
Abstract
Background
The first COVID-19 wave started in February 2020 in France. The influx of patients requiring emergency care and high-level technicity led healthcare professionals to fear saturation of available care. In that context, the multidisciplinary Ethics-Support Cell (EST) was created to help medical teams consider the decisions that could potentially be sources of ethical dilemmas.
Objectives
The primary objective was to prospectively collect information on requests for EST assistance from 23 March to 9 May 2020. The secondary aim was to describe the Cell’s functions during that period.
Research design
This observational, real-time study of requests for Cell consultations concerned ethical dilemmas arising during a public health crisis. The EST created a grid to collect relevant information (clinical, patient’s/designated representative’s preferences and ethical principles strained by the situation), thereby assuring that each EST asked the same questions, in the same order.
Participants and research context
Only our university hospital’s clinicians could request EST intervention.
Ethical considerations
The hospital Research Ethics Committee approved this study (no. CER-2020-107). The patient, his/her family, or designated representative was informed of this ethics consultation and most met with EST members, which enabled them to express their preferences and/or opposition.
Findings/results
33 requests (patients’ mean age: 80.8 years; 29 had COVID-19: 24 with dyspnea, 30 with comorbidities). 17 Emergency Department solicitations concerned ICU admission, without reference to resource constraints; others addressed therapeutic proportionality dilemmas.
Discussion
Intervention-request motives concerned limited resources and treatment intensity. Management revolved around three axes: the treatment option most appropriate for the patient, the feasibility of implementation, and dignified care for the patient.
Conclusions
COVID-19 crisis forced hospitals to envisage prioritization of ICU access. Established decision-making criteria and protocols do not enable healthcare professionals to escape ethical dilemmas. That acknowledgement highlights ethical risks, enhances the added-value of nursing and encourages all players to be vigilant to pursue collective deliberations to achieve clear and transparent decisions.
Keywords
Introduction
In the spring of 2020, Île-de-France (Paris region) hospitals were severely affected by the coronavirus-19 (COVID-19) pandemic, with more than 8000 patients hospitalized and 2700 in intensive care units (ICUs) on April 9th. 1 According to a recent meta-analysis, 21.4% of COVID-19 patients experienced dyspnea or acute respiratory distress syndrome (ARDS). 2
In light of that situation, the influx of patients requiring emergency care and high-level technicity was a dreaded possibility. The massive simultaneous arrival of patients threatened to overwhelm Île-de-France medical infrastructures. Saturation of local hospital ICUs was feared. Healthcare professionals were afraid they would be obliged to ration ICU access to eligible patients. Indeed, other regions and countries had already faced this situation, notably northern Italy. 3 The disequilibrium between population needs and available means forced professionals in those regions to prioritize ICU access and make delicate, difficult-to-conceive-of decisions concerning allocation of limited resources, thereby creating tension among their normal practices, obligations, and possibilities. 4
As the week of 30 March 2020 approached, the 2000 Île-de-France (Paris region) ICU beds were occupied, threatening the region, 5 with foreseeable passage from limited means (level A) to resource saturation (level B). Leclerc et al. 6 defined level A as “constraint,” that is, ICU-bed capacity, despite being raised, becoming limited, while patient transfer to less-solicited ICUs was also limited; and level B as “saturation”: despite increasing capacity, ICUs are not able to manage more patients. Patient transfers to less overloaded ICUs are insufficient to control the situation. When these hospital structures reach saturation, prioritization measures are modified and can lead clinicians to make difficult choices.
From an ethical point of view, transitioning from standard operating procedures to a “constrained” situation and then to saturation degrades decision-making, respectively, from “good” to “bad’ to “dreadful.” 7 Because it adheres in real-time to the flow of hospital arrivals, resource allocation becomes arbitrary once saturation is reached, depriving new patients of ICU access that previously would have been accorded. “First come, first served” allocation is a criterion to exclude during a crisis. 6 Under these circumstances, the resource-distribution model can no longer respect the ordinary egalitarian model 8 but must obey utilitarian criteria to assure the most equitable distribution possible of resources. 9 Île-de-France hospitals reorganized their activities as of late February 2020 and substantially increased ICU-bed numbers to avoid reaching resource saturation.
Rationale
The concept of prioritization in medicine is not new or contemporary to the public health crisis. 10-12 As Mannelli 3 recalled using the example of kidney transplants, medical teams prioritize the attribution of organs by referring to preestablished criteria. The exceptional, COVID-19, public health situation and the impossibility of certain regions and countries to provide equitable ICU access opened the public debate, relayed by the media, on the justness of access to care. 13 Indeed, the magnitude of the public health crisis and its tendency to more severely affect the older adults,14-15 render the notion of prioritization highly sensitive.
Concerning ICU access for the aged, recommendations exist to guide patient orientation. 16 Decisions to admit the elderly should be made in terms of benefits and expected intermediate- and long-term survival post-ICU. 17 Indeed, patient “selection/sorting” should always be exceptional, transparent, based on a relationship of confidence, aim at being equitable, attempt to maximize benefits, be flexible, and temporary.18-19 The pandemic context renders the exercise of hierarchization of priorities for ICU access even more delicate and can lead clinicians to experience horrible dilemmas. Daugherty Biddison et al. 20 tried to modelize respirator allocation in a public health emergency (Maryland, USA) with too many patients to treat; the model built was based on deliberative democracy derived from a citizen’s forum. Two key elements emerged to avoid arbitrary decisions: other than analysis of medical criteria, such as the probability of intermediate- and long-term survival, to apply ethics rules (cited above) and respect certain principles linked to the decision-making process itself. The principles are: separate “treating” and “deciding” clinicians, and regularly reevaluate the decisions made. Notably, decisions concerning ICU resource allocation intervene in two times: first, at admission and then in the ICU. 6
Despite the rationalization of prioritization decisions, founded on objective medical criteria, these situations expose professionals to a major risk of “moral wound,” 21 hence the interest of proposing ethics support inspired by García-Gigorro et al.‘s deliberative approach to help make difficult decisions during a crisis, as recommended in March 2020 by the French National Committee on Ethics. 22
Hospitals rarely established a functional, multidisciplinary Ethics-Support Team (EST) during the first wave of the COVID-19 pandemic. Few data are available from France on the dilemmas teams encountered in which such support cells intervened. Despite the limited number of requests for EST input, this descriptive work could offer an initial basis of reflection on the functioning of such an EST and objectify the dilemmas faced in Parisian university hospitals in spring 2020.
Methods
This observational, descriptive study addressed requests made by any medical team in our university hospital facing an ethical dilemma linked to clinical decisions to offer their patients during the public health crisis.
Objectives
The primary objective was to prospectively collect information on requests for EST input from 23 March to 9 May 2020. The secondary goal was to describe the functions of a multidisciplinary EST created early during the first wave of the COVID-19 pandemic.
Ethic Support Team members and operating modalities
The EST has 15 members: an RN with a PhD in ethics co-headed the EST, a jurist, three psychologists, three geriatricians, a palliative-care specialist, two surgeons, a speech therapist, emergency medicine specialist, internists, neurologist. Seven EST members have degrees in ethics. Only clinicians participated in clinical deliberations.
The EST responded to requests 24/24 h, 7/7 days (on-call duty by telephone from 7:30 p.m. to 8:30 a.m. and weekends). In-person responses were preferred within 90 min following contact, with EST consultations made at least in pairs (physician and non-physician).
Data collection, anonymization, and analysis
Useful information corresponded to a pre-established grid (see the Appendix 1) of questions completed collectively by EST members. The preestablished information-collection grid assured that each team posed the same questions. The search for the patient’s wishes was emphasized. Traceability of the advice given was assured.
The choice of items to address the dilemmas (age, sex, pathology, clinical status, comorbidities, cognitive disorders, dyspnea, and multiorgan failure) were discussed in two preparatory meetings and derived from bibliographic sources, recommendations of Learned Societies, the French National Consultative Ethics Committee, and advice from different Ethics centers.
Responses from all clinical departments seeking assistance during ethics consultations with EST members were recorded in the grid and used for the deliberative discussions (Socratic method). The patient’s clinical information served as the foundation for those discussions to help physicians clarify their thoughts and discuss the different possibilities and make the most appropriate decision.
Data-collection forms were numbered sequentially as assistance requests arrived and were fully anonymized, containing no identifying entries (family name, hospital medical file number…). However, with the perspective of publication, the sex, age, comorbidities (not allowing identification of the patients if combined), and certain specific items that could lead to identification if combined were modified in the presentation of the results to assure patient confidentiality. That information included the patient’s wishes or, if not available, that of a relative, close friend or confidant, caregiver, designated referent. The ethical principles strained by the situation were also noted on the grid.
The EST-intervention forms were read and analyzed by different EST members, who then collegially discussed them to identify ethical dilemmas strained by the situation and the ethical principles stressed by each specific consultation.
The completed information-containing forms are stored in the principal investigator’s office and will be kept for 1 year after the publication of the paper.
Deliberations
The reflection aimed to put into perspective the patient’s preferences, the
The items taken into consideration were presented as questions to ask the clinicians, as follows. Under ordinary circumstances (i.e., outside the COVID-19 crisis), what would your decision be? Is the therapeutic proportionality envisaged reasonable in this precise situation? Is there a dilemma? Yes/no. If a dilemma is identified, what are the ethics principles strained by this situation? For example, are the principles of “do no harm” and justness in opposition.
Regulations and ethical considerations
The Sorbonne University Research Ethics Committee approved this study (no. CER-2020-107).
The patient, his/her family, or designated representative was informed of this ethics consultation and most met with EST members, which enabled them to express their preferences and/or opposition.
Results
Analysis of requested consultations
During the study period, EST intervention was solicited 33 times. Twenty-two consultations were conducted in person, with 20 visits to the patient’s bedside. 30 requests were made during the first 3 weeks of EST implementation. The mean time between the request and in-person deliberation was 32 (range: 10–90) minutes.
Patient population implicated
These patients’ mean age was 80.8 (35–94) years; 29 (88%) of the 33 patients had been diagnosed with COVID-19. At the time, EST intervention was sought, 24 (73%) of the 33 patients had dyspnea and 30 (91%) had comorbidities. Two (6%) patients had advanced directives or expressed their directives.
Types of solicitations
The reasons for these Call interventions varied. Half of them concerned a decision to refuse ICU admission, either immediately or in anticipation of the deterioration of the patient’s status. Seventeen (52%) requests came from the Emergency Department, mainly to reinforce the collegiality of discussions around reasonable or unreasonable ICU admission in the specific patient’s context and standard ICU-admission criteria. Those 17 reflections objectivized the unreasonable side of ICU admission concerning the “do no harm” principle, without any consideration of resource constraints.
Six (18%) of the 33 requests addressed the choice of therapeutic intensity among maximum care on a conventional ward, in the Continuous Monitoring Unit or high-intensity ICU. These situations highlighted the ethical strains concerning intensity modulated by the rarity of resources, as for a 78-year-old man, autonomous before the onset of COVID-19 symptoms, for whom hospitalization continued to be offered without ICU access. One of the solicitations concerned an 80-year-old woman with ARDS, refused ICU admission because of her associated comorbidities. The possibility of non-invasive respiratory assistance with high-flow oxygen therapy was raised for this patient but no bed was available in the continuous monitoring sector that day. Four (12%) requests were for non–COVID-19 patients, whose required therapeutic intensity, notably ICU admission, was discussed in the context of the current situation of constraints. The EST was consulted for an 80-year-old bedridden man, living at home with his wife, with septic shock, multiorgan failure and ARDS unrelated to COVID-19. The choice was made to admit him at the Continuous Monitoring Unit but refuse ICU access after consulting with his primary-care physician and his wife.
Two (6%) requests concerned which therapeutic proportionality to choose should confirmed or suspected COVID-19 infections worsen, in the context of a severe stroke. For one of those men, 82 -year-old, COVID-19 was rapidly eliminated and he received optimal care in the ward associated with his neurovascular disease, without modification of the therapeutic orientation that would have been made outside the COVID-19 context. For the other patient, a 78-year-old with a clinical picture of COVID-19 who had suffered a massive stroke, it was decided to pursue treatment of his neurovascular disease in the absence of confirmed severe acute respiratory syndrome–coronavirus-2 (SARS–CoV-2) positivity.
Two (6%) other requests for interventions concerned decisional dilemmas between high-intensity care and the risk of morphine administration to provide symptomatological relief of polypnea. The tension appeared between a curative orientation and the notion of patient comfort. Both patients had received morphine based on the advice of a palliative-care specialist (also an EST member). Such clinical situations have improved with the establishment of morphine administration without impairing the patient’s respiratory function.
Advice was sought a posteriori by a nursing team concerning the terminal management of a 64-year-old man, ineligible for intubation because of numerous comorbidities (prior stroke, myocardial infarction, obesity, and diabetes) that rendered invasive ventilation unreasonable. The dilemma concerned alleviating dyspnea symptoms (morphine administration in the context of polypnea (45 breaths/minute) versus continuance of curative therapy (non-invasive ventilation). This same patient had been the origin of another request the day before concerning resorting to morphine use versus providing high-intensity care.
One solicitation concerned a 39 -year-old mentally handicapped woman, with other associated comorbidities (heart disease, obesity, and diabetes). This patient was receiving non-invasive ventilation the day of the request, but her behavior in response to treatment was counterproductive (she took the mask off). The solicitation was made to anticipate deterioration and reflect beforehand on a potential ICU admission. This deliberation was conducted with several medical team participants. It was decided to pursue non-invasive ventilation, with reevaluation of her clinical status and to admit her to the ICU if necessary.
Discussion
Early choice of treatment intensity and orientation
Analysis of the different ethics-related solicitations showed that half of them (i.e., 17) concerned the initial decision of ICU admission in a context of resource constraints. A majority (12/17) of those requests came from the Emergency Department, which is explained by the severity of the symptoms of patients admitted with SARS-CoV-2 infections, as found in an Australian epidemiological study on 240 (16%) of 1508 patients, consulting the Emergency Department, who met inclusion criteria 23 (of 122 (67%) with acute dyspnea, 108 (56%) with cough, 98 (51%) with fever, and 5% of whom had hypoxia). The importance of the decision to transfer the patient directly to the ICU from the Emergency Department was paramount for the patient’s future 24 and undoubtedly explains the high percentage of referrals originating there.
Examination of those 17 intervention requests showed that the decision-making process being used seemed to correspond to that in force to prioritize patient ICU access, 12,17,25,26 outside the pandemic situation. The choices were made based on objectivized medical criteria. 10,12,27 Medical reflection concerning ICU admission for invasive ventilation is a routine practice for the teams involved. Those considerations aim to meet “first, do no harm” principles, compassion, and autonomy, 28 while taking clinical parameters into account. 29 It should be noted that resource-allocation models predated the pandemic. 10-12
Weight of limited resources on their allocation
During this crisis, resource allocation (which became constrained) was nonetheless a real preoccupation for all clinicians. 30 The goal was to assure access most equitably as possible to treatments in a context of potentially insufficient means, in light of what could initially have been feared in the Paris region. 5 More specifically, for our EST’s experience, it was to ensure a decision-making process maintaining the patient’s best interests and based on a deliberative model. The objective was to avoid recourse to “poor decisional criteria,” such as those described by Hereros et al., 31 that is, age, “social value” or order of arrival “first come, first served.”
While evaluating the other request motives, it became clear that clinicians retained the notion of limited resources when choosing treatment intensity. The possible options were organized around four axes: maximum care in wards (conventional oxygen therapy), intensive care (non-invasive ventilation), ICU, and palliative care. Some choices seem to have been made for lack of another option or as a way to save ICU-relevant resources. The therapeutic proportionality, notably the indication for ICU admission, was highly sensitive for SARS-CoV-2–infected patients because assessment of their prognoses was difficult, even impossible. 32 In addition to the difficulty of determining the expected benefits according to the therapeutic options, the notion of limited resources probably played a role. The results of the randomized study by Valley et al. 33 showed that knowing that ICU beds were available influenced clinicians in their estimations of expected benefits of ICU care. Although the Paris region situation never reached the saturation threshold, the rarity of resources undoubtedly weighed on the process of attributing ventilators, as in other regions and countries.34,35 The concept of “sorting” to attribute a rare resource (like invasive ventilation), as much as choosing between two patients with equivalent clinical statuses, was not encountered in the deliberations analyzed.
Limited extrapolations
However, the number of EST-intervention requests made represents only a very small proportion of the decisions made during management of the health crisis, making it difficult to generalize conclusions concerning sorting and prioritization. Questions surrounding those concepts require that they be put into perspective with the idea of proportionality of proposed treatments. The therapeutics offered were proportionate to the patient’s specific situation, which probably reduced the arbitrariness of prioritization.
Choice of the evaluation model and relationship to recourse to specific criteria
Evaluation of the patient for whom the EST was solicited was achieved using a synthesis of collected information: items inspired by the fragility-scale rating 36,37 comorbidities or the Sequential Organ-Failure Assessment score to estimate clinical disease severity. 38 That evaluation corresponded, in part, to an examination of the parameters recommended to address ICU-admission decisions. 39
The EST members’ choice of listing these criteria—and not entirely applying those different clinical evaluation scales—to propose recommendations was justified by the intention to initiate exchanges on broad topics with deliberative discussions (see the grid). The goal was to encourage open debate by avoiding a routine list of criteria. This approach was also intended to maintain the centrality of the patient’s preferences, highlighting his/her uniqueness in this discussion, while preserving maximum decisional reasoning as close as possible to that routinely applied, based on the patient’s best interests. The contribution of an unambiguously applied fragility-scale score was discussed in terms of its ability to predict survival of aged patients. 27 The Clinical Frailty Scale seems to have good capacity to predict mortality of individuals > 80 years old 40 admitted to the ICU and its systematic use could potentially be a criterion of interest.
It should be noted that predictive medical criteria on which to base treatment intensity choices, notably ICU access, are not always sufficient, as shown by a 2009 English study on management of the flu pandemic. 41 They should be discussed for each unique situation.
Shared decisions
Unlike the suggestion of 20 that the solicited ethics team be totally isolated from the clinical team treating the patient, our EST chose to establish a multidisciplinary dialogue with the treating team and to deliberate how to resolve the situation together. The originality of our approach was to combine the different perspectives by responding to intervention requests in at least pairs of a nurse and/or a psychologist and a physician. We have not found a similar multidisciplinary ethics-support strategy reported during the first COVID-19 wave.
Decision management
Management of the decision revolved around three axes: the reasonableness of the decision for the given patient’s situation, the feasibility of decision application and, lastly, the possibility of offering adapted care respectful of the patient’s dignity. These points correspond to the model proposed by Leclerc et al. 6 The proportionality of care is organized in four categories: ICU with a ventilator, high-intensity care with non-invasive ventilation, maximum care in conventional hospital wards (maximum oxygen therapy 15 L/minute) and palliative care. Few articles have described such an approach to care offered during the COVID-19 crisis. Moreover, the decision could be revised from 1 day to another, as recommended by the model of Daugherty. 20 The possibility to offer proportionate care coincided with more beds in continuous care and creation of an acute palliative care unit, similar to that described by Fausto and al. 42 That strategy was part of a group of ethics measures characterized by an organization around hospitalized, palliative care patients so their relatives could visit.
One of the strengths of our approach was the in-person evaluation of the patient when possible. Also, EST members could form their own ideas of the patient and his/her clinical state. Being in the presence of the treating team exposing the situation could contribute to facilitating the emergence of questions, doubts and elements at stake, potentially sources of tension (attachment to the patient, differences with the family, difficulties reflecting the patient’s perceived suffering during treatments or because of disease severity…). The collegial procedure was thus reinforced and the decisional burden distributed among clinical deciders and EST members. The multidisciplinary approach enabled elaboration of the perspectives and to avoid as much as possible, subjectivity associated with their profession(s). Diversification of discussion participants’ profiles is recognized as adding some value in ethical decision-making.43-45
Conclusion
The COVID-19 crisis forced hospitals in many countries to envisage prioritization of ICU access, especially because of the rationing of the number of available respirators. 35 Some recommendations concerning patient-prioritization criteria were devised at the onset of the pandemic.46-48 However, the existence of decision-making criteria and protocols does not enable healthcare professionals to overcome ethical dilemmas surrounding the justness and equity of resource allocation and access to care, and in no way avoids the “moral wound” risk. 8 It seems important to offer clinicians support to help deliberate in these difficult circumstances. Our experience in creating the EST showed that it is possible to rapidly mobilize this type of support. The availability of such a resource could prove useful in certain circumstances, notably to reinforce collegiality and deliberations of uncertainties. The existence of such a multidisciplinary team and its institutional recognition represent strong signals that the dilemmas raised by COVID-19 require the input of all players. That acknowledgement puts a spotlight on the ethical risks encountered during this type of health crisis, enhances the added-value of a multidisciplinary approach and encourages healthcare professionals to be vigilant to pursue collective deliberations to achieve clear and transparent decisions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix
Information-collection grid filled out for each request for ethics-support team (EST)-intervention.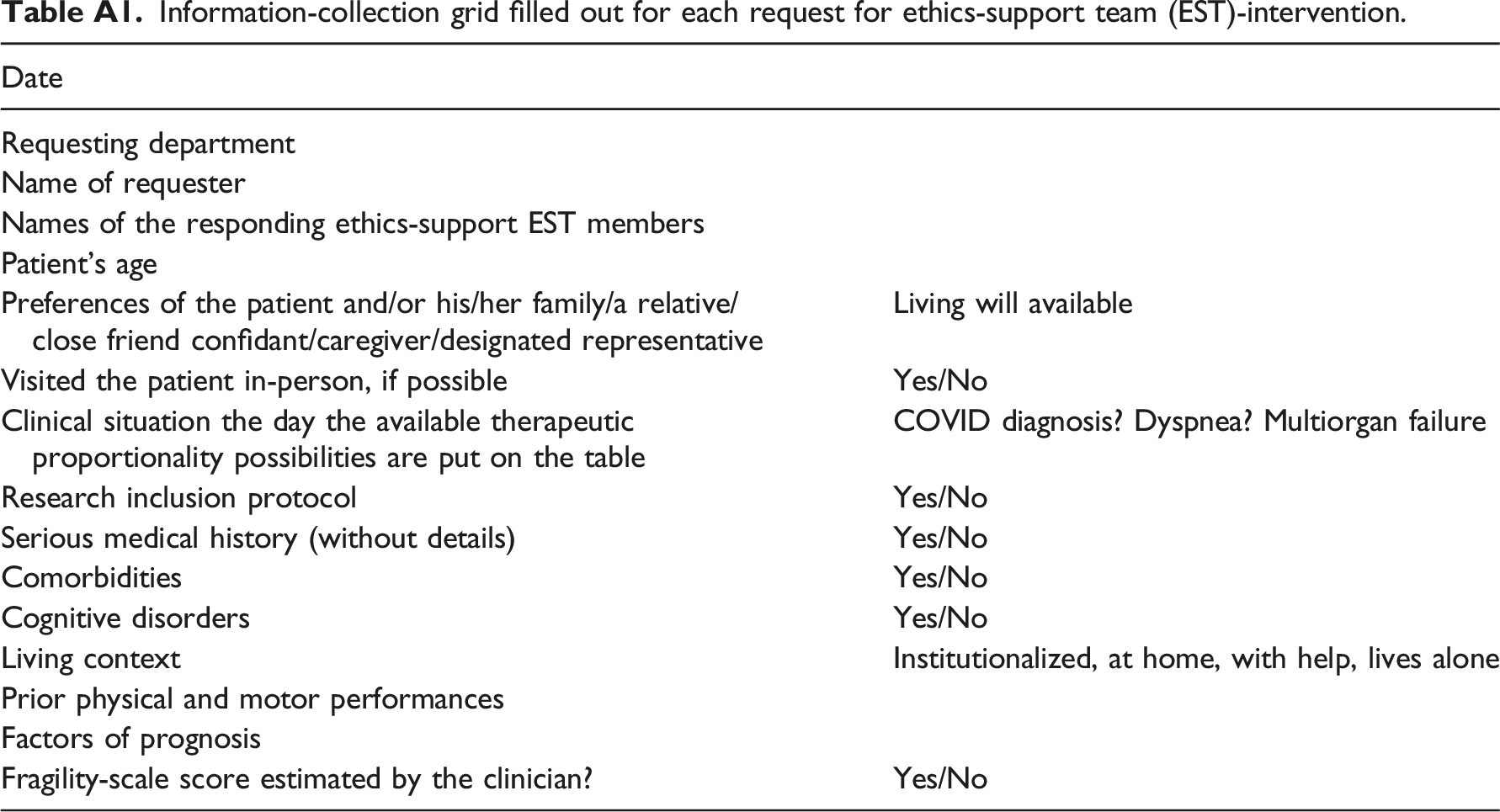
Date
Requesting department
Name of requester
Names of the responding ethics-support EST members
Patient’s age
Preferences of the patient and/or his/her family/a relative/close friend confidant/caregiver/designated representative
Living will available
Visited the patient in-person, if possible
Yes/No
Clinical situation the day the available therapeutic proportionality possibilities are put on the table
COVID diagnosis? Dyspnea? Multiorgan failure
Research inclusion protocol
Yes/No
Serious medical history (without details)
Yes/No
Comorbidities
Yes/No
Cognitive disorders
Yes/No
Living context
Institutionalized, at home, with help, lives alone
Prior physical and motor performances
Factors of prognosis
Fragility-scale score estimated by the clinician?
Yes/No