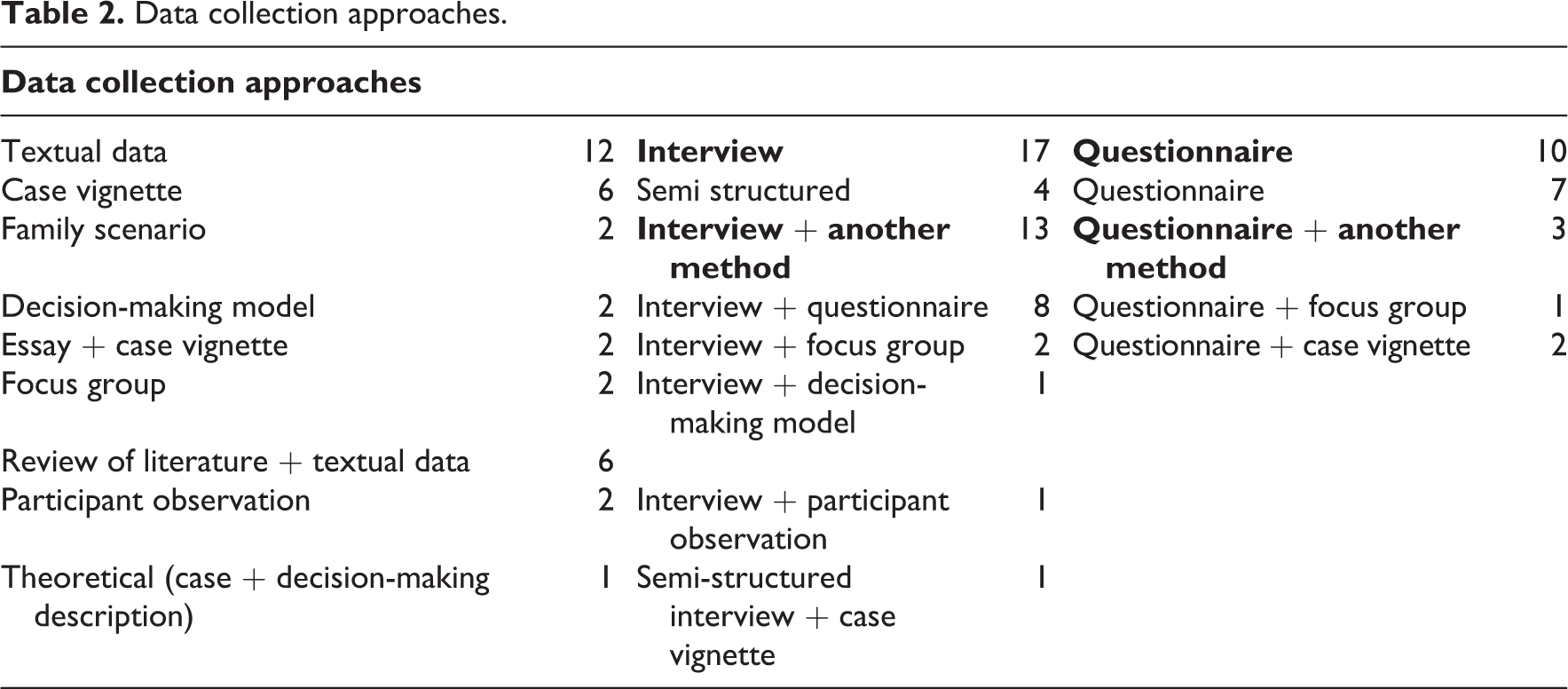
The most common data collection tool was different types of interview (17), textual data (12), questionnaire (10), and focus group (2). Details are described in Table 2.
Data collection approaches.
When analyzing the ethical and legal issues 22 studies were identified to use content analysis, 13 studies used statistical analysis; and others: grounded theory (7), ethnography (2), phenomenology (2), concept analysis (2), and two studies use critical analysis (Table 2).
Textual data (case vignettes, essays, and narratives) were used to study both ethical and legal issues. 11 –14 Two literature review studies analyzing critically the role of autonomy and paternalism in elderly, and the ethical decision-making at the end of life were included in this review. 11,15 One other literature review presented an ethically based pain management action plan for nursing home residents. 12 One bibliometric analysis of keywords and terms used in the literature on ethics and dementia during the period 1980–2000, was found in other literature review studies. 13,16 Furthermore Tuckett 11 in their review describes the elderly and nurses rights in nursing homes.
Ethical consideration, reliability, and validity
In fourteenth studies, the ethical quality of the studies was assured by obtaining ethical approval (from different Ethical Commissions/Institutions) and the informed consent, to implement the studies (Table 3). In six studies, the informed consent was taken from different study participants, and only three studies give information about the ethical approval from different ethic commissions.
Studies reporting ethical consideration, reliability and validity.
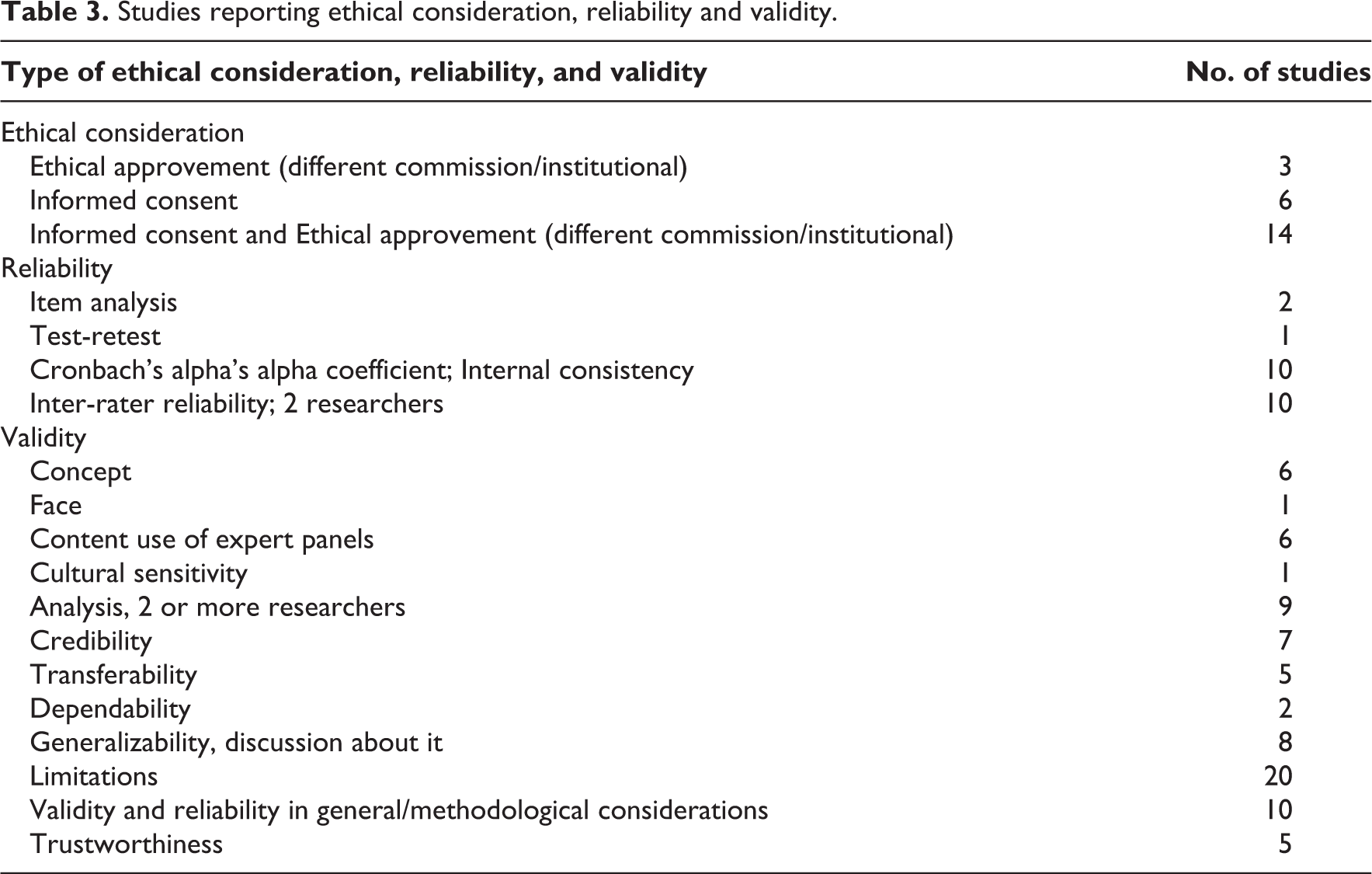
In some studies, information about validity and/reliability was reported. Referring to reliability, 10 studies used the internal consistency test of the data collection instrument by using Cronbach’s alpha coefficient. Ten other studies mentioned the inter-rater reliability that improved by use of several researchers.
Analysis of validity was broader. To enhance the validity of the content two or more researchers were used. Expert panels were also used. In 20 studies, there was general discussion about study limitations, and methodological considerations. Anyway, the discussion about validity and reliability was superficial and limited through the papers.
Supplemental Appendix I. shows the summary of the review. The frequencies of the documented ethical and legal issues are documented in Supplemental Appendix II and Appendix III.
Results
Ethical issues
Principle of autonomy
Respect for autonomy
The reviewed studies focused on several ethical and legal issues in geriatric care. The authors discussed different ethical issues related to the principle of autonomy, which is an ethical principle that emphasizes the rights of every person to make choices, to receive and give information, and to consent. 11,17,18 It is the respect for the geriatric patient’s capacity to hold his views and make decisions without being manipulated by others, but being based on his or her values and beliefs. 11,17,18 Issues on respect for older peoples’ autonomy (or restriction of autonomy, self-determination, and self-esteem) were discussed in 41 studies. 11,15 –46 Issues on human dignity and integrity (respect/lack) were discussed in 20 studies. 35,36,47 –49 It has been argued that respect for the elderly’s needs, wishes, and values is very important both for health care practitioners, elderly people, and their relatives. 14,18,34,49,50 Five researchers gave importance to the family wishes. 23,51 –53 Issues about the information given to/received by the patient were essential for the health care practitioners. 12,28,54 Elderly people and their relatives complained about the lack of information about diagnoses, treatment, and end-of-life treatments. 22,55 Most health care practitioners have to deal with ethical issues on choices and decisions, and cultural influences on elderly decision-making in their daily routine care. 17,41,47,56 Wilmot et al. gave importance to elderly decision-making on prolonging life treatment during artificial feeding. Health care practitioners must respect the patients’ choice of refusing eating or treatment. The findings highlighted that many ethical problems are related to elderly competence and capacity on decision-making. 23,35,44 In many cases, especially when the elderly people were at the end of life and not capable of deciding, the decisions needed to be made by family members (surrogate, next of kin), or by health care practitioners; therefore, different ethical issues come out. 11,13,14,51 Eggenberger and Nelms, and Teeri et al. emphasized the importance of the involvement of the family members and health care practitioners in advocating and deciding when the patients are not able for decision-making. Elderly independence is a crucial issue for health care practitioners and elderly people. 20,39,40,53 Elderly difficulties in communicating their decisions 17,47,51 and informed consent issues 16,18,19,23,57 related to treatment, especially in the end-of-life treatment, were broadly discussed in the studies included in this review.
Principle of nonmaleficence
Nonmaleficence is the principle of not doing any harm to the patients. 1,6,7 Different researchers mentioned ethical issues on feeding and artificial hydration such as refuse of nutrition, or forced nutritional treatment and not doing harm 17,18,54 or tube-feeding patients with dementia, 14 and ethical dilemma on voluntarily stopping eating and drinking, 38 especially when the elderly suffered from dementia, stroke or other end-of-life conditions. Sandman et al. stated that ethical conflicts arose for health care professionals when an elderly stroke patient refused nutrition, and health care professionals should force on nutritional treatment. Wilmot et al. discussed that when dementia patients refuse food, it is unacceptable and impossible to force nutrition, but offering them food on an hourly basis is different. Many researchers discussed issues on life-prolonging and sustaining treatment in the end of life for improving the quality of life, withholding/withdrawing treatment or food, 13,19,36,41,53 choice for no treatment, refuse of treatment, force using for the treatment, or do not harm while treating. 25,27,40,58 Cultural and religious aspects of ethical issues on the treatment of terminally ill elderly people, or end-of-life geriatric care, were emphasized from Enes and De Vries, and Clarfield et al. in their studies. Only three of the studies included in our review focused on euthanesia 13,24,25 and genetic testing. 13,44 Health care professionals have to provide ethical pain 12 in everyday care for elderly people 34,39 and during end-of-life care. 18,53 Advance care planning and different kinds of advance directive were treated as ethical issues in different studies, especially in the end-of-life cases. 18,19,25,53
Principle of beneficence
Under the principle of beneficence which consists of moral obligations, actions performed by healthcare practitioners for the benefit of the patients, while providing holistic care to the patients. 1,6,7,18 researchers discussed different ethical issues in the literature. Ethical problems related to benevolence, 25 well-being, 38 relieve suffering, 17,18 and sanctity of life were necessary for health care practitioners, elderly people and their relatives. Schaffer emphasized that the improvement of the quality of end-of-life care for elderly people would also improve the experience of dying for the elderly and their relatives, and this contributes to their well-being. Benefits and costs are ethical issues with great importance on the end-of-life care for the elderly. 39,42,46 Preventing harm 38,40,42 and acting on patients’ best interest 11,51,54 cause different situations of ethical problems. Issues on utility (on medication, minimizing pain, and maximizing benefits over harm), 11,17 –19 and other ethical issues related to paternalism on decision-making were discussed. 11,21,41,42 McBrien emphasized that it is difficult to avoid ethical problems related to paternalism as a decision made by physicians for the patients’ best interest. Health care practitioners often face different ethical dilemma on respecting elderly autonomy and avoiding paternalism.
Principle of justice
Ethical issues under the principle of justice, which is the ethical principle of being fair to all geriatric patients and providing equal treatment, providing to the patients what is his or her due, 1,6,7,21,48 are often related to elderly abuse, such as physical, psychological, and emotional abuse. 40,48,57 Buzgova and Ivanova found that the most frequent form of elderly abuse is psychological, and the elderly, who are more often abused by the health care practitioners, were aggressive and confrontational. In some cases, elderly people were facing age discrimination. 28 Staff abuse, such as aggressive behavior from elderly people, was reported in different studies. 13,21,47,59 In many studies, ethical issues were related to distributive justice 41,46 and social justice. 22,25,57 Equality 38,41 and fairness 39 were also documented as important ethical issues under the principle of justice.
Legal issues
The majority of the reviewed articles described patients’ rights 13,14,18,22,29,32,38,60 and elderly rights 11,29,38,42 as legal issues. Patient competency, 21 privacy and beneficence, 14 guardianship, 13 and privilege for competent patients 36 were discussed as legal issues, too. Cheung and Yam, and McBrien discussed negligence as a failure of health care practitioners from exercising their legal duty of care. They described battery as an intentional application of force to another person’s body without legal justification, and false imprisonment as an intentional act that causes the restriction of freedom of movement to another person without legal justification. Confidentiality, 32 elderly abuse, 40,46 next-of-kin issues, 21,57 and patient capacity on providing or refusing a valid consent 45,57 were treated as legal issues. Self-determination concerning the quality of care, 42,45,48 physical restraint issues, 21,42,46,49 surrogate decision-making issues, 13,16,18,54,60 and elderly decision-making issues 13,16,23,25,41,52 were also treated as legal issues. According to Chernoff, Clarfield et al., Eggenberger and Nelms, Sandman et al. and Scott et al., autonomy should be discussed as a human right. Informed consent, on the other hand, was seen as a legal issue, 21,22,33,46,49 and professional liability 25,28,38,48,52 and different treatment or nutritional issues as legal dilemmas. 21,25,38,46,60 Studies included in our review showed that usually elderly people with dementia leave their final life decision-making (ethical and legal decisions) to family members, who assign the medical power of attorney. 13,14,23 Living will bring different legal issues for elderly people, especially during the end-of-life period. 15,19,21,54 Eleven studies included in our review described legal issues related to advanced directive, which helps determine the patients’ wishes. 13,14,16,18,21 –23,41,45,48,54
Discussion
The four principles of principlism as outlined by Beauchamp and Childress 6 are autonomy, non-maleficence, beneficence, and justice. These four areas were explored in relation to the findings in this study.
Ethical issues
Autonomy
According to Beauchamp and Childress, 6 autonomy is essential because it provides individuals with the ability to make their own decisions. When dealing with elderly patients, however, different conditions may affect their ability to make decisions on their own behalf. This directly compromises patients’ autonomy, which may entail restriction of autonomy, self-determination, and self-esteem, which were topics of discussion in most of the research explored. 19,41,46,51,54 This is not to say that health care providers are not concerned with elderly patients’ autonomy, but rather, the opposite. The communication of information received by and given to patients proved essential for healthcare practitioners. 12,28,54 A complaint cited by Clarfield et al. 22 and Jonasson et al. 55 touched on a lack of information about diagnoses, treatment, and end-of-life treatments provided to elderly patients, though this may be a direct result of health care practitioners dealing with ethical issues on patients’ choices and decisions, and cultural issues on the elderly patients’ decision-making concerning their care. 17,41,47
The research indicated that patients’ autonomy may be comprised at the best interest of the patient if the patient refuses treatment. 23,35,44 When elderly patients reach the end of their life, they may not be deemed competent to make major decisions, which therefore results in major decisions being made by family members, such as surrogates or next of kin, or by the health care practitioners themselves. 11,13,14,51 Health care practitioners attempt to remove themselves from major decision-making for the patients by involving the patients’ family members in order to determine whether the patient is competent to make his or her own decisions. 18,51 If the patient is deemed incompetent to make their own decisions, the decision to compromise the patient’s autonomy may be made in the patient’s best interest. 18,51
Nonmaleficience
In the care of patients, it is vital to refrain from causing harm to patients, whether psychologically, physically, or in any other form. 61 Health care practitioners are responsible for caring for their patients in a way that ensures their utmost safety and security. Due to the compromise in patient autonomy, healthcare practitioners may be forced to make decisions in the best interest of the patient, with the overall intent of evoking the least harm as possible. This may include the health care practitioner making decisions about food and nutrition. 17,36,54 Patients who suffer from dementia, stroke, or other end-of-life conditions may, for instance, stop eating and drinking entirely. 38 In this instance, decisions come into play as to whether the health care practitioner should force nutritional treatment or tube-feed patient’s. 14,17,18,54 If patients with certain conditions, like dementia, refuse food, the health care practitioner is ethically unable to force nutrition, but they are able to provide a solution by offering food on a daily basis. 17 As part of their care, health care practitioners must administer ethical pain management for elderly people. 12,20,34 Other issues are related to life-prolonging and sustaining treatment, withholding/withdrawing treatment or food, 13,19,36,41,53 choice for no treatment, refuse of treatment, force using for the treatment, or do not harm while treating the patient. 40 The patient’s religious affiliations may also impact the choices that are made in relation to their care, specifically with euthanasia and genetic testing. 13,24,25
Beneficence
This principle supports that health care practitioners are to make decisions that are in their patients’ best interests. 61 This, again, may entail a direct compromise of autonomy, in that if the patient is deemed incompetent, he or she may be unable to make the best decisions for their care. This poses a challenge because health care practitioners strive to avoid paternalism and compromising patients’ autonomy, though it is often a different dilemma to avoid. 11,21,41,42 When making these decisions, health care practitioners must also consider benefits and costs for the patient. 42,46,39 One of the ultimate objectives of health care practitioners is to ensure patients’ benevolence, well-being, to relieve suffering, and to ensure the sanctity of their lives. 17,18,25,38 In order to do so, however, healthcare practitioners may have to aid in the decision-making for patients concerning utility, or medication, pain minimization, and maximizing benefits over harm. 17,18,25,38
Justice
The principle of justice shares similarities with benevolence, in that it supports justness, fairness, and equality among the treatment of patients. 61 In other words, health care practitioners are responsible for health care of the elderly people. Justice is compromised when incidences of elderly abuse occur between the health practitioner and the patient, which may include physical, psychological, and emotional abuse. 40,48,57 Not only does this compromise justice, but non-maleficence and benevolence as well, deeming it an overarching beach of Beauchamp and Childress’s principles, and consequently the failure of the health care practitioner to morally and effectively fulfill their role. Age discrimination is a problem posed in relation to elderly care, 28 a problem that also compromises the health care practitioners’ role of being just in treatment. A complication of justice, or a factor that may trigger ill behavior, is when staff abuse occurs, or when aggressive behavior is exhibited by elderly patients. 13,21,47,59
Legal issues
A major theme in the legal aspect of this study revolved around patients’ rights and elderly rights. 13,14,18,22,29,32,38,60 The human rights framework supports that all human beings are entitled to a set of liberties, and Beauchamp and Childress’s 6 four principles further ensure these standards are maintained by health care providers in the treatment of elderly patients. A significant variable that may affect the patient’s rights, however, is patient competency, which ultimately determines the patient’s decision-making. 21 When it falls under the legal aspect, autonomy is identified as a human right, but informed consent is a legal issue. 21,22,31 –33,46,49,54 Also included in legal matters is professional liability, which includes different treatments or decisions about nutrition. 21,25,28,38,46,48,52,60 The inability to provide informed consent, or the allocation of decision-making to family members or health care practitioners, does not compromise the patient’s human rights; they are still entitled to enjoy certain liberties and should receive fair treatment.
To ensure the proper decisions are made for patients who are unable to provide informed consent for procedures or methods of care, health care practitioners explore various avenues before they are deemed suitable to make decisions for the patient’s care. This includes surrogate decision-making, confidentiality, and the patient’s ability to provide or refuse valid consent. 13,16,18,32,33,45,54,57,60 Dementia patients often have their final decision-making left to family members, who may assign the medical power of attorney, allocating the decision-making to the health care professionals. 13,14,23 To avoid challenges with end-of-life care and decision-making, health care practitioners may look to advance directive, which helps determine the patients’ wishes in end-of-life care 13,14,16,18,21 –23,41,45,48,54 or living wills. 15,19,21,54 If a health care practitioner does not exercise all avenues appropriately as related to patients’ abilities to provide informed consent and decision-making, they are identified as negligent, which is the failure of health care practitioners from exercising their legal duty of care. 21,46
Connection to the nursing code of ethics
In addition, as mentioned above, we compared the results of our literature review with the principlism of Beauchamp and Childress 6 and developed the connection to the nursing code of ethics. 5 There are nine provisions in the nursing code of ethics, which have direct associations to the four principles of Beauchamp and Childress’s standards.
Provision one of the ICN 5 upholds the principle of autonomy and justice; provision two supports the principles of autonomy and beneficence; provisions 3, 6, 7, 8, and 9 support the principles of autonomy, justice, beneficence, and non-maleficence; provision 4 upholds the principles of beneficence, non-maleficence, and justice; and provision 5 upholds the principles of beneficence and justice. The themes underlying the responsibilities of nurses are rooted in the four principles, which call for health practitioners to follow ethical, and legal standards of care in regards to their patients and profession.
Ethical dilemma
Our findings highlighted many ethical dilemmas in caregiving for the elderly such as benefits from treatment versus harm, 14,21,57,58 costs of treatment versus benefits, 14 autonomy versus beneficence, 11,14,18 paternalism versus autonomy, 11,21 futility versus autonomy, 19 the value of good quality of life versus autonomy, 54 and autonomy versus self-endangering behavior. 47 In different care situations, ethical dilemmas were related to nutritional and treatment support 15,25,38 and the duty of health care practitioners to respect the patients’ rights versus the duty to protect them from harm, 21 and longevity versus the quality of life. 39
Other ethical issues in geriatric care
Many researchers stated ethical issues related to patient rights, 14,18,21,24,48 fidelity (trusting nurse-patient relationship), 12,27,53 patient-family relationship, 23,47,51 and the preservation of life. 14,54 Other ethical issues were related to privacy, 14,15,31,36,40,44 and confidentiality. 27,36,62 In addition, many researchers discussed ethical issues related to veracity: truth-telling from the staff to the patients. 13,15,24,25
Professional issues
Most of the researchers discussed health care professional ethical issues, such as issues related to health-care services and systems: a shortfall of financial resources, or organization-related problems. 19,33,43,62 Issues related to staff experience, like staff training, skills and knowledge, were mentioned by Enes and De Vries, Hicks, Scott et al., and Teeri et al. Both the duty to provide care 21,39,52 and professional care ethics 13,20,37 lead to professional issues in the context of ethical caring for the elderly. Professional judgment such as force-feeding or treating 17,40,48,54 and limited staff and time for providing elderly care 21,51,52,59 forced the health care staff into problematic situations. Many ethical issues were related to cultural influences in respecting elderly people, 17,55 not letting them die and treating them emotionally during the terminal phase. 33,42,44,46 Staff conflicts during caregiving were often sources for ethical problems. 20,24
Conclusion and implications
From the above-identified studies, one can conclude that ethical and legal issues differ a lot in different settings and different areas. Twelve studies assessed both ethical and legal issues. 13,14,18,22,29,32,38,46,60 However, there were also studies that lacked the interaction between legal and ethical issues since they mainly focused on ethical issues. Studies done in the United States and Australia focus mainly on discussing legal issues in geriatric care. In Europe, Sweden was the country that was identified with more publications discussing the legal and ethical issues. In this review, we have also included reviews, theoretical papers, as essay and discussion papers, with the aim to get the overall impact of the practical issues and models that are daily routine in the geriatric care. Many studies included in our review focused on ethical and legal issues and conflicts related to nutrition and treatment of elderly people with dementia. 24 In order to solve the conflicts between the ethical principles and the legal issues, education of caregivers, elderly people, and their relatives are needed on advance care planning, 41 advance directive and living wills. 27 Attention should be given to the caregiver (nurse)–family member relationship, for guiding and supporting their decision-making or enhancing end-of-life care. During end-of-life care, many ethical and legal dilemmas were identified, and interdisciplinary group discussions, a collaboration between nurses and doctors, 20 and seminars and conferences can help solve these dilemmas. Elderly care institutions (nursing homes) need to better recognize the palliative needs of patients, 15 prepare their staff to provide quality care for living and dying patients, 12 and collaborate with different stakeholders to make the process of dying more acceptable for elderly people and their families. Integrating hospice and palliative care into health care and providing education initiatives to address end-of-life issues through public health strategies help to improve the quality of end-of-life care, and the quality of death for elderly people and relatives that improves their well-being is necessary. 12,53,60 In every day care issues, resolving different ethical and legal issues within the nurse–elderly person relationship, 48 and educational programs for caregivers and elderly people are needed. 35 Analyzing and solving ethical problems in every day care may increase care givers’ ethical competence. Thus, it is of high relevance to improve education in ethics and law for health care practitioners (mainly nurses). Finally, the assessment of interpersonal skills may need to become a part of admission criteria in nursing programs. 37
This review has included different studies that report a variety of ethical and legal issues in geriatric care including all participants that contribute to health care in geriatric care. In addition, we have explained all known methods used to find out the above-mentioned issues for a period of 15 years. This leads to the strength of this review, a comprehensive analysis of perspectives and settings. However, this review focused on studies identified from three databases, studies published in English language, which may exclude available literature from countries in other languages. Our review concludes that further research is needed to identify ethical and legal issues in geriatric care.
Supplemental material
Supplemental Material, Appendix_I - A systematic review of ethical and legal issues in elder care
Supplemental Material, Appendix_I for A systematic review of ethical and legal issues in elder care by Nertila Podgorica, Magdalena Flatscher-Thöni, Daniela Deufert, Uwe Siebert and Michael Ganner in Nursing Ethics
Supplemental material
Supplemental Material, Appendix_II - A systematic review of ethical and legal issues in elder care
Supplemental Material, Appendix_II for A systematic review of ethical and legal issues in elder care by Nertila Podgorica, Magdalena Flatscher-Thöni, Daniela Deufert, Uwe Siebert and Michael Ganner in Nursing Ethics
Supplemental material
Supplemental Material, Appendix_III - A systematic review of ethical and legal issues in elder care
Supplemental Material, Appendix_III for A systematic review of ethical and legal issues in elder care by Nertila Podgorica, Magdalena Flatscher-Thöni, Daniela Deufert, Uwe Siebert and Michael Ganner in Nursing Ethics
Footnotes
Authors’ note
Nertila Podgorica is now also affiliated with University of Shkodra “Luigj Gurakuqi”, Albania.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Erasmus Mundus Western Balkans (ERAWEB), a project funded by the European Commission.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.