
Abstract
The dual purpose of this article is to present a formal theory analysis combined with recommendations for the use of social justice in nursing as a framework for the study of obstetric violence in US hospitals. A theory analysis of emancipatory nursing praxis as a middle-range theory of social justice in nursing was conducted using the strategy by Walker and Avant. The theory of social justice in nursing was determined to be logical, useful, and generalizable. The soundness and usability of the theory support the recommendations made for it to be applied to the study of obstetric violence, plus quality and outcome problems in maternity care that have been resistant to sustained progress and may benefit from a new paradigm for continued study. The alignment for obstetric violence to be studied with a social justice framework is linked to the theory’s origins in critical social theory and the evolving concept of obstetric violence as a sex-specific form of violence against women that is a violation of human rights. The postmodern expansion of the body of work based on critical theory provides examples from emancipatory and feminist researchers for recognizing how the study of obstetric violence is compatible with a theoretical framework for social justice in nursing. The suitability of this framework to guide the further research needed to better understand, identify, and minimize harms from the occurrence of obstetric violence is argued. In addition, “The Code” for the American Nurses Association (ANA) is cited as a professional reference that outlines nurses’ responsibilities for practice based on ethics, human rights, and social justice that are antithetical to the occurrence of obstetric violence.
Keywords
Introduction
The purpose of this article is to conduct an analysis of emancipatory nursing praxis as a middle-range theory of social justice by Walter 1 using the strategy for theory analysis by Walker and Avant. 2 In addition, social justice in nursing is recommended for its suitability as a framework for the study of obstetric violence in US hospitals. A discussion about why persistent quality and outcome challenges in maternity care can benefit from the application of a social justice framework, because of an alignment with the origins and progression of critical theory, is also addressed.
The World Health Organization (WHO) identified the disrespectful and abusive treatment women experience at facilities worldwide as an important public health and human rights issue.
3
Many examples of disrespect and abuse during childbirth around the globe also apply to childbirth in the United States, yet obstetric violence has been absent in research from the US healthcare sector. Women along the childbearing continuum have been reported to experience psychological trauma, mistreatment and abuse, unnecessary invasive procedures and surgical births, impaired newborn bonding, and avoidable morbidity and mortality.4–18 Recent work from nursing science has provided a definition of obstetric violence from a concept analysis that is used for this discussion: Obstetric violence is abuse or mistreatment by a healthcare provider of a female who is engaged in fertility treatment, preconception care, pregnant, birthing, or postpartum; or the performance of any invasive or surgical procedure during the full span of the childbearing time without informed consent, that is coerced, or in violation of refusal. It is a sex-specific form of violence against women that is a violation of human rights. (p. 661)
18
Background
The American Nurses Association (ANA) provides a clear reference for the ethical duties and conduct for nurses in “The Code,” 19 which can serve as a professional guide for social justice and support for the premise that ethical nursing care is incompatible with obstetric violence. The organization of hospital-based maternity care in the United States is unique from other inpatient specialties. Labor and delivery nurses exercise a great deal of autonomous clinical decision-making and act on a broad range of independent patient interventions within their nursing scope, yet there are arbitrary and inconsistent unit-based limitations that prevent labor and delivery nurses from working to the full extent of their role and curtail the impact of their nursing care.20–24 Labor and delivery nurses spend more time with women in labor than any other clinician, with the exception sometimes being private midwifery care, and they are an underrecognized leverage point for driving maternity care outcomes.
The professional delineation between midwives and nurses in the US encompasses distinct roles. The educational preparation of labor and delivery nurses is at the undergraduate level, and they develop their essential labor and delivery nurse training through their employment with only one required course on maternal/newborn care during the degree-granting curriculum. The common denominator for all hospital births in the United States is the care of the laboring, birthing, and postpartum patient by a labor and delivery nurse. Labor and delivery nurses in the United States attend nurse-assisted births only in cases of rapid delivery or if a midwife or physician is not available when birth is imminent. Labor and delivery nurses are an essential part of all hospital birth experiences within their role, while certified nurse midwives (CNMs) attended only 9.8% of total US births in 2019. 25 Midwifery is not a national standard of care in the United States and is further complicated by several different pathways for midwives that have varying levels of education and formal training.26,27
The combination of confronting obstetric violence in US hospitals along with a theoretical framework of social justice would affirm the principles of compassion, caring, and patients’ rights. This approach also affirms the ethical principles of equity, beneficence, and fidelity. The dual objectives of furthering research on obstetric violence with social justice as a guiding theory can also expand nursing knowledge and offer a new framework for examining the complexity of how obstetric violence is understood, enabled, and perpetuated. The contradiction between ethical nursing and obstetric violence is further demonstrated in the ANA statement that ethics, human rights, and nursing converge as a formidable instrument for social justice (emphasis added) that must be diligently protected and promoted. Nurses have a responsibility to address unjust systems and structures and to model the profession’s commitment to social justice. 19 The International Council of Nurses (ICN) Code of Ethics for Nurses states that the nurse contributes to an ethical organizational environment and challenges unethical practices. 28 The occurrence of obstetric violence is an ethical dilemma, and the ICN Code of Ethics for Nurses calls for nurses to work to resolve ethical dilemmas across the domains of practice, education, research, and management. 28
Significance
The gap in knowledge about obstetric violence is apparent from its absence in US healthcare research, yet the WHO, the United Nations, and the global research community are actively calling for its recognition, prevention, and elimination.3,4,29–31 The related phenomena of birth trauma, mistreatment, disrespect, and abuse in childbirth have been studied with little unifying connection established among them, while research on obstetric violence in US hospitals continues to be neglected outside of advocacy, feminist, and legal publications.6–11,32 The recognition of obstetric violence as a structural form of violence that is embedded in a complex, interrelated network of factors is important to recognize. One of the challenges to developing research on obstetric violence is that it exists beyond the level of the individual. See Figure 1 for a conceptual model derived from the existing literature and online resources that shows a summary of factors believed to enable and perpetuate obstetric violence in the United States.5–7,10,11,30,31,33,34 This model is a dynamic and evolving figure that is newly put forth to illustrate the broad view that obstetric violence cannot be understood in isolation. It is not scientifically proven and is meant to provide a collective visual representation of factors that have been identified in association with obstetric violence.
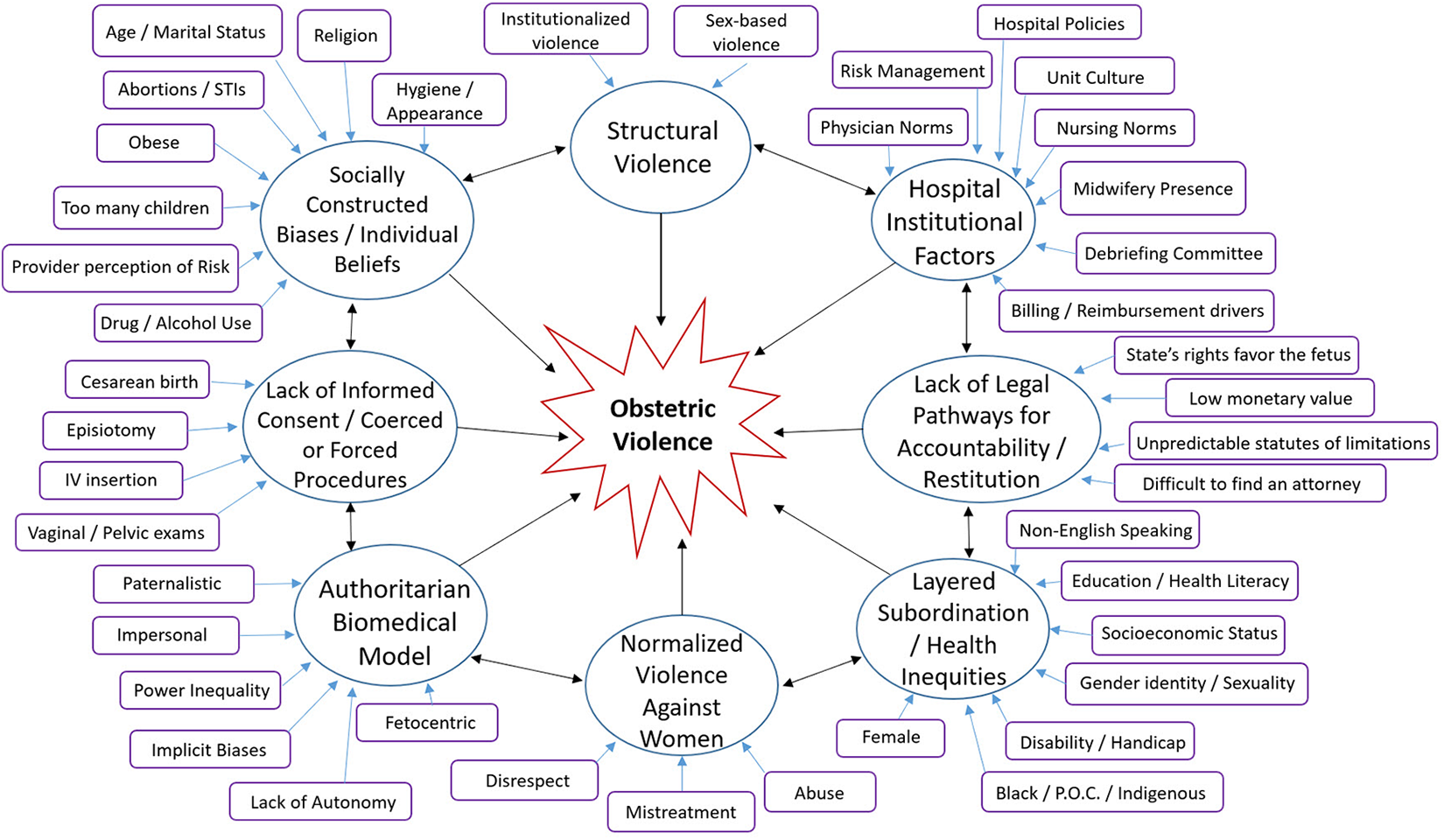
Conceptual model of factors associated with enabling and perpetuating obstetric violence.
Poor quality and outcome issues in maternity care that are resistant to sustained progress are embedded in systems that are riddled with undesirable behaviors characteristic of the structures that intersect
35
during hospital-based care. Leading problems in US maternity care that may be related in their persistence by having a common cause in the occurrence of obstetric violence include: Hospitals have primary cesarean rates for low-risk women as high as 51%, while others have rates as low as 7%.36–38 Significant variation in episiotomy use with a mean-adjusted hospital episiotomy rate of 34.1% among the top 10% of hospitals for frequency of use and 2.5% in the 10% of hospitals with the least frequent use.
39
Women and newborns suffer avoidable morbidity and mortality from unnecessary interventions and cesarean births.12,13 The United States is the only high-resource country with an increasing maternal mortality rate (MMR) along with inequities that include Black women dying from a MMR more than three times greater than White women.14–17 Uncontrolled and escalating cost burdens from the overuse of unnecessary interventions and cesarean surgeries.40,41 Overall, US women report the least positive healthcare experiences and the highest rates of foregoing needed healthcare because of cost compared to women in 10 other high-income countries.
42
The feminist perspective on obstetric violence demonstrates the entrenched challenges to recognizing and effectively responding to it. Restriction of movement, withholding food and drink, denying use of the toilet, repeated internal exams, unnecessary medical interventions, and other domineering practices that deprive women of bodily autonomy are common in hospitals. These practices are also considered part of routine care since labor and birth were moved into hospitals under the control of the biomedical model established by male physicians. The normalization of routine medical practices that are harmful to low-risk women are part of what is expected from a childbirth experience that conforms to embodied oppression, 10 and it is within this normalization that obstetric violence often occurs unrecognized and with no accountability. Multiple vulnerabilities and layered inequities that may be part of women’s existences intersect in the context of hospital-based maternity care where there are power imbalances between women and providers, hospital enforced policies, and being in the biomedical role of the submissive patient.8,17,30,31 This viewpoint helps obstetric violence to be seen in the broader culturally and institutionally enforced problem of structural violence against women. The routine depersonalization and unequal power dynamics in many hospital birth units create the belief that it is normal to have “women’s bodies exposed and displayed, their sexual organs uncovered and interventions that cut, penetrate, and hurt them” (p. 6). 11
Understanding obstetric violence in US hospitals through the use of a theoretical framework for social justice in nursing has the potential to offer a new paradigm for improving primary cesarean rates, overuse of unnecessary interventions, decreasing avoidable maternal morbidity and mortality, and addressing health inequities. The connection is that these problem areas in maternity care may be related by a common cause that has gone unrecognized in the presence of obstetric violence. The theory analysis in the subsequent sections demonstrates the soundness and usability of emancipatory nursing praxis as a midrange theory of social justice in nursing followed by arguments in favor of using it as a theoretical framework for the study of obstetric violence in US hospitals.
Theoretical explanation
Robin R Walter developed emancipatory nursing praxis as a middle-range nursing theory of social justice from an international study of the critical factors influencing nurses’ perceptions of their role in social justice using grounded theory methods. Phase I of the study included 27 registered nurses (RNs) from nine different countries who were English-speaking and self-identified as engaging in social justice. Phase II of the study included six RNs who were considered experts in social justice by being published as a lead author on the subject in a peer-reviewed nursing journal. These Phase II participants confirmed the conceptual and contextual categories of the theory through focus group consensus. Walter states that current nursing practice reinforces the dominant hegemony in healthcare by providing nursing care within the confines of the systems that contribute to inequities rather than offering nursing care that helps emancipate patients from their immediate milieu. 1
The lack of a theoretical framework to guide professional nurses in social justice inhibits them from fulfilling their ethical obligation and social contract with the public. Walter asserts that nursing awareness and engagement in social justice need to be developed so that oppressed and vulnerable populations do not remain interminably at risk. 1 This theory was chosen for analysis and is recommended for the study of the problem of obstetric violence where labor and delivery nurses are central to maternity care, because it is a midrange theory specific to nursing. The study by Walter proposes social justice as a theoretical vehicle to fulfill the ethical obligations that are codified in the profession, and a nursing workforce awakened to social justice engagement would be a powerful force against the factors that enable and perpetuate obstetric violence.
Evaluation of the theory of social justice in nursing by Walter
The relevance of this formal theory analysis is from the evaluation of the worth the theory has as a basis for guiding research on obstetric violence and informing actions needed to improve poor outcomes in US maternity care that have been resistant to sustained progress. The procedures for theory analysis were followed using the six steps detailed by Walker and Avant. These steps in analysis and evaluation include: (1) origins, (2) meaning, (3) logical adequacy, (4) usefulness, (5) generalizability or transferability and parsimony, and (6) testability. 2
Origins
The origin of the theory of emancipatory nursing praxis as a middle-range theory of social justice in nursing is rooted in critical theory referenced back to Marxism. The theory was derived from a systematic inductive approach conducted with Charmaz’s constructivist grounded theory methods. 43 Walter was motivated to develop the theory by her belief that critical theories are too abstract to guide social justice nursing research, and their concepts are too difficult to operationalize to be practical for empirical study. The objective for this theory to be “substantively specific and composed of a limited number of relatively concrete concepts that can be operationally defined and empirically tested” (pp. 226–227) has no evidence as of yet to support or refute it.
Meaning
Structure
This theory is appropriate to nursing and was developed with the purpose of being used to guide nursing education, research, and practice with a theory of social justice that is specific to the discipline. A definition for social justice is not stated in the study by Walter. An overview of what social justice represents as a concept in professional nursing codes and historical examples of nurses’ changing relationships with social justice are included as background, but the term does not reside in the work as fixed. The findings from the theory of social justice in nursing by Walter are described as a dynamic, transformative process, not a static definition. A concept analysis of social justice for contemporary nursing was conducted by Matwick and Woodgate.
44
It was published the year prior and is not referenced in the theory by Walter. The co-authors proposed an operational definition for social justice in the context of nursing that is consistent with the use of the concept in the paper by Walter: Social justice in nursing is a state of health equity characterized by both the equitable distribution of services affecting health and helping relationships. Social justice is achieved through the recognition and acknowledgment of social oppression and inequity and nurses’ caring actions toward social reform. (p. 182)
44
There is no ambiguity in the relational propositions of the core concepts. They are supported by their connection to existing nursing theory from the complexity sciences and have the shared tenets of simultaneity, being inseparable from the environment, all things are interconnected, self-organizing into patterns, and constantly evolving.1,45–48 The complexity sciences in nursing often defy a singular definition because of the recognized, continual fluctuations they have in open systems. The connection between Walter’s theory of social justice and emancipatory nursing praxis being congruent with complexity science theories in nursing provides a logical argument for extending the application to obstetric violence research. This is because both are known to be rooted in structural systems where outcomes are often the result of multilevel, nonlinear, and diverse factors that intersect over time in relational encounters between clinicians and patients.33,34,49
The semantics of the theory become confused in a couple of areas. The purpose of the study by Walter is stated as the goal of constructing a midrange theory of social justice specific to nursing, and a model for emancipatory nursing praxis is co-constructed. It is not always clear what the relationship is between the two principal purposes. The author sometimes switches between discussing emancipatory nursing praxis and nurse engagement in social justice as if they are interchangeable, but they are identified as distinct co-constructs. Walter makes the relational statement in the abstract that the four implementing processes for emancipatory nursing praxis (becoming, awakening, engaging, and transforming) and two conditional contexts (relational and reflexive) are what provide an understanding of the learning process that determine nurse engagement in social justice. This relationship does not always remain clear throughout the article. An explanation may be that it is not possible to isolate a singular concept at a defined point in the ever-evolving process, because the theory is nonlinear, dynamic, and its factors are interrelated.
Most of the findings are about emancipatory nursing praxis, but the research questions are about social justice. The primary research question was “What are the critical factors that influence nurse professionals’ perceptions, attitudes, and behaviors regarding their role in social justice?,” and the secondary questions were “How do nurse professionals come to know and engage in social justice? [and] How do nurse professionals determine the context in which they will engage in social justice?” (p. 227). 1 The research questions and the stated purpose of the study to construct a middle-range theory of social justice for nursing practice can make the co-construct of emancipatory nursing praxis distracting. It is clearly stated that the implementing processes for emancipatory nursing praxis are meant to provide an in-depth understanding of the process for nurses to engage in social justice. The linkages make sense when they are dissected and considered piece by piece. The study is not easily understandable when it is viewed as a whole. It may be that this is a quality of a theory that aligns itself with the nursing complexity sciences, and it requires a shift in thinking by the reader to remain open to simultaneous, transformative thought.
Part of the interpretive conclusions were vague and then later clarified. Walter refers to “Privilege” in the introduction and beginning of interpretive conclusions without stating what kind of privilege. This was later clarified as “White Privilege,” which could be assumed from focusing on the demographics of the Phase I RN sample with 23 White participants and 4 non-White participants. Yet I read most of the article thinking “Privilege” meant that professional nurses have the benefits of college education and are assumed not to be living in poverty.
Concepts
A theory of transformational learning for achieving emancipatory nursing praxis was composed of four dynamic and inter-relational core conceptual categories and two contextual categories. Becoming, awakening, engaging, and transforming are the core concepts for implementing emancipatory nursing praxis, and relational and reflexive efforts are the conditional contexts. These implementing processes and conditional contexts are what provide an understanding of the transformative learning process that determines nurse engagement in social justice. Definitions of the four conceptual categories are summarized in Table 1 (pp. 231, 233, 235). 1
Conceptual categories in transformative learning process that determine nurse engagement in social justice.
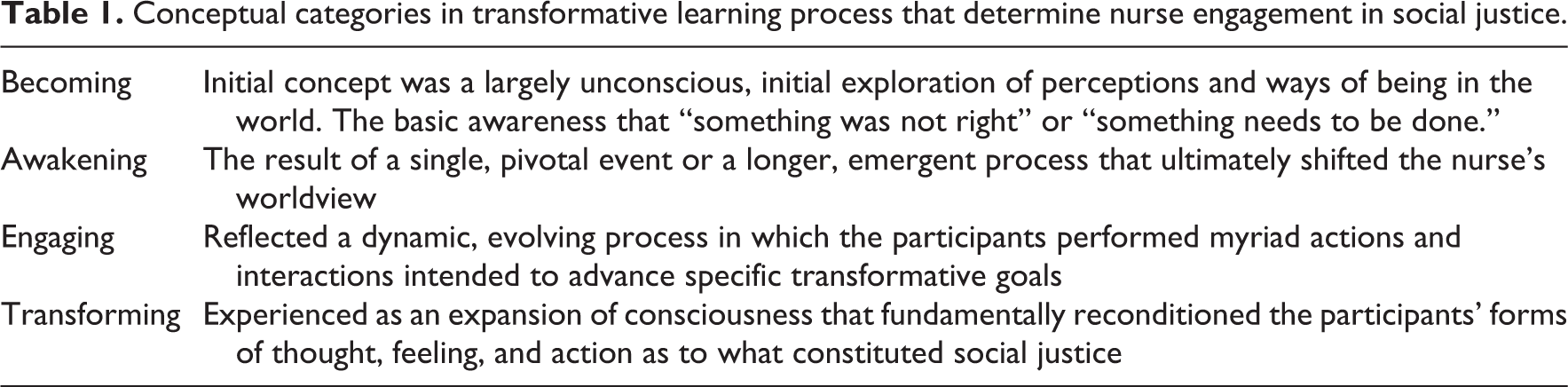
The core concept of engaging includes analyzing power, collective strategizing, praxis, and persisting as the four processes that characterize it. In addition, the core concept of transforming has human flourishing, achieving equity, and transforming social relationships as the three goal-directed processes identified by Walter. 1 The two contextual conditions that emerged influenced the basic social process of emancipatory nursing praxis. The relational context consisted of the range of relational realms, from the individual to global, in which nurses can engage in social justice. Reflexivity was the other necessary contextual condition for emancipatory nursing praxis, and it was found that participants’ reflexivity moved dynamically through the dimensions of descriptive, self-aware, critical, and emancipatory reflection. 1
Propositions
Key propositions that link emancipatory nursing praxis and social justice in nursing to other concepts include the perspective of pragmatism and the philosophical underpinnings from grounded theory. The phenomenon of emancipatory nursing praxis was linked to pragmatism to strengthen the intent for the findings to be usable. 1 The theory was also related to Marxism, Habermas, and Freire for their positions on critical social theory that address the social order itself along with the intent to emancipate people from structures of oppression. Walter made relational statements about Marxism as the foundation of all critical theory and used Marxism as a base to explore the study’s relevance to Habermas and Freire as additional critical philosophers and change agents. The theory of emancipatory nursing praxis is consistent with Habermas’ critical and emancipatory theory and is also consistent with Freire’s view of praxis as a transformative force for liberation. 1
Another key proposition related the middle-range theory to the nursing complexity sciences of Rogers’ Science of Unitary Human Beings, Newman’s Health as Expanding Consciousness, and Parse’s Human Becoming Theory. This is supported by emancipatory nursing praxis being a theory based on the human–environment as an integral whole, where praxis is the catalyst for emancipatory human–environment change. 1 The emancipatory nursing praxis theory is also considered as a dialectical model that is consistent with Gadow’s dialectical reasoning process, 50 because “the 4 conceptual categories and 2 conditional categories are not hierarchical, nor can one be of more value than another, and it is the overall process that represents completion and wholeness” (p. 239). 1
An additional step taken by Walter in the section on interpretive conclusions was to identify external validity for the theory of emancipatory nursing praxis by comparing it to the findings from Giddings’ study of nurses’ development of social consciousness within the context of professional nursing practice. 51 The agreement comes from the three dialectical positions in Giddings’ theory of social consciousness being identified as acquired, awakened, and expanded, which are consistent with the attributes of becoming, awakening, and engaging described by Walter. Transforming is the fourth implementing process for emancipatory nursing praxis constructed by Walter, and it is not mentioned in the discussion of similarities from Giddings’ study.
Logical adequacy
The content of the theory makes sense to the extent that logical adequacy can be addressed. This is a newer theory and performing literature searches in PubMed and CINAHL as of 29 August 2020 does not yield studies by other nursing scholars who have used the theory to make predictions or published discussions about agreement on its use for providing a system to make predictions. The logical fallacy may come from the primary research questions being about social justice, while most of the findings are about the co-construct of emancipatory nursing praxis. The stated reasons are clear for how this theory of social justice would be better suited for empirical study than critical theory, but no direct explanation for them follows. Walker and Avant explain that “determining the correctness of the conclusion is more difficult in an inductive theory,” and the analyst will “have to use the notion of the preponderance of evidence to determine the relative truth of the premises” (p. 218). 2 The assumption for truth in an inductive theory was met for this analysis.
Usefulness
The theory is useful because it provides new insights into emancipatory nursing praxis and social justice in a form intended for nursing practice. It can also be considered useful for explaining emancipatory nursing praxis and social justice differently along with the claim that the theory offers a better framework to guide nursing issues with the inclusion of social justice. 1 The points that Walker and Avant 2 consider when determining usefulness showed that this theory (1) has not yet generated any new research that could be found for this analysis, (2) is clinically relevant to a wide range of nursing problems that seek answers beyond the level of the individual, and (3) has the potential to influence nursing education, practice, research, and administration. Elements of the theory that are useful for application to the study of obstetric violence are the need to deconstruct factors that are abusive or oppressive in maternity care systems and to reconstruct them in harmony with the parts of systems that have been proven to support best outcomes for women and newborns.
Generalizability and parsimony
The theory of emancipatory nursing praxis and social justice in nursing has a wide focus and can be broadly applied. The boundaries are tied to human potential, beliefs, and actions, not to the limits of the theory itself. This can be seen in the open-endedness of the emancipatory nursing praxis model that illustrates the ongoing, evolutionary, and ever-growing interrelationships that can lead to full human expression and flourishing for all. 1 The generalizability of the theory is well accomplished, but the parsimony is not. The theory is not simple or brief in expression. The co-construction of the emancipatory nursing praxis and social justice elements may be what cause this theory to lack parsimony. The theory is complete, but it is not easily understood as a whole. The precision of the relational statements is lessened by the need to switch between thinking of emancipatory nursing praxis as implementing processes for what is supposed to provide the understanding of the transformation that leads to engagement in social justice, and the learning processes that are supposed to determine nurse engagement in social justice.
The theory can be summarized to understand nurse engagement in social justice as a transformational learning process that is realized in the exemplars of human flourishing, achieving equity, and transforming social relationships. 1 A significant aspect of reflexivity in emancipatory nursing praxis is recognizing one’s own privilege and internalized dominance along with the ability to dismantle these obstacles to authenticity so that members of oppressed groups can be the ones to determine what constitutes a social justice ally. 1 The achievement of social justice in nursing, as a continual process of relating to others and acting together, is also synchronous with women-led care. This is significant for supporting the diversity of the full range of women’s unique needs and expectations for a positive birth experience.
Testability
The theory is testable in principle. The potential exists for the theory to generate hypotheses about nursing questions from all areas of the profession. The few points where it has been stated that the theory is lacking are not meant to discourage from further development and use. On the contrary, it was disappointing not to find examples of the theory used in other research or analyses that discuss its strengths or recommendations for modifications. Walter proposed that this theory was composed of relatively concrete concepts that can be empirically tested. 1 It is expected that knowledge needs to be developed around testability, because the theory is new.
Application of the theory to advance the science of obstetric violence
Obstetric violence is a complex phenomenon that is not well understood. The goal of understanding what enables and perpetuates obstetric violence in US hospitals using the theory of social justice in nursing as a framework to guide the research is well matched. The alignment comes from obstetric violence causing avoidable harms to women that are a violation of human rights, while social justice in nursing recognizes the professional duty to call out and correct injustices. Obstetric violence includes the performance of any invasive or surgical procedure during the full span of the childbearing continuum without informed consent, that is coerced, or in violation of refusal. 18 Cesarean births that lack informed consent, are coerced, or are forced are part of the concern with overuse of the surgery. Attorneys who represent women seeking redress for harm from these types of cases argue that these instances of cesarean birth constitute obstetric violence.7–9 It is important to advance the understanding of why violations that occur around the vulnerable time surrounding childbirth are a social justice issue. This includes the need to employ a wide-angle view for the study of how avoidable harms to women and newborns persist in a high-resource nation like the United States where those problems cannot be attributed to lack of resources.
The connections for applying the theory of social justice in nursing to obstetric violence in US hospitals involve recognizing nursing as a marginalized profession within hospitals that are dominated by a medical model. 52 In addition to the hospital milieu that favors physicians, labor and delivery nurses are almost exclusively women. Childbirth is a female function, and different layers of oppression and marginalization add to risk and inequities in pregnancy and birth outcomes. For example, maternal mortality persists as a compounded inequity for Black women in the United States who die at disproportionately higher rates than White women even when professional-level education and middle-class or above socioeconomic status have been attained.16,17 Furthermore, Vedam and colleagues found that women of color reported consistently higher rates of mistreatment during pregnancy and childbirth and having a Black partner increased reported mistreatment regardless of maternal race. 5
Elements of obstetric violence and the related concept of obstetric racism provide examples of the structural injustices that contribute to health inequities and poor outcomes in maternity care. Obstetric racism involves the recognition that Black women suffer an additional layer of harm from “racism as the institutionally and state sanctioned practices that make particularly designated groups of people vulnerable to harm and premature death” (p. 561). 17 The ways in which power and privilege intersect during the time surrounding childbirth demonstrate how using this theory of social justice is well suited as a framework for the study of obstetric violence. The actualization of social justice as a nursing principle, when applied in practice to expand the role of the nurse from advocate to ally, 1 may be discovered as an area that can influence sustained positive change. “The emancipatory nursing praxis prompts nurses to engage as social justice allies in a manner that is deliberate, reflexive, and always in concert with those whom we have aligned ourselves” (p. 242). 1
There is something missing in US maternity care that allows health disparities and inequitable outcomes to expand and persist despite efforts and resources directed at meeting recommended targets for quality outcomes. There are examples of countries with interdisciplinary systems where a midwifery model is the normal organization for women’s health and childbirth care. Integrated care with role respect and collegiality among nurses, midwives, and physicians is recognized as the standard for best outcomes for women and newborns, and staff retention with job satisfaction. This is not the norm in the United States where there is no universal health system, and there are significant differences in policies, regulations, and normative practice behaviors at local, state, and regional levels. The United States is geographically vast and includes significant variations in the different types of midwifery care that are accessible and legal in different states. This includes several states where midwife-attended home birth is illegal. Women and families sometimes travel across state lines to birth how they choose with whom they prefer. Normalized access to midwives remains suppressed by dominant, competing physician interests and restrictions by insurance groups for payment coverage.
The fact that each state determines its own regulations and scope of practice for different types of midwives has led the Midwives Association of North America (MANA) to maintain a state-by-state resource guide. 53 The lack of access to women-led choices about where and with whom birth can occur is a significant part of the problem with recognizing obstetric violence in the United States where the entrenched, biomedical hospital context is the norm. The total percentage of out-of-hospital births for the United States in 2017 was 1.61% with over 10 states reporting less than 1%, and the greatest percentage of 7.88% was reported in Alaska. 54 These totals represent birth center and home birth settings and do not distinguish between home births that were not planned. There are alternatives to mainstream hospital maternity care in the US, but a woman must be informed, capable of self-advocacy, and have geographic and financial access to successfully navigate to midwifery care and preferred place of birth.
Discussion
There is an ethical and scientific duty to fill the gap in knowledge on obstetric violence. Walter was clear about the origins of her theory being connected to seminal critical theorists. The application of critical theory in nursing scholarship is meant to expose and challenge relations of domination that exist in the profession of nursing itself and within the institutionalized power structures where nurses provide care. 55 The full circle view of obstetric violence in US hospitals overlaps with findings from postmodern critical theorists whose body of work helps explain how obstetric violence is at its essence directed at women because they are women.10,11 Harden’s goal of emancipatory nursing is a reminder that true humanistic care cannot be given until the dual oppression of being nurses and women has been transcended along with the achievement of critical consciousness. 56 This ambition is linked to the operational potential of the theory of social justice in nursing in that engagement as an ally requires intentional participation in a transformative learning process. The holistic, relational perspective that social justice engagement opens up would result in better recognition of individual and systemic factors that enable and perpetuate obstetric violence through actions and lack of action.
Bent made a significant step in combining perspectives on critical and feminist theory, which offers a better understanding of how the domination of the medical model toward patients also affects nurses. Nurses and patients, in particular when women, remain marginalized as long as they continue to internalize the myth of the superiority of “the empirical positivist values of medicine and the traditional male paternalistic health care structure” (p. 297). 57 Chinn suggested that feminism offers more to nursing than pure critical theory, because feminism includes the recognition of a lack of freedom or power at the individual level, rather than being limited to an analysis of the mechanisms of oppression at the societal level. 58 A feminist model of caring combined with the true nature of nursing offers holism, equality, power sharing, and respect for others, which is incompatible with the occurrence of obstetric violence.
Conclusion
An obvious limitation of the conceptual model presented for factors associated with enabling and perpetuating obstetric violence is that the relationships, directionality, and strength of associations have not been tested. In addition, a weakness in rigor and reproducibility for further theory construction on obstetric violence comes from the scarcity of research from the US healthcare sector and minimal scientific studies worldwide. Most published resources on obstetric violence do not employ scientific methods, or they are from the gray literature and online. Another limitation for this article is that only resources written in English could be considered because of no support for translation services.
Moving the science forward on obstetric violence with a unified theoretical framework may be able to offer a new construct to leverage change in key areas where maternity care fails to meet standards of care, cost containment, and reductions in avoidable harms to women and their newborns. Obstetric violence can be better identified as it is better understood. As this is achieved, obstetric violence cannot remain embedded as a normalized part of maternity care where it continues unnamed without established pathways for effective interventions or accountability.
The application of the midrange theory of social justice in nursing by Walter can also be advanced by demonstrating its usability as a theoretical framework. The theory of social justice in nursing originates in critical theory and is well-suited for application to the study of the multidimensional intersection of layered vulnerabilities that converge during the childbearing continuum. Advancing the science on obstetric violence from a nursing perspective that incorporates social justice theory provides an opportunity for nurses to take a leadership role in creating and disseminating knowledge about an understudied area in maternity care. This also promotes social justice in the profession so that the identification and understanding of obstetric violence can be improved along with nurse engagement in the transformative potential to recognize and minimize oppressive structural and institutional power imbalances worldwide. The macro-level goal is to change the view of obstetric violence to one of zero-tolerance with its universal recognition as a sex-based, gendered form of violence against women that is a human rights violation. When this happens obstetric violence will have standardized means for identification, risks and harms will be mitigated, and factors that enable and perpetuate obstetric violence will be corrected so that it can no longer continue.
Footnotes
Acknowledgements
I would like to thank my Health Care Systems Seminar professor, Dr Mary Beth Flynn Makic, PhD, RN, CCNS, FAAN, FCNS, FNAP, for reviewing the early form of this article and her encouragement to continue building a body of research on a complex, systemic problem in US maternity care.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.