
Abstract
Background
Protecting a person’s right to privacy and confidentiality is important in healthcare services. As future health professionals, nursing students should bear the same responsibility as qualified health professionals in protecting patient privacy.
Objectives
To investigate nursing students’ practices of patient privacy protection and to identify factors associated with their practices.
Research design
A cross-sectional study design was adopted. A two-part survey was used to collect two types of data on nursing students: (1) personal characteristics, including demographics, clinical experience and use of information and communication technology and social media and (2) practice of patient privacy protection, collected using the Patient Privacy Scale.
Participants and research context:
A total of 319 nursing students aged 18 or above, studying pre-registration nursing programmes and who had attended at least one block of clinical placement, were recruited from a university in Hong Kong.
Ethical considerations
The study received ethical approval from the Survey and Behavioural Research Ethics Committee of the Chinese University of Hong Kong. The participants were informed of the study aim and written consent was obtained before completing the survey.
Findings:
The mean total score on the Patient Privacy Scale was 119.7 out of 135. Nursing students who were regular users of Instagram and those who had never taken photographs with patients and hence did not need to obtain patient consent were associated with better practices of patient privacy protection (higher total scores on the Patient Privacy Scale).
Conclusions
The findings improve our understanding of nursing students’ practice of patient privacy protection and the associated factors. This will inform the development and revision of current strategies to enhance nursing students’ practice of patient privacy protection, especially their use of social media.
Introduction
Privacy and confidentiality are fundamental human rights in society generally and in healthcare systems specifically. 1 Maintaining privacy and confidentiality is important for protecting people from physical, psychological and social harm. 2 As future health professionals, nursing students should bear the same responsibility as qualified health professionals in protecting patient privacy. This study investigated nursing students’ practices of patient privacy protection and to identify factors associated with their practices.
Background
Privacy can be understood as control over others’ access to oneself, including the extent, timing and circumstances of sharing oneself (physically, behaviourally or intellectually) with someone else. Confidentiality, which can be considered a sub-branch of privacy, refers to the prevention of the re-disclosure of information that is initially disclosed within a trustful and fiduciary relationship. 2 Strong protection of the right to privacy and confidentiality is important in healthcare because it increases patients’ confidence in the use of healthcare services and the work of health professionals. In addition, safeguarding these rights helps patients to establish open communication with health professionals and to feel that health professionals can be counted upon. 3
Communication underlies the clinical relationship between health professionals and patients. Communication involves both objective written records and discussions around a patient’s personal health information. Given the importance of limiting data disclosure, health professionals and patients typically discuss measures to ensure the privacy of personal information. 2 However, patient privacy is not limited to personal health information; it extends to other areas, including physical, decisional and proprietary privacy, which are equally as important as the privacy of personal health information. 2 Physical privacy is related to one’s personal space and degree of physical contact with others, decisional privacy concerns one’s choices and proprietary privacy relates to one’s property, which in this context could include images of the body or body parts. 2 Therefore, patient privacy should not focus solely on limiting access to personal health information; rather, other aspects of privacy related to the person under care should also be carefully considered.
Nurses are vital members of a healthcare team. As such, they spend a substantial amount of time with patients. Nurses are more frequently required to handle patients’ personal health information than other health professionals. 4 According to the International Council of Nurses’ (ICN’s) Code of Ethics for Nurses, 5 nurses should hold all personal information obtained in a professional capacity in confidence. The code also states that nurses should only use technology and social media in a way that is compatible with the rights of patients to safety and privacy, including personal, informational or proprietary privacy, as well as confidentiality. 5
With the increasing emphasis on patient privacy in healthcare systems and the existing code of ethics guiding the practice of health professionals, studies have attempted to reveal health professionals’ perceptions and practices around privacy protection and the provision of information.6,7 Studies have shown that both perceptions and practice are generally good among health professionals, including nurses.6,8 However, the obligation to protect patient privacy is not limited to health professionals, such as medically licensed doctors and nurses; it extends to nursing students who are involved in clinical practice as part of their nursing education. During clinical practice, nursing students participate in various care procedures that may involve privacy issues, such as the exposure of a patient’s body during a physical examination. 9 Moreover, nursing students may have to read patients’ written records or interview patients to obtain data. 9 However, although nursing students are required to complete courses on healthcare ethics, information about nursing students’ actual practices to protect patient privacy during clinical practice is lacking. 10 In addition, nursing students are increasingly using information and communication technology (ICT) platforms, such as email, WhatsApp and Telegram, as well as social media platforms, such as Facebook, Instagram and Twitter, to communicate, and these platforms represent potential threats to patient privacy. For example, a study in South Africa revealed that some nursing students experienced blurred boundaries between their personal and professional lives when using social media. 9
No study has yet examined nursing students’ practice of patient privacy protection. Information concerning their use of ICT and social media platforms to share their clinical experience is also limited. An investigation of nursing students’ practice would provide valuable insights to guide the development of relevant interventions to enhance both their understanding and practice of privacy protection; such interventions could be implemented before they begin clinical practice. Therefore, this study investigated nursing students’ practice of patient privacy protection and the correlation between their practice and their demographic characteristics, clinical experience and use of ICT and social media.
Method
Study design
This was a cross-sectional, descriptive correlational study conducted from November 2020 to July 2021 in Hong Kong.
Participants and study setting
Nursing students were recruited using convenience sampling from a local university that offered pre-registration nursing programmes. The inclusion criteria for nursing students were as follows: (1) enrolled in pre-registration nursing programmes at the university; (2) aged 18 years or above; (3) had attended a course covering healthcare ethics; (4) had attended at least one block of clinical placement and (5) could read and understand Chinese. A total of 633 potential students met the eligibility criteria, and the proportion of female to male students was 3:1. Potential students were approached before skill practice sessions or clinic visits when the time and location were suitable for recruitment.
The sample size was determined to ensure that the study had adequate power to identify factors associated with the practice of patient privacy protection. As there was no empirical effect size to guide the sample size estimation, we aimed to detect factors with small to moderate effect sizes with values as small as R2 = 0.025. 11 Using the power analysis software PASS 16.0 (NCSS, Kaysville, USA), it was calculated that a sample size of at least 309 participants would give the study 80% statistical power to detect associations at the 5% level of significance with effect sizes as small as R2 = 0.025.
Study instrument
A self-administered structured questionnaire comprising two sections was used to collect data from the nursing students. These sections covered (1) personal characteristics and (2) practice of patient privacy protection. The personal characteristics comprised demographics, namely, study programme, year of study, age and sex; clinical experience, namely, length of clinical practice, areas of clinical practice and any experience of part-time healthcare-related jobs in a public or private setting, including the length thereof and the use of ICT and social media platforms, namely, WhatsApp, WeChat, Facebook, Instagram and Twitter. The students were asked whether they had used these channels to share clinical experiences. The practice of patient privacy protection was measured using the 27-item Patient Privacy Scale (PPS).12,13 The scale was originally developed by Ozturk et al. 13 and was translated into Chinese by Chen et al. 12 and validated. The PPS is multi-faceted and includes, but is not limited to, informational privacy. The Chinese version of the scale comprises five subscales: (1) confidentiality of personal information and private life (seven items), (2) sexual privacy and management system (eight items), (3) privacy of those unable to protect themselves (four items), (4) physical privacy (four items) and (5) ensuring a favourable environment (four items). The items are scored on a 5-point Likert scale (1 = strongly disagree; 5 = strongly agree). The total scores range from 27 to 135. A higher score indicates a higher level of practice of patient privacy protection. The Chinese version of the scale has been shown to be reliable, with a Cronbach’s alpha of 0.94 for the overall scale and of 0.89, 0.73, 0.87, 0.88 and 0.84 for subscales 1 to 5, respectively. 12
Data collection procedure
Potential participants (nursing students) were initially approached by a member of the research team at the teaching or visiting venue before skill practice sessions or clinical visits. The research staff explained the purpose of the study, eligibility criteria and data collection methods using a face-to-face approach. Moreover, the research team member explained clearly that participation was voluntary and that the participants had the right to withdraw at any time. A paper-based information sheet was distributed to the participating nursing students. Written consent regarding study participation was obtained on site from the participants, who were then asked to complete the paper-based questionnaire. The research team member stayed at the venue and collected all completed questionnaires from the participating students. A monetary incentive of HK $20 (US $2.57 or EUR €2.26) was given upon completion of the questionnaire as a token of appreciation.
Ethical considerations
Ethical approval was obtained from the Survey and Behavioural Research Ethics Committee of the Chinese University of Hong Kong. Permission for the use of the Chinese version of the PPS was obtained from the original author. Written/verbal consent were obtained from participants upon agreement of participation. Participants could withdraw from the study at any time and without giving reasons. All collected data were kept anonymous and confidential.
Statistical analysis
The characteristics related to demographics, clinical experience and use of ICT and social media by the participating nursing students were categorised and presented using frequencies and percentages. The normality of the PPS scores was assessed based on the skewness statistic and normal probability plots. The total PPS score was used to quantify the students’ practices of patient privacy protection. Univariate analyses based on independent t-tests and one-way ANOVA were conducted to identify student characteristics potentially associated with the total PPS score. Characteristics with p < .1 in the univariate analyses were selected as candidate independent variables for a multivariable regression analysis to delineate factors significantly and independently associated with the total PPS score. As most of the regular users of Twitter were also regular users of Instagram, these two variables were combined into a composite independent variable with four levels (regular users of Instagram and/or Twitter) before entering into the multivariable regression analysis. All statistical analyses were performed using IBM SPSS 25.0 (IBM Corp., Armonk, NY, USA). All statistical tests were two-sided with the level of significance set at 0.05.
Results
Recruitment and response rate
Demographics and clinical experience of the study sample (N = 319).

Data are presented as frequency (%).
Participants’ characteristics
Uses of information and communication technology (ICT) and social media.
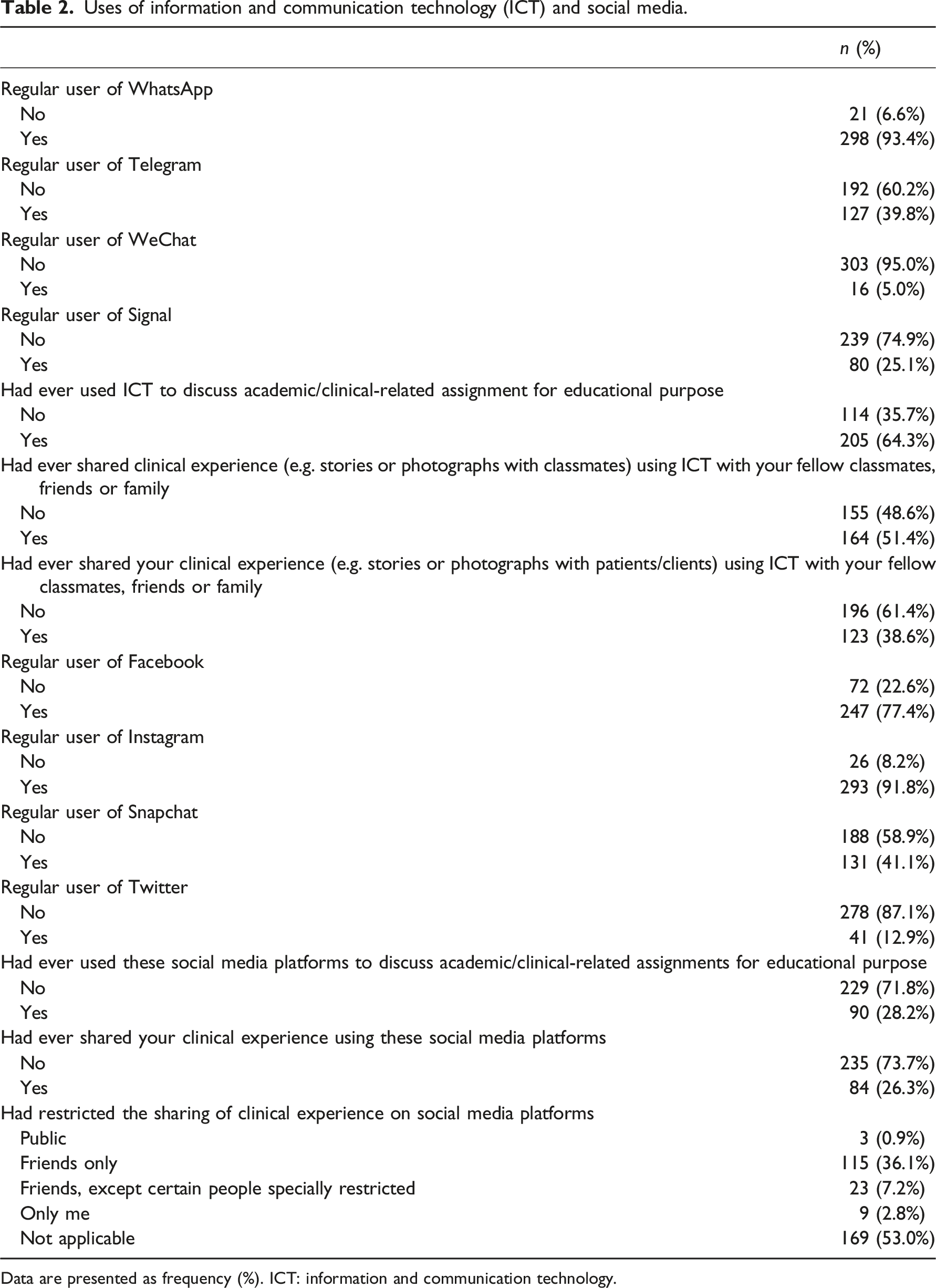
Data are presented as frequency (%). ICT: information and communication technology.
Practice of patient privacy protection
Scores of the Patient Privacy Scale.
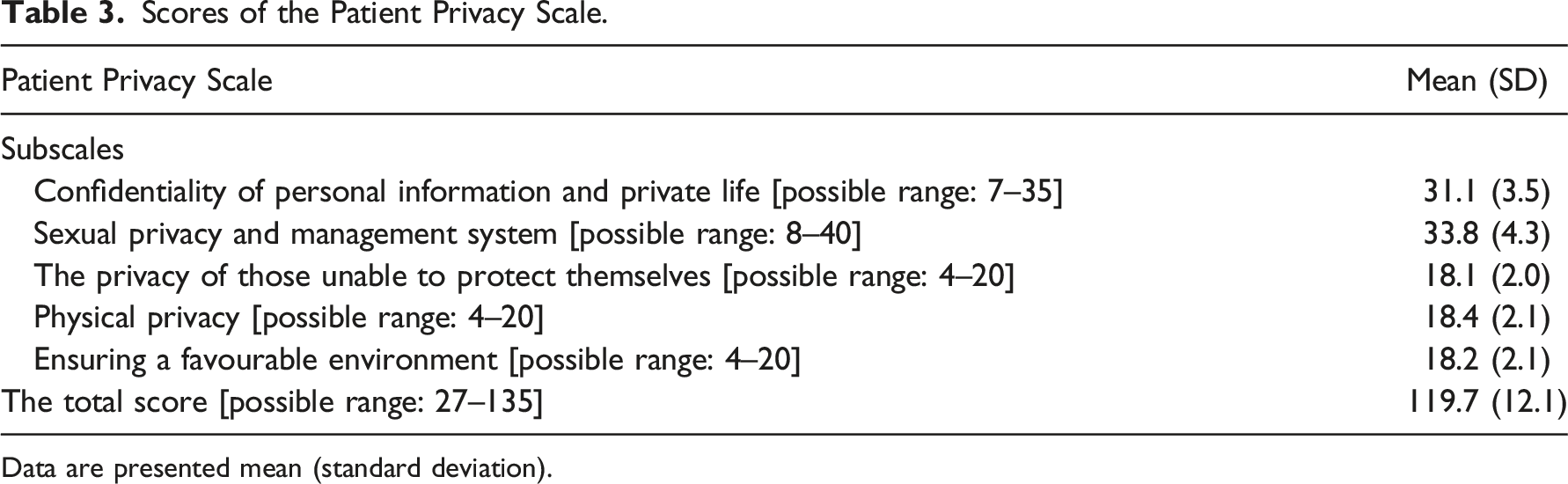
Data are presented mean (standard deviation).
Factors associated with practice of patient privacy protection
Total score of Patient Privacy Scale by demographics and clinical experience of nursing students.
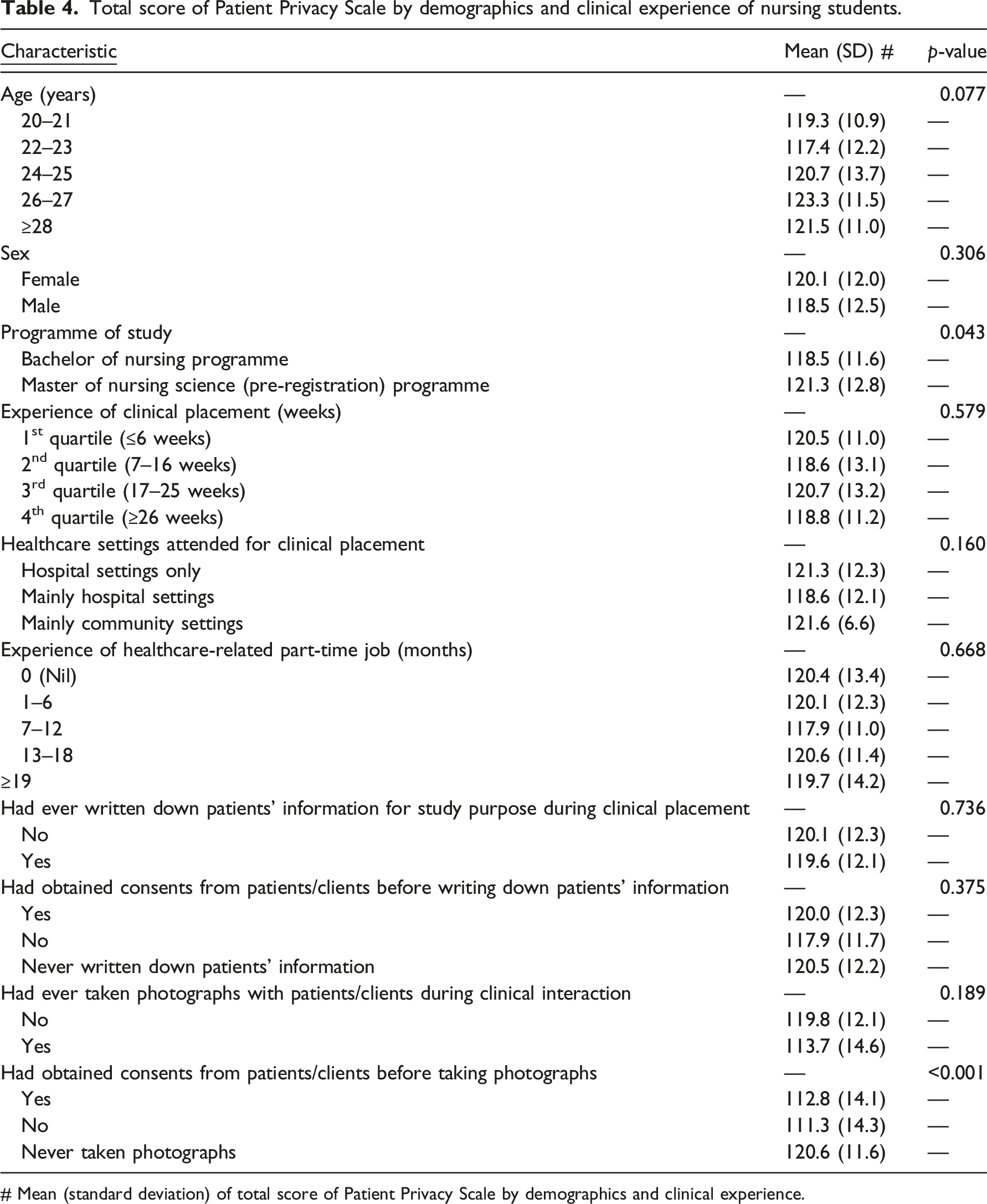
# Mean (standard deviation) of total score of Patient Privacy Scale by demographics and clinical experience.
Total score of Patient Privacy Scale by characteristics related to uses of information and communication technology (ICT) and social media.
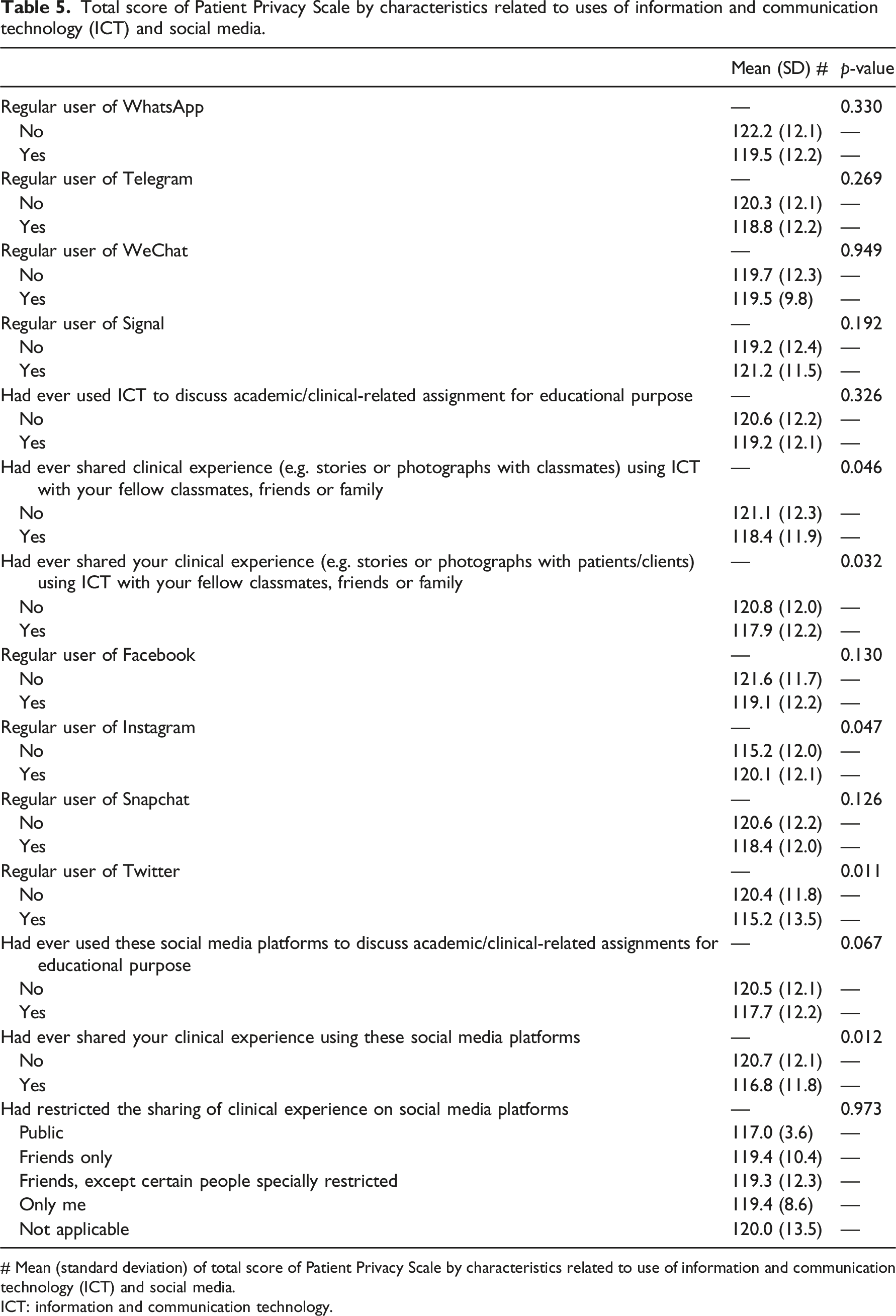
# Mean (standard deviation) of total score of Patient Privacy Scale by characteristics related to use of information and communication technology (ICT) and social media.
ICT: information and communication technology.
Regression analysis of nursing students’ characteristics regarding demographics, clinical experience and uses of ICT and social media associated with the total score of Patient Privacy Scale.
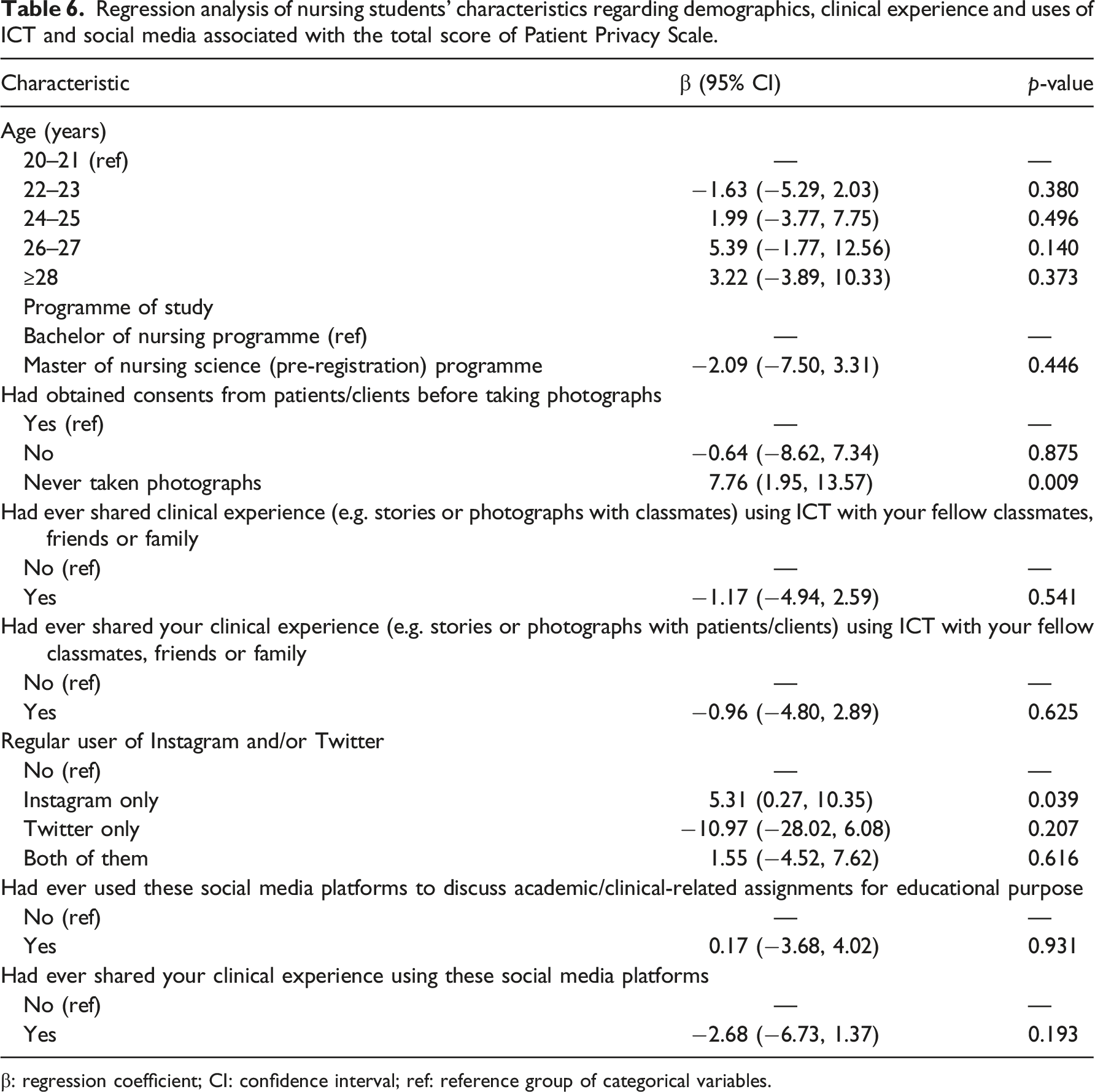
β: regression coefficient; CI: confidence interval; ref: reference group of categorical variables.
Discussion
This is the first study to investigate nursing students’ practices of patient privacy protection and to identify factors associated with their practices. Two major student characteristics were significantly associated with the total PPS score, namely, regular use of Instagram and never having taken photographs with patients.
The total PPS score and the scores of the subscales of the PPS for these students on pre-registration programmes were high and were comparable to those found by Chen et al., 12 whose participants were graduate nurses working in a clinical setting with between one and more than 11 years of experience. The scores revealed that our nursing students were aware of the importance of practising patient privacy when providing nursing care. The students in pre-registration nursing programmes in this study are required to complete courses on healthcare ethics during their junior years of study before commencing their first clinical practice. Patient privacy and confidentiality are heavily emphasised in these courses and students are continually reminded of their importance. Students in all clinical practice courses are assessed for professional behaviour using a checklist that covers professional attitude and practice. Maintaining patients’ confidentiality and privacy at all times is a critical item on this checklist and students cannot complete the clinical practice courses without satisfying this criterion. 10 Through continual reminders and regular assessments, patient privacy protection is incorporated as an essential duty of nursing students during their clinical practice.
The ICN’s Code of Ethics mentions that nurses should pay attention to and respect patients’ privacy and confidentiality in relation to personal matters, information or freedom from intrusion into one’s physical body. 5 The scores of the subscales reflected that the students generally understood the breadth of not only informational privacy but also physical, sexual, decisional and environmental privacy. More than 85% of the students agreed or strongly agreed with the measures used to protect the multiple aspects of privacy included in the PPS. In view of the multi-faceted nature of privacy, a clearer and more comprehensive explanation of privacy should be included in the ICN’s Code of Ethics.
Notably, in our study, we found that being a regular user of Instagram was associated with a higher PPS score. The better practice among Instagram users may be related to the fact that it is currently the most commonly used social media platform by university students in Hong Kong. Students are therefore aware that any inappropriate posts on Instagram will immediately be discovered by their classmates. A study in mainland China found that most nursing students spent at least 2 to 4 h a day using social media and half of them had witnessed inappropriate posts from their classmates, such as negative comments about university teachers, offensive language and breaches of patient confidentiality. 14 In Hong Kong, several incidents have been reported of nursing students using a social media platform (Facebook) to share clinical experiences in a way that breached patient privacy.15,16 The students involved eventually received penalties leading to suspension of studies and delayed graduation.15,16 These events may have alerted the nursing students in our study to the importance of appropriate posting behaviour on popular social media. Thus, topics on appropriate social media behaviour should be incorporated into healthcare ethics or clinical practice courses to reinforce nursing students’ awareness of the proper use of social media platforms so that they adopt good practices of patient privacy protection at all times.
With the increasing use of mobile phones, all students are likely to own one, making it easy for them to take photographs in clinical settings. A previous study found that nursing students usually did not obtain patients’ consent before doing so. 9 In the current study, our nursing students did have a good awareness of the importance of maintaining patient privacy and confidentiality. The responses to the question about obtaining patients’ consent before taking their photograph included the option ‘not applicable’. Many respondents chose this option, indicating that they knew it was inappropriate to take photographs of or with patients during clinical practice regardless of whether consent was obtained. Refraining from doing so minimises the risk of accidental disclosure of patients’ information or medical status. Thus, it is important for the academic staff responsible for students during their clinical practice to remind them about appropriate behaviour in relation to the use of mobile phones and photography.
It was noticed that the study response rate was high, which may have been related to the monetary incentive that was provided for study participation and questionnaire completion. During the data collection period, the research staff (the data collectors) usually arrived early at the venues for data collection, typically 20–30 min before the start of the skill practice sessions or clinic visits. Usually, the students arrived at these venues 15 min before the start of the sessions. Thus, our research staff had adequate time to approach them, explained the study purpose and obtained their consent. The students generally spent around 5–10 min completing the questionnaire. Questionnaire completion did not affect classes/visits, which was why many students were willing to complete the questionnaire.
This study has some limitations. First, the sampling method was convenience sampling in a university. This may limit the generalisability of the study findings to other nursing students at other universities offering pre-registration nursing programmes in Hong Kong. Second, the data on the practice of patient privacy protection were self-reported, raising the possibility of social desirability bias in the results. In addition, the study topic was related to privacy, which might have raised the respondents’ awareness of the importance of privacy, causing bias in the responses. Third, because of its survey design, the study may have been unable to acquire a deeper understanding of the use of ICT and social media by students in relation to the protection of patient privacy. A better understanding of how responsible nursing students are in this respect could be obtained through qualitative methods in a future study. Fourth, the PPS included items mainly related to ICT. Both ICT and social media platforms are increasingly being utilised by students to discuss their academic and clinical assignments; thus, the PPS should be updated to include items covering both ICT and social media.
Conclusion
Nursing students’ practice of patient privacy protection was generally good, and several factors, namely, the use of social media and the act of taking photographs, were associated with the level of patient privacy protection. The findings will inform the development and revision of current strategies to enhance nursing students’ practice of patient privacy protection, especially the proper usage of social media.
Footnotes
Acknowledgements
We thank all of the research and teaching staff for their support and help with participant recruitment.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Seeding Grant for Developing Teaching and Learning Strategies [Ref No., TL2001]