
Abstract
Background
Midwives frequently encounter ethical dilemmas in a critical unit such as a delivery room. Determining these ethical dilemmas is very important to prevent ethical problems and develop an ethical approach.
Aim
This study aims to identify the ethical dilemma experiences of midwives working in delivery rooms in Turkey.
Research design
This study follows a qualitative phenomenological research design.
Participants and research context
The sample comprised 13 midwives with at least two years working experience in delivery rooms, having completed the midwifery program of Manisa Celal Bayar University Health Sciences Institute in the 2017–2018 academic year. Data were collected through audio-recorded semi-structured interviews to reveal their experiences. Content analysis was done using the Nvivo software package program. All interviews were digitally recorded, transcribed verbatim, and transferred into NVivo for analysis.
Ethical considerations
Ethical approval was granted by Manisa Celal Bayar University University Health Sciences Ethics Committee (Date: 16.12.2016 No: 372). Participation in this study was voluntary. Written and verbal consent was gained. These consents include protecting midwives’ privacy, keeping information confidential, and/or allowing the participant to remain anonymous.
Findings
Four themes were identified: differences of approach to the birth process, hospital management, communication, and differences in ethical approach. Several factors explained these ethical dilemmas while the midwives adopted different approaches to ethical decision making.
Discussion
These midwives experienced various dilemmas while working in the delivery room and are aware of most of them. They also took responsibility in the decision-making process and experienced many intense emotions that they had to cope with.
Conclusion
The ethical dilemmas faced by these midwives while working in delivery rooms were mainly caused by hierarchy. Future studies could investigate clarifying job descriptions of midwives, who are authorized to manage normal births under their own responsibility, within the hospital management and the health care team.
Introduction
Midwifery is a particularly dynamic profession within health science that involves the care of women, newborns, and the family. Due to their dynamic role in accordance with the job description, midwives must take actions that affect the woman herself and her newborn, colleagues, institution policies, and administrators. 1 Faced with an ethical dilemma, midwives may consider several solutions depending on their personal beliefs, experiences, and value judgments. Nevertheless, they are expected to select the best option and act consistently with that decision.2,3 The interaction of ethics with midwifery must be questioned and appropriate answers must be found. Otherwise, the occupation will be unable to fully develop professionally and the coping process for midwives will be blocked. 3 Ethical and social factors affecting the health of newborns and pregnant women are becoming increasingly complex, particularly due to developments in reproductive technology, maternity care, and newborn care. 4 Midwives provide an active care role in the labor process and childbirth in Turkey, but they are not in an influential position as a decision-maker. 5 It is stated that midwives have a lack of autonomy, and the legal arrangements about it are insufficient in Turkey.5,6 These may increase the risk of midwives facing ethical dilemmas.
Background
Ethical dilemmas are conditions when one cannot choose one clearly right decision, which creates discordance and difficulty while selecting among the alternatives.2,7 A crucial step towards making the correct decisions to resolve ethical dilemmas is to clearly describe the issue. While ethical decision making is inherently complex, the preliminary requirement to proceed is accepting that the situation has an ethical side. To recognize this, it is essential to have ethical sensitivity.8–13 Ethical sensitivity is defined as the ability to recognize value-related issues when they arise in practice. 14 It is stated that midwives who experience ethical dilemmas have high ethical sensitivity. 15 Ethical decision making is affected by several factors, particularly institutional and social structure, universal and professional ethics, national and institutional legal regulations, proficiency, knowledge, critical thinking skills, personal skills, complexity and quality of the assigned operation and decision environment.8–13
The concept of moral distress in midwifery practice is described as “a psychological suffering following clinical situations of moral uncertainty and/or constraint, which result in an experience of personal powerlessness where the midwife perceives an inability to preserve all competing moral commitments”. 16 Midwives experience moral distress when they cannot manage the decision-making process well in case of an ethical dilemma, which can frequently occur when working in a critical unit such as a delivery room. 17 This moral distress may have a variety of personal or institutional causes that impact midwives’ lives socially and psychologically. This in turn may reduce their career motivation, job satisfaction, and self-respect, which can impair their professional performance. 18 Ultimately, by impairing the profession of caring, this chain of adverse effects from ethical issues through ethical dilemmas to moral distress concerns the whole health system. 19
It is important to know what ethical dilemmas are experienced by midwives working in the delivery room so that they can provide better quality care. This research is the first to explore the ethical dilemmas of midwives working in the delivery room in Turkey. The objective of this study is to describe the ethical dilemma experiences of midwives working in delivery rooms in Turkey.
Methodology
Design
This study follows a qualitative design based on the descriptive phenomenological approach to describe the ethical dilemma experiences of midwives working in delivery rooms. The descriptive phenomenological approach is to describe lived experience. Understanding lived experiences exposes the intentionality of consciousness, or how meaning. 20 In this approach, the primary data collection method is interviewing. This enables investigators to create an appropriate interactive environment whereby interviewees can comfortably express themselves to reveal their experiences and the meanings that they attribute to them. 21 The semi-structured interview form provides a guide for the interviewer, consisting of questions that orient them during the interview. In this particular study, an in-depth interviewing method was applied with open-ended questions to reveal midwives’ exposure to ethical dilemmas, their experiences, and decision-making processes.
Setting
The participants in this research represent the people who were eligible for the focus of the investigation to conduct a phenomenological approach. 21 The universe of the study comprised thesis and non-thesis master’s degree students (N = 19) and PhD students (N = 6) studying at Manisa Celal Bayar University, Institute of Health Sciences during the 2016–2017 Spring Semester. All students graduated from midwifery bachelor, and they were continuing their postgraduate education. Purposive sampling, specifically criterion sampling, was used for this qualitative study. The inclusion criteria included having at least two years’ post-graduation delivery room experience, voluntariness, and informed consent. These criteria yielded 15 potential participants. However, because one was unwilling to be interviewed while another was unwilling to allow audio recording, the final sample comprised 13 participants. These participants were working as midwives in an institution.
Data collection tools
In-depth interviews were conducted with the midwives using the semi-structured interview guideline. Before the interview, their background information was obtained, including their age, education status, desire to proceed with the profession, career satisfaction level, area of work and years of experience, delivery room experience, and ethics training status.
The semi-structured interview guideline described the midwives’ experiences of social dilemmas in the delivery room. The interview guideline was prepared based on qualitative and quantitative studies in the national and international literature.2,4,7,8,18,22,23 This guideline had seven questions addressing the factors determining the midwives’ experience of social dilemmas in delivery rooms, the causes of these ethical dilemmas, the decision-making process while dealing with ethical dilemmas, and the effects of experiencing these ethical dilemmas. In addition, while discussing the participants’ most remarkable ethical dilemma experiences and related decision-making processes, they were asked for suggestions to manage ethical dilemmas and improve decision-making processes. All the questions were open-ended, while some had sub-questions (time of the ethical dilemma experience, what it feels like, current feelings) to increase the intelligibility of answers.
The applicability of the questions was tested by conducting pre-interviews with two midwives with delivery room experience. The semi-structured interview guideline was modified to their final shape based on their feedback.
Data collection method
All data were collected by the first researcher (HT). HT has been a midwife for four years and has two years of delivery room experience. Appointment dates were scheduled for the 13 eligible participants. The interviews were conducted outside work hours and the workplace of midwives. The midwifery training room of the faculty was a place where midwives could feel safe and comfortable. Midwives were familiar with the midwifery training room as they used during where their postgraduate education. The 13 interviews took place in the midwifery training room as a safe space free of interruptions and where the participants would feel comfortable revealing information. Scientific working conditions were ensured, and a reassuring private environment was constructed.
Prior to each interview, the participants were given information to reassure them and create a more comfortable interview environment. Specifically, they were notified that their names would not be revealed for any reason, they could end the interview, pause the audio-recording at any time, or leave the room if they wished, read and sign the informed consent form, and that the interviewer could explain in detail any parts that were unclear.
The midwives were asked to fill in a socio-demographic questionnaire. The audio recording started, and verbal consent was taken from each midwife to proceed with the interview. The interviewer asked the seven open-ended questions and sub-questions to obtain in-depth interview data. In the end, each participant was thanked for their contribution and notified that they would receive an audio-recording copy or interview transcript. Guided by the semi-structured interview form, the interviews lasted 32 min on average (max: 47 min, min: 14 min).
Data analysis
Content analysis, which is a common data analysis method in qualitative research, was used to interpret the data. In qualitative research, inductive analysis, that is, content analysis based on coding, should be applied if the phenomenon under investigation cannot be related to any theory. The revealed codes (concepts) and relations between them (themes) are critical to clarifying the phenomena accounting for the data. 21 In this study, data processing and content analysis were conducted using NVivo software in several steps.
First, the audio recordings were transferred to computers and transcribed using Microsoft Office by the first researcher (HT). The accuracy of the transcriptions was ensured by repeatedly listening to the audio recordings and re-reading the transcribed data.
Second, the transcribed data were organized according to the interview questions and a list of related codes was generated. More specifically, using the analysis criteria, the data were coded, the main themes were generated, and the data relating to each theme were re-analyzed. The interview transcripts were analyzed independently and then coded to identify themes by two researchers. The fact that the first researcher had 2 years of experience and the second researcher had 15 years of working experience in the delivery room contributed to the analysis and coding of the birth experiences of the midwives.
Third, the researchers checked each coding for accuracy. Each investigator identified the main themes and sub-codes through separate analyses. Similar codes were grouped, re-grouped, and refined to generate themes that were meaningful units on ethical dilemmas experiences of midwives working in the delivery.
Fourth, the researchers discussed the analyzed data in relation to similar previous studies to generate a research report explaining the data. The researchers used detailed descriptions. This describes the data while conserving its nature by not adding further annotations. A detailed description of the data also allows readers to discuss the findings and reach their own conclusions. 21 The study held that the lived ethical dilemma experiences of midwives were reported during interviews conducted in a non-threatening environment and faithfully represented their world. The fact that the first researcher was a graduate student like midwives provided a safe interview environment.
Ethical considerations
Ethical approval of the research was taken from Manisa Celal Bayar University Health Sciences Ethics Committee (Date: 16.12.2016 No: 372). Accordingly, necessary permissions were granted by Manisa Celal Bayar University Institute of Health Sciences, Board of Directors, where postgraduate students are enrolled. After the permissions were obtained, the midwives were informed about the research and participants’ anonymity and confidentiality. It was expressed that they can withdraw from the research at any time. Thirteen midwives who met the research criteria expressed volunteered and willingness to participate in the study. During this first contact, the midwives’ collaboration was requested, and the time for the interview was scheduled. All participants were asked for their written and verbal consent to ensure that participation was voluntary during the interview. These consents include protecting midwives’ privacy, keeping information confidential, and allowing the participant to remain anonymous. Assurance was given to each midwife that the information on the audio recordings would not be shared with anyone other than the research supervisor and the researcher. The names of midwives and their healthcare institutions were not identified to avoid linking quotes to participants their participation.
Findings
Socio-demographic characteristics of the midwives.

Themes and categories extracted from content analysis.
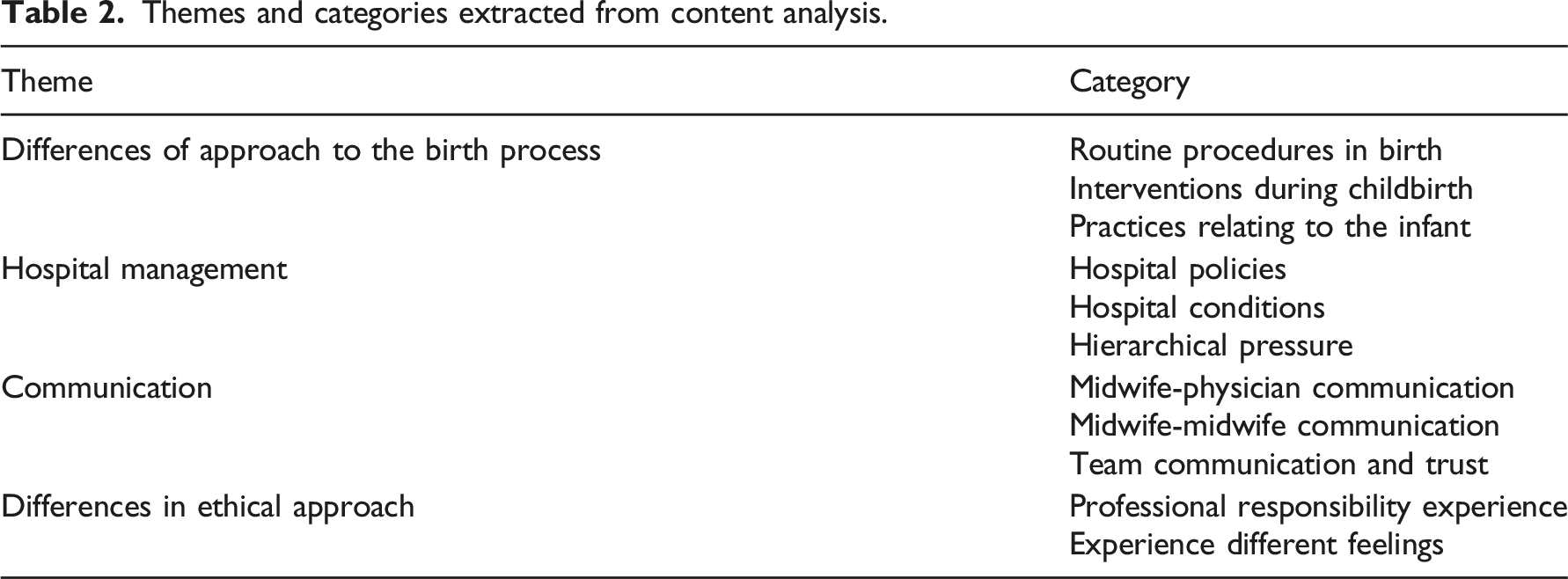
Differences of approach to the birth process
According to the midwives, ethical dilemmas arose most frequently from differences in the approach to the birth process. These particularly concerned routine procedures in birth, interventions during childbirth, and different practices relating to the infant at birth. Regarding routine procedures, the most frequently mentioned ethical dilemmas were the use of induction, confining the mother to the bed to enable continuous fetal monitoring, and ignoring new evidence-based practices in favor of routine practices. These are considered in more detail below, using the participants' own words, starting with induction: There are some things which we can’t stop. We start induction with a mother whose contractions are regular and adequate, and who should not be started on induction. We are obliged to because there’s a doctor’s order, but it’s something that in conscience I’m not happy about it. (Midwife 12) I’m not happy that the mothers who I monitor stay attached to the bed. If conditions are suitable, I would very much like to allow the woman to walk around the room and sit or squat while straining, but some of our doctors insist that the mother must stay in bed. In such circumstances, I face an ethical dilemma. I know what I should do, I know that it will make the mother more comfortable and speed up the birth, and I want to do it. (Midwife 3) When I attend at a birth, the doctor says to immediately cut the umbilical cord, take the baby, and aspirate. What I want to do is lay the baby on the mother’s breast and establish body-to-body contact. There’s no emergency situation, the infant is fine, there’s no need to aspirate its mouth or nose – it’s enough for me to take the secretions out of its mouth. But they insist on taking the baby away from the mother and aspirating. (Midwife 3)
Regarding unnecessary interventions being performed during the birth process, the midwives said that they faced ethical dilemmas when making decisions on cesareans or applying fundal pressure, knowing this was not an appropriate approach but not having the authority to make a different decision. The midwives expressed that in the following excerpts: Of course, this has nothing to do with us midwives, but directing a woman who can have a normal birth to a cesarean leaves me in a dilemma. (Midwife 1) The doctor suddenly starts fundal pressure when the mother is pushing perfectly well. ‘There’s no need!’ I say, ‘The baby’s coming along; the mother can push it out herself.’ But it is like that, a completely unnecessary intervention. (Midwife 5) Regarding intervention decisions concerning early preterm babies, the midwives faced a dilemma regarding whether it was necessary to try to revive every preterm infant. A baby was born at 20–24 weeks of pregnancy, and its chances of survival were very low. But when it was born, it was alive. I think it was 20 weeks. It was below 200 g, but when it was born, it was breathing, and its muscle tone was good. The doctor came, and no intervention was made for the baby. (Midwife 10)
Hospital management
The second main theme, hospital management, was divided into three sub-themes: hospital policies, hospital conditions, and hierarchical pressure. The hospital management policies depended on the expectations of doctors and patients because of legal procedures, which created ethical dilemmas. The midwives also faced an ethical dilemma between carrying out routine treatment and midwife care because of the excessive load placed on them by the hospital management. Midwife 6 said: If somebody in the administration saw, all hell would be let loose. Birth should take place on a gynecological table, not in a bed. It was a rule of the hospital. But sometimes women didn’t want to give birth on a gynecological table. “I’m not going up there,” they would say, and at times like that, I was left in a dilemma.
Regarding hospital conditions, the midwives could not maintain the privacy of women while giving birth as more than one birth took place simultaneously in the same room. Two midwives expressed that in the following excerpts: The location of the delivery ward was not at all suitable. Anyone could go in from the corridor, and I couldn’t maintain the mothers’ privacy. This greatly upset me. (Midwife 12) The buildings and the delivery room were inadequate. For example, there were times when we were delivering two babies in the same room at the same time. (Midwife 3)
The midwives also could not carry out appropriate interventions on preterm babies because there were no neonatal intensive care services or incubators, and too few midwives. Midwife 4 said: We had a 23-week mother give birth, and the baby was alive. But there was no neonatal incubator, and we didn’t know what would happen until it was transferred elsewhere. We couldn’t do anything. We just waited for it to die.
Regarding hierarchical pressure in the hospital administration, the midwives said that they lacked authority to make crucial decisions relating to births and faced ethical dilemmas because of hierarchical pressure from doctors and hospital management. Some midwives who had experienced an ethical dilemma because of hierarchical pressure had made their decision to avoid attracting conflict to themselves. Midwife 4 said: I don’t want to perform a lot of vaginal examinations on the women I’m monitoring. But when the doctor wants a vaginal examination every time he comes, I’m in a dilemma. If I say there’s no need for so many examinations, there’ll be an argument, and if we perform an examination without saying anything, I feel guilty.
Communication
The midwives had faced ethical dilemmas arising from communication with their own colleagues and doctors. They said that when making decisions on topics regarding the mother and her relatives, they were careful not to upset communication with the team. However, this created ethical dilemmas. Midwife 13 expressed that: I had doctor and midwife friends who weren’t on speaking terms. When they were on duty, this doctor and midwife wouldn’t speak to each other, so when this was a problem for the patients, I had to communicate between them. The two people weren’t speaking, and there were patients, interventions needed to be made. I had to do everything. I had to mediate between the doctor and my midwife friend.
One factor affecting the midwives’ experience of ethical dilemmas was communication within the group. In particular, when there was an ethical dilemma, they made better decisions and faced fewer ethical dilemmas when they were in an environment where they felt secure. The midwives expressed that in the following excerpts: When I’m in a dilemma, I share it with my friends on the team. I ask them what they think. Having them think the same as me makes my decision-making easier. (Midwife 4) When there was a doctor, I felt more secure. However sure I was about what I was doing, having a doctor on the shift supporting my decisions made me feel more secure. (Midwife 7)
Differences in the ethical approach
The existence of differences in ethical approach caused ethical dilemmas, particularly due to differences between midwives, influenced by their differing professional experience. While making decisions, midwives experienced different feelings. Some stated that they openly took professional responsibility and implemented decisions to benefit the patient, whereas others said that they wanted to avoid taking professional responsibility because they could not know beforehand the results of their decisions. At a normal birth, I often say to the doctor, ‘Go to your room and rest, and if there’s a problem, I’ll call you,’ so that the mother can comfortably walk around the room and not stay confined to the bed. (Midwife 3) There are situations when I have to make decisions on my own. Taking responsibility on my own is difficult, and I’m afraid. (Midwife 7)
Midwives with more professional experience reported fewer ethical dilemmas and made better decisions when faced with a dilemma. They also emphasized that the hospital administration and doctors supported the decisions of experienced midwives. Experienced midwives make better decisions when faced with a dilemma, and generally, doctors give more support to the decisions of experienced midwives. (Midwife 5)
Regarding feelings, the midwives mostly experienced sadness, helplessness, and reduced motivation when they faced a dilemma. These feelings then affected the decision-making process. Look, I still get emotional when I talk about it. It was very bad—it was my first experience. It was the first time I had experienced anything like that (preterm infant death), and I was very affected, I felt very bad … I cried a lot in the next few days, and I felt very unhappy. (Midwife 4) When I’m in an ethical dilemma or when I can’t make an ethical decision, my motivation is less. I think that concerning myself with the mother, upsetting her, and the training I’ve given are all for nothing. (Midwife 5)
Discussion
The 13 participants had worked for at least two years in the delivery rooms of various government hospitals. They mainly were master’s degree students who were also working as midwives. Their experiences of ethical dilemmas were examined under four themes: differences of approach to the birth process, hospital management, communication, and differences in ethical approach.
The midwives stated that while working in the delivery room, they lacked authority to make decisions on unnecessary obstetric practices or interventions in the birth process. 11 Midwives who are upset by the medicalization of birth regularly experience emotional stress and conflict within the team. Their ethical decision-making behaviors are particularly affected by hospital regulations and hierarchical pressure.12,24,25 In this study, the midwives face ethical dilemmas when doctors insist on continuing routine practices in the birth process that are not evidence-based, and unnecessary obstetric interventions. The midwives believe that certain routine practices are wrong and want to manage a normal birth according to their own decisions. However, they are obliged to comply with the doctor’s orders regarding interventions in the birth process, and avoid conflict because of hierarchical pressure. Previous studies17,24,26 have also found that, faced with ethical dilemmas, midwives take decisions to avoid conflict with the hospital administration or the doctor. It was stated in the feminist approach studies that obstetricians have a powerful position at the lead of maternity care hierarchy. Both midwives and women who give birth have insufficient autonomy at birth.27,28 Although midwives are supposedly responsible for managing normal births, the primary responsibility for the procedure lies with the doctor, which restricts what the midwife can do. Midwives who favor a non-interventional birth approach frequently face ethical dilemmas because of limitations in their autonomy, authority, and responsibilities, which impairs the decision-making process.
The birth of an early preterm infant can lead to complex medical, social, psychological, and ethical challenges to the family and healthcare professionals.29–31 In early preterm births, the midwives experience ethical dilemmas regarding reviving the infant. 29 In this study, the midwives faced a particularly emotionally distressing ethical dilemma when doctors refuse to intervene to the extremely infant, hospital conditions are inadequate, neonatal intensive care or incubators are lacking. Midwives who faced ethical dilemmas because of the approach taken to an early preterm infant have still not forgotten the incident at the time of the interview, and remain upset whenever they think about it.
One of the essential ethical values is being respectful of privacy and trust.7,32 The inability to protect the privacy of women as an ethical principle due to hospital conditions has caused an ethical dilemma for midwives. Inadequate conditions also prevent midwives from preserving mothers’ privacy in the delivery room because several women have to give birth at the same time. These conditions cause strong feelings of helplessness and sadness. Recently, however, hospital conditions and technological developments have improved, which has made these ethical dilemmas less frequent.
Childbirth care requires good clinical evaluation and strong decision-making skills. 11 When midwives face ethical dilemmas at birth, they can solve problems by using their ethical decision-making skills. Ethical decision-making is affected by various factors, such as health professionals’ specializations and experience, the knowledge resources they use when making a decision, their personal characteristics, their cooperation with the obstetrician, and the birth location. 8 To avoid conflict, midwives may prefer to accept a sub-optimal situation even if they are right. One reason is that midwives believe it is essential to maintain positive communication with team members where there is conflict as good quality obstetric care depends on communication between team members. 11 This study found that midwives who had ethical dilemmas avoided conflict with their team members and faced difficulties in making moral decisions. Trusting the team and good communication helps the midwives to make decisions more easily. When midwives work in an environment where communication is good, and they feel secure, they find it easier to overcome ethical dilemmas. In these environments, intra-group sharing is easier, enabling a better quality of midwife care. However, if the midwives recognize a suitable ethical approach but lack the authority to implement it, they experience moral difficulties, which are sometimes traumatic for them. 17 In this study, it was found that midwives try to maintain team communication when they experience ethical dilemmas. The protection of team communication by midwives made it difficult for them to make ethical decisions. Hierarchical pressure or lack of midwives’ self-confidence could have affected their ethical decision-making process.
After a traumatic birth, the midwives feel deep sadness and blame themselves. These negative experiences affect every aspect of their personal and professional lives.18,33 Midwives experience many different emotions while making decisions in different situations in the delivery room. Studies have shown that they feel guilty even if they are not at fault in situations that may lead to serious and permanent harm to the baby or the mother.12,18 Many of the midwives in our study experience sadness and helplessness. In particular, being unable to intervene in an early preterm baby, especially it then dies, is an unforgettable negative experience. Furthermore, the limited professional authority of midwives and the inability to make their own decisions because of hospital management or hierarchical pressure may cause them to avoid taking professional responsibility and accept decisions that they think were wrong. Midwives need to work in an environment with ethical principles to present ethical care at birth.
Midwives may face ethical dilemmas due to differences in ethical approach among their colleagues. Avoiding professional responsibility, not wanting to take risks and the thought of acting according to hospital protocols also cause differences in ethical approach. 34 Making ethical decisions that prioritize the patient’s wellbeing may cause conflict with other midwives, doctors, or hospital management.12,35 In this study, when making ethical decisions, professional experience is very important for these midwives. Those with greater professional experience face fewer ethical dilemmas and make better decisions when faced with a dilemma, which are then accepted and supported by the hospital authorities. Conversely, midwives with only two years of experience are afraid when they take on professional responsibility, and unsure of themselves when making decisions when faced with a dilemma. The more experienced midwives feel sure of themselves when making decisions, and willing to take on any responsibility to protect mother and baby. Undoubtedly, the skill of making ethical decisions increases with a midwife’s professional experience as they face more ethical dilemmas and the associated decision making. At the same time, during ethical dilemmas, all health workers should also pay attention to the decisions of midwives who are aware of ethical principles despite being new to the profession. This is an ethical response that can be expected of all health workers. It is also important for the team to support decision-making by midwives who are new to the profession or have little professional experience. This represents correct management and enables midwives to gain positive experience.
Conclusion
The findings show that the ethical dilemmas experienced by midwives working in the delivery room in Turkey reflect differences in the approach to labor, hospital management, communication, and differences in individual ethical approaches. Midwives’ ethical decision making is greatly affected by the hierarchical structure in their working environment. The midwives cannot fully express themselves in situations that create ethical dilemmas due to their limited power and fear of conflict within the team. Consequently, they experience sadness and helplessness in these situations. In contrast, if the working environment allows good communication within the team and there are experienced midwife colleagues, midwives feel safe when they face ethical dilemmas, which facilitates their ethical decision making.
The findings suggest that various measures and initiatives are needed to reduce midwives’ experience of ethical dilemmas in the delivery room and to ensure appropriate ethical decision making. To provide ethical health care to women and newborns at birth, evidence-based birth approaches should be adopted by all health professionals, and the job descriptions and authority of midwives should be respected by the team and hospital management. Training can be planned to improve the communication skills of midwives and to facilitate the ethical decision-making process. For midwives to fulfill their independent professional roles, midwifery education and profession should be strengthened by the government policies. Finally, further studies should be carried out to evaluate the ethical dilemmas of midwives.
Limitations
This study has two main limitations. First, the sample group consisted of midwives who had received postgraduate education. It does not include the ethical dilemma experiences of midwives with different education levels. Second, the narratives in this qualitative study were recorded in Turkish. Therefore, certain expressions, including cultural words, could not be translated into English.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Ethical approval was granted by Manisa Celal Bayar University Health Sciences Ethics Committee (Date: 16.12.2016 No: 372). This study was approved as Hazal Türken’s midwifery master thesis by Manisa Celal Bayar University Health Sciences Institute in 2019.