
Abstract
People with mental illness are subjected to stigma and discrimination and constantly face restrictions in the exercise of their political, civil and social rights. Considering this scenario, mental health, ethics and human rights are key approaches to advance the well-being of persons with mental illnesses. The study was conducted to review the scope of the empirical literature available to answer the research question: What evidence is available regarding human rights and ethical issues regarding nursing care to persons with mental illnesses? A scoping review methodology guided by Arksey and O’Malley was used. Studies were identified by conducting electronic searches on CINAHL, PubMed, SCOPUS and Hein databases. Of 312 citations, 26 articles matched the inclusion criteria. The central theme which emerged from the literature was “Ethics and Human Rights Boundaries to Mental Health Nursing practice”. Mental health nurses play a key and valuable role in ensuring that their interventions are based on ethical and human rights principles. Mental health nurses seem to have difficulty engaging with the ethical issues in mental health, and generally are dealing with acts of paternalism and with the common justification for those acts. It is important to open a debate regarding possible solutions for this ethical dilemma, with the purpose to enable nurses to function in a way that is morally acceptable to the profession, patients and members of the public. This review may serve as an instrument for healthcare professionals, especially nurses, to reflect about how to fulfil their ethical responsibilities towards persons with mental illnesses, protecting them from discrimination and safeguarding their human rights, respecting their autonomy, and as a value, keeping the individual at the centre of ethical discourse.
Introduction
People with mental illness are a vulnerable group, facing barriers in the exercise of political, civil, and social rights. In addition, they may face stigma and discrimination and are much more likely to experience disability and die prematurely, compared with the general population. 1 In this context of social exclusion and deprivation, mental health, ethics, and human rights are key approaches to advancing the well-being of persons with mental illness.
Social and economic rights, such as the rights to health and to mental health, deserve respect because they are a foundational set of rights. 2 The concept of mental health as a human right, and not as a moral claim, involves the states obligations of respecting, defending, and promoting this entitlement. 3 Nevertheless, there are constant political failures in the provision of adequate social and healthcare services to persons with mental illness, especially concerning their right to self-determination and legal protection from coercive interventions of uncertain benefits. 4
Issues regarding mental healthcare are complex. Therefore, strong lines of communication that are meaningful to health professionals and patients’ relationships are necessary in order for both of them to understand and adequately deal with these different mental healthcare issues. They are related not only to healthcare ethics, but also to moral decision making in situations health professionals are confronted with on a daily basis. In this perspective, the International Code of Ethics for Nursing adopted by the International Council of Nurses (ICN) states that nurses’ primary responsibility is to people requiring care. Inherent in nursing is the respect for human rights, including cultural rights, the right to life and choice, to dignity and to be treated with respect. Nursing key professional values are respectfulness, responsiveness, compassion, trustworthiness and integrity.
5
In this context, civil liberties and professional ethics become active parts of mental health nurses’ daily practice, 7 which is grounded in values. 8 Results from a study held in six New England states with the purpose to identify the frequency of ethics and human rights issues experienced by Psychiatric-Mental Health and Substance Abuse Registered Nurses (RNs) (162 participants) showed that 23% of them were directly involved in ethics and human rights issues “daily or almost daily.” The most experienced issues were protecting patients’ rights and human dignity (61.7%), providing care with possible health risks to RNs’ health (e.g. tuberculosis, HIV, or violence) (45.1%), use/nonuse of physical/chemical restraints (40.1%), respecting/not respecting informed consent to treatment (38.3%), and staffing patterns that limit patient access to nursing care (30.9%). 9 In sum, mental health nurses often deal with ethics and human rights issues. Therefore, it is important to further discuss these issues as well as their implications for nursing professional practice. Considering this complex scenario faced by mental health nurses, this scoping review focuses on human rights and ethical issues regarding nursing care to persons with mental illness.
Method
The review was based on the interpretive scoping design framework described by Arksey and O’Malley 10 and was conducted to provide an estimation of the broadness and scope of the available research literature as well as to provide knowledge for further research on the theme. The scoping study method is guided by a requirement to identify all relevant literature regardless of study design. These authors point out that a scope study differs from a systematic review in several ways. The latter answers questions from a relatively narrow range of studies, after assessing the quality of the evidence. Scope studies are less likely to have very specific research questions or to conduct quality assessments, usually addressing broader topics that are likely to involve a variety of different projects. The sequential process involved formulating the research question; identifying relevant studies; selecting studies against inclusion and exclusion criteria; and charting the data and collating, summarizing, and reporting the results. 10
Formulating the research question
The human rights and ethical issues regarding nursing care to persons with mental illness were the central problem which motivated the development of this scoping review. The guiding question for the scoping review was identified as, “What are the experiences of nurses who care for people with mental illness in relation to human rights and ethical issues?”
Identifying relevant studies
A search of international research on human rights, ethics, and psychiatric/mental health nursing published in English from the year 1970 was used to identify the studies. The year of 1970 was chosen because it marked the movement of Psychiatric Reform in different countries in the globe, mainly due to violations regarding the human rights of persons with mental illness. In addition, authors also aimed to enable the comprehension of the breadth of studies and knowledge published on the theme.
In consultation with a reference librarian, relevant databases were identified and search terms were refined. The electronic databases were PubMed, Scopus (multidisciplinary databases that index articles of high impact factor), CINAHL (data base of the Nursing area), and HEIN (database of relevance in Rights). In the search for the literature related to the proposed theme, the qualification of the process occurred through the search for descriptors through MeSH (Medical Subject Headings) and DeCS (Health Sciences Descriptors). The vocabularies used were “human rights” AND “ethic” AND “mental health” AND “nursing.”
Selecting studies against inclusion and exclusion criteria
The collected materials were obtained through electronic databases: PubMed (72 studies), CINAHL (168 studies), Scopus (45 studies), and HEIN (27). A total of 312 articles were found in the databases. Articles were submitted to a pre-selection by reading the title and abstract, contributing to selecting the list of studies associated with the guiding question. Following title screening, 228 articles were excluded and 84 studies were selected for title and abstract review. After this pre-selection, with the filtering of articles by means of readings, 26 articles were excluded and 26 articles were identified as potentially eligible (Figure 1). This scoping review was conducted by two independent reviewers according to the established criteria.

Flow of information.
All the publications on the relationship between human rights and ethics regarding nursing care to people with mental illness, in English, were included in the analysis. The exclusion criteria adopted were the impossibility of acquiring the article, and those that did not correspond directly to the theme, with focus including other health professionals or people with other problems (relationship of human rights, ethical issues, and different health conditions).
Charting the data and collating, summarizing, and reporting the results
The articles’ contents were analyzed, sorted, codified, categorized, and summarized in a unified and integrated conclusion, according to the instrument developed by Ursi and Galvão. 11 Data analysis included summarizing some characteristics: author, year, periodical, origin, design/methods, and focus (Table 1). Collating, summarizing, and reporting the results were carried out in accordance with the research question.
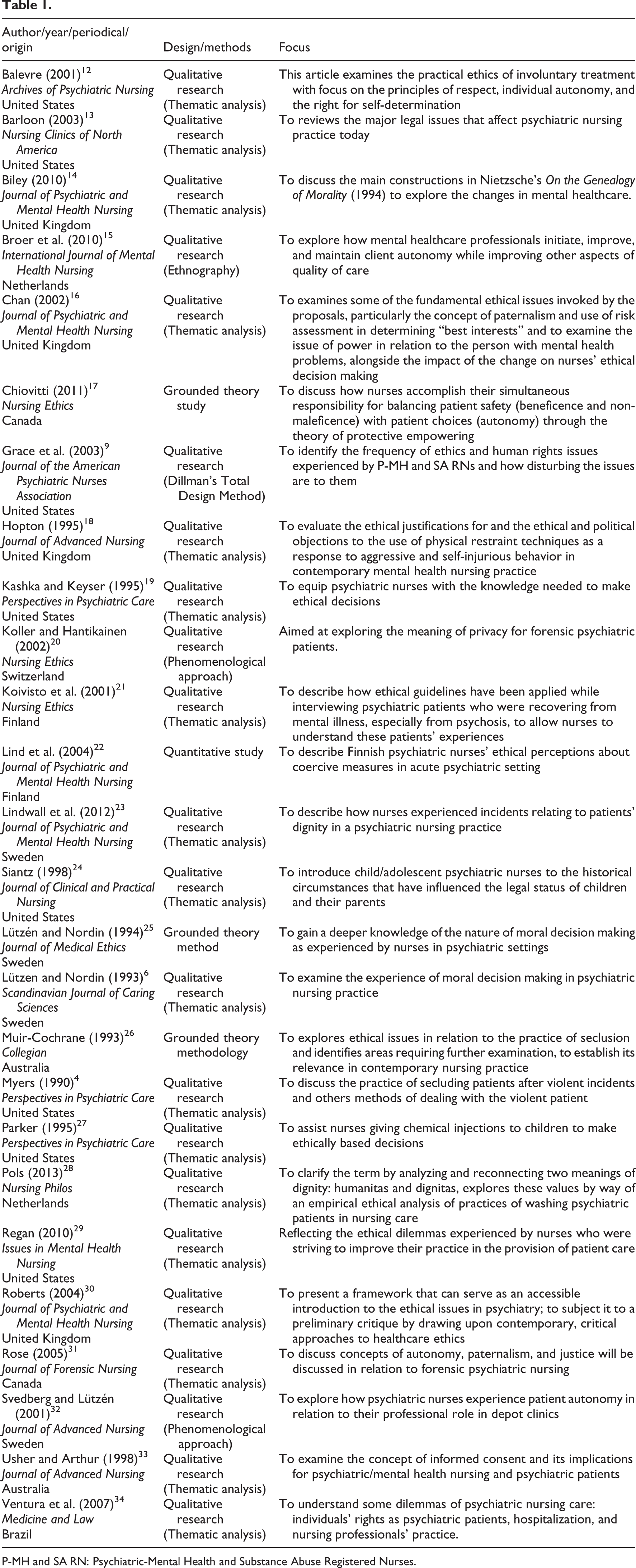
P-MH and SA RN: Psychiatric-Mental Health and Substance Abuse Registered Nurses.
The central theme which emerged from the selected literature was “Ethics and Human Rights Boundaries to Mental Health Nursing Practice,” which comprised the following subthemes: Nursing and mental illness: the limitation of autonomy and individuals’ rights; The value of dignity and the ethics of nursing care; Advocacy, informed consent, confidentiality, privacy, and mental health nursing practice; and Health services polices and legal aspects of psychiatric nursing practice and research. In the analysis process, a qualitative approach was applied to the selected publications in order to briefly describe the results obtained, elaborating a synthesis of the material analyzed.
Results
Considering the objective of identifying the human rights and ethical issues regarding nursing care to persons with mental illness, the analysis summarized the main results of the literature, which were articulated with the human rights theoretical framework, ethical principles, and mental health nursing practice (Figure 2).

Human rights and ethical issues regarding nursing care to people with mental illness.
The studies were conducted mainly in United States (30.8%), United Kingdom (15.3%) followed by Sweden (15.3%), Netherlands (7.7%), Canada (7.7%), Australia (7.7%), Finland (7.7%), Switzerland (3.9%), and Brazil (3.9%). The studies were published between 1990 and 2013. In 1990, only one study was published (3.6%); in 1993, two studies (7.4%); and 1994, one study (3.6%). In 1995, three studies were published (11.3%) and in 1998, two studies (7.4%). In 2001, three studies were published (11.3%), two studies in 2002 (7.4%), and two in 2003 (7.4%). In 2004, two studies were published (7.4%), and only one was published in 2005 (3.6%) and 2007 (3.6%). Three studies were published in 2010 (11.3%), one in 2011 (3.6%) and 2012 (3.6%), and one in 2013 (7.4%). Of the selected articles (n = 26), most are qualitative research (84.6%), grounded theory research (11.5%), and only one (3.9%) was classified as quantitative research.
The studies were published in 16 different peer-reviewed scientific journals. A total of 10 (38.4%) studies were published in Psychiatric Nursing journals and 3 (7.6%) studies were published in Psychiatry and Mental Health journals. The other 13 (50%) studies were published in Nursing and Medical journals, focusing on ethics and care.
Most of the studies aimed to discuss and explore ethical issues and nursing practice (61.5%), followed by ethical issues and decision making by nurses (26.9%). Besides that, there were studies approaching ethical issues and coercive measures (7.6%).
Discussion
Ethics and Human Rights Boundaries to Mental Health Nursing Practice
Mental health nurses play a key and valuable role in ensuring that their interventions are based on ethical and human rights principles. Considering that nurses are the professionals who provide direct care to patients, they are routinely faced with patients’ pain and suffering resulting from coercive treatments such as involuntary hospitalizations, and restrictions on movement involving seclusion and restraints. 29 Thus, in involuntary hospitalizations, mental health nurses’ practice requires overcoming the conditions of being a mere specialized technician within the service. In addition, physically restraining a patient is a human rights issue and should not be done without significant cause. 9 Therefore, nurses cope with the constant challenge of assuring the respect for the human rights of patients during their care. 34
Yet, mental health nurses seem to have difficulty engaging with the ethical issues in mental health, and with the common justification for those acts. 30 Ethical issues involving behavior control are centered on the conflict regarding how to consider the individual’s autonomy in situations involving a psychotic illness in which the suppression of autonomy may be rationalized in terms of the common good of ward community. 32 In this context, autonomous persons should be respected in their own right, and treated accordingly, rather than considered the means to an end of others. 26
Research results indicate that when nurses identify two opposing courses of justifiable action and are unsure about which alternative to choose, they experience an ethical dilemma. Although some articles selected for this review use the word “dilemma,” it is important to emphasize that philosophically a true dilemma is irresolvable. In this sense, there are very few true dilemmas, considering that most conflictual situations have routes of possible action, some of which may be better than others. In addition, in these cases, we also are able to gain more information and understand better the particularities of the situation. 35 Generally, the resolution of an ethical conflict is based on the determination of the patient’s “best interests.” 34 In this scenario, it is important to open a debate regarding possible solutions for this ethical conflict, with the purpose to enable nurses to function in a way that is morally acceptable to the profession, patients, and members of the public. 16
Furthermore, when nurses already know the right course of action but do not act accordingly because they feel powerless due to lack of support, institutional barriers, or legal limits, the ethical conflict can generate moral distress. Moral distress can also arise when nurses do not agree with a course of action chosen by the health team or other professionals. These conflicts can result from the nurses’ belief that a patient’s rights have been violated or when there has been confusion with respect to healthcare goals and direction. 29
Nursing and mental illness: the limitation of autonomy and individual rights
In everyday practice of mental health nursing, there are many examples of paternalism. 26,27,30 Generally, in healthcare settings, paternalism does not necessarily have a negative connotation. Based on the “Parens Patriae” doctrine, paternalistic actions are supposed to be those that serve the patient’s best interests when they are unable to protect themselves. 36 However, according to the articles analyzed in this review, paternalism corresponds “to the policy or practice on the part of people in positions of authority of restricting the freedom and responsibilities of those subordinate to or otherwise dependent on them.” 37 Within the mental health professional–patient relationship, as “patient,” a person is generally required to respect the health professional authority, listening and accepting the medical instruction. In addition, there is an expectation that patients must respond with gratitude for any attention given. 27,30
Patients with mental illness are dependent upon psychiatrists, nurses, and other mental health professionals for validating their experiences, and will often be deemed to be “psychologically well-adjusted by those mental health professionals insofar as they accept the diagnoses and treatments imposed upon them.” 18 This experience may be compounded in psychiatry, as the person may have already had a history of being a “patient” and of experiencing negative consequences regarding attempts to exercise autonomy. 30
Autonomy results from freedom of choice or “the right or condition of self-government.” The understanding of autonomy has acquired different meanings such as of privacy, freedom of will, individual choice, and self-governance. 19,30 The healthcare professional’s rigor to pursue autonomy as an end state reflects the value given by that health professional to paternalism. Generally, professionals act paternalistically based on the assumption that their actions may allow the patient to live a more autonomous life in the future. 19
In sum, paternalism is a result of an exercise of power within nurse–patient relationships. In dealing with paternalism, it is also important to consider how patients’ race, age, gender, education, and socioeconomic class may contribute to their “powerlessness.” In addition, nurses’ understanding about mental illness may also impact how they identify, explore, and respond to ethical situations involving mental health issues. Roberts 30 affirms that if mental illness is understood as an “objective fact” or some form of bodily disease, paternalism will be exercised by means of interventions aiming at alleviating the human suffering of those “afflicted” with that disease. On the contrary, if mental illness is linked to the belief that persons are deviating from a culture’s values and norms, then acts of paternalism may be driven toward the maintenance of the cultural status quo and therefore, they become political acts. 30
Autonomous decision making is a basic human right, and patients with mental illness can be considered competent to make autonomous decisions by themselves. 21 The principle of respect for autonomy involves the patients’ right to make decisions regarding the health services they receive. 27,31
The literature is far from a consensus on this theme and opinions vary on the universality of the need for autonomy. 15 According to Kant, autonomy comprises a responsibility and a right, both of which are guided by reason. Thus, individuals have the responsibility, through the capacity of reason, to know what is morally required of them. However, in psychiatry, patients’ autonomy may be threatened as the illness often compromises reason, and generally, the person with a mental illness is not considered autonomous and decision making is revoked. 31 As patients’ capabilities for making decisions may vary, mental health nurses face the problem of balancing their level of control with their aim to provide their patients’ choices. 17
This conflict is even more intense when nurses provide care to children with mental illness because they are not legally autonomous until a certain age. 27 In most cultures, children and adolescents are considered legally incompetent to make treatment decisions for themselves, and parents or legal guardians have the right to make such decisions. Nonetheless, there are exceptions in some jurisdictions for minors to consent for certain types of treatment, such as prescribing contraceptives, treatment for sexually transmitted diseases, suicide prevention, and substance abuse. 13 In these situations, mental health nurses combine the responsibility of advocating for the rights of the child at the same time as respecting parental obligations and rights. 38
An argument in favor of paternalism may emphasize the utilitarian principle that decisions involving the control of patients’ behavior may be taken to benefit more people than the individual patient, and seclusion may be justified accordingly. It is important to consider, from an opposing perspective, that the negative consequences of forced treatment may include further alienation from treatment and possible risk of a violent outbreak requiring the use of restraints and seclusion. 12 Acceptance of seclusion can be based on the idea that it can assist the patient to gain control over his or her aggressive behavior, through the means of reducing different types of sensory stimuli, providing a safer environment and removing frustrated social interactions. 4 In spite of these justifications, the use of behavior control is questioned as this treatment deprives patients with mental illness of their fundamental right to choose. 26,27
When analyzing mental health professionals’ choices between paternalism and autonomy, some authors affirm that maintaining or improving the patient’s autonomy may result in problems at different mental healthcare settings, as mental illness may diminish, to varying degrees, a person’s capacity to choose. 15,30 In this context, a study with members of a quality-improvement collaborative network explored how mental healthcare professionals initiate, improve, and maintain patients’ autonomy while improving other aspects of the care provided. Four approaches to autonomy were identified: “professionals removed constraints to autonomy and passed initiative to patients; professionals made an active effort to learn and support patients’ preferences; patients were given opportunities toward independent lifestyles; professionals tried to normalize their relationship with patients.” Therefore, improving or modifying the relationship with patients may also be a goal within an autonomy framework. 15
Limitations regarding individual rights must always be considered a serious deviation from the standard of care. It can be only justified when no less restrictive means are available to keep the patient safe and preserve justice and the rights of others. 29 According to a study carried out in Finland with 170 psychiatric nurses from acute wards in five psychiatric hospitals, nurses perceived coercive measures as ethically problematic. Among these measures, nurses emphasized the implementation of forced medication (18%), four-point restraints (16%), and patient seclusion (11%). The study recommended that supporting nurses’ capacity to discuss ethical dilemmas is important to base an informed healthcare practice. 22
Therefore, there is a need for more discussions among mental healthcare professionals regarding problematic violations of individual rights such as loss of autonomy, disregard of self-determination, and disrespect. In some cases, the decision to hold and treat patients against their will is related to the potential danger of having this individual back into society. Although dangerousness is, for the most part, a subjective concept, it is still considered “behavioral health law standard” in many countries. In this perspective, stereotyped ideas regarding “dangerousness” continue to condemn the freedom of patients with mental illness. 16,12
Another issue involving the limitation of autonomy of persons with mental illness is the persuasion of patients to take medication, which may be very coercive, even if physical force is not implemented. In these situations, the use of informal coercion may be considered part of a mental health nurse job description, in spite of inducing negative feelings in patients and discomfort in nurses. 22 Coercion can be formal, informal, and/or perceived. In some cases, it may provide a sense of safety for patients, although it can also cause feelings associated with fear and disempowerment. As nurses have the responsibility to protect the human rights of patients, it is important for them to be aware of the potential adverse effects of situations in which informal coercion is underestimated. 39
In addition, nurses must be properly trained in safe and humane methods when manual restraint is used. According to human rights laws, “restraint of a severely distressed and disturbed person is only justified as long as the method of restraint did not involve inhuman or degrading treatment.” Thus, proactive therapeutic strategies based on less damaging forms of expressing frustration and anger may be a better response to a disruptive behavior than using reactive strategies such as physical control and restraint, which must be seen as a last resource. 18
Yet, there are some examples of involuntary hospitalizations in which patients calmly refuse medication, therapy, or other psychiatric treatments, but due only to noncompliance, they are kept in more restrictive units. In these cases, hospitalization can become an incarceration while the patient is waiting for the review panel’s hearings. This situation opens up space for discussions, especially regarding the practical ethics of involuntary treatment interlinking the principles of respect for patients’ individual autonomy versus their right to self-determination. 12
Based on the right to self-determination, one must emphasize the patient’s right to refuse treatment. In addition to concerns about side effects, there are multiple reasons patients can use to refuse medication, including denial of their mental illness and the stigma involving taking a psychotropic medication. In many countries, patients have the right to refuse medications unless there is a court order obligating them to take the medication or in emergent situations and with limited use. This is a change from previous practices when it was accepted that a patient who was involuntarily hospitalized did not have decision-making capacity and was not able to refuse any kind of medication. Nurses are responsible to assess and objectively document in such cases. 22
A phenomenological study aiming to explore how psychiatric nurses experience patient autonomy in relation to their professional role in depot clinics found that the interventions were related to the nurses’ experiences regarding patients’ attitudes to medication and their ability to make responsible choices about medication. The interventions were most dependent on the nurse–patient relationships. If they were brief, interventions were focused on the injections. On the contrary, if nurses were considered the key workers for patients, the interventions fostered a collaborative relationship among them. 32
The issues regarding restriction of autonomy and individual rights of persons with mental illness are even more complex in forensic psychiatry, which includes the criminal justice system and the provision of care to offenders with mental illnesses, their families, and communities. Forensic psychiatric services vary across a continuum of restriction and security, from maximum secure programs to community-based outpatient programs. In all these situations, forensic psychiatric patients are subject to compulsory psychiatric treatment and lack autonomy due to incarceration. However, acknowledging the influence of social relationships may change nurses’ perception of autonomy, enabling them to view the patient as an interdependent person, rather than only the sum of his or her criminal offense and risk. For nurses, understanding their own positionality, history of oppression, and its influence on their autonomous decision-making skills facilitates their reflectiveness and their attitudes regarding their sense of autonomy in the patient’s daily treatment and rehabilitation decisions. 31
In order to preserve integrity, nurses have the duty to remain consistent with their personal and professional values as well as to accept compromise only in the case it remains an integrity-preserving compromise (Figure 3). Therefore, when a particular intervention is morally objectionable to the nurse, whether intrinsically so or because it is inappropriate for the specific patient, or where it might jeopardize both patients and nursing practice, the nurse is justified in refusing to participate on moral grounds.
29
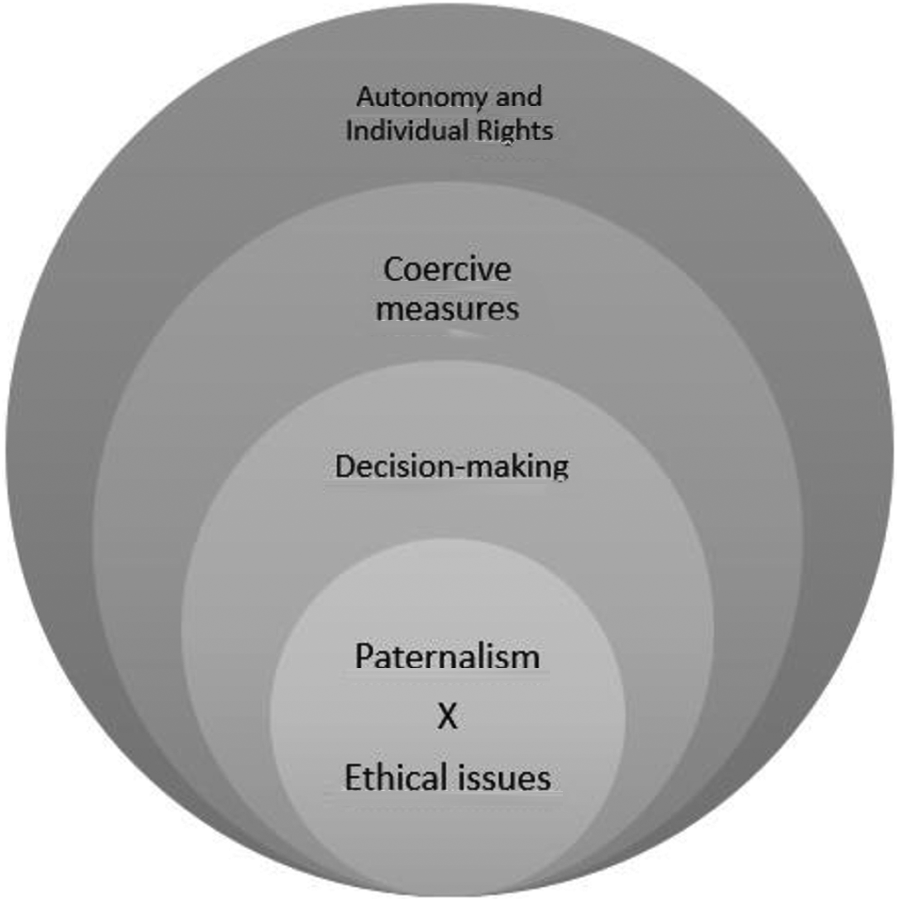
Relationship between paternalism and ethical issues in the nursing care provided to persons with mental illness.
The value of dignity and the ethics of nursing care
Dignity is an intrinsic value of the right to health. In this sense, it is necessary to understand the meaning of human rights, which demands full citizenship and dignity for all. 40 Dignity is related to the values of freedom, equality, autonomy, and interdependence. These values are central to the normative approaches regarding nursing care to persons with mental illness. 28 In this context, the ethics of care is especially relevant to mental health nursing, in which interpersonal relationships are central and are themselves the means for treatment. Awareness about the person with mental illness’ feelings regarding the proposed healthcare intervention introduces significant considerations regarding ethical reasoning. A combination of reason and emotion is, therefore, essential for an ethical decision making that can be considered appropriate. 30
Patients with mental illness are in a vulnerable situation and although decisions concerning their “right” medical treatment must be based on professional codes of ethics, it may not always be possible to make “good” nursing care decisions only considering rules and regulations. Mental health nurses deal with the need to be aware of patients’ helplessness and loss of privacy, as well as their total dependency on others for basic needs. Building upon their own experience and practice in dealing with mental health patients, these nurses may be able to increase their understanding beyond the law, focusing on the connection between patients’ limited self-choices and their consequent vulnerability. 9,25,27
Thus, dignity is a concept in nursing, which has been increasingly emphasized in Sweden’s health policy and professional documents over the past decades. 22 In this perspective, nurses must accept accountability for actions in order to safeguard their patients’ human rights. In order to do so, nursing care involves acknowledging the values of the patient and respecting their choices regarding what is important in their lives. In this context, the results of a study on psychiatric nurses’ experiences regarding patient’s dignity indicated two types of dignity: “preserved dignity, when caregivers allow themselves to be touched by patients’ stories; and offended dignity, when caregivers create powerlessness, abusing their power and punishing their patients.” 22
Respect for human dignity is also essential in safeguarding privacy. A study based on a phenomenological approach conducted at a Swiss psychiatric clinic aimed at exploring the meaning of privacy for forensic psychiatric patients. Authors described the meaning of privacy as a dynamic process. The four functions of privacy—personal autonomy, emotional relief, self-evaluation, and protected communication—were considered important strategies to maintain and restore personality, 20 especially in the case of persons with mental illness (Figure 4).

Ethics of nursing care and human rights in interpersonal relationships between nurses and people with mental illness.
Advocacy, informed consent, confidentiality, privacy, and mental health nursing practice
Results of a study with RNs with the purpose to understand human rights and ethics issues experienced by them demonstrated that nurses have a clear advocacy role to protect patients from harm and to promote patients’ well-being. 9 This is even more crucial in cases involving child psychiatric nurses as they play a dual advocacy role focusing on the child as well as on the parents. In this process, it is important for nurses to consider “(1) the child’s right to due process in decisions concerning his or her future, (2) parental rights and responsibility in seeking care which guarantees the best interests of their child, and (3) the nurse’s ethical responsibility during the psychiatric admission of a child.” In addition, nurses may base their decisions on the principles of beneficence, non-maleficence, and justice. The assumption of the personhood of the child will also help the nurse to determine a course of action during a psychiatric admission, which may support the child and the parent. Therefore, the nurse’s role in promoting beneficence includes a detailed assessment of procedures and information collected and used during admission aiming at determining the treatment needed. 38
In all these situations, nurses must be aware of different contentious issues involving psychiatric nursing care and, as a consequence, become more proactive in the protection of patients’ rights. 33 However, nurses may have the fear of being harmed and this can cause a negative impact on the care provided as they can be less proactive to advocate for patients’ rights. Also, when there are issues related to physical safety due to a disease process, such as in many psychiatric disorders, this could potentially result in discrimination against the patient. 9 Education programs for nurses may be a key strategy to reduce the use of seclusion through preventive interventions. 4
In this perspective, informed consent is crucial in psychiatric practice for the protection of patient’s rights. This must involve an environment of education, shared information, communication, and decision making in order to assure individual dignity. 33 Informed consent is the process by which information is shared about treatment options, alternatives, and risks. Nurses are often involved in this process, which can include written information and the patient being asked to sign a form. 13 Three elements are essential to the consent process: “information disclosure, competency, and voluntariness.” These elements have been reformulated in clinical psychiatry in order to involve abilities to “communicate a choice, understand relevant information, appreciate the situation and its consequences, and manipulate information rationally.” 19 Nevertheless, it is important to emphasize that the issue of informed consent depends upon the person’s competence to consent. 33
In addition, psychiatric nurses are responsible for maintaining the confidentiality of information shared by patients with the treatment team and within the medical record. Considering the nature of psychiatric care, patients must trust that the information shared will be only used for the treatment itself and will not be disseminated to other parties. Privileged communication is a right of patients that protects information from being shared in a court of law. 13
Over time, the boundaries of mental health are changing with the purpose to assure a more humanized practice. 14 “Moral sensing” is a capacity for moral knowledge that is exercised in a specific situation, integrating practical experience, contextual knowledge, intuition, and the genuine feeling of doing good for the patients. This process of integrating all known aspects is prior to action. 25
In these contexts, one of the main goals for nurses is to encourage patients to act autonomously, at the same time as defending their well-being and the exercise of the right to self-determination “within the bounds of therapeutic environment.” Applying critical thinking to bioethics keeps up the standards of the professional and also enables nurses to protect the rights of their patients. 4
The ethics of care stresses the importance of care and caring within nurse–patient relationships. This issue is particularly important to mental health nursing in which interpersonal relationships play such a central role and are themselves means of the treatment. Mental health nurses build relationships with patients who are vulnerable and in need of care. Therefore, an appropriate ethical response to those clients is to be involved with their needs rather than only considering general principles. Thus, rather than asking what mental health nurses should do, virtue ethics suggests that the guiding question should be “what type of person must the mental health nurse be in order to make ethically correct decisions?.” In particular, it suggests that mental health nurses adopt and develop virtues such as commitment, empathy, and trust in order to cultivate a character that will ensure ethically appropriate decision making. 30
From this discussion on the ethics of care emerge dilemmas on how mental health nurses can empower the users of health services. In this context, a protective empowering can serve as the basis for advocacy for the quality of practice environments, impacting education, practice, policy as well as future research studies. 17
Mental health nurses must be ethically grounded because of the potential abuses that exist in this specialty. Therefore, when nurses are not sure about their course of action regarding specific situations, it is important for them to discuss their concerns with other members of the healthcare team. Often, these feelings are “a clue that ethical concerns are present” and voicing such feelings can lead to awareness that the situation has competing ethical values (Figure 5). 19
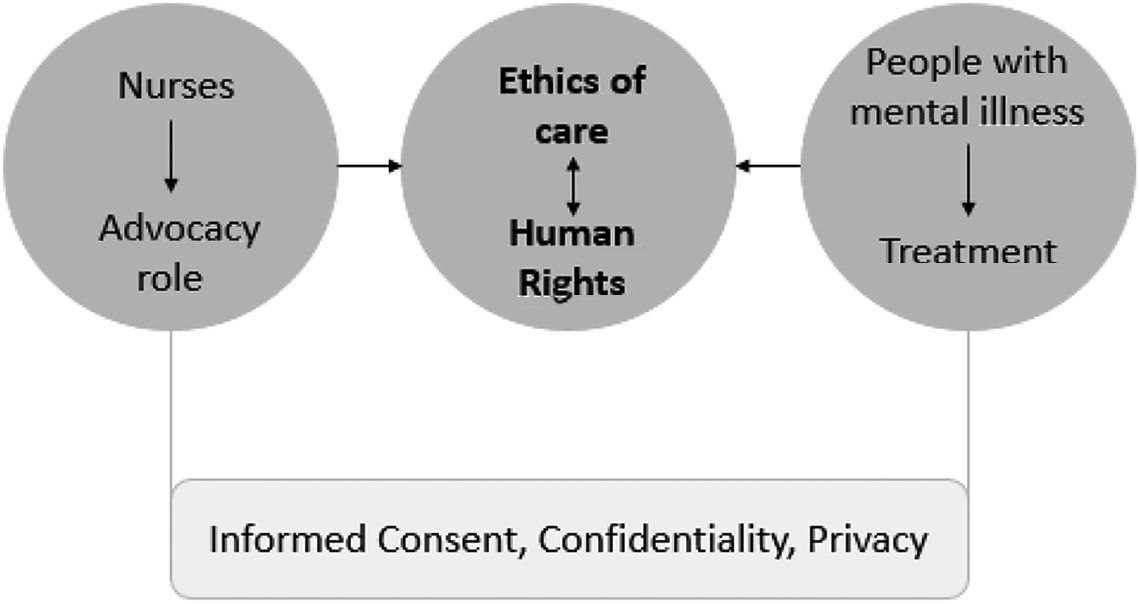
Ethics of care and human rights in the mental health nursing practice.
Health services policies, legal aspects of psychiatric nursing practice and research
The legal parameters of professional practice are based on different sources. Therefore, there are several measures to judge nursing practice. 22 Patients have the right to make choices about tests, procedures, and treatments to be used in their care and nurses are expected to respect this right. 9 The American Nurses Association published the Scope and Standards of Psychiatric-Mental Health Nursing Practice in 2000, “identifying specific standards of practice for nursing activities and criteria for measuring these standards.” Similarly, the American Psychiatric Nurses Association (APNA) and the International Society of Psychiatric Nurses (ISPN) have published standards to guide practice. With respect to patient’s rights, psychiatric treatment must be provided aiming at allowing the most freedom and the least restriction to meet the particular needs of a patient. Also, seclusion and restraint must be used only when other less restrictive means have been considered and ruled out. In addition, documentation must support the need for these measures, confirming that other alternatives were considered and that nurses are responsible to ensure standards and that seclusion and restraint are not being used for staff convenience or as threats and punishment. 13
Within nursing codes and standards of ethics, promoting patient’s choice (autonomy) must be balanced with ensuring patient’s safety through limits to patient choices (beneficence and non-maleficence). Nursing codes and standards of ethics in Canada adopt a patient autonomy-oriented approach to ethics. The ethical principles of non-maleficence, respect for autonomy, and beneficence are included in nursing codes and standards of practice, addressing the patient’s well-being. Together, they correspond to the main theme of balancing nurses’ duty to respect patients’ autonomy and choices with their duty to protect patients and others from harm. 17
The nursing profession articulates nurses’ rights and responsibilities in terms of duty of care. In a study developed in Australia, nursing clinicians identified their duty of care in terms of assuring the ward safety and their role as gatekeepers of control on the closed wards. The moral principles of maximizing benefits (beneficence) and minimizing harm (non-maleficence) were used to justify the seclusion of individuals. The ethical dilemma for clinicians lied in “their responsibility to provide a safe ward environment while still respecting the integrity of an acutely disturbed individual.” 26
Within international legal instruments, the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) is based on a social model of disability, which includes mental illness. Disability is a term used with an inclusive meaning, incorporating all forms of physical, psychosocial, and learning disabilities. However, the UNCRPD poses challenges to the mental health sector, particularly in relation to the common practices of detention and treatment without consent. Thus, nurses working in education, research, and clinical practice must be familiar with the scope of the UNCRPD in order to review their current ethical frameworks for the justification of compulsory treatment. The presence of mental illness, even when linked to the criteria of dangerousness, is not enough; indeed, it can be held to be discriminatory. 41
Findings from several studies have suggested the existence of unexplained differential decisions on imposing compulsory psychiatric treatments on patients from different ethnic and socioeconomic groups. These findings suggest that sufficient attention has not been given to justice as an ethical principle. 41 There is an urgent need to explore non-coercive alternatives to compulsion in all forms, and to address the social conditions and consequences of mental illness. 42
Another important topic concerning nursing practice is the development of research and the ethical guidelines used to interview psychiatric patients who were recovering from mental illness, especially from psychosis, aiming at allowing nurses to understand these patients’ experiences. In addition, as psychiatric patients are vulnerable, their participation in research involves ethical dilemmas, such as legal capacity to consent, voluntary consent, freedom of choice, and sufficient knowledge and comprehension. Although there are guidelines concerning human research with the purpose to protect the human rights and dignity whenever research participants are vulnerable persons or their capacity to consent is limited, there are no special regulations to guide research involving adults with any mental illness. The capacity to consent can be considered one of the main questions when the participants are psychiatric patients recovering from a psychotic illness, because these disorders may limit their ability to understand correctly what comprises their involvement in the research. Therefore, there is need for better guidance to define the capacity to decide in the research context and to outline procedures for assessing such capacity (Figure 6). 21
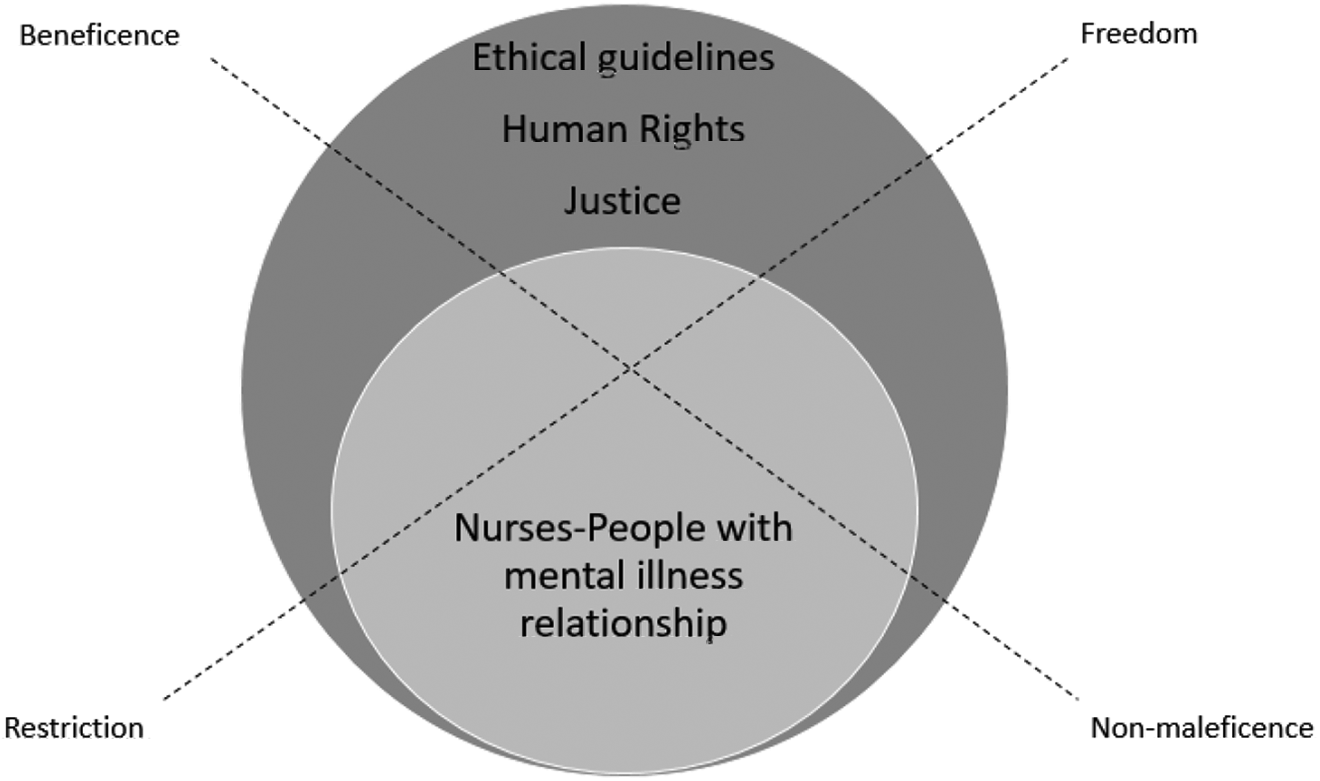
Relationship between ethical principles and psychiatric nursing practice.
Conclusion
Results from this scoping review present a foundation to better understand the relationship between ethics and human rights in the nursing care provided to persons with mental illness, reflecting issues on nursing; mental illness; limitation of autonomy; individual rights; value of dignity; ethics of nursing care; advocacy; informed consent; confidentiality; privacy; mental health nursing practice; health services polices; and legal aspects of psychiatric nursing, practice, and research.
Mental health nurses play a key and valuable role in ensuring that their interventions are based on ethical and human rights principles. Nurses cope with the constant challenge of balancing human rights with their practice, with a view to attending the human needs of their patients or, better, of the human beings who are under their care at that moment. Based on their knowledge regarding ethical and human rights principles in mental healthcare as well as in the exercise of moral agency, mental health nurses are better prepared to deal or mitigate the challenges evidenced in this review. In addition, mental health nurses can lead the discussion about these challenges at the healthcare settings and with patients, promoting a better understanding of the limitations and potentials of the different choices made during mental healthcare.
Protecting human being’s dignity is a fundamental value, although several studies inform that dignity is not always promoted within mental health services. Therefore, mental health policy affects human rights, and human rights violations affect mental health. In sum, the positive promotion of mental health and human rights, based on ethical values, are mutually reinforcing.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.