
Abstract
Background:
In the midst of the Covid-19 pandemic, healthcare workers increasingly encounter serious ethical issues that negatively affect their professionalism.
Purpose:
The study aims to examine the ethical sensitivity levels of physicians and nurses working in surgical units during the Covid-19 pandemic and the associating factors.
Method:
The sample of this cross-sectional online questionnaire–based study consists of 161 healthcare workers working at the surgical units in Turkish hospitals. The data were collected using the “Nurse Descriptive Information Form” developed by the researchers and the “Ethical Sensitivity Questionnaire.”
Ethical considerations:
Approval was granted by the ethics committee. Verbal and written consent was received from the healthcare workers.
Results:
Ethical sensitivity in the dimension of conflict was found to be higher in healthcare workers who had ethical issues during the Covid-19 pandemic, who were married, who were nurses, who worked more than 45 h, and who had a work experience of 7–10 years (p < 0.05). Healthcare workers with a family member diagnosed with Covid-19 had high ethical sensitivity in the dimension of conflict (p = 0.008), while those who reported being fully competent and ready (p = 0.038) about Covid-19 were found to have low ethical sensitivity. Besides, those who experienced inadequate supplies (p = 0.045), long working hours (p = 0.038), and problems in asepsis–sterilization (p = 0.046) during the Covid-19 pandemic were found to have low sensitivity in the holistic approach dimension.
Conclusion:
The study revealed that ethical issues during the Covid-19 pandemic, sociodemographic characteristics, knowledge-skills about Covid-19, and the problems encountered in the work environment during the pandemic affect the ethical sensitivity of healthcare workers in the dimensions of conflict and holistic approach. Therefore, it is recommended that governments and all healthcare workers, and stakeholders in the health system in our country and other countries take action to promote ethical sensitivity in response to the rapidly increasing epidemic by considering the factors that adversely affect ethical sensitivity.
Introduction
Covid-19, which appeared in Wuhan, China, in December 2019 and was accepted as a pandemic by the World Health Organization (WHO) on 11 March 2020 led to great changes in individual and social aspects. The increasing number of cases and uncertainties in the health system have created ethical issues for healthcare professionals. 1 The physicians and nurses often have ethical problems due to working in units like surgical units where there are complex structures, circulation, and use of technology is high, surgical patients have a high risk of injury, infection, and exposure to dangerous substances, unexpected, life-threatening, and rapid decision-making situations often develop.2,3
The ethical issues experienced in our country during the Covid-19 pandemic can be listed as follows: to whom priority will be given as the intensive care bed capacity is low (how to use scarce resources), how healthcare professionals providing care and treatment for patients diagnosed with Covid-19 will continue their work without risking themselves and their families, how to implement the isolation and lockdown, how to find the medication, and if it is found, who will be given the priority.1,2 Throughout the world, the Covid-19 pandemic causes ethical issues for physicians and nurses, who are the primary heroes of the healthcare system, in maintaining both their physiological and psychological health. It has also been reported that physicians and nurses experience ethical dilemmas in the distribution of security and limited resources.4–6 Research cites that ethical issues often occur in situations such as the distribution of the limited number of medical resources, 7 the inability to use intensive care beds and respirators for each affected or unaffected individuals, physician/nurse inadequacy, 6 intensive care bed shortage, and triage uncertainty.8–12 These problems also revealed the need to establish an ethical standard in the effective use of available resources.7,13 Some international associations and studies suggest that the pandemic should be managed as a crisis and that ethical principles should be followed and cooperation should be ensured with a solid scientific basis for the fair distribution of resources. Otherwise, health professionals may experience ethical issues.14–16 In the literature, certain criteria are presented to prevent the emergence of ethical issues that healthcare professionals frequently encounter during the pandemic. In this period, the first ethical principle is reported to be “respect for human dignity.” Therefore, to prevent ethical issues, everyone should have the right to have an objective and transparent triage, as well as access to information, and receive all necessary medical support. 7 It is also emphasized that justice should be the basic principle in resource allocation, healthcare should be provided and maintained, pain should be relieved in all cases, there should be standard protocols for the correct management of resources, resources should be directed to individuals who will truly benefit based on the existing clinical evidence, it should be recognized that not all patients can benefit from all resources in the same way, priority should be given to frontline healthcare professionals (saving the lives of those who can save more lives), 7 at least two people should be involved in triage, gender, socioeconomic status, ethnic origin, mental disability should not affect the triage, and a standard scoring system is required to avoid ethical issues.17–19
The pandemic period in which ethical issues may be encountered requires the development of ethical sensitivities of physicians and nurses to make ethical decisions.3,6,20 High ethical sensitivity not only contributes to professionalization but also directly affects the quality of treatment and care for patients.3,21 In professional healthcare practices, identifying the attitudes and behaviors of surgical physicians and nurses on ethical sensitivity, which is one of the significant components of qualified treatment and care, can contribute to taking the necessary precautions by identifying the deficiencies and errors in this regard and can also be beneficial in raising the awareness level of health professionals and the treatment.3,22 In light of this information, this study aimed to determine the ethical sensitivity levels of physicians and nurses working in surgical units during the Covid-19 pandemic and to raise awareness on the subject. The study is seeking answers to the following questions: What are the ethical sensitivity levels of surgical physicians and nurses, and what are the associated factors?
Materials and methods
Research type
The research is a cross-sectional, online questionnaire–based study.
Population and sample
The universe of the study was composed of 364 physicians and nurses who volunteered to participate in the study, answered questionnaire questions, and worked in the surgical units of Kocaeli University Research Application Hospital between 21 September 2020 and 21 October 2020 through social network sites and applications. The sample consisted of 161 physicians and nurses working in surgical units who voluntarily filled out the questionnaire within the specified period.
Data collection
A 16-question “Nurse Descriptive Information Form” developed by the researchers and the “Ethical Sensitivity Questionnaire (ESQ)” were used as data collection tools. After the questionnaire was created with “Google Forms,” it was sent to healthcare professionals by the researchers via social networking sites and apps (Instagram, Facebook, and WhatsApp). The questionnaire was set in such a way that respondents cannot pass the next question before answering the question coming. On the questionnaire form, the participants were informed about the purpose of the study, that the data would be used for scientific purposes, and that they agreed to participate in the study by filling out the questionnaire form.
Inclusion criteria were: (1) being a healthcare worker (HCW), (2) being a social media user, (3) being a volunteer for the study, and (4) those who answered the questions only once using the same Internet Protocol (IP). Exclusion criteria were determined as not fully answering the questionnaire. In the study, 52 people were excluded because they did not fully complete the questionnaire, and data were evaluated with a total of 161 participants. The survey response rate was calculated as 44.2%.
The Ethical Sensitivity Questionnaire
The ESQ, developed by Lützen, was first used in the Karolinska Nursing Institute (Sweden-Stockholm) in 1994 to determine the ethical sensitivity of physicians and nurses working in the psychiatric clinic and then in other units. ESQ is a 7-point Likert type measurement tool including 30 items and 6 sub-dimensions. The sub-dimensions are as follows: “autonomy” (reflects respect for the principle of autonomy and patient preferences), “benevolence” (reflects actions to increase the benevolence of the patient), “holistic approach” (refers to actions that will not harm the patient but also protect the patient’s integrity), “conflict” (reflects an experience of an internal ethical conflict), “practice” (demonstrates considering the ethical dimension in decision-making and implementation), and “orientation” (reflects the interest of healthcare professionals in their actions that affect their relationship with the patient).23,24 The validity-reliability study for the adaptation of ESQ to Turkish society was performed by Tosun in 2005, and the Cronbach alpha value was found to be 0.84. On the scale, statements are rated between 1 point (totally agree) and 7 points (totally disagree). 1 point indicates high sensitivity toward a complete agreement, 7 points indicate low sensitivity toward a complete disagreement, and the total score to be obtained range from 30 to 210. The evaluation is made on the total score, and a high score indicates a low ethical sensitivity and a low score a high ethical sensitivity. 24
Ethical considerations
To carry out the study, an institutional permit from the hospital, written permission from the nursing services directorate and the Kocaeli University Non-Invasive Clinical Research Ethics Committee dated 17 September 2020 and numbered NICREC-2020/16.04, and verbal and written informed consent were obtained from the participants.
Data evaluation
Statistical evaluation was performed with IBM SPSS 20.0 (IBM Corp., Armonk, NY, USA) package program. The Kolmogorov–Smirnov test was used for compliance with the normal distribution. Numerical variables were demonstrated as medians (25 and 75. percentile) and frequency (percentages). Differences between groups for numerical variables that do not have normal distribution were tested with Mann–Whitney U-test, Kruskal–Wallis, one-way analysis of variance, and Dunn’s multiple comparison test. The relationship between the numeric variables was obtained via the Spearman correlation analysis. For two-way tests p < 0.05 was considered as statistically significant.
Results
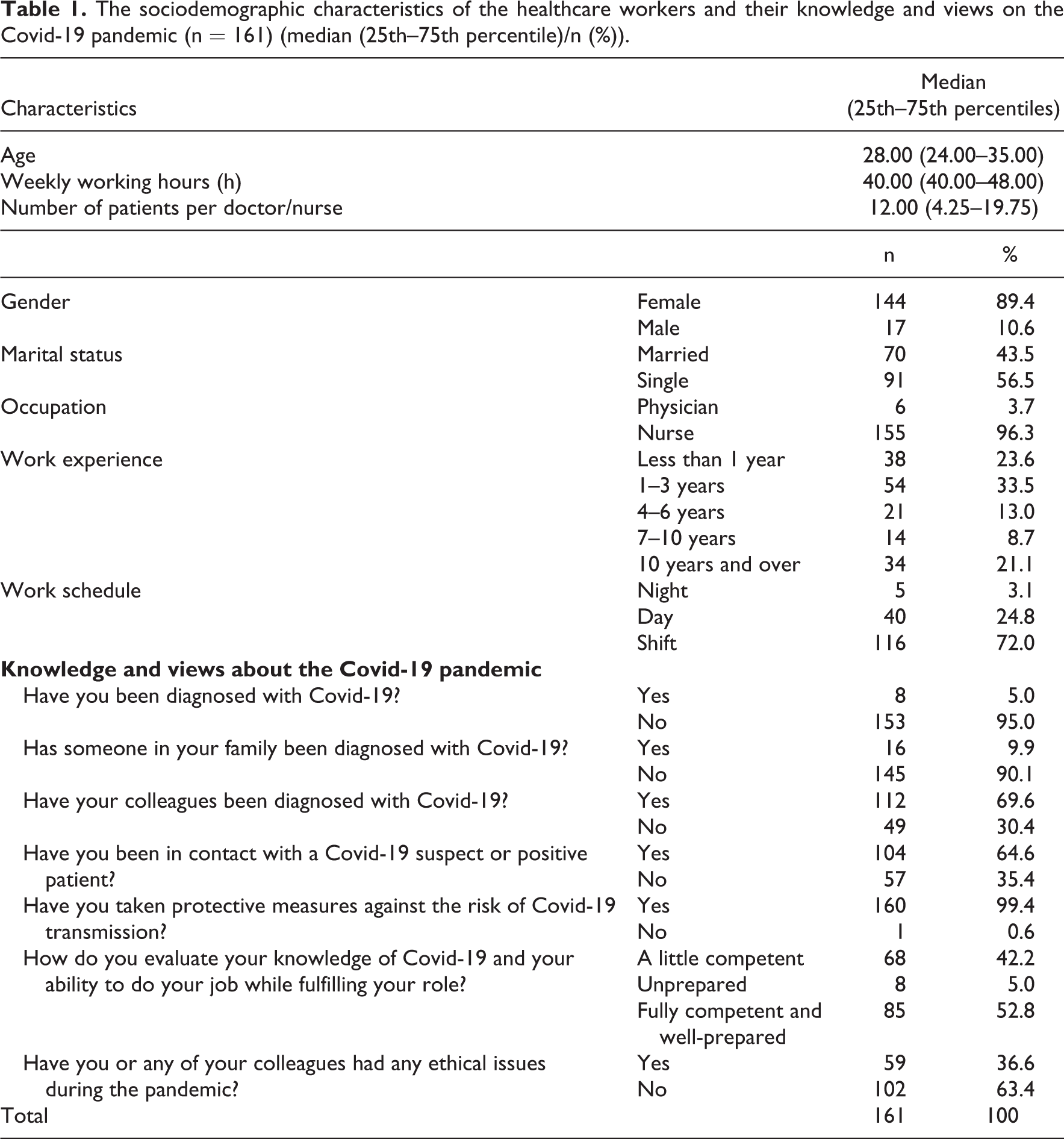
The study demonstrated that the median age of the HCWs was 28.00 (24.00–35.00) years, the weekly working hours was 40.00 (40.00–48.00) h, the number of patients per physician/nurse was 12.00 (4.25–19.75), 89.4% were women, and 96.3% were nurses. In addition, the knowledge and views of HCWs on the Covid-19 pandemic are shown in Table 1.
The sociodemographic characteristics of the healthcare workers and their knowledge and views on the Covid-19 pandemic (n = 161) (median (25th–75th percentile)/n (%)).
The study demonstrated that the ESQ sub-dimension median scores were moderate. Besides, no statistically significant relationship was seen between the age of HCWs and ESQ sub-dimensions (p > 0.05), but there was a positive significant relationship between the number of patients per doctor/nurse and the “orientation” sub-dimension (r = 0.171, p = 0.032; Table 2).
Relationship between the medians of the ESQ scale scores of HCWs and some of their characteristics (n = 161) (median (25th–75th percentile)).

ESQ: Ethical Sensitivity Questionnaire; HCW: healthcare worker.
a Spearman’s correlation analysis.
Bold faced values are shown as p < 0.05.
In terms of having ethical issues during the Covid-19 pandemic, the “conflict” median score of HCWs who were female (p = 0.017), married (p = 0.015), nurse (p = 0.032), and had more than 45 h weekly working hours (p = 0.010) was found to be lower, and the median scores of HCWs with a working experience of 7–10 years in “holistic approach” (p = 0.024) and “conflict” (p = 0.036) were found to be significantly lower (Table 3).
Comparison of the sociodemographic characteristics and ESQ subscale median scores of the HCWs according to their status of experiencing ethical issues during the Covid-19 pandemic (n = 161) (median (25th–75th percentile)).

ESQ: Ethical Sensitivity Questionnaire; HCW: healthcare worker.
a Mann–Whitney U-test.
Bold faced values are shown as p < 0.05.
It was found in the study that the conflict median score of HCWs with a family member diagnosed with Covid-19 was significantly lower (p = 0.008, Table 4).
Comparison of ESQ sub-dimension score medians according to the status of having a family member diagnosed with Covid-19 (n = 161) (median (25th–75th percentile)).

ESQ: Ethical Sensitivity Questionnaire.
a Mann–Whitney U-test.
Bold faced values are shown as p < 0.05.
A significant difference was also seen between the competency of the HCWs about Covid-19 and the “conflict” sub-dimension of ESQ (p = 0.020), and those who described themselves as fully competent and well-prepared about Covid-19 had high “conflict” score median than those who felt unprepared (p = 0.038, Table 5).
Comparison of ESQ sub-dimension score medians according to HCW assessment of their knowledge and skills about Covid-19 (n = 161) (median (25th–75th percentile)).

ESQ: Ethical Sensitivity Questionnaire; HCW: healthcare worker.
a Kruskal–Wallis test.
b Multiple comparison test.
c Unprepared to fully competent and well-prepared.
Bold faced values are shown as p < 0.05.
The “holistic approach” scores of the HCWs who experienced inadequate supplies (p = 0.045), long working hours (p = 0.038), and problems in asepsis–sterilization (p = 0.046) during the Covid-19 pandemic were found to be significantly higher (Table 6).
Comparison of ESQ sub-dimension score medians according to the problems faced by the HCWs during the Covid-19 pandemic (n = 161) (median (25th–75th percentile)).

ESQ: Ethical Sensitivity Questionnaire; HCW: healthcare worker.
a Mann–Whitney U-test.
Bold faced values are shown as p < 0.05.
Discussion
Considering the complaints about ethical approach and health rights in the world and our country and the limited number of studies in this field, it is an undeniable need to determine the ethical sensitivity of physicians and nurses who provide health services directly to the individual and the society during the Covid-19 pandemic. No study in the national and international literature to our knowledge has examined the ethical sensitivity of physicians and nurses working in surgical units during the Covid-19 pandemic. The lack of literature exploring ethical sensitivity in HCWs in surgical units during the pandemic has also caused challenges in discussing the findings in a detailed way.
Nurses’’ making ethical decisions in dilemma situations is making the best decision with a critical and systematic approach using their cognitive abilities in line with ethical principles. This process is also critical in terms of paying attention to ethical issues and displaying a professional approach. 25 Research on the ethical sensitivities of HCWs reveals different results that suggest that sociodemographic characteristics are effective in making ethical decisions. The study by Ertuğ et al. 26 in which they examined the ethical sensitivity levels of nurses working in a hospital environment and related factors (n = 111) reported that there is no statistically significant difference between the marital status of the nurses, their work experience, the hospital, and the unit they work in and the average ethical sensitivity score. Studies by Lutzen et al. 27 and Buyuk et al. 21 reported that people with more experience have higher moral sensitivity in terms of making the right decision in the face of ethical dilemmas. Basar and Cilingir 28 argue that there is a significant difference only in the autonomy sub-dimension of male nurses and that ethical sensitivity is higher in men. They also emphasize that the ethical sensitivity of married nurses is higher than single nurses, that the ethical sensitivity is the highest among nurses working in the surgical intensive care unit for 0–1 year, and that the ethical sensitivity of high school graduate nurses is higher than others. Consistent with our research findings, Tazegün and Çelebioğlu 29 and Dalcalı and Şendir 30 reported that female nurses had lower total ESQ mean score and higher ethical sensitivity than male nurses. In this study, while HCWs who experienced ethical issues during the Covid-19 pandemic, who were female, who were married, who were nurses, and who worked for more than 45 h had a higher ethical sensitivity, those with 7–10 years of work experience had higher ethical sensitivity in the holistic approach and conflict dimensions. This result can be interpreted as that HCWs who had ethical problems during the Covid-19 pandemic could cope better with conflict situations since they experienced more ethical decision-making processes or took more responsibility.
HCWs frequently suffer from ethical issues due to difficult working conditions and providing acute or intensive care services,3,31,32 and consequently, they are exposed to conflict and tension situations intensely.5,11,33,34 In the study, HCWs with a family member diagnosed with Covid-19 had high ethical sensitivity in terms of the dimension of conflict. The result suggests that dealing with ethical issues encountered in this process increases the awareness and sensitivity of the participants about ethical issues, and this situation reflects positively, especially in the field of conflict. It can be said that the significant findings among some sociodemographic characteristics according to the status of experiencing ethical issues presented in Table 3 affected this result.
Nurses’ reaction to ethical issues is stated to vary according to professional experience, autonomy, and competence.27,31 Grundstein-Amado 35 reported that physicians and nurses cannot make ethical decisions and follow a consistent model mainly due to their lack of education in ethical issues. In a study by Wiegand and Funk 36 in 2012, nurses reported that negative patient consequences of moral conflict included prolonged dying, undignified dying, delayed treatment, prolonged hospitalization, disrespect, and inappropriate care. In a study on Chinese nurses, Huang et al. 37 defined the obstacles to moral sensitivity as lack of knowledge about ethics, lack of work experience, hierarchical organizational climate, and conformist work attitude and defined facilitating factors as a positive workplace culture environment and practical application of ethical knowledge and ethical sensitivity. In a cross-sectional online study (n = 472) in which Afulani et al. 38 examined the preparations and related factors of HCWs in Ghana to control the spread of Covid-19, it was found that 66.7% of the HCWs know how to treat a patient with suspected Covid-19 and only 22% know how to manage a confirmed Covid-19 case. In the study, HCWs, who described “themselves fully competent and ready” about Covid-19, had lower ethical sensitivity in terms of the dimension of conflict compared to those who reported being unprepared. It is thought that the significant results among some sociodemographic characteristics according to the status of experiencing ethical issues in Table 3 and the high number of HCWs describing themselves “fully competent and ready” were thought to influence this result. For HCWs to provide qualified treatment and care during the pandemic period in which ethical issues may be encountered frequently, they must have the skills and competence to deal with moral conflicts and to solve problems. In this period, evaluating the knowledge and skills of HCWs about Covid-19, their approach to ethical issues and problem-solving skills is believed to be a supportive approach.
Evidence6,28,33,39 shows that lack of personnel and materials, uncertainty and limitations in their professional duties, powers, and responsibilities (uncertainty about independence in care and dependence on other procedures, inability to intervene in the patient urgently, uncertainty about the treatment given by the physician), communication problems, problems with patients and their families (lack of informed consent) due to intensive working conditions, and a large number of patients are the main causes of ethical issues for nurses. It is emphasized that nurses cannot provide enough ethical nursing care under these conditions, even if they want to. 33 Borhani et al. 40 reported that overwork and lack of staff are two significant factors that negatively affect the quality of care and ethical sensitivity. In the study, in which Amiri et al. 32 examined the relationship between the moral sensitivity of nurses and the quality of care, it is emphasized that ethical decision-making is not only related to the moral sensitivity of nurses, but the lack of organization in the institution and the obstacles encountered by nurses affect ethical decision-making. In Sperling’s 41 study (n = 231) on the care given by nurses during the Covid-19 pandemic and the impact of the pandemic on the ethical and motivational aspects of care (n = 231), it is stated that working under the high risk of infection caused by the obligation of care on the one hand and insufficient infection control measures on the other creates ethical problems and dilemmas for nurses in times of crisis. It is also emphasized that they seek a supportive environment for their basic needs and ethical concerns in this period. Another study on the ethical difficulties that Covid-19 poses for nurses indicates that employers are responsible for providing personal protective equipment to HCWs, and any harm that may come to patients due to the lack of personal protective equipment and personnel in providing care to patients safely is the failure of the systems rather than employees. 5 In this study, it was seen that HCWs, who reported to have problems in the lack of materials, long working hours, and asepsis–sterilization areas during the Covid-19 pandemic, had low ethical sensitivity in terms of the holistic approach dimension. The holistic approach includes care interventions in which the bio-psychosocial needs of the individual are addressed.23,42 Considering the result, it can be said that the presence of unfavorable working conditions negatively affects the ethical sensitivity of HCWs in fulfilling the bio-psychosocial needs of the patients. In addition to the positive workplace cultural environment, the application of ethical knowledge is also important as a potential facilitator of ethical sensitivity. 37 During the pandemic, HCWs should have a strong ethical sensitivity to fulfill the bio-psychosocial needs of patients in the best way. It can be said that this sensitivity can be realized by creating supportive working environments, thus improving the professionalism and ethical sensitivity of HCWs. Policymakers in the health system should also be able to identify or change the barriers nurses face in displaying their ethical performance. These barriers and facilitators can offer new and essential strategies to support or improve nurses’ sensitivity to ethical issues.
Limitations
Performing the study with a limited number of volunteering HCWs through social media, using an online questionnaire and scale is one of the limitations of the study. Therefore, the findings cannot be generalized to all in Turkey. Another limitation of the study is the fact that the study included only the first wave and surgical units, and the number of surgical physicians was low.
Conclusion
In the study, it was determined that the ethical sensitivity of HCW, who had ethical issues during the Covid-19 pandemic, differed in terms of some sociodemographic characteristics, and the ethical sensitivity of HCWs with a family member diagnosed with Covid-19 was high in terms of the conflict dimension, and HCWs who described themselves fully competent and ready about Covid-19 had a low ethical sensitivity in terms of conflict dimension. In addition, HCWs who had inadequate supplies, long working hours, and problems in asepsis–sterilization during the pandemic had low ethical sensitivity in terms of the holistic approach dimension. The results of this study provide basic information on the ethical sensitivity and the associated factors for HCWs in the pandemic period. This research may provide an opportunity for the implementation of various interventions against situations that adversely affect the ethical sensitivity of HCWs during the Covid-19 pandemic to increase the quality of health services.
Although health systems and HCWs know how important it is to maintain adequate ethical sensitivity in the Covid-19 pandemic, relatively few studies have examined this dimension of the pandemic response. To fill this gap in the literature, more research is needed to evaluate ethical sensitivity in fields other than surgery. There is also a need for studies to be conducted in different countries including a wider sample group about the effect of ethical sensitivity on the physical, mental, social well-being, quality of care, and patient outcomes of HCWs during the pandemic period. This type of research can assist hospital managers and health policymakers in resolving ethical issues faced by healthcare providers worldwide.
To reduce the ethical dilemmas of HCWs, it is recommended to make ethical committees functional, to establish ethical counseling systems, to provide digital ethics trainings, and to develop/publish ethical guidelines that will guide HCWs during the pandemic period.
Footnotes
Acknowledgements
We would like to thank all physicians and nurses who participated in the study.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.