
Abstract
Research suggests that the incidence of moral distress experienced by health professionals is significant and increasing, yet the concept lacks clarity and remains largely misunderstood. Currently, there is limited understanding of moral distress in the context of midwifery practice. The term moral distress was first used to label the psychological distress experienced following complex ethical decision-making and moral constraint in nursing. The term is now used across multiple health professions including midwifery, nursing, pharmacy and medicine, yet is used cautiously due to confusion regarding its theoretical and contextual basis. The aim of this study is to understand the concept of moral distress in the context of midwifery practice, describing the attributes, antecedents and consequences. This concept analysis uses Rodgers’ evolutionary framework and is the first stage of a sequential mixed-methods study. A literature search was conducted using multiple databases resulting in eight articles for review. Data were analysed using NVivo12©. Three core attributes were identified: moral actions and inactions, conflicting needs and negative feelings/emotions. The antecedents of clinical situations, moral awareness, uncertainty and constraint were identified. Consequences of moral distress include adverse personal professional and organisational outcomes. A model case depicting these aspects is presented. A midwifery focused definition of moral distress is offered as ‘a psychological suffering following clinical situations of moral uncertainty and/or constraint, which result in an experience of personal powerlessness where the midwife perceives an inability to preserve all competing moral commitments’. This concept analysis affirms the presence of moral distress in midwifery practice and provides evidence to move towards a consistent definition of moral distress.
Introduction
A growing number of Australian midwives consider leaving the profession each year, citing reasons such as role stress and workload pressures,1,2 lack of professional development opportunities,1,3 working within a medical model of care, 4 low professional recognition and high institutional expectations in a changing demographic of care needs. 4 The inability to practice congruent with professional values due to a lack of autonomy, organisational constraints and/or poor work culture may also contribute to attrition. 1 The impact of not being able to provide care in a manner that supports professional practice values and beliefs may be described as ‘moral distress’.5,6
Moral distress is a term that was first used by Andrew Jameton
6
to label the psychological distress experienced following complex ethical challenges in nursing practice
6
where an individual is morally constrained: Moral distress occurs when one knows the right thing to do, but institutional constraints make it nearly impossible to pursue the right course of action. (p. 6)
6
Further to the two types of moral distress described above, repeated exposure to morally distressing situations is thought to progress to what Epstein and Hamric 12 refer to as ‘moral residue and the crescendo effect’(p. 330). This type of moral distress is believed to arise from the cumulative effect of working in environments of low ethical climate. 12
In many health professions including nursing, medicine, physiotherapy and midwifery, moral distress has been identified as a concerning feature of clinical practice.8,13–16 Withdrawal from client care,17,18 workforce attrition18,19 and psychological harm 18 have been linked to moral distress. While there is a growing interest in moral distress and its impact on health professionals, there are varied definitions that lead to confusion and a lack of clarity. 5 Despite this, it is agreed that moral distress is a legitimate and disturbing phenomenon that needs to be better understood within the varied paradigms of healthcare practice.5,20–22
Although moral distress is considered an important issue in practice, the cautious use of this term is largely due to theoretical and contextual confusion, 23 with health professionals not able to articulate this in the context of their experiences. 23 The purpose of this article is to present a concept analysis to explore moral distress in midwifery practice. Using Rodgers’ 24 evolutionary concept analysis framework, characteristics, antecedents and consequences of midwifery practice will be examined. Following this, a model case will be proposed and a contextual definition will be provided.
Methods
It is argued that when a concept is abstract or not well defined, it limits the ability of an individual to communicate its presence. 24 A concept analysis can be useful in these situations as it can contextualise and clarify how the terminology is used, strengthening the theory and distinguishing it from other related concepts. 25 While there are multiple strategies for undertaking a concept analysis, Rodgers’24,26 evolutionary concept analysis promotes a cyclic inductive process that acknowledges the fluidity of concepts as they change with time and context. This approach was deemed most appropriate, as it advocates a view of the contextual and individualistic nature of experiences such as moral distress.
The seven-step framework provided by Rodgers 24 seeks to determine the use of a concept within the literature as a basis for continual development.24,27 The steps include the following: (1) select a concept of interest; (2) identify related terms and relevant uses of the concept; (3) identify and select an appropriate realm (sample) for data collection; (4) identify the attributes of the concept; (5) identify the references, antecedents, and consequences of the concept, if possible; (6) identify concepts that are related to the concept of interest; and (7) identify a model case of the concept (p. 333). 24 As a cyclic framework, the steps do not need to be undertaken in any specific order, and Rodgers 24 promotes the adaptation of the framework to meet the needs of each concept as it is presented within the literature. All seven phases of Rodgers’ framework have been adopted for this study (Figure 1).
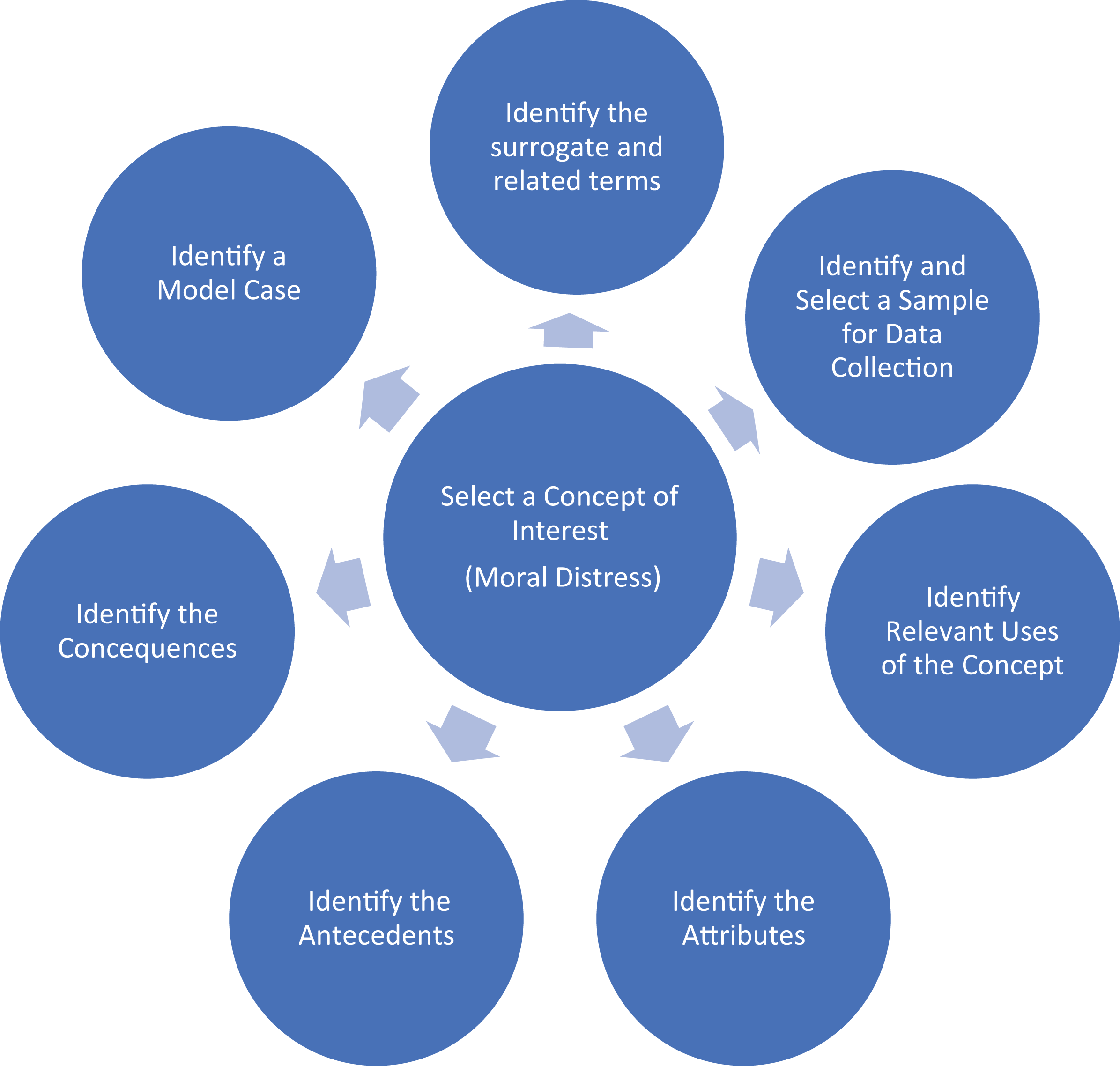
Concept analysis framework. Adapted from Rodgers. 24
Identify related terms
At times, individual concepts may appear ambiguous, and this can be associated with the use of related terms.24,27 It is suggested that this is a ‘problem of terminology rather than a problem of concept’ (p. 333). 24 The first step of this concept analysis was to identify related terms. This occurred before the formal literature search to enable insight into the concept and how it could differ or relate to other concepts. Currently, there is no dictionary notation provided for the phrase ‘moral distress’, and although mentioned in some nursing texts, 28 it is not recognised as a diagnosable psychological disorder.
The word ‘moral’ (adjective) is defined as ‘of or relating to principles of right and wrong in behaviour’. 29 Related terms for moral include ethical, virtuous and righteous. 29 As a primary source of confusion, the terms morals and ethics are often used interchangeably. While morals have been defined as the character and virtue of doing the right thing, ethics is the philosophical study of moral actions. 30
The word ‘distress’ (noun) is defined as ‘pain or suffering affecting the body, a bodily part, or the mind’. 31 Stemming from the French term destresse, meaning ‘restraint or affliction’, 31 it implies that an individual has sustained an insult to his or her psychological or physical health. Related terms include: affliction, agony, anguish, hurt, misery, pain, torment, torture and woe. 31 Outside of dictionary definitions, one term related to moral distress that was identified was ‘stress’. The confusion between stress and distress is well recognised. 32 In an attempt to distinguish the two terms, it is stated that distress is a failure to return to a ‘normal’ state of function following a negative experience. 32 Stress, however, is defined as ‘constellation of behavioural or physiological mechanisms to counter the perturbation and return to normalcy’ (p. 20). 32 From this definition, it could be assumed that although stress may precipitate distress, it is characterised by the ability of the individual to use mechanisms to manage or cope with the situation. Conversely, distress occurs when the insult surpasses the coping mechanisms of the individual, causing a lasting negative psychological impact. 32
The terms moral constraint, moral uncertainty and moral dilemmas have all been considered in establishing a true definition of the concept of moral distress and are therefore inter-related. 33 A moral constraint can be considered as any barrier impacting an individual’s ability to follow what they believe to be the right action.6,11 The key feature of moral constraint is that the individual must have a clear understanding of what the correct action should be, but feel there is a barrier preventing them from acting.6,33 Conversely, moral dilemmas have been referred to as ‘cases in which morality itself pulls a person in competing directions’ (p. 5). 11 Moral dilemmas, from this definition, indicate the individual has two possible actions, with neither preferable over the other. The result of a moral dilemma is that the individual is not able to meet the moral needs of all parties involved in the situation. Moral uncertainty refers to experiences in which an individual is not clear on the best possible action to take. There may be several possible actions; however, the individual is unsure of which would best meet the moral requirements of the situation. In both moral constraint and moral dilemmas, the individual can determine possible correct moral actions, which is not possible in moral uncertainty. Moral uncertainty has been defined as ‘the inability to determine the “right” course of moral action to pursue’ (p. 1). 34
Moral injury and moral distress are thought to be closely related,35,36 though the terms moral stress, 37 ethical stress 38 and ethical distress 39 have also been used through the literature. Moral injury is most commonly referred to in the context of military veterans and traumatic stress-related injury. 40 Although the two terms are often used interchangeably, it has been proposed that they are two separate conditions that present across a continuum 36 (Figure 2).
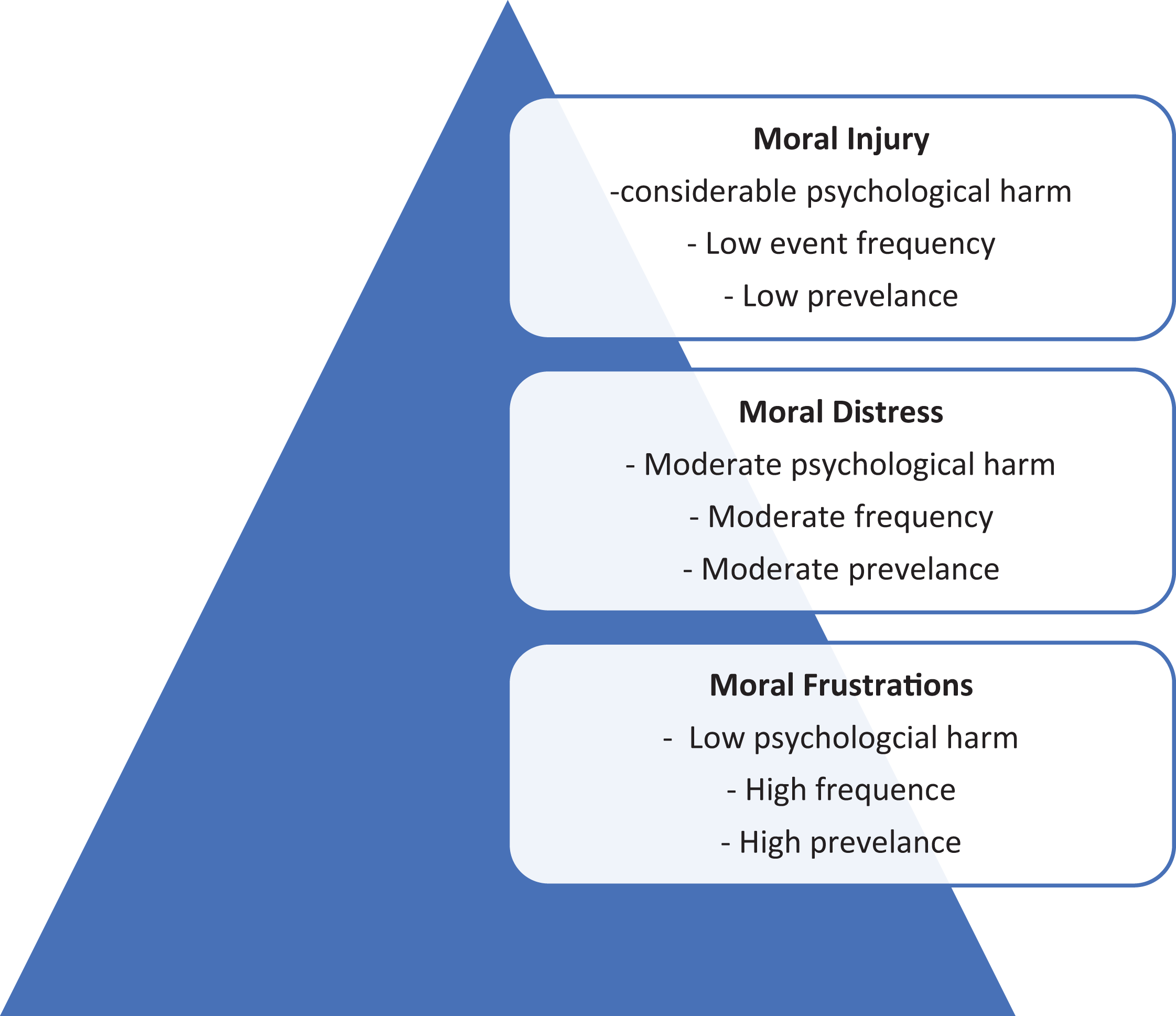
Types of moral compromise. Adapted from Liz and Kerig. 36
Identify sample for data collection
Three databases were searched: PsycINFO, OVID-Medline and OVID-Emcare. The Internet search engine Google Scholar was subsequently searched to identify any additional research that had been overlooked by the initial searches. These searches used combinations and truncations of the key terms including moral, distress, midwife, maternity, obstetric, nurse and maternal-child nurse. The terms nurse and obstetric were included to potentially capture experiences of maternity care workers without the title of midwife (Table 1). Due to the recommendations of Rodgers 24 to gain a historical perspective of the subject, no date limited was applied to the search.
Search strategy example.

A total of 91 articles were identified, and following the removal of duplicates, 56 articles remained for review. The abstracts of all 56 articles were assessed for relevance. Research concerning the experiences of neonatal nurses was initially considered as many midwives also practice within neonatal units; however, these papers were subsequently excluded as they either pertained specifically to the role of the registered nurse or focussed on the neonatal intensive care unit which is outside of the scope of the midwife. One article 41 considered moral distress in nurses working in surgical units providing care to women having a termination of pregnancy (TOP). While this was initially included, the scope of the participants being surgical nurses rather than midwives excluded them from the final review. One article referred to the experiences of a labour and delivery nurse. 8 This study was the first to describe moral distress in the maternity care setting. Although it is acknowledged that nursing and midwifery have different professional philosophies, midwifery as a standalone profession was not recognised at the time of the study (1984) in many countries. While this study 8 did not refer specifically to midwifery practice, given the relevance to midwifery practice, it was deemed as acceptable for this review. The database search resulted in seven articles, with one additional article retrieved from the Google Scholar search, totalling eight articles for the final review (see Figure 3). Included and excluded articles were reviewed by all members of the research team.
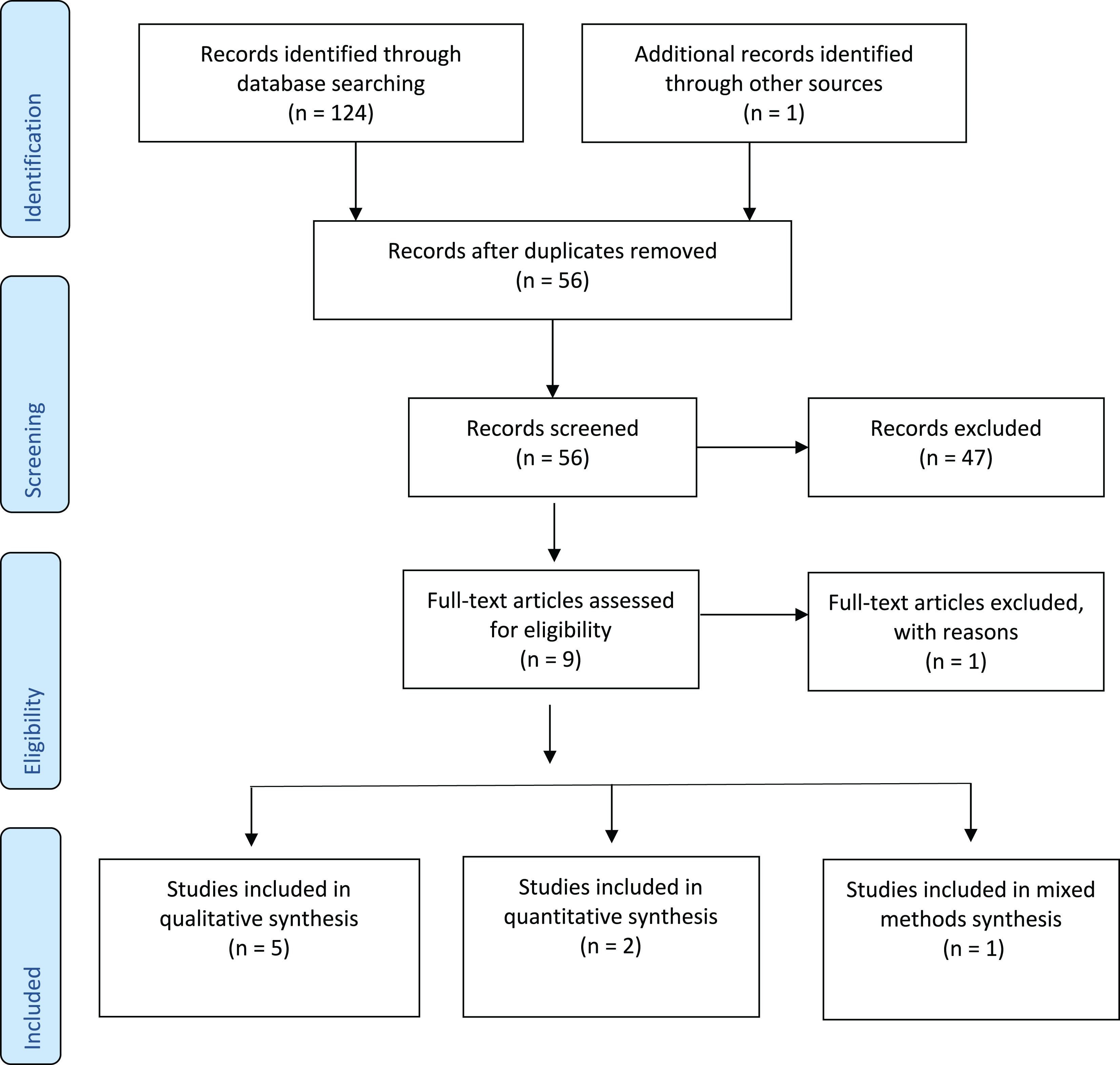
Prisma flow diagram. 42
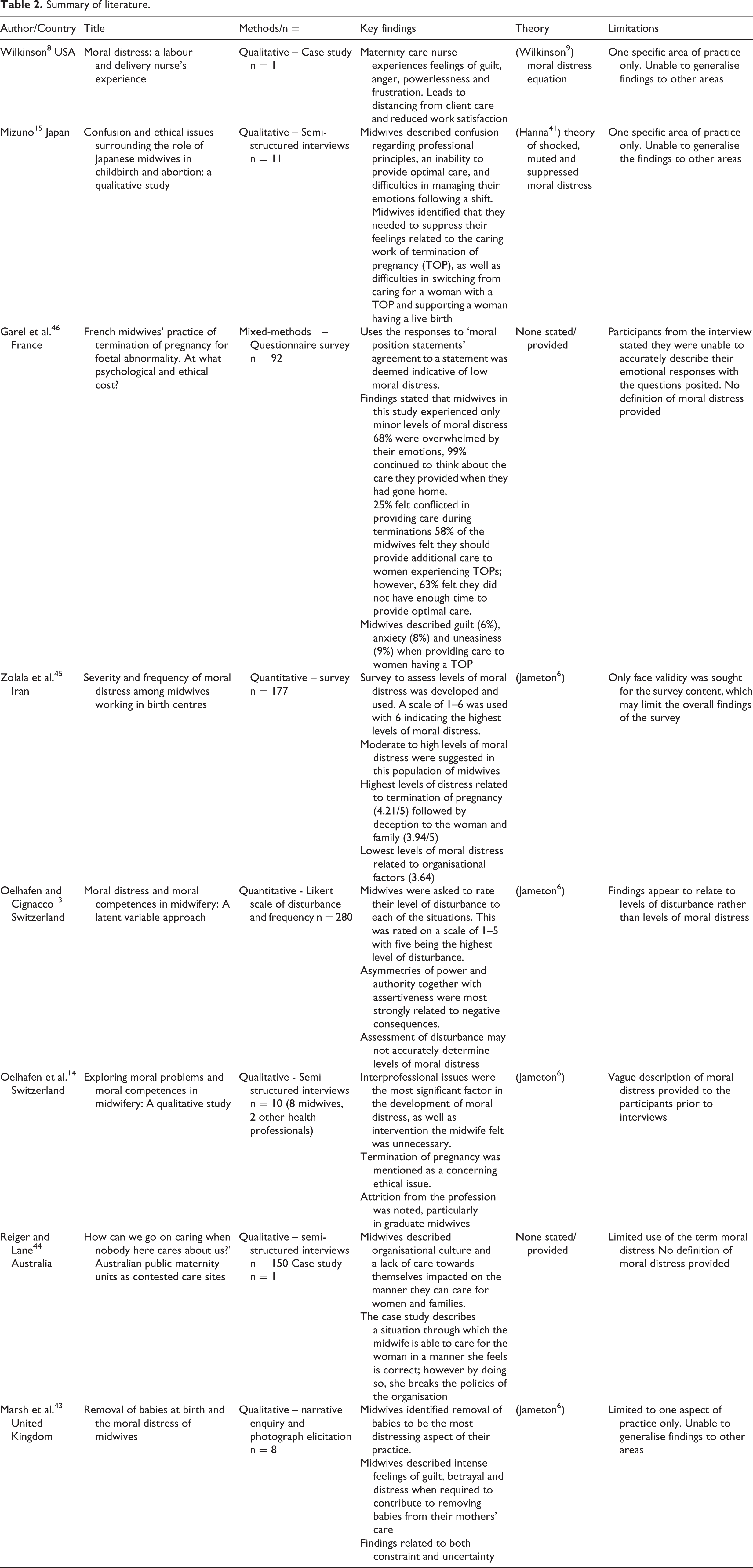
Of the eight articles included in this concept analysis, five were qualitative,8,14,15,43,44 two were quantitative13,45 and one mixed-methods 46 research (Table 2). Included articles described care during labour and birth, TOP, removal of babies from their mother for child protection orders, as well the daily work of midwives and the contested nature of maternity care systems. This literature described attributes of moral distress from the late 1980s, with all but one of the articles undertaken since 2007.
Summary of literature.
Data analysis
All articles were read a minimum of three times prior to data extraction and analysis. This allowed for immersion into the research, promoting a deep understanding of the methodology, associated findings and limitations of each study. All articles were coded using NVivo 12© software. Top-level nodes were named as attributes, antecedents and consequences. Using these three nodes as a guide, a thematic analysis of each of the articles was undertaken. The coded data were subsequently reviewed by the other members of the research team, and agreement was achieved.
Findings
Identify the attributes, antecedents and consequences of the concept
Following Rodgers’ 24 framework, it is necessary to identify attributes, antecedents and consequences. This process is described as the ‘core analysis phase’ (p. 24). 27 The attributes of a concept have been described as the characteristics of specific situations that the concept occurs within, while antecedents are events or experiences that arise prior to the concept occurring. 27 The consequences refer to the outcomes or impact of the concept occurring within a specific context. 27
Attributes
Three core attributes of moral distress in midwifery emerged from the literature, namely, concerns surrounding moral actions and inactions, meeting conflicting needs, as well as negative feelings and emotions. Although these attributes were identified individually, they were most often interwoven within the context of each interaction.
Action and inaction
Action and inaction were strongly related to other aspects of moral distress, particularly meeting competing demands. Action referred to any instances where the midwife felt she was contributing to harm during her care of the woman.14,43 Inaction related more specifically to situations where the midwife did not speak up or challenge or aspects of care that they felt was detrimental to the woman or her interests.8,43
In specific situations, such as the removal of babies from their mothers, the midwife felt her actions were in opposition to her professional obligation to the woman. 43 In these situations, the midwife felt her actions were harming the woman. Participating in TOPs was also seen as an action that contributed to the development of moral distress. Midwives felt that although they were in many cases, not opposed to the woman’s choice to terminate her pregnancy, the action of giving the medication left them feeling that had contributed to harming the foetus.13–15,45,46 This was also identified through examples where midwives felt they were contributing to harm when they were asked to administer medications to expedite labour and birth, without what they felt was adequate rationale.14,45
Inaction referred to any time when the midwife felt she was unable to speak up to support the woman. Midwives often felt conflicted when they did not agree with other members of staff, or they did not advocate for the woman when they felt it was warranted.8,43 This related to aspects of care such as interventions the midwife felt were unnecessary, 45 as well as derogatory comments made about the woman by other members of staff,43,45 Midwives often felt a sense of obligation to uphold the decisions made by medical staff. This was attributed to both hierarchical structures within the organisation,8,14,44 and a perceived loyalty to the doctors, despite disagreeing with their chosen course of care.8,13,14,43,45 This situation was further complicated as the midwife attempted to balance feelings of conflict regarding her responsibility to advocate, but also as being co-responsible for the action or intervention. 14
Inaction was further described when the midwife was not able to provide care due to organisational issues, particularly inappropriate staffing, excessive paperwork and inexperienced medical staff.14,44–46 Low staffing levels prevented the midwife from providing care they felt was optimal to the woman’s needs, as the midwife prioritised one aspect of her responsibilities over another.14,44 This led the midwife to feel as though she could not provide the level of care the woman required, posing significant safety concerns.14,44–46 The safety concern translated to a moral consideration as the midwife did not feel the woman or baby would have adequate care should higher-level support be required. In this instance, the inaction was derived from institutional constraints on the midwife’s ability to deliver appropriate care.
Conflicting needs: loyalties, priorities and values
Conflicts regarding the midwife’s loyalties, priorities and values were three separate yet intertwined attributes under the attribute of conflicting needs. Conflicting loyalties relate to the discordance between the mother–midwife relationship and interprofessional relationships. Conflicting priorities refer to organisational demands, while conflicting values refer to care the midwife provided she felt was not congruent with her own personal values and beliefs.
Conflicting loyalties
Midwives in this analysis detailed the importance of their relationship with women and their philosophical understanding of the holistic nature of their role.43,44 Any situation that was seen to oppose these professional values caused conflict for the midwife. This was seen primarily through interactions where the midwife felt she was betraying the woman through withholding information. The term ‘deception’ was used often when describing the conflict that the midwife felt when she was required to withhold information or be dishonest in her communications with a woman and her family.8,43,45 One of the key concerns for the midwife when removing babies from their mothers was the perceived betrayal. 43 Quotes from midwives stated that although they felt an obligation to the baby, they were conflicted in how their loyalty should be divided between caring for the baby and the mother, when their needs were not congruent with each other. 43
Conflicting priorities
The conflict between organisational demands and providing quality care was evident.8,14,15,44,46 Low staffing, as well as excessive documentation, was highlighted as barriers to care, and midwives often felt obligated to undertake these administrative and task-driven activities over the provision of quality care. One example of this compromise was demonstrated when midwives had requested shorter appointment times to see all of the women requiring care. 44 This request compromised the midwives’ professional values of providing wholistic, safe and appropriate care in favour of meeting the organisational demands attending to a large volume of women. 44 In this instance, it is the quantity over quality approach to the maternity care that led to moral distress.
Conflicting values
Conflict with personal values was most identified as an interwoven aspect of caring for women experiencing a TOP. While many of the midwives described their obligation to the woman and their professional responsibility, specific circumstances, such as disagreeing with the rationale for the termination, were a cause of distress.15,45,46 One study identified that 25% of the midwives in their study cited social, religious or spiritual reasons for feeling uncomfortable caring for a woman experiencing a TOP.
46
A midwife in a separate study stated, Why should this baby have life, but that baby cannot?…I don’t know what human destiny is…I wonder whether a healthy child is being terminated…the child may become a great artist! (p. 504)
15
Of particular concern was the ethical issue of how to proceed if the baby in late terminations displayed signs of life. 46 This concern was described as a dichotomous position of midwives working between birth and death and the moral implications this could have. 15
Negative feelings and emotions
Fear, guilt and confusion were examples of negative feelings and emotions attributed to moral distress. Many of these emotions related to hierarchical medical models of care and a perceived inability to speak up.43,44 This finding was thought to be of particular concern for less experienced and graduate midwives. 14 Fear often related to wanting to advocate for the woman, yet also fearing liability if there was a negative outcome. 14 Guilt was expressed in a sense of failing to help in relation to both advocacy 8 and TOP.15,46 When caring for women experiencing a TOP, guilt, anxiety and sadness were all expressed.15,46 Midwives, however, also felt they needed to suppress their emotions to continue caring for women, especially when they were required to change from caring for a woman having a TOP to a woman having a live birth.14,15,46
Antecedents
An antecedent refers to something that must be in place for an outcome to occur. 27 It is important to note that according to Rodgers’ 24 framework, the antecedents should not be thought of as an empirical set of structures that must be in place, but rather a suggestion of preceding factors that may influence the development of a concept. Consideration should be made for the fact that moral distress is an individual response and is therefore difficult to apply in a broad sense. The individualistic nature of moral distress was emphasised in the finding that midwives were not able to describe a uniformed phenomenon when exploring incidences of moral distress. 14 It appears from this analysis, however, that moral distress arises when the midwife experiences a clinical situation in which her value systems are compromised following a significant moral situation. It is indicated from this statement that the antecedents include: (1) a moral clinical situation; (2) recognition of individual values and beliefs and (3) perceived moral constraint, moral dilemma or moral uncertainty.
Moral clinical situations
For moral distress to be present in the context of midwifery practice, there must be a clinical situation that holds a moral concern for the midwife. Ultimately, midwives in this analysis described any practice in which they provided care to a woman to be a moral situation; one that they felt had been built on the professional values of woman-centred care, trust, honesty and autonomy.14,43–46
Individual values and beliefs
Outside of professional duty, however, situations that challenge the midwife’s own personal beliefs and values may also lead to moral distress. It is difficult to determine what these situations may be as they are unique to each individual. For example, as described through this analysis, only 25% of midwives found it to be morally concerning to attend a woman experiencing a TOP. 46 However, another midwife in the same study indicated that her duty to care outweighed any personal feelings or moral concern. 46 From the examples provided above, it is implied that the midwife must be able to identify their own personal and professional value systems and situations that compromise them to experience moral distress.
Moral constraint, moral dilemma or moral uncertainty
The final required antecedent appears to be a limitation on the midwife’s moral agency. This limitation may refer to a constraint, a dilemma or uncertainty of moral action. Moral constraints indicate that there is a barrier impacting on the midwife’s ability to take a correct moral action. This referred to organisational issues such as inadequate staffing, hierarchical professional relationships and extraneous tasks.14,15,43–46 Moral dilemmas refer to situations in which the midwife was not able to rationalise a correct course of action between two possible solutions. This referred to situations such as balancing feelings of deceit to the woman or addressing safety concerns for the baby in the case of child protection orders.
43
Moral uncertainty was highlighted in situations when the midwife was not sure of her professional or moral obligation within a situation. This uncertainty commonly referred to within the context of TOP,
15
as well as times when the midwife was not sure of her convictions to act.
14
Moral uncertainty and the challenging decision-making process were described well by one midwife who stated, It’s always a balancing act. Is it worth getting involved? Or maybe I’m exceeding my competence? (p. 1378).
14
(Midwife)
Consequences
The consequences of moral distress were described in six of the eight studies reviewed.8,13–15,43,44 Identified consequences included negative personal, professional and/or organisational outcomes. Consequences may be long or short term, with varying degrees of intensity and impact. Short-term consequences related to negative feelings and difficulty in ‘switching off’ following shifts. One study identified that the nurse/midwife would often think badly of themselves as people and professionals, due to their failure to act. 8 Feelings of anger, frustration and guilt were also key features,8,14,15 as well as an inability to ‘let go’ following a shift.8,14
The long-term effect of moral distress was both personal and professional. On a psychological level, midwives described ruminations of specific situations long after the event had occurred. One midwife stated that many years later, she still experienced flashbacks regarding her actions within a moral situation. 43 The long-term professional impact indicated that with repeated exposure to morally distressing situations, midwives would choose to work in casual and agency-based employment to avoid negative workplace culture 44 and/or withdraw from caring and become less sensitive to the needs of the women. 8
When considering moral distress as a factor impacting workforce retention, it was identified that if the coping skills of the midwife were severely challenged, midwives may consider leaving the profession. 8 Cases where staff had left their positions following morally distressing experiences and unethical hospital environments were reported. 14 Although no correlation was establish between moral distress and intent to leave the profession, this finding was based on a level of disturbance rather than the level of moral distress. 13 This gap in knowledge highlights the need for a validated scale to assess moral distress in midwifery and explore its impact on the profession.
Identify a model case for the concept
Identifying a model case is the final step in Rodgers’s concept analysis, providing an illustration to contextualise the attributes, antecedents and consequences of a concept. 27 The following case has been developed through examples synthesised from the literature in the preceding analysis. 43
A midwifes’ story
On an early shift in the labour and birthing ward, Suzie takes handover of Peta, a 21-year-old woman having her third baby at 39 + 3 weeks’ gestation. She is being induced, as she is currently in unstable housing, and has a history of drug misuse and domestic violence. Peta does not have either of her previous children in her care.
Suzie receives relevant clinical handover from the nightshift midwife in the room regarding Peta’s antenatal history and the labour to this point. Following handover, the nightshift midwife asks Suzie to check some medication in the next room. Following the nightshift midwife, Suzie is informed that the baby will not remain in Peta’s care, and that child protection services would be removing the baby soon after birth. Suzie is told that she will need to tell Peta that the baby is tachypnoeic so they can take the baby to the neonatal unit away from Peta.
Through the labour, Suzie builds a rapport with Peta, responding to her needs, encouraging and assisting her as required. Peta seems to respond well to Suzie and tells her how excited she is to meet her new baby. Suzie maintains her focus on Peta, yet she feels guilty, and anxious at the thought of deceiving her. She is aware that there is a sound rationale for removing the baby from Peta as she is not in a safe environment, yet she is conflicted. Suzie is aware that she has built a relationship with Peta and feels it is deceitful to lie. Suzie believes there is no clear answer to her moral dilemma. She could refuse to care for Peta, but she feels that Peta needs her support at this time. She could refuse to lie; however, another staff not known to Peta may then take the baby, causing additional stress. She could tell Peta of the plan to remove the baby from her care, but she also has a responsibility to the safety of the baby. There is no correct course of action, and Suzie feels she is not able to protect her moral integrity.
The baby is born and transitions well with an APGAR score of 9 and 10. Suzie upholds her obligation to the organisation and to the baby and tells Peta that the baby needs to be taken. Suzie leaves her shift with a headache, feeling sad, guilty and helpless. She continues to ruminate about the shift and her involvement in removing the baby. Following repeated exposure to similar situations, Suzie begins to withdraw from connecting to the woman to protect herself. Over time, the negative psychological impacts intensify, and she begins to question her own moral worth, leading to poor self-perception.
Discussion
This concept analysis has demonstrated a historical and contemporary understanding of moral distress and has explored how this concept is positioned within midwifery practice. Key terms and phrases surrounding moral distress have been identified and defined, along with a description of the attributes, antecedents and consequences of moral distress for midwives. Acknowledging the need for further research, a preliminary definition of moral distress in the context of midwifery practice has been developed. Moral distress in midwifery practice is described as a psychological suffering following clinical situations of moral uncertainty and/or constraint, which result in an experience of personal powerlessness where the midwife perceives an inability to preserve all competing moral commitments’.
The above definition clearly details the attributes of action and inaction, as well as the presence of a moral situation, and awareness of moral obligation to the woman and baby. The consequences are reflected in the requirement of a negative psychological outcome. Similar to the findings of Nathaniel, 47 this proposed definition highlights that the midwife may experience moral distress from a range of situations outside of institutional constraints.
There are similarities between the findings of this analysis and descriptions of moral distress in other disciplines, particularly nursing. The perception of harm to clients in care through action and/or inaction, meeting conflicting needs, as well as negative feelings and emotions have been detailed in one systematic review of health professionals’ interpretation of moral distress. 16 Likewise, outcomes of moral distress including negative self-perception, reduced work engagement and an inability to recover from challenging shifts have also been described.18,48
Despite the noted parallels in the description of attributes and consequences of moral distress with other disciplines, the antecedents challenge some aspects of the original theory described by Jameton 6 and Wilkinson. 9 Although it can be agreed that a moral situation must take place for moral distress to occur, what constitutes the required situation remains contentious. Issues regarding the inclusion of situations of moral uncertainty have been described, as well as the understanding of how a morally distressing situation is defined compared to other similar concepts.
As identified in the background, two possible types of moral distress have been proposed: constraint distress and uncertainty distress. Examples of both constraint distress and uncertainty distress have been identified through this concept analysis. Constraint distress has been demonstrated with the midwife describing barriers such as hierarchical relationships.14,45 In these examples, the midwife felt an obligation to the woman, yet perceived the doctors’ orders to be unchallengeable, preventing her from speaking up. Hierarchical relationships in nursing practice have also been identified as one of the organisational barriers that have prevented nurses from speaking up and preserving their moral integrity, 49 highlighting similarities in moral distress between nurses and midwives. Unlike nursing, however, the midwife is responsible for not only the woman but also the baby further complicating the moral decision-making process. Uncertainty distress was most pronounced in the examples of TOP 15 and removal of babies from their mothers. 43 The conflicting loyalties to the woman and baby, and the conflict of personal values led the midwife to feel there was no ‘right action’ to take. Although many of the articles included in this analysis followed Jameton’s 6 narrow definition of moral distress, the language of moral distress in midwifery practice reflects both uncertainty and constraint distress.
In an attempt to move towards a definition of moral distress, Jameton
22
poses the question ‘Why is it being labelled as “moral” distress and not simply as psychological distress? (p. 618).
22
Wilkinson
8
states that there is a significant difference between a stressful situation and moral distress. Providing an example of this difference, Wilkinson
8
describes a conflict of opinion between a nurse and a doctor of whether a patient requires a stool softener or a laxative. It is suggested that this could not lead to moral distress as it is a medical rather than an ethical disagreement. This example, however, fails to acknowledge the essence of morality in everyday practices of healthcare professionals, and suggests that it is possible to separate clinical and ethical decision-making. It could be argued that all clinical interactions hold a level of ethical and moral consequence, given the nature of the relationship between the practitioner and the client. One example of both medical and ethical decision-making demonstrated through this analysis was the moral distress midwives felt when required to augment labours where it was not medically indicated.14,45 Although this is a medical issue, the International Midwifery Code of Ethics states that a midwife has the ethical responsibility to the woman: Midwives encourage the minimum expectation that no woman or girl should be harmed by conception or childbearing. (p. 2)
50
In similar findings, moral distress in a nursing context become evident following situations in which the nurse did not agree with a treatment plan for a client. 7 This finding further reflects the inability to separate the clinical and ethical decision-making in practice. The midwives in this analysis described feeling of being complicit to poor practice. One example of this was described through the midwives’ role during inductions of labour. By intervening, given their understanding of the ‘cascade of interventions’, they believed they had placed the woman and baby in harm’s way.
Core to midwifery philosophy is the understanding that pregnancy and childbirth are a normal physiological process. However, contemporary practice occurs in a landscape of heightened risk avoidance and intervention, which may expose the midwife to increased incidence of morally challenging situations. According to the International Confederation of Midwives (ICM), Midwives have responsibilities to themselves as persons of moral worth, including duties of moral self-respect and the preservation of integrity (p. 2)
51
This analysis indicates that it is not always possible for midwives to meet their responsibility, leading to negative personal and work-related outcomes. It has confirmed that moral distress appears to be evident in midwifery practice and may impact the psychological welfare and professional engagement of the midwife. To support and protect the future of the midwifery workforce, further research is required to both qualify and quantify the presence and impact of moral distress in practice.
Limitations
Several limitations have been identified through this concept analysis, namely, a dearth of literature, inconsistent definitions of moral distress within this literature and the lack of acknowledgement of the individual nature of moral distress. Tofthagen and Fagerstrøm 27 suggest that approximately 30 articles is ideal when conducting an evolutionary concept analysis. While the lack of available literature is an acknowledged limitation, the breadth of historical and situational experiences detailed have allowed for a beginning understanding and a framework for ongoing research. Likewise, multiple definitions of moral distress were presented throughout the literature, which needed to be considered in the analysis process. However, these variations also provided a lens to consider a broader definition such as the possible cumulative nature of moral distress. In addition, as moral behaviour and moral distress are unique to each individual, attempting to describe moral distress as a homogeneous concept is in itself a limitation.
Conclusion
The term moral distress has been used increasingly across a range of professions since the early 21 century, with many professions seeking to understand this concept within the paradigm of their own practice. Acknowledging the lack of research focussed on moral distress within the profession of midwifery, this analysis offers a beginning definition of moral distress in the context of midwifery practice. Inherent in this definition is the understanding that clinical situations, moral awareness and instances of moral uncertainty and/or constraint may lead to the experience of moral distress. Furthermore, it should be highlighted that the consequences of moral distress are varied, and far-reaching, impacting on the midwives, women and families, as well as the organisation and profession. The findings of this concept analysis will guide further research and may inform the development of tools to measure moral distress in midwives.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
We hereby confirm that this project has received approval from the Human Research Ethics Committee at the University of South Australia. Approval was granted on 18 June 2020. Approval number 202801.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work has been support by a scholarship from The University of South Australia.