
Abstract
Background:
Ethical care in maternity is fundamental to providing care that both prevents harm and does good, and yet, there is growing acknowledgement that disrespect and abuse routinely occur in this context, which indicates that current ethical frameworks are not adequate. Care ethics offers an alternative to the traditional biomedical ethical principles.
Research aim:
The aim of the study was to determine whether a correlation exists between midwifery-led care and care ethics as an important first step in an action research project.
Research design:
Template analysis was chosen for this part of the action research. Template analysis is a design that tests theory against empirical data, which requires pre-set codes.
Participants and context:
A priori codes that represent midwifery-led care were generated by a stakeholder consultative group of nine childbearing women using nominal group technique, collected in Perth, Western Australia. The a priori codes were applied to a predesigned template with four domains of care ethics.
Ethical considerations:
Ethics approval was granted by the Edith Cowan University research ethics committee REMS no. 2019-00296-Buchanan.
Findings:
The participants generated eight a priori codes representing ethical midwifery care, such as: 1.1 Relationship with Midwife; 1.2 Woman-centred care; 2.1 Trust women’s bodies and abilities; 2.2. Protect normal physiological birth; 3.1. Information provision; 3.2. Respect autonomy; 4.1. Birth culture of fear (midwifery-led care counter-cultural) and 4.2. Recognition of rite of passage. The a priori codes were mapped to the care ethics template. The template analysis found that midwifery-led care does indeed demonstrate care ethics.
Discussion:
Care ethics takes into consideration what principle-based bioethics have previously overlooked: relationship, context and power.
Conclusion:
Midwifery-led care has been determined in this study to demonstrate care ethics, which suggest that further research is defensible with the view that it could be incorporated into the ethical codes and conduct for the midwifery profession.
Introduction
Ethical principles that govern maternity care practice are central to the care of childbearing women. However, there is growing perception and acknowledgement that many women are not receiving ethical care. There is limited evidence related to ethical perspectives in maternity care and a paucity of empirical evidence in addressing the ethical needs of childbearing women. This article first situates the research topic in the background of global concern about increasing reports of disrespect and abuse in childbearing women, with a concerning lack of ethical input. An overview of the feminist ethic of care, referred to as care ethics, and its relationship with midwifery is then presented as a possible solution.1,2
Childbearing over the last 100 years has become increasingly medicalized and technocratic; with the move of childbirth from home to hospital, the medical model has become the dominant model of care. 3 Maternity care medicalization is a multidimensional dynamic, which pathologizes normal birth processes, increases intervention and standardizes care of the woman within a culture of fear and risk reduction. 4 A resulting factor of medicalization is women having less power and control over their birth experiences, which have detrimental effects on women’s psychological, emotional and physical health.3–5 Furthermore, the literature describes obstetric violence, physical abuse, verbal abuse and disrespect within the maternity system as a global systemic issue.6,7 It has been suggested that ethical care is sometimes rhetorical or even disregarded in the medicalization of birth. 2
While researchers have been addressing the pervasiveness and epidemiology of disrespect and abuse in childbirth, one perspective that has not been widely explored in countering injustices and oppression of women in maternity care is that of ethics.1,2 There is limited evidence about how ethical principles are used and understood in maternity care, and yet, ethical issues arise in almost every aspect of pregnancy, labour, birth and the puerperium.1,2 There is contemporary literature that describes maternity care decision-making and ethical dilemmas after the fact, but ethical care is more than these, it is how the whole notion of care is approached and the impact this has on women.1,2,7,8
Ethical behaviour for midwifery care is guided by the International Code of Ethics for Midwives. 8 The code has four domains which point to the expectation of respectful, humanized practice. The Code of Ethics four domains are midwifery relationships; the practice of midwifery; professional responsibility of the midwife; and advancement of midwifery knowledge. These mandates detail how midwives prioritize relationships, how they practice upholding professional responsibilities and how they ensure integrity of the midwifery profession. The four bioethical principles (non-maleficence, beneficence, justice and autonomy) are implicit in the International Code of Ethics for midwives, which additionally acknowledges the human rights of women, seeks justice for all women and is based on respectful relationships.
The four bioethical principles may suit the standardized medical model of maternity care but may not necessarily suit the woman being cared for. Where bioethical principles perceive principles, norms and specific rules, they do not recognize the complexity or context of the human experience, which includes: the influence of relationships; the context of decision-making as part of a greater story: the responsibility of care as forming part of the complex matrix of a woman’s life and the role of emotions in decision-making. 2 While bioethical principles are important, in the conventional model of maternity care, these are determined by those who hold the balance of power and, therefore, may tend to support institution-centred care rather than woman-centred care. 2
Midwifery and care ethics
MacLellan, 1 and more recently, Newnham and Kirkham 2 have proposed the ‘care ethics’ approach as one solution to the many ethical problems associated with the medicalization of childbirth and make the appeal for empirical research into care ethics.
Care ethics is an emerging normative ethical theory based on a feminist philosophical perspective, which is also referred to as ethics of care or relational ethics. 9 Care ethics is defined by Held 10 as ‘compelling moral salience of attending to and meeting the needs of the particular others for whom we take responsibility’. (p. 6). Care is a social practice that constitutes the care giver and the care receiver and is an ethical phenomenon in and of itself because care is identified as a universal human experience, with a moral responsibility attached to those relationships of care.11,12 Care ethics proposes that the web of relationships – the context, power dynamics and individual preference – are as morally significant to consider as the principle-based moral judgements of bioethics, in determining what is good. The care ethics paradigm would assist midwifery in drawing attention to the sociopolitical power imbalances embedded in the current medical dominated maternity system.
Contemporary care ethics comprises four broad aspects – relationship, the practice of care, attention to power and sociocultural context.10–17 The practice of care has been further described as including the characteristics of responsiveness, attentiveness, responsibility and competence. 13 Relationship is the underpinning focus of care ethics that ensures power imbalances are made visible during care and recognizes the sociocultural context in which caring is happening, thereby enhancing ethical sensitivity and the practice of good care. 14 Attention to broader sociocultural contexts and power imbalances extends ethical consciousness from a decision-making or moral dilemma focus to greater ethical attention in meeting the care needs of the individual. 15
Research is now needed to determine whether and how the care ethics approach might be more appropriate for midwifery. There is, to date, no published primary research in midwifery utilizing care ethics, although other fields are using this emergent paradigm.16,17 Our study aims to fill this gap as the first study to examine care ethics in midwifery.
Research aim
The aim of this study was to determine whether there is a correlation between midwifery-led care (MLC) and care ethics using template analysis with a priori codes generated by participants.
Research design
This inquiry was grounded in the ontology of critical realism, which acknowledges the influence of power structures on observable reality. We therefore used the emancipatory methodology of participatory action research, with a feminist theoretical perspective (FPAR). Participatory action research was chosen to partner with women in the research process, and the feminist critical lens was chosen to highlight the historical and sociocultural complexities of contemporary maternity care that lead to the disempowerment of women. Template analysis was chosen for this part of the action research, as the best method for testing the theoretical concept (care ethics) to practice (MLC). A key benefit of this study method is it enables direct questions to be asked of the data; in this case; does MLC demonstrate care ethics? This discursive approach confirmed with primary research the theoretical questions posed by the midwifery profession.
Designs that test theory against empirical data require pre-set codes 18 to aid data extraction. A data extraction template was created with four a priori codes that represent the main characteristics of care ethics, synthesized from contemporary literature,9–17 as shown in Table 1. Next, a priori codes that represent MLC were generated by participants and were applied to the template as shown in Table 2. Then, evidence to support the a priori codes was populated into the template as shown in Table. 3.
Data extraction template: Care ethics.

Care ethics data extraction template populated with MLC codes.
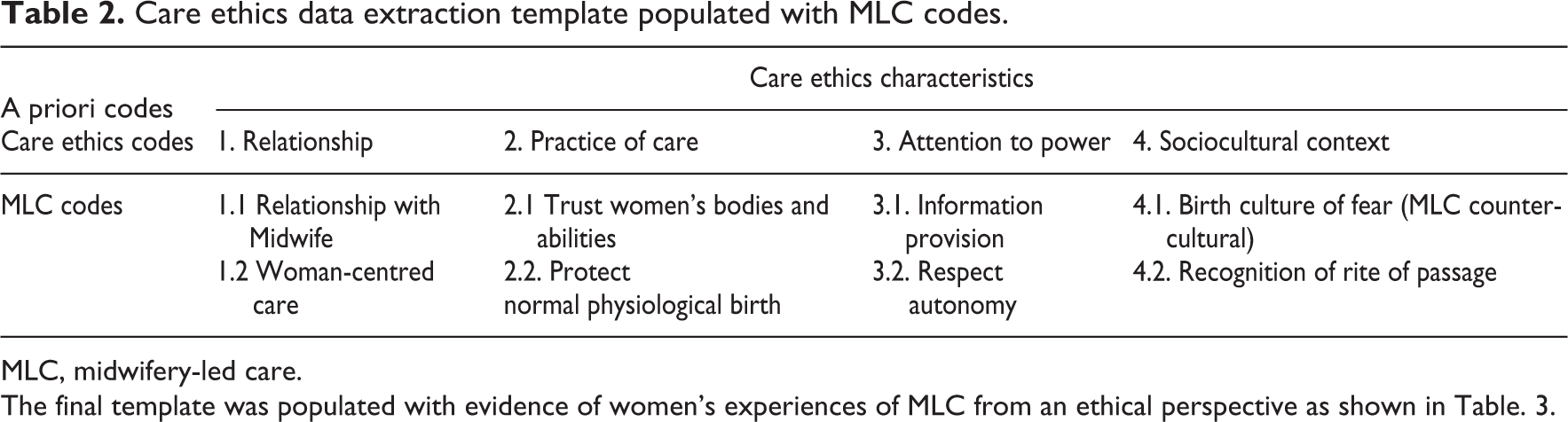
MLC, midwifery-led care.
The final template was populated with evidence of women’s experiences of MLC from an ethical perspective as shown in Table. 3.
Final care ethics template with populated evidence of MLC.
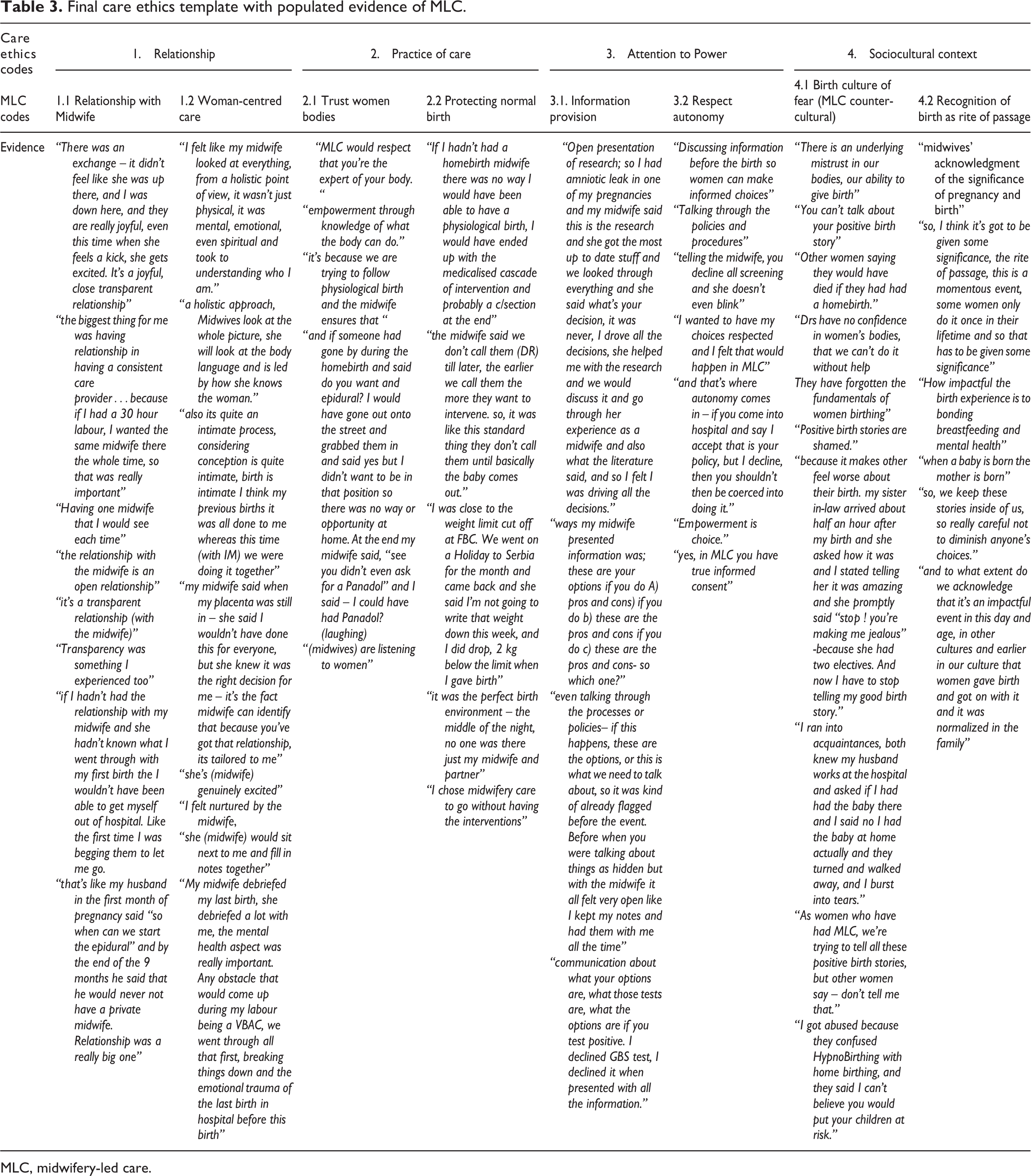
MLC, midwifery-led care.
Participant and research context
The study sample included women (n = 9) who had experienced a midwifery-led model of maternity care. Participants were recruited through purposive sampling and self-selected from an electronic bulletin advertising the research in maternity consumer forums. A participant information sheet and consent form were provided and returned via email. Consent to the study was voluntary. Thirteen women returned the consent forms, and four were not included in the study as they had not had a midwife as the primary care giver. A stakeholder advisory group of nine women called the ‘community action research group’ or (CARG) was formed.
Data was collected in Perth, Western Australia, September 2019. The purpose of this data collection was to generate a priori codes, which would be used to test theory, rather than rich, thick, qualitative data. Thus, the nominal group technique (NGT), useful in groups that include stakeholders to discuss and rank hierarchy of importance, was chosen. 19 A discussion topic guide was used which was informed by a literature review. The discussion questions included: Why did you choose MLC? What was good/beneficial about MLC? Can you share an experience that you felt was wrong, unethical or harmful?
The NGT process commenced as each participant was invited to discuss their views of the topic guide, often with group discussion ensuing. After each guiding discussion point was exhausted, the group summarized the views expressed into five to eight keywords. From this list, each participant was then asked to prioritize, in hierarchy of importance, their top three keywords that summarized the answer to the discussion, both privately and individually. These were collated after the focus group using enumeration, the process of quantifying data, which tallies the number of times the code was documented. The final eight a priori codes were member-checked by participants. This process is a compelling example of FPAR design, co-collaborating with the women during the research process.
The a priori codes were then mapped to the predesigned care ethics template. The template was finalized with examples from the participants under each category, thus retaining women’s voices in the research process.
Ethical considerations
Ethics approval was granted by the Edith Cowan University research ethics committee REMS no. 2019-00296-Buchanan. Consent to the study was voluntary, the participants contacted the research team from an electronic bulletin advertising the research. The participants signed the participant information document detailing the research and verbal consent was gained prior to the interviews. Pseudonyms were assigned at transcription to ensure anonymity and confidentiality.
Trustworthiness measures
Trustworthiness was ensured through method choice, reflexivity and an audit trail recording decision-making rationale. Despite having a small data set for this part of the project, the methods were true to aim in testing theory against practice. Dependability was ensured through correct method choice of template analysis and NGT that could be repeatable. Participant-generated a priori codes ensured credibility, and confirmability was ensured through retention of raw data in the examples within the final template.
Findings
The participants generated eight a priori codes that represent ethical MLC. These findings were then applied to the care ethics template as shown in Table 2.
The findings established that MLC demonstrated the four core domains of care ethics. The participants identified the importance of relationship as demonstrated by MLC, as significant for care to be deemed ethical, that midwives demonstrate the practice of care ethics, that MLC levels power and that the sociocultural contexts of birth are significant.
Care ethics category – relationship
‘Relationship’ and ‘woman-centred care’ were major findings of this study. Women described the relationship with the midwife as ‘continuous’ and ‘woman-centred’ based on equality and transparency. All women wanted continuity of care with the same caregiver throughout pregnancy and beyond. The priority for the woman was that the midwife shared the same philosophy of birth, respected her agency and would aim to strengthen her capabilities. All participants confirmed that continuity with the midwife was extremely important in what they described as ethical care.
Georgia – ‘the biggest thing for me was having relationship in having a consistent care provider…because if I had a 30-hour labour, I wanted the same midwife there the whole time, so that was really important’.
Annie – ‘I felt like my midwife looked at everything, from a holistic point of view, it wasn’t just physical, it was mental, emotional, even spiritual and took to understanding who I am’. ‘a holistic approach, Midwives look at the whole picture, she will look at the body language and is led by how she knows the woman’.
The relationships with the midwife were also described as open. All the women confirmed transparency as being a key component of ethical care. Ava – ‘it’s a transparent relationship’ confirmed by another Kara- ‘Transparency was something I experienced too’. Elisa explaining ‘also its quite an intimate process, considering conception is quite intimate, birth is intimate I think my previous births it was all done to me whereas this time (with MLC) we were doing it together…(midwives) are listening to women’
Lucy – ‘There was an exchange – it didn’t feel like she was up there, and I was down here, and they are really joyful, every time she feels a kick, she gets excited. It’s a joyful, close transparent relationship…in the appointments the midwives are transparent, she would sit next to me with the notes on the desk and we would fill in notes together’
Practice of care
This category, the practice of care, as set out in care ethics includes responsibility and competence. This was matched to the a priori codes ‘trusting women’s bodies’ and ‘protecting physiological birth’. Trusting women’s bodies to birth was an important theme for the women in describing good care. They felt it was important that the care provider shares the same beliefs about normal physiological birth and trust in women’s bodies and abilities. Lucy said – “Midwifery-led care would respect that you’re the expert of your body”. Annie explained – “empowerment is through knowledge of what the body can do”. The women felt empowered and their capabilities strengthened through the trust midwives had in birth and women.
The women identified responsible and competent ethical care as prevention of intervention and facilitating normal physiological birth. When sharing their experiences of midwifery care, each woman consistently referred to how the care empowered her towards achieving a normal physiological birth. The women concurred that it was MLC that facilitated normal physiological birth through intervention prevention. Harriet said – ‘If I hadn’t had a homebirth midwife there was no way I would have been able to have a physiological birth, I would have ended up with the medicalised cascade of intervention and probably a c/section at the end’. Clare shared – ‘my midwife said to me – when my placenta was still in (physiological third stage) –“I wouldn’t have done this for everyone”, but she knew it was the right decision for me – it’s the fact midwife can identify that because you’ve got that relationship, its tailored’.
Attention to power
This category was represented by the subcategories, ‘information provision’ and ‘respect autonomy’. The women identified that the balance of power within the relationship influenced how ethical the care was. Their collective experience led to the recognition that the midwife builds relationship by working to equalize the power between the woman and midwife, whereas in the medical model, the care provider often retains their power and authority in the relationship. Kara – ‘Yes it’s all about the relationship – some women would prefer to hand over all the consent (to the Dr.)’
Women described the relationship with the midwife based on open provision of information and respecting autonomy. The women felt that this established a sense of mutual trust on which the foundation of decision-making could occur. They described that in the midwifery model of care, information was presented in a transparent manner, which enhanced ethical care. They felt fully informed, empowered with knowledge and could exercise their autonomy and be responsible for decisions. Georgia described – ‘(midwives) give open presentation of research; so I had amniotic leak in one of my pregnancies and my midwife said this is the research, and she got the most up to date stuff and we looked through everything and she said “what’s your decision?”…, I drove all the decisions, she helped me with the research and we would discuss it and go through her experience as a midwife and also what the literature said, and so I felt I was driving all the decisions’.
Participants identified that this knowledge and information provision was necessary for true informed consent and enabled them to make decisions and hold responsibility for those decisions. Information was identified as either given transparently to women, to enhance their agency, or as withheld, which limited their autonomy. The women felt ethical care was demonstrated when they had the power to make decisions and to exercise agency. Elisa said – ‘They (midwives) talk through policies and processes and discuss options. If this happens these are the options or this is what we need to talk about, so it was kind of already flagged before the event. Before you were talking about when things are hidden but with the midwife it all felt very open’ Harriet described this process – ‘the ways my midwife presented information was; these are your options if you do A) pros and cons) if you do b) these are the pros and cons if you do c) these are the pros and cons- and I made the decision’. Elisa confirmed this – ‘communication about what your options are, what those tests are, what the options are if you test positive. I declined GBS test, I declined it because when presented with all the information, I could make a decision’.
Sociocultural contexts
This category was further enhanced through subcategories: ‘Birth culture of fear’ (MLC counter-cultural) and ‘Recognition of birth as a rite of passage’. The women identified as a group that the sociocultural context of the maternity system was patriarchal and was underpinned by a fear approach to care, which they felt oppressed women. They agreed that this culture is unethical in the care of women. Ava said – ‘Doctors have no confidence in women’s bodies, that they can’t do it without help, they have forgotten the fundamentals of women birthing, there is an underlying mistrust in our bodies, our ability to give birth’. Trinny described – ‘In that first appointment women are making a choice for physiological or pathological birth’ but highlighted achieving a care provider that shared this philosophy was hard to find; Annie – ‘a homebirth midwife is really hard to find – I thought it would be as simple as Googling it’. Annie said – ‘Positive birth stories are shamed…because it makes other feel worse about their birth. My sister in-law arrived about half an hour after my birth and she asked how it was and I stated telling her it was amazing and she promptly said “stop ! you’re making me jealous” – because she had two electives. And now I have to stop telling my good birth story’. Harriet explained – ‘And also acknowledgment of the significance of the pregnancy and birth so I think it’s got to be given some significance, the rite of passage, this is a momentous event, some women only do it once in their lifetime and so that has to be given some significance and I think that gets lost’. Ava added - ‘And how impactful the birth experiences are and how they, generational trauma, all our experiences and anything that happens to us before our labour and afterwards, really does impact everything – the bond with our child, the breastfeeding, and all these things and the studies of increased perinatal anxiety and how it impacts our partner’.
Discussion
This article examined women’s experiences of maternity care from a care ethics perspective to map midwifery practice against care ethics categories. The women clearly identified what was and what was not ethical to them. They generated the a priori codes, as subcategories, that could then be mapped to care ethics, thereby demonstrating the correlation between the MLC and care ethics. It was identified that MLC reflects the categories of care ethics and could therefore be considered as more ethically sensitive, which is a new finding for the midwifery profession.
These findings of this study support the theoretical questions posed by MacLellan, 1 and Newnham and Kirkham 2 who suggest that care ethics should be further explored as an alternative paradigm to the bioethical principles that currently guide maternity care in Australia and internationally. The findings are consistent with previous research into care ethics, which demonstrates care ethics utilization as an ethical paradigm for enhancing ethical care.16,17
The a priori codes decided by the participants were mapped to the four domains of care ethics: relationship, practice of care, attention to power and sociocultural context.
Power imbalances are subtle and the work by O’Brien et al. 28 identified that informed choice is not the clear process as outlined in bioethics. Their study identified that midwives levelled power relations through information provision and that women require support and relationship with their care provider for decision-making. Autonomy is achieved through relational, cultural and emotional support to make decisions and give informed consent.
Conclusion
These findings using participant-generated a priori codes demonstrated that MLC exhibits the four domains of care ethics. The care ethics approach may, because of its consistency with feminist midwifery philosophy, values and priorities, yield better professional adherence to ethics and care of the childbearing woman. The apparent inconsistencies between contemporary maternity care and the default bioethical model can potentially be clarified when juxtaposed with the care ethics paradigm. Care ethics takes into consideration what principle-based bioethics have previously overlooked: relationship, context and power.
This study is the first to demonstrate a relationship between a midwifery-led model of care and care ethics. It contributes to the existing body of knowledge by providing further insight and deeper understanding of the ethics of caring for childbearing women and provides valuable foundational information on which to explore further. Further work is required to ascertain whether care ethics would be a better fit for the midwifery model of care.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethics approval was granted by the Edith Cowan University research ethics committee REMS no. 2019-00296-Buchanan on 27 July 2019.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.