
Abstract
Background:
Serious Illness Conversations aim to discuss patient goals. However, on acute medicine units, seriously ill patients may undergo distressing interventions until death.
Objectives:
To investigate the feasibility of using the Surprise Question, “Would you be surprised if this patient died within the next year?” to identify patients who would benefit from early Serious Illness Conversations and study any changes in the interdisciplinary team’s beliefs, confidence, and engagement as a result of asking the Surprise Question.
Design:
A prospective cohort pilot study with two Plan-Do-Study-Act cycles.
Participants/context:
Fifty-eight healthcare professionals working on Acute Medicine Units participated in pre- and post-intervention questionnaires. The intervention involved asking participants the Surprise Question for each patient. Patient charts were reviewed for Serious Illness Conversation documentation.
Ethical considerations:
Ethical approval was granted by the institutions involved.
Findings:
Equivocal overall changes in the beliefs, confidence, and engagement of healthcare professionals were observed. Six out of 23 patients were indicated as needing a Serious Illness Conversation; chart review provided some evidence that these patients had more Serious Illness Conversation documentation compared with the 17 patients not flagged for a Serious Illness Conversation. Issues were identified in equating the Surprise Question to a Serious Illness Conversation.
Discussion:
Appropriate support for seriously ill patients is both a nursing professional and ethical duty. Flagging patients for conversations may act as a filtering process, allowing healthcare professionals to focus on conversations with patients who need them most. There are ethical and practical issues as to what constitutes a “serious illness” and if answering “no” to the Surprise Question always equates to a conversation.
Conclusion:
The barriers of time constraints and lack of training call for institutional change in order to prioritise the moral obligation of Serious Illness Conversations.
Keywords
Introduction
It is important to discuss with patients their wishes and goals for healthcare, to promote patient autonomy, and ensure care is congruent with patient beliefs and wishes, especially if the patient ever becomes incapacitated. This may include goals of care discussions, which focus on planning for current healthcare decisions. 1 In addition to goals of care discussions, conversations may include Advance Care Planning (ACP), which focuses on planning for future healthcare; ACP is a process of reflecting on one’s own values and beliefs, learning about medical treatment options, deciding on a Substitute Decision Maker, discussing wishes with family and the medical team, and documenting these wishes. 2 These two types of discussions are often referred to under the umbrella term Serious Illness Conversation (SIC). 3 Ariadne Labs’ Serious Illness Conversation Guide (SICG) is a structured framework of setting up these discussions with patients who have a serious illness or life-limiting disease, on key topics such as illness understanding, prognosis, preferences, goals and fears, acceptable trade-offs, and wishes. 4
While SICs may help nurses to fulfill their ethical duty to promote patient autonomy and patient-centered care, lack of time is a factor against having SICs. 5 –7 Discussions on goals of care may be seen as time-consuming during a busy clinical day. 8 However, the amount of time spent on a SIC may not be as long as perceived by clinicians. 9 In addition, these conversations are ongoing in nature as patient care goals may change over time.
Conversely, the timing of SICs may be a factor as it can be difficult to discern when to initiate a SIC because of uncertainty in prognosis. As a result, SICs may be started late in the course of illness, when a patient may no longer have the capability to choose their course of care. 5,10,11 Patients and families may prefer less aggressive treatments than prescribed; however, these wishes and values are rarely explored in early ACP conversations during the hospital stay. 12,13 This uncertainty in conveying an accurate prognosis can be related to fear of destroying the patient’s hope of survival. 14
Another factor is lack of coordination between team members to gain a holistic picture of patients, resulting in inconsistent end-of-life messages. 7,15 Doctors are often expected to initiate SICs and nurses to provide emotional comfort, address concerns, and act as support persons. 7,10,14 All these barriers speak to the need for a coordinated interprofessional team approach to SICs. 15 The present study aims to address some of these barriers by promoting a coordinated interprofessional team approach to SICs through a quick and efficient collaborative method for identifying patients for SICs.
Background
As mentioned earlier, SICs can promote the ethical principle of patient autonomy by engaging them in care planning. Moreover, the benefits of early SICs relate to the well-being of patients and families and quality of life (QOL). 16,17 Relieving pain and suffering and improving QOL, especially at the end of life, is an intrinsic ethical responsibility for healthcare providers. 18 Earlier SICs prepare patients and families for the end of life with better bereavement outcomes for family. 5,14 Psychosocial support is also an important factor in having earlier SICs as more time does not guarantee the patient’s and family’s acceptance of their circumstances. Acceptance of prognosis is related to less anxiety, and those who do not accept their poor prognosis are more likely to perceive themselves as a burden to others and have a worse QOL. 19 The provision of emotional and spiritual support is important in these circumstances. 12,19 The ethical principle of beneficence depends greatly on the patient’s perspective on QOL and outcomes, 20 so SICs would help nurses determine what would most benefit the patient from the patient’s own perspective.
To address the time barriers of conducting SICs, the Surprise Question, “Would you be surprised if this patient died within the next year?” can be used to quickly identify patients who may benefit from having a SIC. If the answer to the question is “no,” a SIC is indicated. The Surprise Question has been shown to be quick and efficient with reasonable accuracy in some studies when it came to identifying patients at high risk of death who may benefit from palliative care services. 21 –23 The Surprise Question has been used in primary care and long-term care settings to promote SICs 24,25 ; if the goal is not to accurately prognose patients, but to promote early SICs, the Surprise Question can be a quick and efficient tool. The Surprise Question has mostly been studied in oncology settings and usually with just doctors and nurses 21 –23 ; so this study will expand the Surprise Question to include the whole interdisciplinary team (doctors, nurses, and allied health) on an acute medicine unit.
Objectives
The objectives of this study were to investigate the feasibility of using the Surprise Question to identify patients who would benefit from early SICs and study any changes in the interdisciplinary team’s beliefs, confidence, and engagement in SICs as a result of asking the Surprise Question.
Methods
Study design and setting
This pilot prospective cohort study with two Plan-Do-Study-Act cycles (Figure 1) was part of a healthcare organization’s Research Challenge. The Research Challenge is an annual competition for frontline staff to learn how to design and implement a research project; basic research skills are learned and small-scale research projects are conducted. The study took place on the Acute Medicine units at a 435-bed, acute care, teaching and research hospital located in Vancouver, British Columbia, Canada. The patient population on Acute Medicine is diverse and includes vulnerable groups with complex psychosocial backgrounds and substance use disorders (SUDs). For investigating the feasibility of using the Surprise Question to identify patients who would benefit from early SICs, two Plan-Do-Study-Act cycles were used. The Plan-Do-Study-Act cycle method is a common four-stage cyclic approach used in healthcare quality improvement projects 26 ; the “plan” stage identified the objective of using the Surprise Question to indicate patients for early SICs, the “do” stage tested the use of the Surprise Question, the “study” stage examined how the Surprise Question was used and the data associated with its use, and the “act” stage identified issues and needed adaptations for better use of the Surprise Question for a new Plan-Do-Study-Act cycle. Primary outcomes related to feasibility were assessed through keeping track of how the Surprise Question was used for each patient, and healthcare staff’s qualitative feedback on the use of the Surprise Question. Primary outcomes related to beliefs, confidence, and engagement in SICs of healthcare team participants were measured through questionnaires (Online Supplemental Appendix 1). Engagement in SICs of healthcare team participants was also measured via chart review. During the recruitment period in March 2019, a pre-intervention questionnaire was administered, followed by the intervention period (including chart review) in April 2019; the healthcare team participants were followed until the end of May 2019, when the final questionnaire was administered.
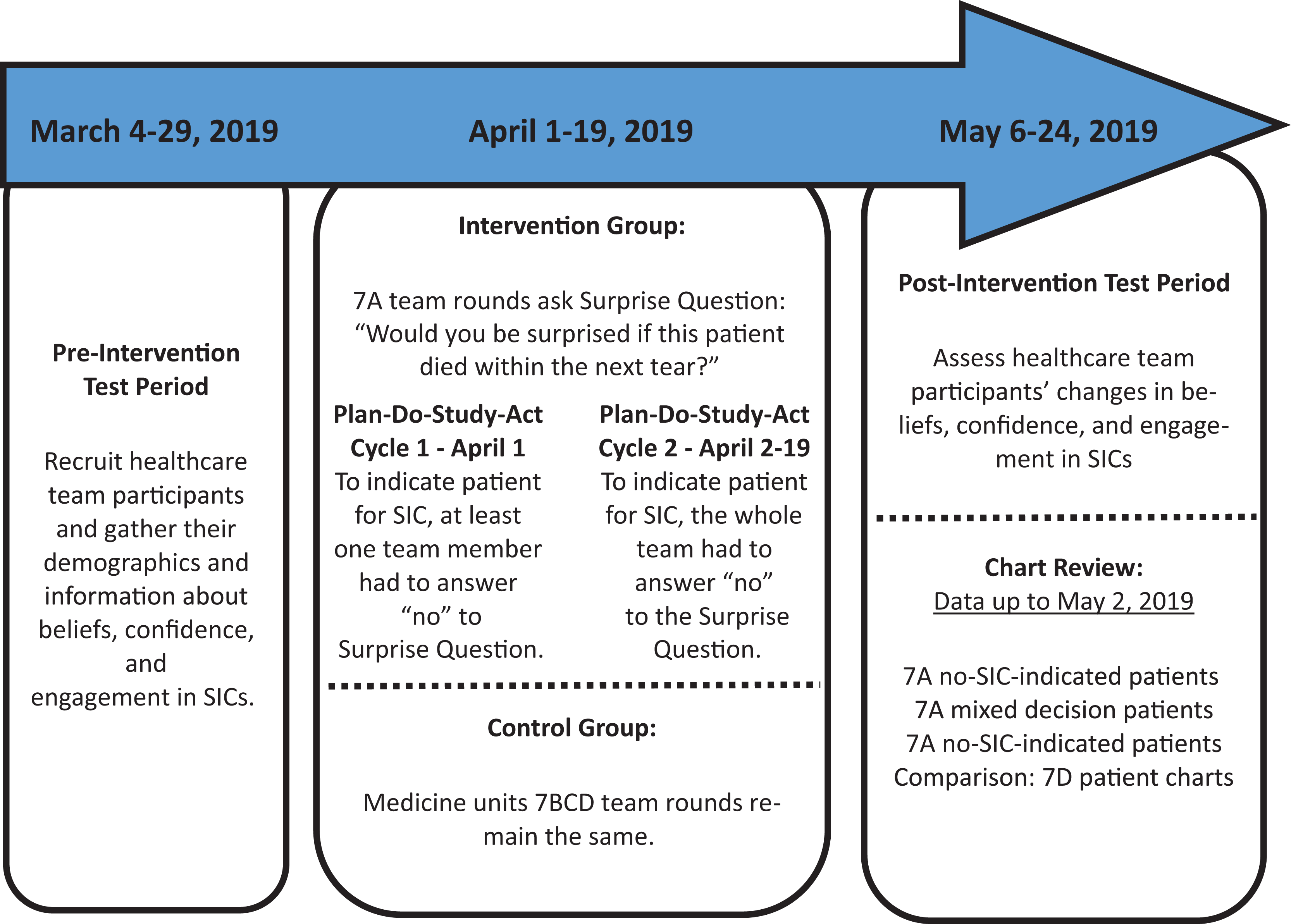
Study design with timeline.
Ethical considerations
All healthcare team participants provided written or online informed consent prior to data collection. The study was approved by the University of British Columbia–Providence Health Care Research Ethics Board in Vancouver, British Columbia, Canada (Research Ethics Board #H18-02609).
Participants
In all, 300 healthcare team staff (e.g. clinical nurse leaders (CNLs), clinical teaching unit (CTU) doctors, nurses, and allied health) were eligible for recruitment from Acute Medicine units 7A, 7B, 7C, and 7D (collectively grouped as 7ABCD). These Acute Medicine units are homogeneous with respect to size, staff, and type of patients. Recruitment on 7ABCD involved sending emails to staff, putting up posters, and asking healthcare staff in-person to complete the first questionnaire. Eligibility criteria included being an Acute Medicine healthcare team member who attended interdisciplinary rounds. When recruited to complete the first questionnaire, it was unknown whether participants were in the intervention or control group, because healthcare staff may work on several units. For the post-intervention questionnaire, participants were asked if they attended 7A interdisciplinary team rounds when the Surprise Question was used, to sort participants into the intervention group or control group. Posters were put up on 7ABCD reminding participants to complete the post-intervention questionnaire. The post-intervention questionnaire was offered through email and in-person administration to those who completed the pre-intervention questionnaire.
Standard care (control) group
Typically on 7ABCD, the CNLs, CTU doctors, nurses, and allied health attended daily (Monday–Friday) interdisciplinary rounds on their respective units, where CNLs led discussion on medical, nursing, functional, and psychosocial updates on all patients on the unit. The control group included healthcare team participants who attended rounds on 7BCD, where standard procedures occurred. In this setting, Surprise Question would not be asked, and patients are not systematically identified for SICs.
Intervention group
The 7ABCD are all Acute Medicine units, and 7A was arbitrarily chosen to be the intervention group unit, based on alphabetical order (7A vs 7BCD) of the units. Only one unit was chosen to be in the intervention group due to the pilot project’s resource limitations. The intervention group included the healthcare team participants who attended interdisciplinary rounds on 7A when the Surprise Question was used. Beginning 25 March 2019, the 7A CNL, CTU teams, nurses, and allied health all received paper copies, daily reminders, and explanations of the Surprise Question algorithm. The researchers and 7A CNLs walked through how to use the Surprise Question algorithm with staff from 25 March to 1 April 2019. A copy of the SIC guide was also on the Surprise Question algorithm paper as a reminder; the SIC guide was a pre-existing hospital protocol and pre-printed in all patient charts in the ACP section. The project did not train staff on how to use the SIC, as it was part of hospital policy and many staff received education on the SIC in new employee orientation. Just as in standard care where the CNLs would lead discussion for interdisciplinary rounds, the 7A CNLs also led 7A interdisciplinary rounds. In addition to leading discussion, the 7A CNLs were trained to use and lead the Surprise Question algorithm during 7A interdisciplinary rounds. The Surprise Question algorithm intervention took place on 7A from 1 to 19 April 2019. On 1 April, the Surprise Question was asked for all CTU patients on 7A. From 2 to 19 April, the Surprise Question was asked for all newly admitted CTU patients on 7A. For the first Plan-Do-Study-Act cycle on 1 April, the original Surprise Question algorithm criteria to indicate a SIC for a patient was that only one team member had to not be surprised if a patient died within the next year (Figure 2). However, feedback from 7A healthcare staff indicated they would prefer to be in full agreement to indicate a SIC for a patient. One reason provided by healthcare staff was that the threshold for indicating an SIC (having even just one team member not be surprised if a patient died within the next year) was too low, and many patients would have SICs indicated, leading to time constraint issues; another reason was some healthcare staff felt the SIC was not appropriate to have with certain patients, and they did not want mixed messages conveyed to patients from different healthcare providers. This resulted in a second Plan-Do-Study-Act cycle with changes to the Surprise Question algorithm effective 2 April. In order to indicate a SIC, all team members needed to be in agreement about the Surprise Question answer and agree that a SIC was indicated (Figure 3). For the second Plan-Do-Study-Act cycle, the new Surprise Question algorithm was used 2–19 April in 7A interdisciplinary rounds to ask the Surprise Question and decide which patients may need SICs.
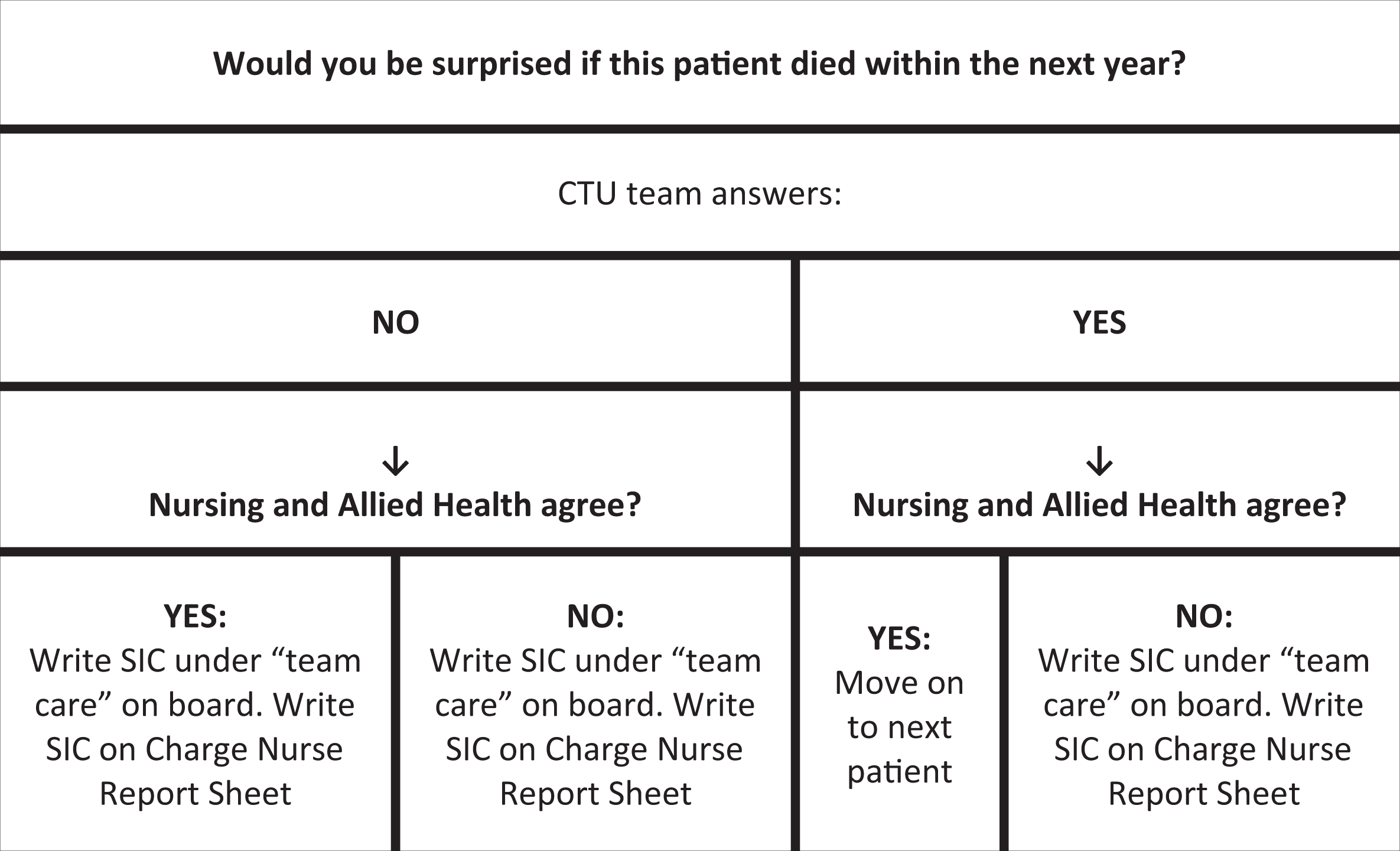
Surprise Question Algorithm used on 1 April 2019 during 7A rounds.
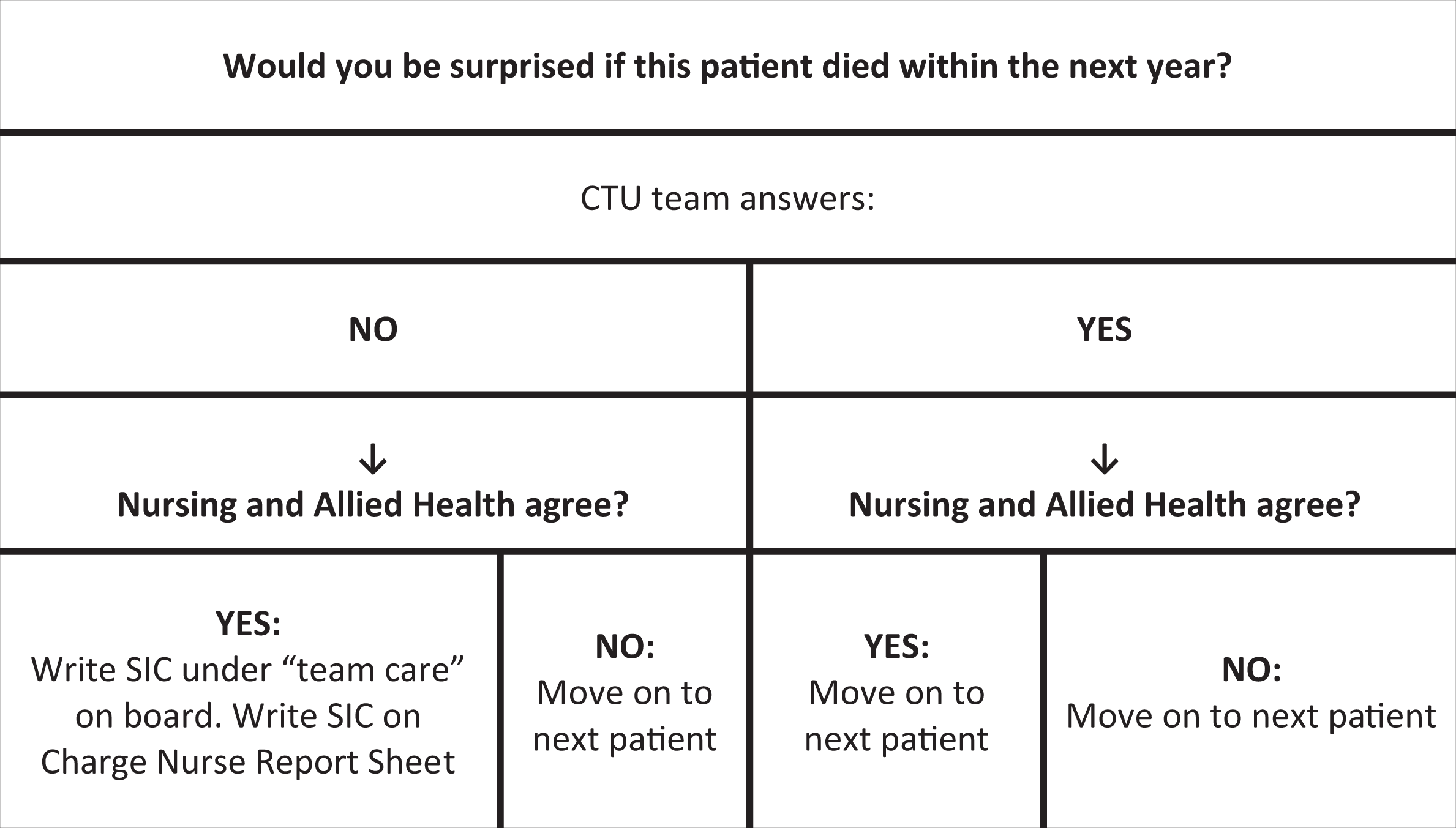
Surprise Question Algorithm used 2–19 April 2019 during 7A rounds.
Outcome measures
Feasibility of the use of the Surprise Question during interdisciplinary team care rounds was defined as being relevant for use on all patients and sustainable for use for future subsequent team care rounds. The Surprise Question algorithm (Figure 3) was kept for each 7A patient, so the Surprise Question algorithm process for each SIC-identified patient could be tracked, helping to ascertain the feasibility of using the Surprise Question to identify patients for SICs. Post-intervention qualitative feedback from the 7A healthcare staff also contributes to investigating the feasibility of using the Surprise Question to identify patients for early SICs.
The effects of using the Surprise Question during rounds to identify patients for SIC on the healthcare team participants’ beliefs, confidence, and engagement in SIC were the other outcome measures assessed in this study. These outcomes were measured via self-report through pre- and post-intervention questionnaires adapted from the literature, 27 –29 and included measurements on beliefs on whose role ACP belonged to, confidence in conducting aspects of SICs, and actual engagement in SICs.
For beliefs, participants were asked two open-ended survey questions regarding who they thought was responsible for informing patients about ACP and who was responsible for documenting patient ACP preferences. Although best practice would be a team approach to ACP, 15,27 these questions from similar studies 29 were used to explore what actual healthcare providers on 7ABCD believed. Participants were also asked which factors they believed to be barriers to having SICs, with a “check all that apply” question. For confidence, participants were asked 10 Likert-type questions where they had to rate their confidence in certain aspects of SICs. These barriers and confidence questions were adapted from an American national survey of hospitalists. 28
For self-reported engagement, participants were asked how many different patients they had SICs with, and on average, how many SICs they had with the same patient. These questions 29 had the numbers and wording changed with the consultation of the healthcare organization’s ACP lead, to better suit the needs for Acute Medicine.
The outcome of engagement in SIC was also measured via chart review in May 2019 for 7A and 7D patients (chart data during the April 2019 intervention period); 7D was selected as the comparison group for chart review due to similarities in patient population yet differences in healthcare staff participants. All 7A patients where the Surprise Question was used had their charts reviewed, and all 7D patients admitted during the April intervention period also had their charts reviewed. The charts for 7B and 7C were not reviewed due to the pilot project’s resource limitations. Data regarding changes in ACP forms, code status, and documented discussion of serious illness domains such as goals, strengths, and fears were collected from the charts.
Statistical analysis
Demographics and prior SIC experience for participants were summarized using descriptive statistics (e.g. medians and proportions). To compare outcome differences between the intervention (Surprise Question) and control groups (No Surprise Question), bivariable tests (Kruskall–Wallis test for continuous variables and Pearson’s chi-square test or Fisher’s exact test for categorical variables) were used.
The level of significance was set at p < 0.05 for all statistical analyses, and all reported p-values reflect two-tailed tests. All analyses were conducted using R 3.3.1 statistical programming. 30
Findings
Participants
The study recruited 97 out of 300 (32.3%) healthcare team members on 7ABCD to complete the pre-intervention questionnaire. Fifty-eight of these 97 (59.8%) healthcare participants completed the post-intervention questionnaire. The intervention group (exposed to Surprise Question during 7A interdisciplinary rounds) had 16 healthcare participants, and the control group (standard care during 7BCD interdisciplinary rounds) had 42 healthcare participants.
Descriptive data
Among participants who completed the post-intervention questionnaire, most were bedside nurses (n = 42); other roles recruited were doctors (n = 6), allied health (n = 4), student nurses (n = 3), and nurse leaders (n = 3). Participant ages ranged from 22 to 63 years old (median = 30 years old), and most participants held a bachelor’s degree. Most participants had 1–5 years of professional experience, and many (75.9%) in the sample had seen and received previous education about SICs.
Outcome data
Results regarding feasibility
The 7A healthcare staff used the Surprise Question to identify 6 out of 23 patients for early SICs (as evidenced by the completed Surprise Question algorithms for each 7A patient). However, post-intervention qualitative feedback from the 7A staff revealed issues with using the Surprise Question for certain patient populations and situations, which is further discussed in the “Discussion” section. These issues revolved around interpretations of “serious illness,” and whether answering “no” to the Surprise Question always meant a SIC was needed.
Pre- and post-intervention results
There were no significant results regarding the use of the Surprise Question positively affecting healthcare team participants’ beliefs in whose role it was to inform patients about ACP and document this (Table 1), beliefs about barriers to SICs (Table 2), nor engagement in SICs. However, the intervention group (n = 16) had a statistically significant (p = 0.028) decrease in confidence in conveying serious news to patients (Table 3).
Pre- and post-intervention beliefs about whose role it was to inform patients about ACP and document this, stratified by intervention status.
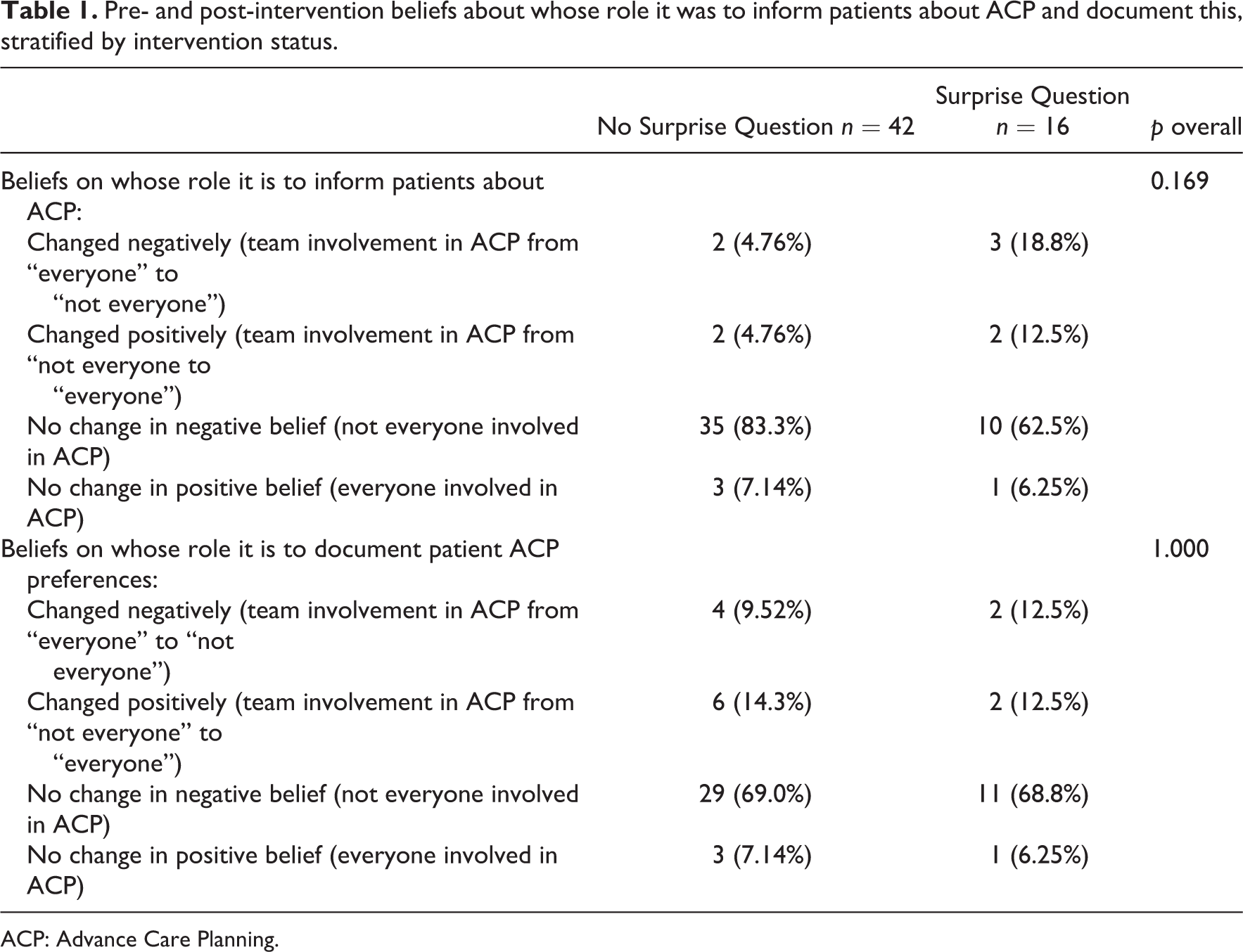
ACP: Advance Care Planning.
Pre-intervention beliefs in barriers to SIC, stratified by intervention status.

SIC: Serious Illness Conversation.
Change in confidence in conducting SICs by intervention status.

SIC: Serious Illness Conversation.
Chart review results
Thirty-seven CTU patient charts were reviewed in total; 23 CTU patient charts on 7A for when the Surprise Question intervention was used, and 14 CTU patient charts on 7D as a comparative. All the 23 7A CTU patients who had the Surprise Question asked about them had their charts reviewed. On 7A, this included six SIC-indicated (full team agreement to the Surprise Question) patient charts, three mixed-decision (disagreement about the Surprise Question answer) patient charts, and 14 no-SIC-indicated (full team agreement to the Surprise Question) patient charts. The three 7A mixed-decision patient charts were for those patients where the healthcare team disagreed on the answer to the Surprise Question, so according to the updated Surprise Question algorithm, would not have a SIC indicated. One of the mixed-decision patient charts had the Surprise Question asked on 1 April and the other two patient charts had the Surprise Question asked after 2 April; however, the healthcare team followed the updated Surprise Question algorithm so that all three “mixed decision” patients did not have a SIC indicated. Healthcare team agreement using the Surprise Question algorithm was tracked for our purposes to see if there would be a difference if a patient had a “mixed decision.” Two of the six (33%) SIC-indicated 7A patients charts had Options for Care (indicates code status) forms changed after the Surprise Question intervention compared to none in the comparison group and none in the no-SIC-indicated group. SIC domains were charted on more often in the 7A SIC-indicated patients charts than the 7A no-SIC-indicated patients charts (palliative care 66.67% vs 0%, end-of-life care 83.33% vs 14.29%, prognosis 100% vs 0%, family meeting 33.33% vs 0%, priorities 50.0% vs 14.29%, and code status 83.33% vs 7.14%) (Table 4). For the 7D comparison charts, prognosis (100%) and code status (71.43%) were documented more commonly, but there was no designation process done regarding SIC need for those patients.
Frequency table for occurrence of each Serious Illness Conversation domain in the interdisciplinary notes chart review.

SIC: Serious Illness Conversation; ACP: Advance Care Planning.
Other analyses
When comparing those who did not complete the post-intervention questionnaire (n = 39) to those who did (n = 58), the former is less knowledgeable about SICs, has less confidence, and engages less in SICs. The 58 healthcare team participants who completed the study (did both the pre- and post-intervention questionnaires) had a higher self-reported confidence in discussing goals of care with patients than those 39 healthcare team participants who did not complete the study (p = 0.041). Those who completed the study also had more self-reported SICs than those who did not complete the study (p = 0.045).
Discussion
The study investigated the feasibility of using the Surprise Question to identify patients who would benefit from early SICs, and found healthcare participants identified six out of 23 patients for SICs, but also identified issues with the Surprise Question affecting its feasibility with different patient populations and situations. There were equivocal findings for the Surprise Question’s impact on the interdisciplinary team’s beliefs, confidence, and engagement in SICs.
Equating the Surprise Question to a SIC
The Surprise Question is aimed at identifying people near the end of life, and therefore may be helpful for a select population including those with chronic illnesses who continue to decline despite medical intervention. 22 Studies 21 have shown that the Surprise Question was more accurate in patients with cancer than those with non-cancer illness; most of the Acute Medicine patient population would fall into the latter group. The Surprise Question has limitations with this patient population due to unpredictability of mortality in patients with SUDs and the perception that such patients do not require a SIC as it relates to their continued SUDs. Part of the issue was how the healthcare providers defined a serious illness. People with a history of SUD have a risk of overdosing, which can have serious health consequences and may lead to death; since a large proportion of the population on Acute Medicine has a SUD history, the medical plan usually involves discussion around addictions treatment rather than prognosis and goals of care. 31 However, marginalized patients who may have a low QOL would also benefit from conversations around QOL, to promote autonomy and a dignified QOL. 7 The premise of the Surprise Question intervention was, answering “no” to the Surprise Question meant a SIC was indicated; however, it was found that for some healthcare team members that answering “no” to the Surprise Question did not always mean they thought a SIC was required. For example, some healthcare team members may have thought, “I wouldn’t be surprised if this patient overdosed and died within the next year, but I don’t think they need a serious illness conversation for that.” For the intervention of the Surprise Question during 7A rounds, it was explicitly emphasized to participants that the Surprise Question was not used as a medical prognosis tool, but as a method of identifying patients who would benefit from having a SIC. Feedback from the 7A Surprise Question (intervention) group was that the trust in the Surprise Question equating to a SIC was not strong enough for some healthcare team members. Some thought that bringing up a SIC with a patient with SUD may damage the provider–patient relationship by unnecessarily causing fear, especially if the medical prognosis was not poor.
As in other studies, 32 when using an interdisciplinary approach to the Surprise Question, physicians and nurses may greatly differ in their answer to the Surprise Question; this may be due to each discipline’s focus on disease processes and personal relationships with the patient, all of which can affect the answers to the Surprise Question. Our study relied on a concordant response to the Surprise Question in order to indicate a SIC, to promote an interdisciplinary approach to having the SIC with the patient. The literature 33 reports that a barrier to the Surprise Question may be healthcare providers’ concerns that their responses to the Surprise Question may be inaccurate; the Surprise Question has been shown to vary in terms of accuracy, from poor to moderate to reasonable. 21,22 However, the purpose of the study was not prognostic accuracy, but to identify which patients would most benefit from an early SIC, so the Surprise Question can still be a useful tool to identify patients who require SICs.
Filtering process
The Surprise Question intervention may have acted as a filtering process, in which the patients where the answer was “no, I wouldn’t be surprised if this patient died within the next year,” would be identified as SIC candidates and those where the answer was “yes” were not candidates. This identification of patients may have led to less overall engagement with patients, but an increase in engagement with the right patients. This theory is supported by the healthcare team participants’ self-reported data appearing to have no change in SIC engagement levels, contrasted with the chart review data showing changes in ACP forms for the 7A SIC-indicated patient charts (two ACP forms were changed from 7A SIC-indicated patient charts vs none from the other groups). In addition, more of the SIC domains were documented in the 7A SIC-indicated than the 7A no-SIC-indicated patient charts (Table 4). For the 7D comparison charts, prognosis (100%) and code status (71.43%) were documented more commonly, but there was no designation process done regarding SIC need for those patients; perhaps if the 7D comparison charts’ patients had the Surprise Question asked about them, there would be a filtering process as well and the proportions of SIC charting may differ.
A caveat is that if healthcare providers answer “yes” to the Surprise Question, there is a chance that they may miss opportunities to engage in discussions with patients who could actually benefit from a palliative approach. A filtering process focusing on the patient’s context, which includes symptom control in comparison to closeness to death may be better in indicating who needs a SIC. 32,34
Moral obligation and lack of time
Feedback received from the 7A Surprise Question (intervention) group included questioning the moral obligation of having a SIC with SIC-identified patients, and the conflict of this obligation with lack of time. The literature 21 shows that false positives are common for clinicians answering “no” to the Surprise Question, which may not be surprising, as the Surprise Question considers whether death within the next year is possible rather than probable. High false positive rates for Surprise Question would be concerning, especially if they triggered SICs for too many patients. In an ideal world, healthcare providers would have SICs with all patients, sharing information about prognosis, worries, and goals. However, due to a lack of time, SICs are not always possible. Asking the Surprise Question about patients during interdisciplinary rounds may have caused moral distress as patients were explicitly identified for SICs and healthcare providers felt morally obligated to have SICs with these identified patients despite time constraints. Like previous studies, 33 clinicians may have felt the Surprise Question was acceptable and useful for ACP discussions between patients and the healthcare team; however, a major issue was finding the time for discussions.
Negative changes for confidence
Even though there did not appear to be much difference in demographics and previous education about SICs in the 7A Surprise Question (intervention) and 7BCD no-Surprise Question (control) groups, the 7A Surprise Question (intervention) group was slightly more confident in some areas of SIC prior to intervention initiation, despite the fact that 7A was arbitrarily chosen to be the intervention unit. This decrease in confidence may have been due to the 7A Surprise Question (intervention) healthcare team members having experience in conveying serious news, and now consciously using the SICG instead of just communicating like they usually do. Perhaps being more cognizant of using a new model for what you usually do can decrease confidence 35 ; this paradigm shift could have led to the questioning of their own abilities and a decrease in confidence in conveying serious news. Another reason may have been that asking the Surprise Question made healthcare providers feel more aware that SICs should happen, whereas those who were never asked the Surprise Question may have not thought as intentionally about their own confidence and the need to start a SIC. These issues may produce cognitive dissonance where people try to rationalize inconsistencies in beliefs, attitudes, or behaviors that cause psychological discomfort. 36 To alleviate this discomfort, healthcare staff may rationalize that patients do not need a SIC and not engage in such discussions.
Limitations
Sample size, attrition, and composition limit generalizability and significance of findings. The small sample size is not enough to generalize to the four medicine units (7ABCD). In addition, the results may differ if the data of the 39 participants who did not do the post-test questionnaire were included. When comparing those who did not complete the second survey (n = 39) to those who did (n = 58), the former is less knowledgeable about SICs, have less confidence, and engage less in SICs. The findings cannot be generalized to all medicine staff since the results represent those who are slightly more informed about SICs.
Other SIC education and projects occurred simultaneously with this study, so there may be the confounding variable of exposure to SICs, even though previous SIC education was inquired about in the pre- and post-intervention questionnaires.
Bias
When recruiting for the study, participants were only made aware that the study was exploring participants’ beliefs, confidence, and engagement in SICs. The Surprise Question intervention was not mentioned at all, nor the fact that 7A interdisciplinary rounds would hold the intervention and 7BCD would be the control units. It was only in the debrief after the post-intervention questionnaire period that participants were made aware of the whole study and its parts. This withholding of information from participants was to minimize any bias in questionnaire answers and also to minimize selection bias; if participants knew that 7A interdisciplinary rounds would hold the Surprise Question intervention, they may purposely try to pick up shifts on that unit or vice versa.
The change in the Surprise Question algorithm from 1 April to 2 April may have made a difference in responses to the Surprise Question; some healthcare providers who otherwise would have answered “no” to the Surprise Question may have just answered “yes” because they knew a full team agreement was needed to indicate SIC, and may have thought answering “no” to the Surprise Question would not have made a difference if they were the only one to answer so.
Conclusion
In our assessment of the feasibility of using the Surprise Question to identify patients who would benefit from early SICs, 6 out of 23 patients were indicated for SICs and healthcare staff feedback provided insight into issues needing further exploration. Healthcare providers’ interpretation of “serious illness,” the Surprise Question, and its use for patients with SUDs was an issue brought up often. Different approaches to identifying someone in need for a SIC may be needed based on the definition of “serious illness” and the patient’s QOL factors.
Furthermore, the SIC approach also needs to consider diverse cultural and ethnic backgrounds. ACP has poorer uptake by those of diverse cultural backgrounds than those of European ancestry; religiosity, spirituality, family-centered decision-making, and low health literacy are factors that may influence ACP in other cultural contexts. 37 Most ACP programs function within the context of a medical model, but may benefit by integrating spiritual and cultural community leaders in ACP as well. 37
Whether pertaining to patients with SUDs or patients from diverse cultural backgrounds, the ethical principle of justice indicates that all patients should have fairly allocated access to healthcare. 20 This includes the patient’s right to be identified for SICs and the right to a culturally appropriate engagement in SICs.
However, lack of specific training on approaching patients with varied backgrounds may contribute to nurses not feeling confident enough to bring up sensitive issues such as illness trajectories, fears, and wishes. Therefore, more emphasis on developing cultural competence to have the ability to care for patients with diverse values, beliefs, and behaviors is also essential in creating cultural safety in the context of having SICs. 38 Considering the social, economic, and political position of groups and how these affect social relations and health practices can impact the type of approach one would take with a patient. 39
Further research with larger sample sizes are needed to evaluate what impact the Surprise Question may have on the interdisciplinary team’s beliefs, confidence, and engagement in SICs, as the healthcare participant questionnaires indicated the Surprise Question negatively impacted confidence in conveying serious news, whereas the patient chart reviews had some positive evidence showing increases in SIC engagement through changes in ACP forms and documentation on SIC domains. Using the Surprise Question to identify patients for SICs may have led to an appropriate increase in engagement with the right patients and less unnecessary engagement with other patients, fulfilling the ethical duty of using healthcare and human resources appropriately. This pilot study provided equivocal findings, so we are uncertain whether the Surprise Question has any positive effects; further evaluation is needed.
Supplemental material
Supplemental Material, sj-pdf-1-nej-10.1177_0969733020983392 - The Surprise Question and Serious Illness Conversations: A pilot study
Supplemental Material, sj-pdf-1-nej-10.1177_0969733020983392 for The Surprise Question and Serious Illness Conversations: A pilot study by Kathy Le, Jenny Lee, Sameer Desai, Anita Ho and Holly van Heukelom in Nursing Ethics
Footnotes
Acknowledgements
Thank you to the Providence Health Care Research Institute Research Challenge for funding this study. Thank you to Lillian Vera, Padraig Reynolds, Julie Kille, Shazbeen Ali, and Wilma Chang for all your work on this study. Thank you to Wallace Robinson, Carrie Smith, and Sarah Cobb for advising on this study.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Providence Health Care Research Institute Research Challenge.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.