
Abstract
The empathy of nurses is associated with self-care and self-compassion, which may enhance the quality of the nurse-patient relationship. Yet, research on the empathy of nursing staff has mostly used cross-sectional designs, which cannot capture the degree of empathy changes over time. To explore changes in empathy among nurses in China from 2009 to 2018. A cross-temporal meta-analysis was used to examine continuous changes in the empathy of nurses. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were used to conduct this cross-temporal meta-analysis of 57 samples of nurses in China who completed the three subscales (perspective-taking, compassionate care, and walking in the patient’s shoes) of the Jefferson Scale of Empathy-Health Professionals from 2009 to 2018 (N = 13,825). This meta-analysis was conducted following good scientific practice in every phase, and approval by ethics committees was not required according to the local regulations in China. The findings suggest that the nurses’ mean total scores of empathy and perspective-taking on the Jefferson Scale of Empathy-Health Professionals declined significantly over time, but the trend in compassionate care and walking in the patient’s shoes was not significant. No significant changes were found in the overall empathy or the three dimensions of empathy of the nurses in the Eastern region across time, whereas a significant decline was found on the total empathy and perspective-taking scores of the nurses in other regions (i.e. the Central and Western regions). The mean total score of empathy and walking in the patient’s shoes of the nurses who worked in the intensive care units showed a significant decrease over time. Furthermore, these findings indicate that the empathy of Chinese nurses has decreased steadily over the past 10 years. High levels of empathy can effectively reduce healthcare risks, errors, and disputes among nursing staff and enhance patient satisfaction and well-being.
Keywords
Introduction
With the transformation of modern health concepts and the development of medical models, patients’ expectations of medical staff have risen. During the treatment process, more patients are beginning to voice their opinions of and preferences for service quality and the nursing environment. The field of modern nursing has shifted from the disease to the patient as the focus of care (“patient-centered care”), with greater attention paid to the nurse–patient relationship. A recent study found that a good relationship between nurses and patients can create a working environment in which both parties provide mutual psychological support so that the nurse can understand the patient’s needs better and ultimately formulate effective nursing interventions. 1 This also helps to improve the professional identity and subjective well-being of nurses. 2 The establishment of harmonious relationships between nurses and patients, improvements in the quality of nursing care and nurses’ level of empathy are closely related. A recent study found that a higher level of empathy is associated with a higher level of professionalism, better observation and communication skills of nurses, which can effectively reduce healthcare risks, errors, and disputes among nursing staff, thereby improving patients’ satisfaction. 3 Therefore, we asked how the empathy of Chinese nurses has changed over time, which was the focus of this study.
Background
Empathy refers to the perception and experience of the emotional state of others and the ability to understand and analyze the emotions of others. This is reflected in nurses’ understanding of patients’ true problems and needs. 4 Some researchers 5,6 divide empathy into two categories: emotional empathy and cognitive empathy. Emotional empathy refers to the ability of individuals to develop rapport with others. 7 Cognitive empathy refers to the ability of individuals to recognize and understand other people’s emotions and attitudes. Although there are many tools to measure empathy, most of them are designed to identify empathy in the general population. However, the day-to-day encounters of nurses working in clinical settings with patients who require acute care for medical illnesses are different from the daily encounters of the general population. Thus, the accurate measurement of empathy in nurses working in clinical settings requires a valid instrument that taps empathy in this clinical context. Therefore, Hojat et al. 8 developed the Jefferson Scale of Empathy-Health Professionals (JSE-HP), which was translated to Chinese and revised by An. 9 The Chinese HP version was used in this study to assess the empathy of nurses on three dimensions: perspective-taking, compassionate care, and walking in the patient’s shoes. A large number of studies have shown that the JSE-HP has good reliability and validity and is widely used in China and elsewhere. The scale has demonstrated evidence of substantial convergent and discriminant validity, and measures of its internal reliability across different studies range from 0.750 to 0.836. 10,11 The JSE-HP is designed specifically for medical staff and can accurately measure the empathy of clinical nurses. 4,12,13
There has been a growing concern about the relationship between medical staff and patients in recent years, so China has promoted the development of measures of medical service quality, which has led researchers to broaden their research on empathy. Studies have found that nurses face increasing work pressure and have a low sense of personal accomplishment, which increases their likelihood of developing serious job burnout. This leads to a continuous decline in empathy and an increase in conflicts between nurses and patients. 14,15
The effects of work stress are especially evident among nurses who work in the intensive care unit (ICU). Studies have reported job burnout is common among these nurses because they work in an intense environment, with high work pressures and high workloads. 16 Compared to nurses in other departments, ICU nurses also have poorer mental health, which has shown a downward trend over the years. 17
However, other research provides different perspectives. For example, Yang et al. 18 and Zhang 19 found that the level of empathy of nurses is higher than in past years. The phenomenon is attributable to nurses receiving more attention from their managers, the implementation of active and effective ways to cultivate the humanistic qualities of nursing staff, and systematic training to enhance the empathy of clinical nurses, all of which contribute to improvements in empathy. However, consensus has not been reached on whether the empathic ability of nurses improves with year. Besides, previous research on the empathy of nursing staff has mostly used cross-sectional designs, which cannot accurately capture changes in empathy over time among Chinese nursing staff from the perspective of a large longitudinal sample. The inferences that can be drawn from these studies on the status of nurses’ empathy are based on small samples of data collected one time from nurses working in one department in one region of China. 1,13– 15 Although one cross-temporal meta-analysis (CTMA) reported increased empathy levels in Chinese college students between 2009 and 2015, it included 18 studies conducted with only students, which cannot provide a true representation of trends in the nursing profession. 20 Therefore, we conducted a CTMA to explore changes in the empathy of Chinese nursing staff in the past 10 years and to analyze the factors affecting this trend to close this research gap in China.
A CTMA was first used in a study by the American scholar Twenge. 21 The CMTA uses a cross-sectional “design” to examine psychological differences or changes associated with long time-spans and historical developments. Individual studies are examined systematically in chronological order, and historical changes in cross-sampling are discussed from the perspective of large longitudinal samples. 22 The Chinese scholars Xin Ziqiang et al. introduced this method in their studies on anxiety, 23 trust, 24 loneliness, social support, 25 and other psychological indicators that were measured over a series of empirical studies. Their research found that these psychological indicators showed obvious changes each year. Therefore, this study was conducted to examine changes in empathy yearly.
Methods
We examined changes in the empathy of Chinese nurses from 2009 to 2018 using the meta-analytic technique known as CTMA. In contrast to a traditional meta-analysis, a CTMA does not compute an effect size for each study. Instead, correlations between the mean scores on a measure and the year of data collection are analyzed and weighted for sample size to assess changes in a particular measure over time. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used as a guide for conducting this study and reporting the results.
Instrument measuring empathy—the JSE-HP
Among the various instruments measuring empathy, the JSE-HP has been the most widely used. This study examined research that used the JSE-HP, which was developed by Hojat et al. 8 and revised and translated by An. 9 The instrument has 20 items, 10 of which measure perspective-taking, 7 items measure compassionate care, and 3 items measure walking in the patient’s shoes. The items are rated on a 7-point scale ranging from agree (1) to disagree (7). Higher scores indicate higher levels of empathy.
Inclusion and exclusion criteria
The included papers had to meet the following criteria to be selected for our meta-analysis:
An article had to be empirical research; theoretical articles and literature reviews were excluded.
A study had to use the JSE-HP and report the sample size and mean scores of its three dimensions.
All study samples had to be independent. If the same data were published more than once, the larger study or the study with more details was analyzed.
All of the study samples were Chinese nurses; doctors and other staff members were excluded.
All the studies’ sample sizes were reported.
After the first author and the corresponding author identified the keywords through discussion and negotiation, the other authors searched the literature using the keywords. The inclusion and exclusion of studies were determined after they were discussed.
Literature search
Literature searches were conducted in the China National Knowledge Infrastructure (CNKI) (www.CNKI.net), Wan-Fang (www.WanFangData.com.cn), CQVIP (www.cqvip.com), and China Doctor/Master Dissertations full-text databases. The language for articles searched was restricted to Chinese. The electronic searches were supplemented with manual searches of the reference lists of the retrieved articles.
The terms “Nurse,” “Nursing,” “Doctor and Nurse,” “Empathy,” “the Jefferson Scale,” “JSE-HP,” and “JSE” were used as keywords in full-text searches. The JSE-HP was revised in 2008; therefore, the search years began in 2008. After screening, a total of 57 studies were collected from 2010 to 2019 that included the year of data collection and measured participants’ empathy (Figure 1). According to the calculation requirements for cross-temporal meta-analyses, the year of data collection was coded as 2 years prior to publication if the date was not reported in the study. 21,22 The 57 studies involved 13,825 nurses, as shown in Table 1.
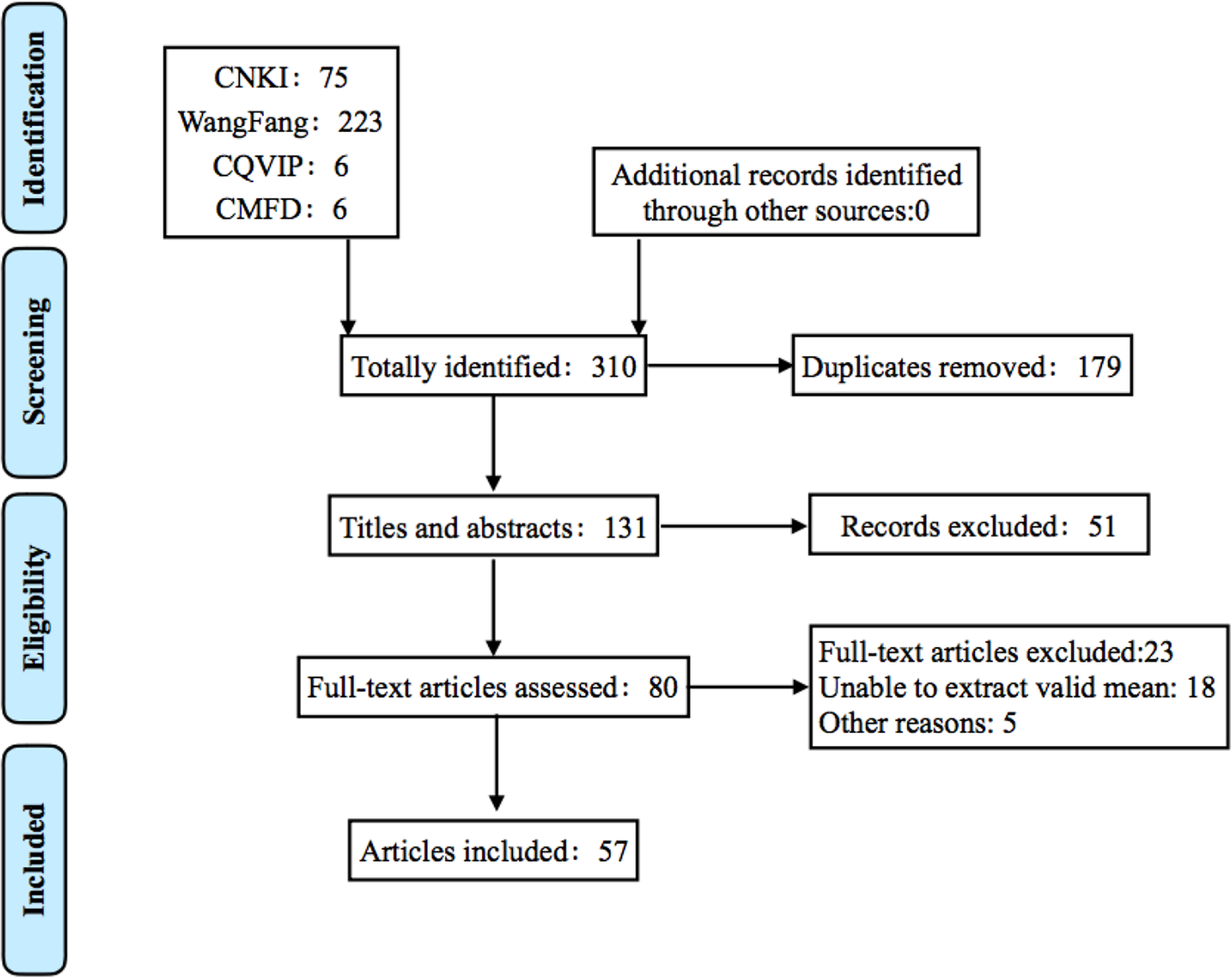
Flow chart of the literature search and screenings.
Characteristics of the included studies.
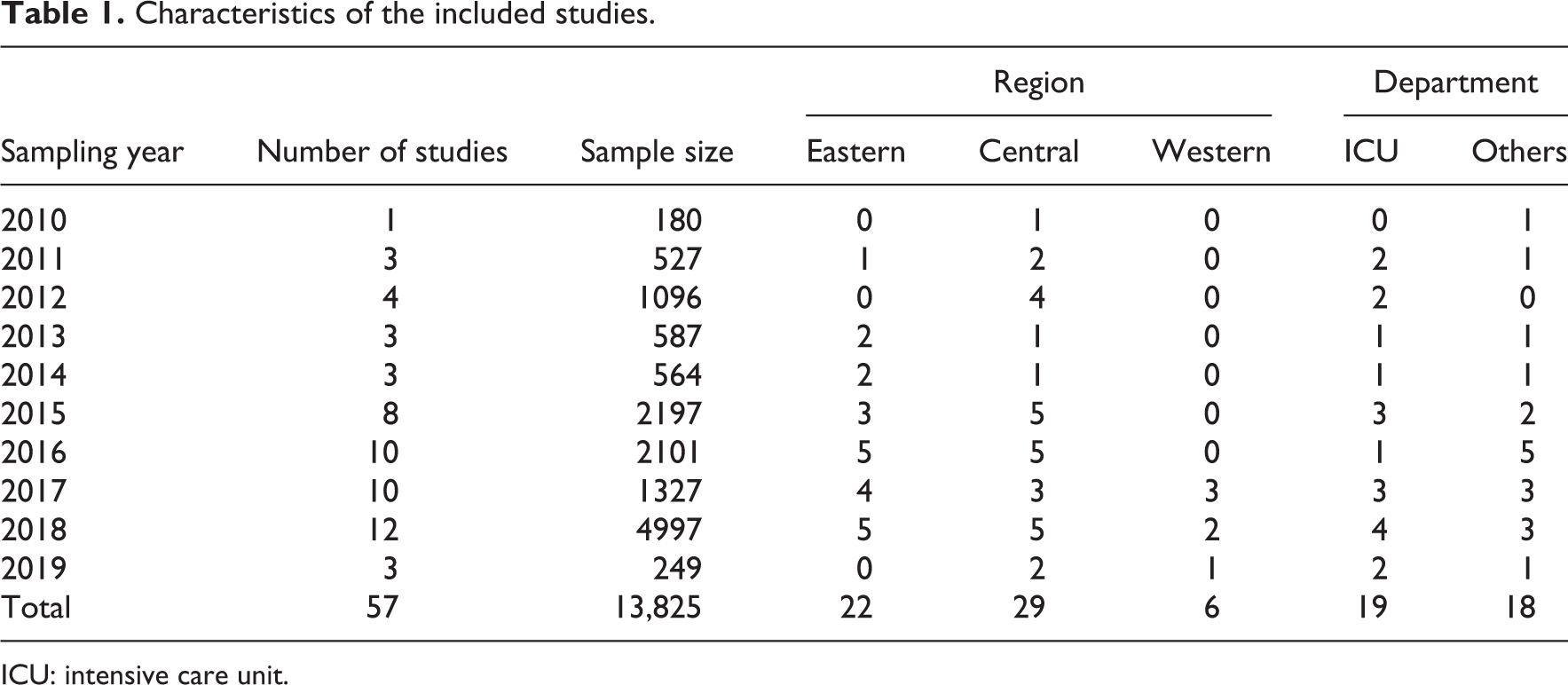
ICU: intensive care unit.
Data coding and analysis
In accordance with the guidelines for cross-temporal meta-analyses, the 57 studies were coded independently by two experienced graduate students in nursing. Ambiguous coding situations were resolved by the first author to achieve a 98% consensus of the two coders.
The following information was extracted from each study: year of publication, year of data collection, sample size, and the total scores, mean scores, and standard deviations of each empathy dimension.
The following information was recorded to analyze the data pertaining to the variables: department and region. The departments included in the studies were coded as ICU and other (psychiatry, obstetrics, orthopedics, and so on). The regions included in the studies were coded as Eastern, Central, and Western. The Central and Western regions of China were merged into a single category (Other regions) for the analysis because (a) they have similar levels of economic development, (b) they belong to important development areas, 26 and (c) there were only six studies from the Western region (Table 1).
Other information recorded in the database included sex ratio, professional title, and types of journals.
For those studies that provided scores on the three JSE dimensions but not the total JSE score, we calculated the total mean and standard deviation using the following two formulas (xi
, Si
, ni
,


Results
Correlations between year and mean empathy scores
The overall annual trend in Chinese nurse’s empathy from 2009 to 2018 was first explored using scatterplots of the data’s fit to a linear trend in the empathy scores. The results, which are shown in Figures 2– 5, indicate that the mean total score for overall empathy and the scores of the three empathy dimensions decreased somewhat year by year.
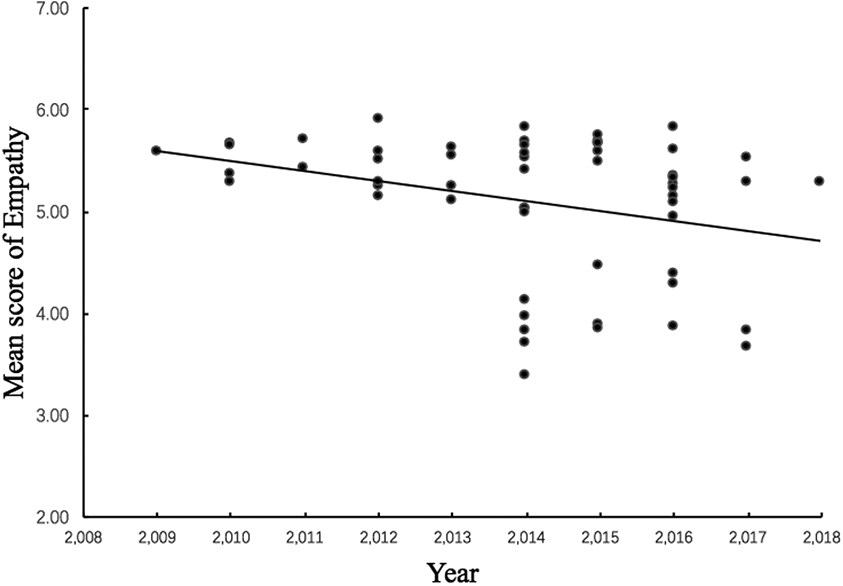
Changes in nurses’ total empathy score from 2009 to 2018.
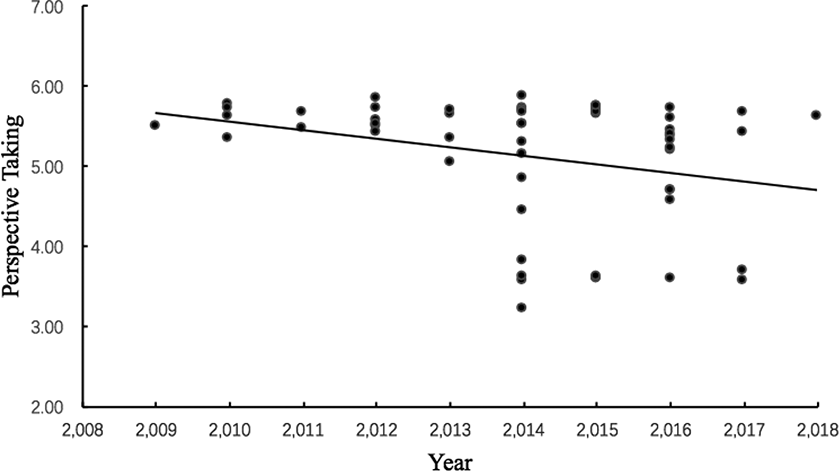
Changes in the empathy dimension of perspective-taking from 2009 to 2018.
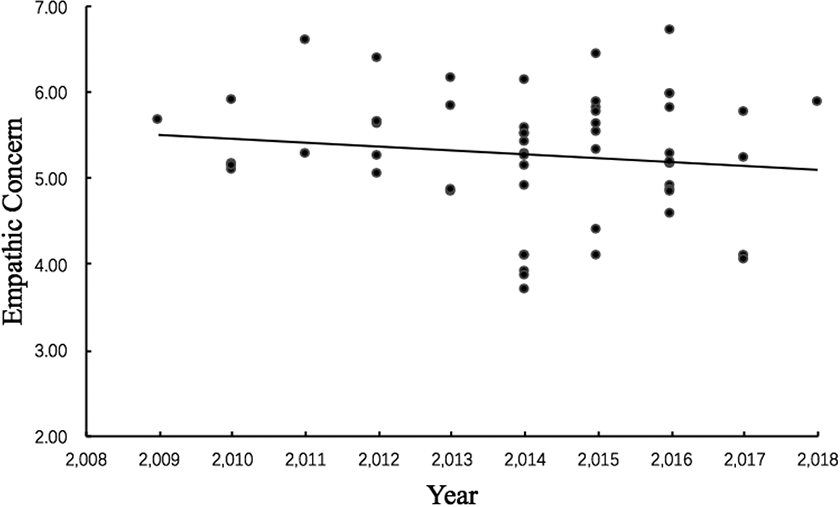
Changes in the empathy dimension of empathic concern from 2009 to 2018.
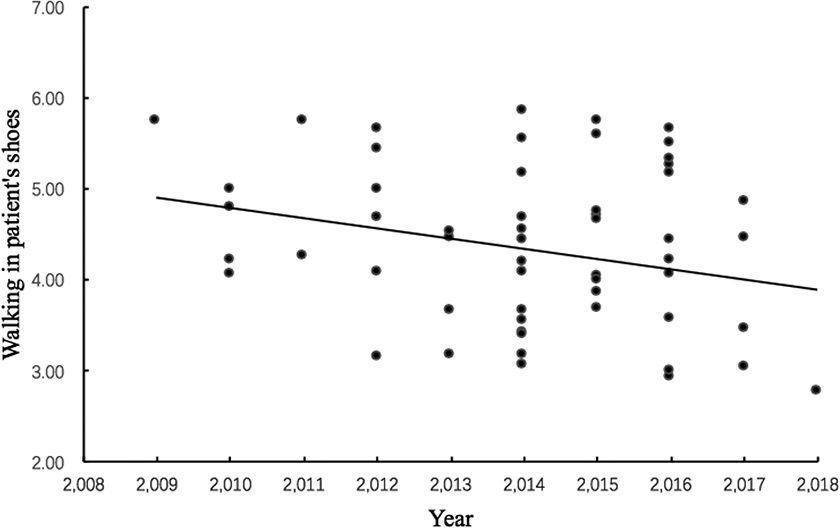
Changes in the empathy dimension of walking in the patient’s shoes from 2009 to2018.
Next, we conducted correlation analysis and weighted linear regression to measure the decrease in empathy over years (Table 2). The results of the correlation analysis showed significant negative correlations between time and the total empathy score and the perspective-taking score of the Chinese nurses; the correlations for compassionate care and walking in the patient’s shoes were not significant. The regression analysis showed, after controlling for sample size, that the year of data collection explained 9% and 11%, respectively, of the variance in total empathy and perspective-taking, indicating that the overall empathy of Chinese nurses declined significantly between 2009 and 2018.
The relationship between the mean scores for total empathy and the empathy dimensions over 10 years (N = 13,825).
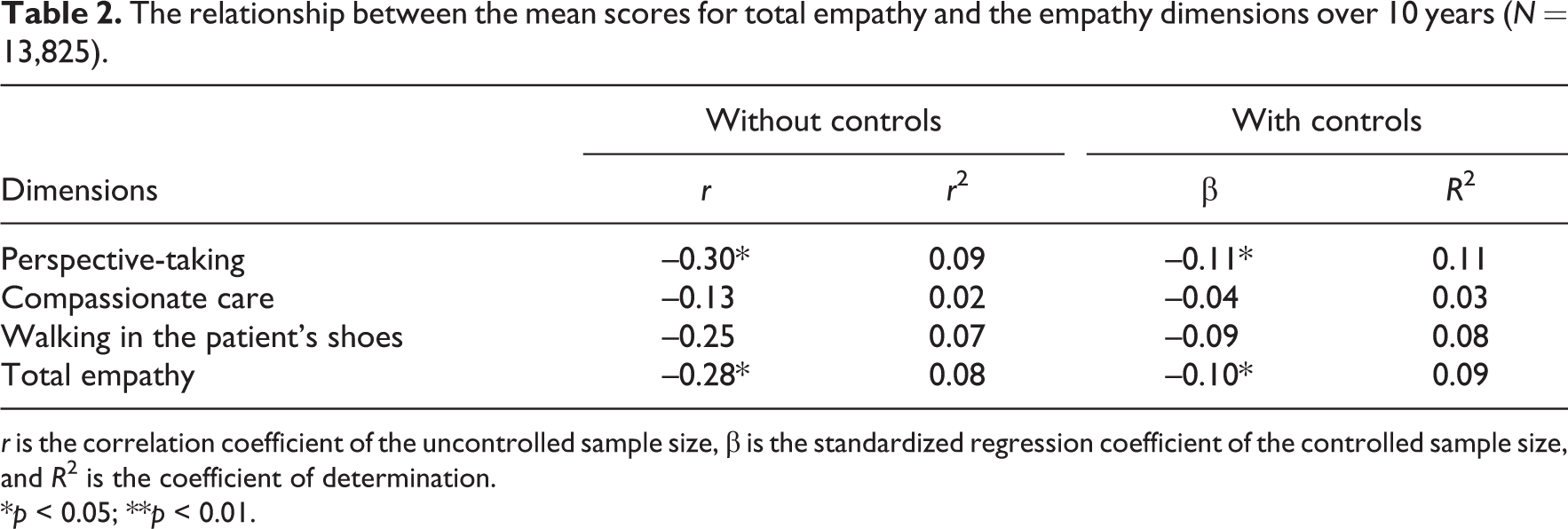
r is the correlation coefficient of the uncontrolled sample size, β is the standardized regression coefficient of the controlled sample size, and R 2 is the coefficient of determination.
*p < 0.05; **p < 0.01.
Magnitude of change
We used the effect size (d) and the coefficient of determination (r 2) to examine the magnitude of change in each empathy dimension during the past 10 years. We calculated the mean scores for each individual year using the following regression equation: y = Bx + C, where y is the mean score for empathy and x is the year. The regression equation showed that the mean scores for the empathy dimensions decreased from 0.40 to 0.76; converting the d values (0.45–0.86) into r 2 values indicated that the year of data collection explained 5%–16% of the proportion of variance in empathy scores. 27 Perspective-taking had a large effect size (i.e. it exceeded d >0.8), walking in the patient’s shoes had a medium effect size (i.e. it was 0.5–0.8), and compassionate care had a small effect size (i.e. it was 0.2–0.5) (Table 3).
Magnitude of changes in the dimensions of empathy of nurses from 2009 to 2018.
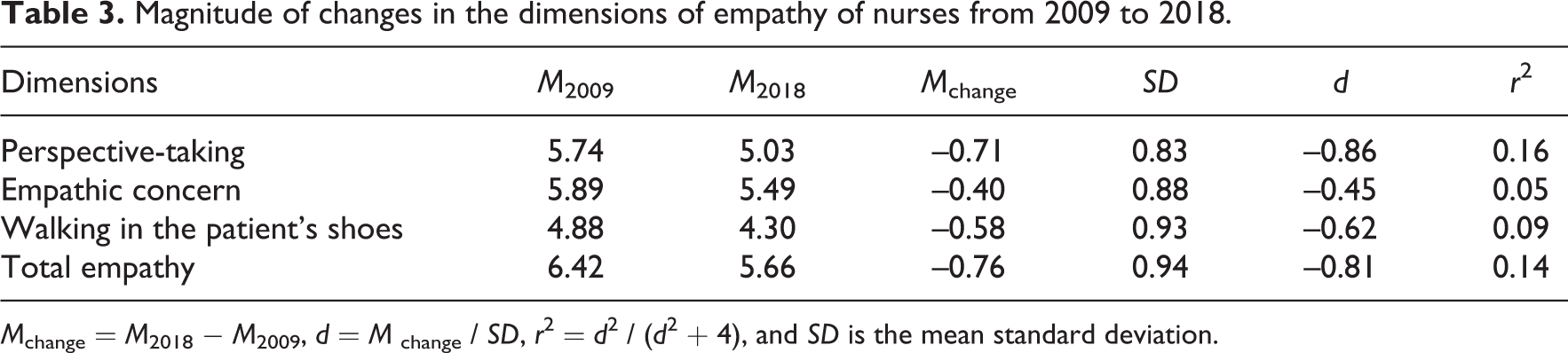
M change = M 2018 − M 2009, d = M change / SD, r 2 = d 2 / (d 2 + 4), and SD is the mean standard deviation.
Changes in the empathy of nurses in the different regions over 10 years
The results showed, controlling for sample size, that the empathy of nurses in the Eastern region did not change significantly over 10 years (see Table 4). In contrast, the total empathy score and the perspective-taking score of the nurses in the other regions significantly decreased over 10 years and explained, respectively, 14% and 19% of the variance in these two empathy scores.
Relationship between nurses’ empathy over 10 years and their different regions.
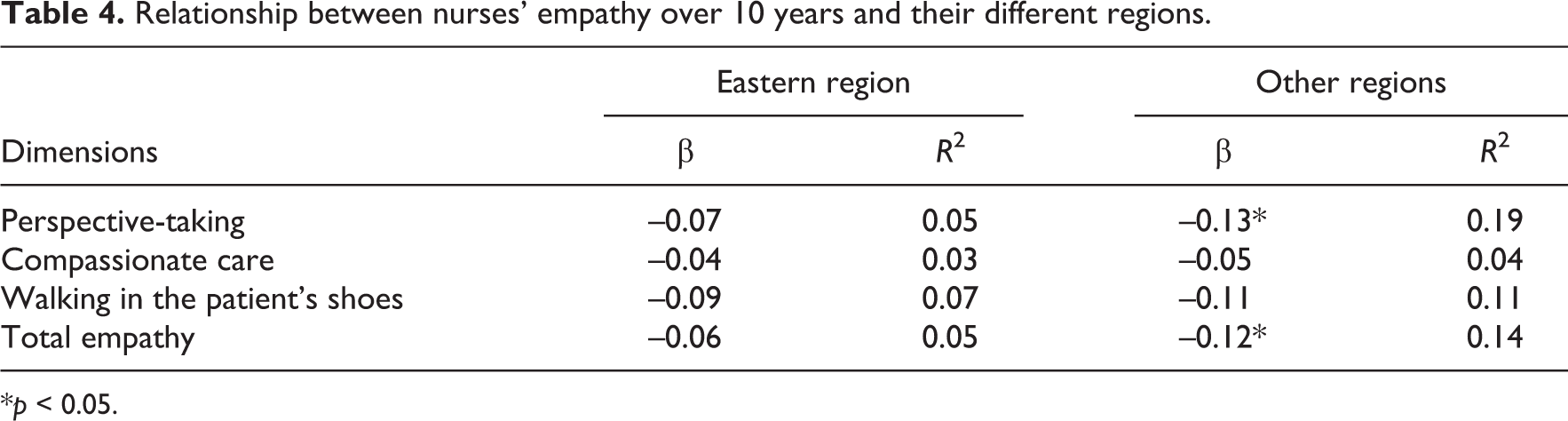
*p < 0.05.
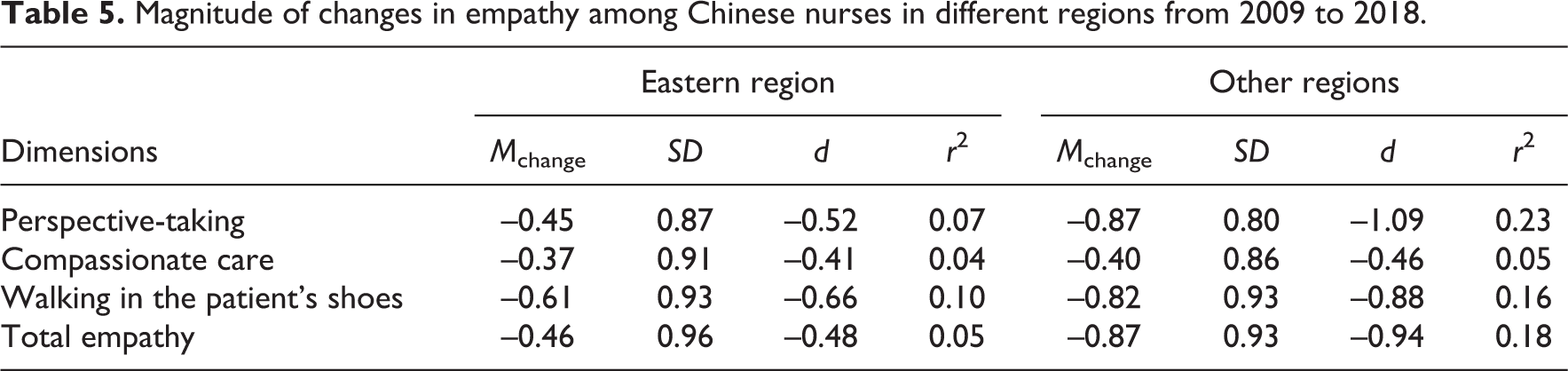
The effect size (d) and the coefficient of determination (r 2) were calculated to quantify regional differences in empathy using the regression formula. As shown in Table 5, the year of data collection had small effect sizes for the total empathy score and the score for compassionate care of the nurses in the Eastern region, whereas year of data collection had a medium effect size for the dimensions of perspective-taking and walking in the patient’s shoes. In other regions, the effect size of year was small for compassionate care, but large for the overall empathy score and walking in the patient’s shoes and perspective-taking. Overall, compared with the nurses in the Eastern region, the empathy of nurses in other regions showed an obvious downward trend by year.
Magnitude of changes in empathy among Chinese nurses in different regions from 2009 to 2018.
Changes in the empathy of nurses in the different departments over 10 years
In all, 19 papers included samples of ICU nurses and 18 papers included nurses from other departments. The results in Table 6 show, after controlling for sample size, the empathy of nurses in other departments showed a significant downward trend over 10 years and explained 14% of the variance in perspective-taking. The empathy of ICU nurses also showed a significant downward trend with respect to total empathy and walking in the patients’ shoes, explaining 14% and 22%, respectively, of the variance in these two measures. As shown in Table 6, the scores of the ICU nurses were significantly lower on these two measures of empathy than were those of the nurses in the other departments.
Dimensions of empathy among nurses in different departments over 10 years.
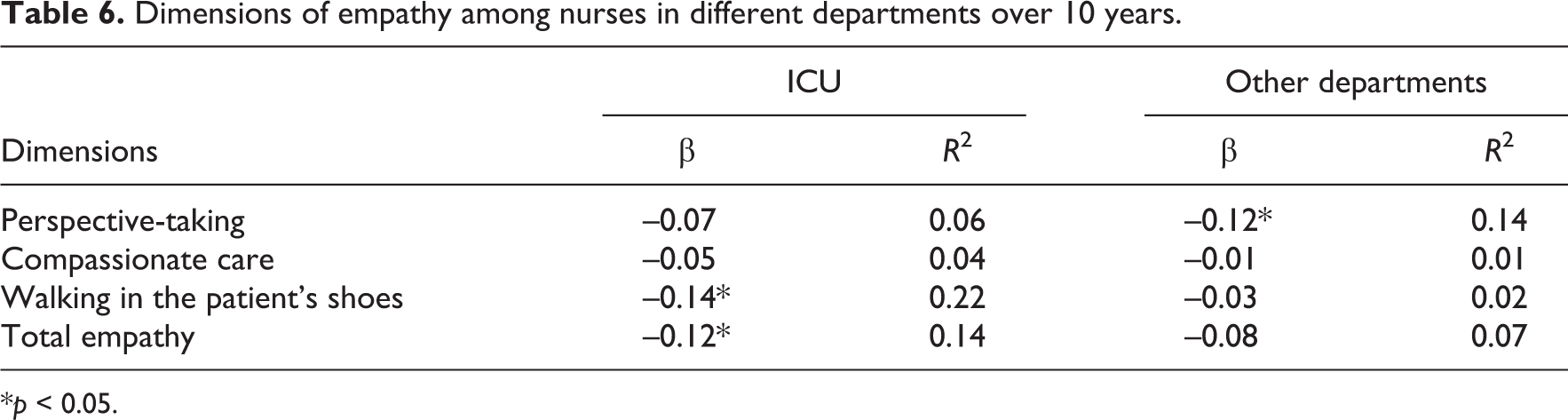
*p < 0.05.
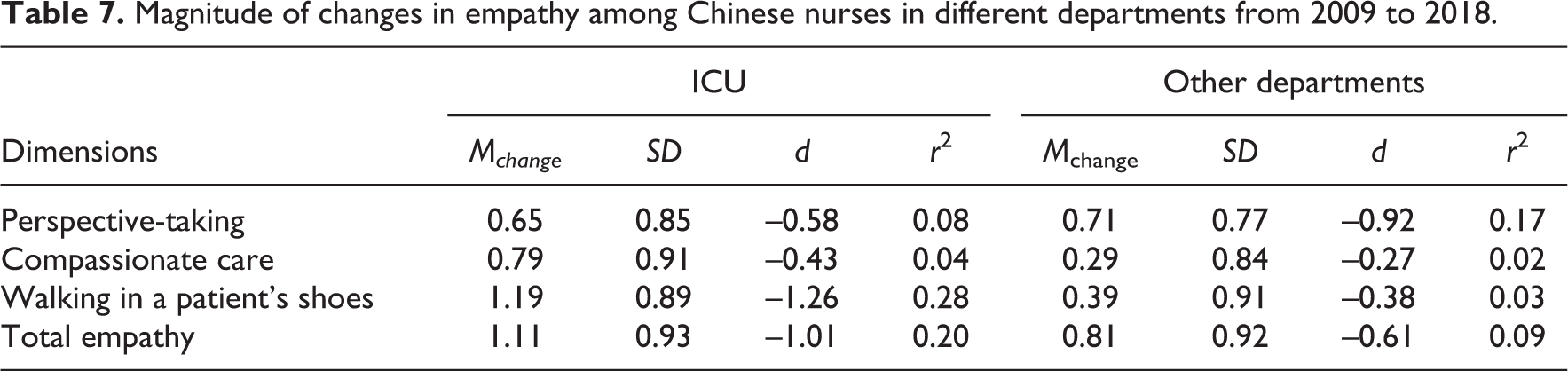
As shown in Table 7, year of data collection had a small effect on the compassionate care scores of the ICU nurses, a medium effect on their perspective-taking scores, and a large effect on walking in the patient’s shoes and the total empathy scores. In the other departments, the effect size was small for compassionate care and walking in the patient’s shoes, medium for the total empathy score, and large for the score on perspective-taking. Overall, the total empathy score of the ICU nurses showed an obvious downward trend by year.
Magnitude of changes in empathy among Chinese nurses in different departments from 2009 to 2018.
Discussion
We examined data from 57 studies related to changes in empathy among Chinese nurses from 2009 to 2018. Our results showed that empathy decreased over time among Chinese nurses, which is consistent with the results of studies from other countries. An Iranian study, for example, showed that nurses’ empathy has declined annually in recent years as work pressures have increased. 28 Similarly, studies conducted in the United States and Australia have reported a more pronounced decline in empathy among nursing students exposed to clinical encounters with patients in their second year of nursing studies, compared with those in their first year. 29– 31 These findings suggest that the decline in contemporary nurses’ empathy may be a global trend. It is worth noting, however, that the above studies had small samples. Whether the results are robust or not should be verified through meta-analyses. To be specific, our outcomes showed that the mean scores of total empathy and perspective-taking decreased by 0.81 and 0.86 (large effect sizes), respectively. The magnitude of change in the mean total score of empathy was lower than that of perspective-taking; thus, it can be inferred that the decline in the mean score of total empathy was mainly due to the decline in perspective-taking.
Why is the empathy of Chinese nurses declining?
First, the decline in the overall empathy of Chinese nurses may be related to the increase in job burnout. Previous studies have shown that individuals with high levels of burnout exhibit passive behavior and emotional depletion, which have a significant negative correlation with empathy. 32 Recent developments in China’s medical model, specifically the Plan for a Healthy China 2030, call for a comprehensive, full-process, and three-dimensional service model and service experience that integrate “prevention, first aid, treatment, rehabilitation, and health management” as the key points. Therefore, hospitals’ requirements and expectations of nurses have continuously increased. Current nurses must have a solid theoretical knowledge base, clinical technology skills, and specific academic and research abilities, so pressure on nurses is increasing. In hospitals, newly qualified nurses with performance deficits (e.g. nursing procedures) due to inexperience or knowledge deficits of hospital procedures are likely to experience aggravation and frustration, which directly affects the quality of their work and ultimately leads to emotional and behavioral responses, such as job burnout. 33 Nurses cope daily with high workloads, night shifts, fewer holidays, and unpredictable break times for prolonged periods, which can easily cause physical and mental exhaustion, thereby increasing their risk for burnout. 15 A CTMA showed that the degree of burnout of female nurses has increased yearly, 34 further supporting the finding that the empathy of Chinese nurses showed a decline by year.
Second, the decline in the nurses’ empathy may be related to workplace violence. A study by Wang and Li 35 found that violence against medical staff in the workplace has increased, and it has become a major threat to the occupational safety of medical personnel. According to a survey, the proportion of nurses involved in all incidents of hospital violence is very high, and more than 50% of nurses have experienced various types of violence, including physical, psychological, and sexual abuse. 36 Violent incidents have traumatic effects on nurses and can lead to pessimistic and negative emotions, such as fear, anxiety, anger, and depression. 37 Violent incidents reduce the satisfaction that nurses derive from helping patients and result in nurses’ unwillingness to contact patients, thereby ending the relationship between the nurse and the patient. 35 In short, violence against nurses is likely to have a negative effect on the nurse’s concern about the patient and the patient’s needs, to the degree that the needs are not satisfied (reduced perspective-taking), which might lead to a decline in the nurse’s overall empathy.
Third, education and continuous professional development of nurses are the key factors in nurses’ empathy. The existing research literature indicates that a lower educational level of nurses is associated with lower levels of empathy. 38 In addition, some studies have reported that the level of empathy of nurses is related to continuing professional development. 19,39 Thus, lack of attention to continuing education and in-service education might have affected the empathy of nurses in this study. Other studies have reported that empathy is associated with work-related stress, professional attitude, social support, reflective practice, work experience, and personality characteristics. 40– 43
Changes in empathy of nurses in different regions
Our study found that the overall empathy and the three dimensions of empathy of the nurses in the Eastern region had no significant chronological effects, compared to the other regions (Central). The difference between the regions might be related to their different incomes. The Central and Western regions have made great progress in raising nurses’ salaries with the implementation of the “Central Rise Plan” and the “Western Development Strategy” in recent years, but there is still a large gap between these regions and the Eastern region. 44 At present, wage levels are still the main factor affecting the income gap. According to the data from the National Bureau of Statistics, 11 by the end of 2017, the gross domestic product (GDP) had reached 74,412.72 billion yuan and the regional income gap had shown a growing trend. Per capita disposable income in the Eastern region had reached 30,654.7 yuan, which is much higher than the 20,006.2 yuan reached in the central region and the 18,406.8 yuan in the Western region. Thus, salaries for nurses in the Eastern region are generally higher than those of other regions. Previous studies have shown that salary is an important factor in job satisfaction. High-income nurses tend to have greater job satisfaction and subjective well-being, making them more willing to participate actively in providing services, placing themselves in the patient’s position, and providing more care. 45 This may be an important reason why the rate of decline in empathy of the nurses in the Eastern region was slower than that of other regions.
Furthermore, these differences could be due to an imbalance in the development of medical services in China. According to the 2017 China Health and Family Planning Statistical Yearbook, there were obvious regional differences in the service levels and management of public hospitals in 31 provinces (municipalities and autonomous regions) in China. The service level in the Eastern region was higher than that of most of the Central and Western regions. 46 Unlike the Central and Western regions, the Eastern region relies on its geographical environment (coastal) and economic development advantages, and attracts national quality medical and health resources and service teams, paying more attention to humanistic literacy and service concepts. 47,48 Therefore, the corresponding training of nursing staff is more likely to foster empathy and more likely to delay the decline in nurses’ empathy levels.
Changes in empathy of the nurses in different departments
This study found differences between the departments. The mean scores for total empathy and walking in the patient’s shoes among ICU nurses showed a significant decline by year, while no significant decline was found in the other two dimensions. The perspective-taking of nurses in the other departments showed a significant decrease by year, but the total score and the scores on the other two dimensions did not decrease significantly. These results might be related to the intensity of nursing tasks. Patients treated in ICUs are often critically ill and their health status changes rapidly. The number of nurses working in ICUs has been inadequate to meet the increasing demands of patients in China; the long-term intense workload of ICU nurses is likely to cause them physical and mental exhaustion and loss of interest, thereby reducing their enthusiasm for work. They have no extra energy to consider the patient’s perspective, which leads to their inability to walk in the patient’s shoes. 49 Moreover, because ICU nurses are one of the professional groups with most frequent contact with high-risk patients, (e.g. sudden death), they experience frequent fluctuations in their patients’ conditions, resulting in negative emotions, which increases their vulnerability to occupational (emotional) exhaustion. ICU nurses work under high stress for prolonged periods, and the traumatic events they encounter in their work often exceed those of other departments. An important reason for decreased empathy is indirect trauma caused by traumatic stress. 50 It is worth noting that our study did not find a significant downward trend over 10 years in the perspective-taking of ICU nurses. A possible reason for this is that ICU patients are critically ill, and patients who are confused or comatose cannot convey their opinions and needs to nurses, causing changes in perspective-taking to be inconspicuous. The severity of the illnesses among the patients in other departments was relatively mild, and most of the patients could express their thoughts and wishes, and therefore, they more accurately reflected the changing trend in the perspective-taking dimension of empathy.
Relevance to clinical practice
Influential departments of hospitals and the society should pay more attention to improving the empathy of Chinese nurses as much as possible to ensure patients’ needs are satisfied. At the same time, these measures will require the joint efforts of hospitals, nurses, and patients and their families. First, hospitals should create a good working environment. Improving the work environment of nurses could be an effective way to boost their compassion and satisfaction, 51 as could helping nurses increase their ability to manage their emotions, truly understanding their needs, and building harmonious relationships with them. A cooperative relationship could reduce the level of burnout and create optimal conditions for improving nurses’ empathy. Healthcare organizations should focus more of their attention on new nurses. If the cultivation of nurses’ empathy is fostered earlier, it may have a protective effect against exposure to negative and/or stressful events.
Second, emotional intelligence and self-care are important ways of nurturing empathy. 10,42 Therefore, we should encourage nurses to strengthen their awareness of self-care and self-compassion. During students’ clinical practice, faculty and clinicians in schools and hospitals can help students improve their emotional intelligence through different teaching and training methods, which could enhance their ability to address patients’ needs and prevent burnout and compassion fatigue.
Third, nurses should learn to manage their emotions in the workplace, express their empathy appropriately, communicate with patients actively, and understand the perspectives of patients in a timely manner. Nurses should participate in empathy training or psychological counseling to improve their empathy skills and avoid exhaustion and fatigue. Fourth, individual guidance and/or group presentations to patients and their families can be used to help patients. When patients acquire health-related knowledge, they have a better understanding of the professional characteristics of nurses and the difficulties they face. These activities can promote patients’ understanding of, support for, and cooperation with their nurses, and perhaps reduce the incidence of workplace violence and foster harmony in the nurse–-patient relationship. Finally, nursing colleges should pay more attention to empathy training of nursing students. An increasing number of colleges in China have developed relevant courses to improve the empathic abilities of nursing students. They can improve the communication skills and emotional intelligence of nursing students, help them learn how to gain patients’ trust, and promote the development of quality nursing care and the nursing discipline. 52
Limitations
This CTMA of 57 studies assessed the empathy of nurses in China from 2009 to 2018 based on the JSE-HP. The results could provide a basis for further examination of nurses’ empathy and suggestions for related policies. However, the study has the following limitations. First, only the JSE-HP revised by An was used in the study. Although there are other instruments measure empathy, such as the Interpersonal Reactivity Index (IRI). Future meta-analyses of studies on empathy using other instruments should be conducted. Second, due to the number of included studies, only differences between regions and departments were analyzed in this meta-analysis. Hospital level and marital status are also important factors affecting empathy. Finally, this study is limited by the number of other departments identified in each of the included studies, such as the psychiatric, obstetrics, orthopedic, and oncology departments. The effect size of each department could not be calculated separately. Therefore, we cannot discuss the internal differences between the departments in this study and we combined all of these studies. In future research, we might be able to increase the number of included articles to analyze the influence of different care settings on changes in nurses’ empathy.
Conclusion
This study found that the empathy of nurses in China has changed over the years. Their empathy has decreased steadily over nearly a decade, and the decrease was correlated with the regions in which the nurses lived and the departments in which they worked.
Footnotes
Authors’ note
YX and S-CX contributed equally to this article.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Health and Family Planning Commission of Hunan Province of China (B20180944).