
Abstract
Background
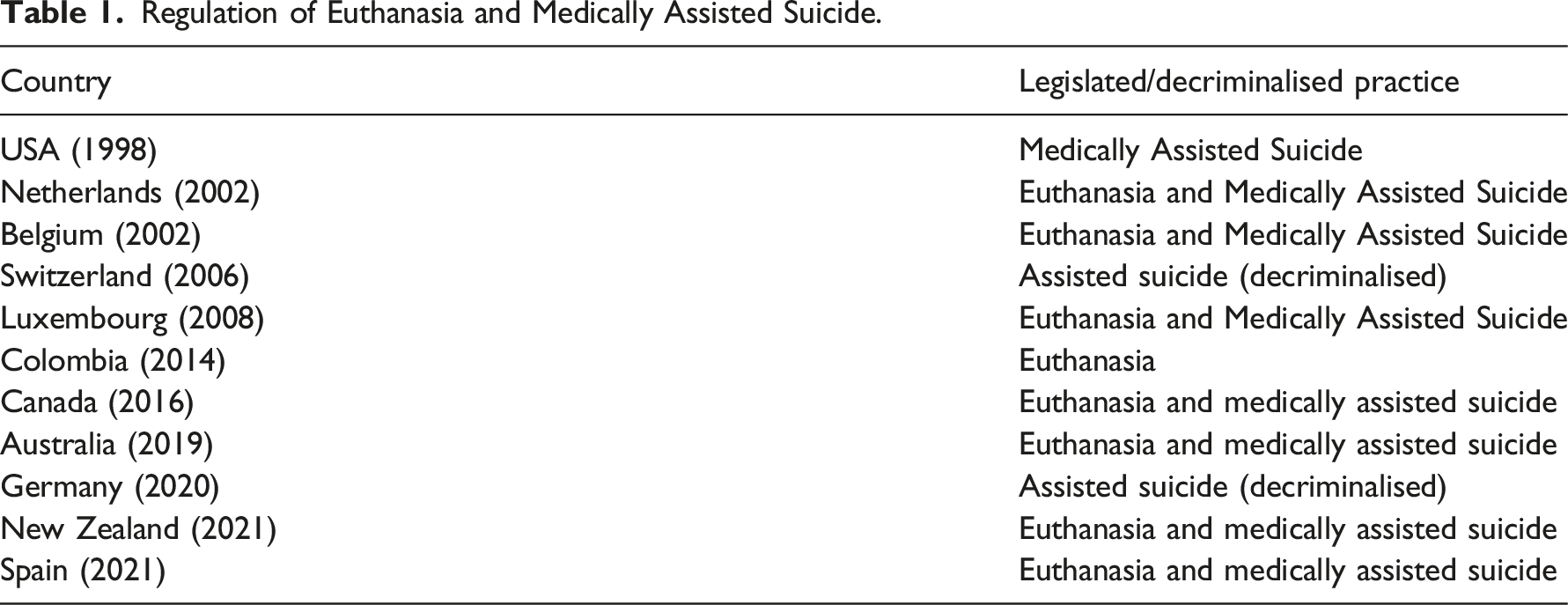
Safeguarding the right to die according to the principles of autonomy and freedom of each person has become more important in the last decade, therefore increasing regulation of Euthanasia and Medically Assisted Suicide (MAS).
Aims
To learn the opinions that the nurses of the autonomous region of Madrid have regarding Euthanasia and Medically Assisted Suicide.
Research design
Cross-sectional descriptive study.
Participants and research context
All registered nurses in Madrid. The study was done by means of a self-completed anonymous questionnaire. The variables studied were social-demographic, giving opinions about Euthanasia and MAS.
Ethical considerations
Each participant was assured maximum confidentiality and anonymity, ensuring the ethical principles set out in the Declaration of Helsinki, as well as in the Organic Law 3/2018, on Personal Data Protection and guarantee of digital rights.
Findings
A total of 489 nurses answered the questionnaire. In total, 75.7% of the nurses confirmed that Euthanasia should be regulated in Spain. 66.3% indicated that information on Euthanasia should be provided jointly by doctors and nurses, and 42.3% considered that it could be applied by both medical and nursing professionals. A total of 87.2% advocated the participation of nurses in health policy, influencing the drafting of the law. In the face of possible regulation, 35% would request Conscientious Objection, being closely related to their religious beliefs.
Discussion
Different authors point out that nurses’ perceptions and attitudes towards Euthanasia are conditioned by different factors, such as religion, gender, poor palliative care, legality and the patient's right to die.
Conclusion
Nurses are positioned in favour of the regulation and practice of Euthanasia and MAS, depending on their age, years of experience, training, model of care and especially religious beliefs.
Keywords
Introduction
This document addresses nurses' attitudes towards Euthanasia and Medically Assisted Suicide (MAS) in relation to the regulatory text itself, a few months prior to the actual regulation of the Assistance in Dying Benefit in Spain. Special importance is given to possible cases of nurses showing conscientious objection and their participation in the process.
Background
The literature shows different studies1,2 related to nurses’ attitudes towards euthanasia and its regulation. However, only few studies address the attitudes related to the nurses’ own role during this process,3,4 including conscientious objection, which is one of the most important prerequisites for its legalisation, as has been pointed out by the International Association for Hospice and Palliative Care (IAHPC). 5
Despite the crucial role of nurses in the process of providing assistance in dying, they are in most cases not taken into account in such discussions. 3
Regulation of Euthanasia and Medically Assisted Suicide.
Death, beyond a biological event, encompasses a social, spiritual and anthropological fact that has been changing over time, influencing in an important manner the ways of acting, thinking and feeling of both patients and healthcare professionals.
Safeguarding the right to die according to the principles of autonomy and freedom of each person has become more important in the last decade. These arguments have created the greatest controversy in the ethical debate on Euthanasia and MAS. 8
As the bioethicist Simón Lorda 9 pointed out, there is a sufficient degree of ethical agreement with respect to the limitation of life-sustaining treatment, refusal of treatment and palliative sedation as acceptable actions, which are in turn included from the legal point of view. However, there is no such ethical agreement on Euthanasia or Medically Assisted Suicide, which is still classified as the criminal offence of homicide in many countries.
Nevertheless, within the ethical debate on the end-of-life process, it is worth considering whether there are differences between allowing death as a process of disease progression by limiting life-sustaining treatments, shortening life in the face of a refractory symptom in a terminal situation by means of palliative sedation, or causing death in a situation of total suffering expressed by a patient repeatedly by means of Euthanasia or MAS.
In recent years, in countries such as Spain,10–15 these reflections have led to a growing social trend of support for the regulation of Euthanasia and MAS, both by citizens and healthcare professionals, reflected in several legislative proposals for their regulation.
In 2017, two legislative proposals were presented, one that sought the regulation 16 of euthanasia and MAS, and another that proposed only the decriminalisation 17 of both practices through the modification of the Spanish Penal Code. 18
In 2018, another new attempt at regulation 19 was presented, and finally, on 31st January 2020, the Chamber of Deputies approved the proposal for the Organic Law on the Regulation of Euthanasia, 20 which, after several amendments by the Congress and the Senate, was approved on 24th 2 March 2021, 1 and came into force on 25th June 2021.
It establishes its purpose and scope of application, the requirements for people to be able to request the provision of aid in dying and the conditions for its exercise (Figure 1), using criteria very similar to previous international regulations, especially European ones; by highlighting the need to be an autonomous, repeated decision, in a context of terminally ill or chronic, advanced illness with unbearable suffering.
21
Requirements for the application of Euthanasia or MAS in Spain.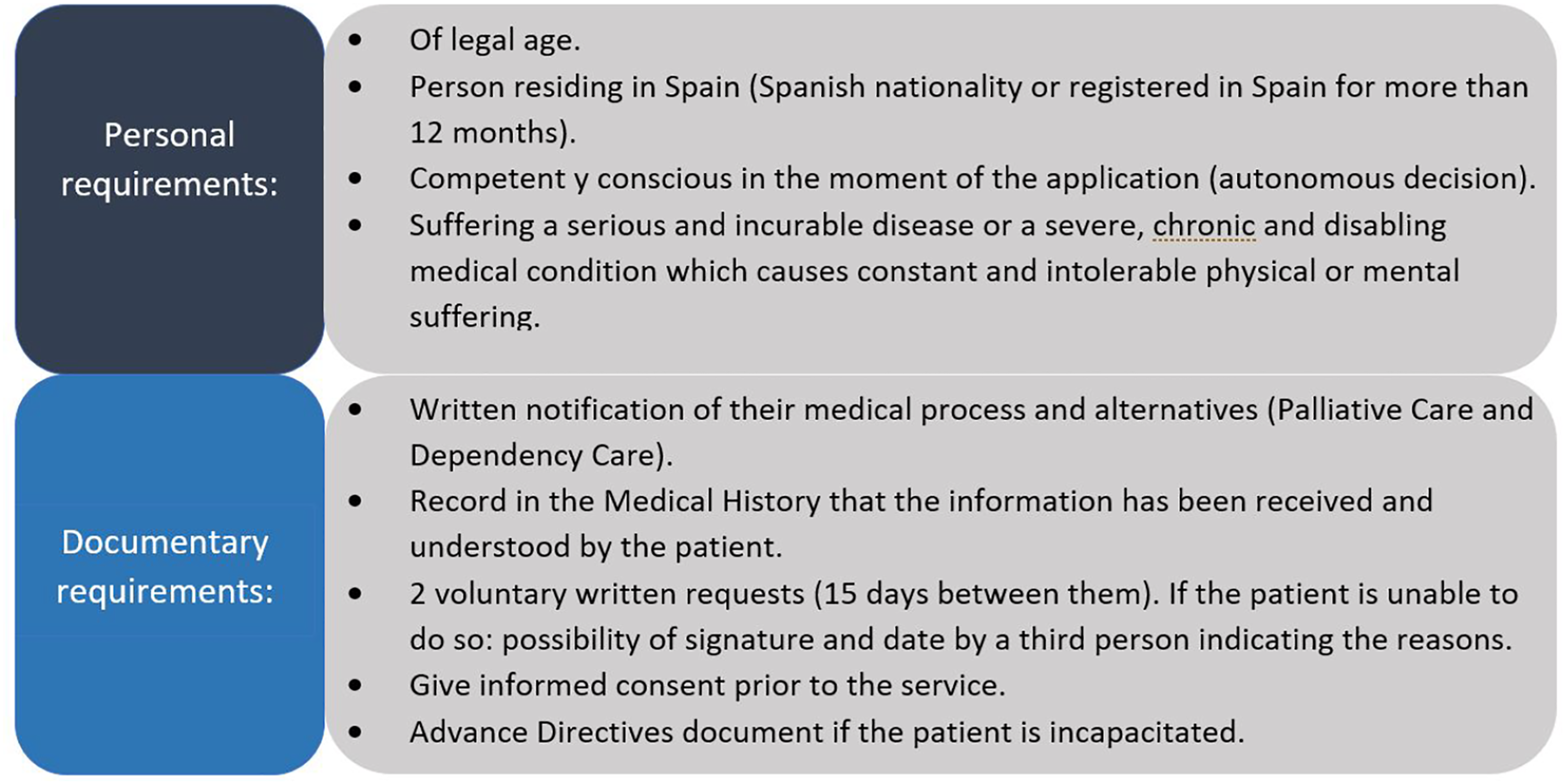
The Spanish law sets out the procedure to be followed for the provision of aid in dying and the guarantees to be observed, stipulating three mandatory prior verification filters: the responsible doctor, the consultant doctor and the Guarantee and Evaluation Commission (GEC) (Figure 2). It should be noted that this multidisciplinary commission is created at regional level as a body with pre- and post-verification functions, which is one of the main differences with the rest of the approved regulations of other countries, where the commissions only have functions after the service has been provided, not before.
21
Procedure for the regulation of Euthanasia and MAS in Spain.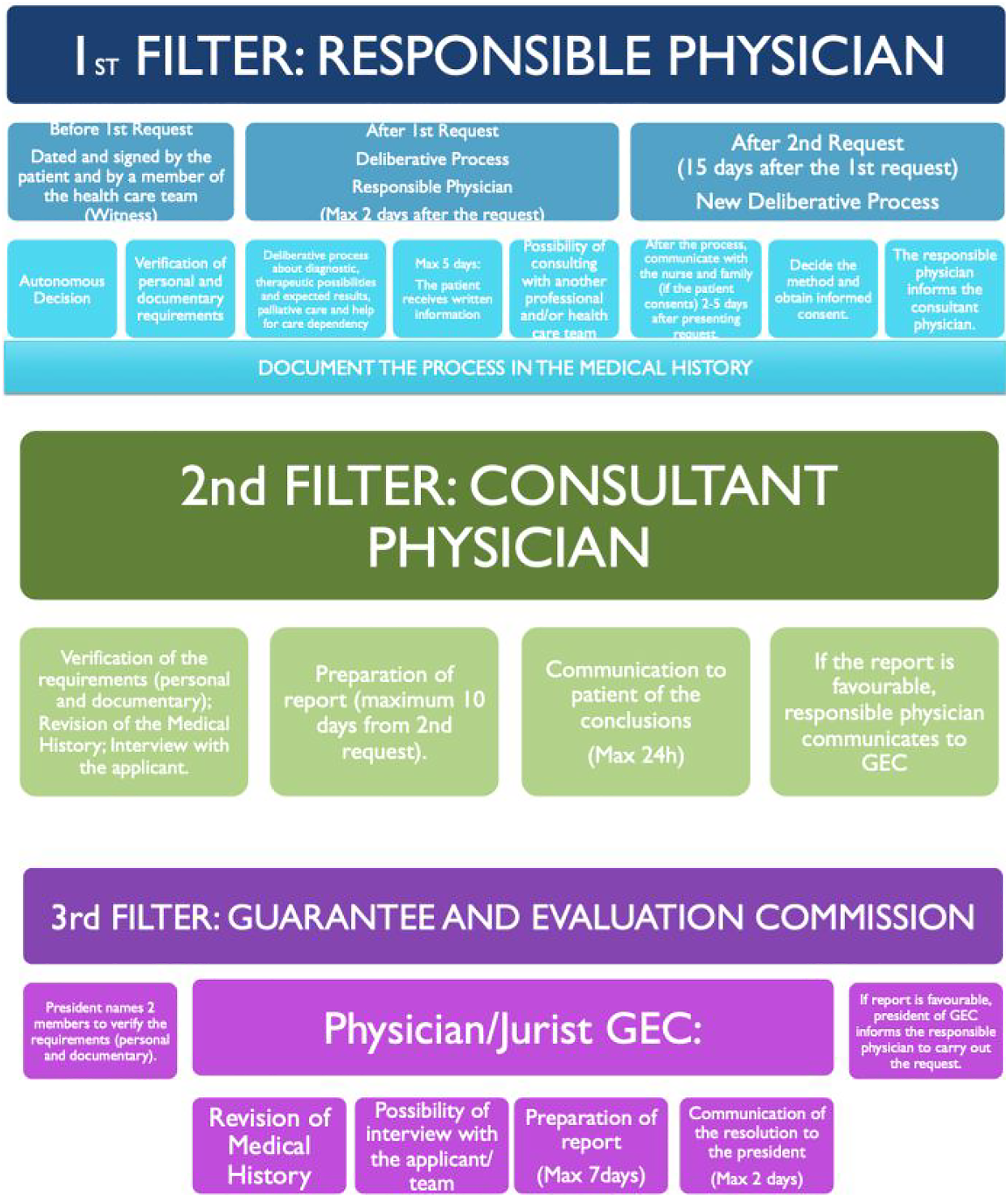
The Spanish law guarantees equal access to the service for all citizens, including both public and private centres.
It also regulates the right of the health professionals directly involved to exercise Conscientious Objection (CO) by creating a specific register in each Community or Autonomous Region. In this aspect, the main differences with European regulations are that the Netherlands and Luxembourg only contemplate the possibility of CO for doctors, while Belgium includes, in addition to doctors, that no professional will be obliged to provide assistance in a euthanasia procedure, and nurses can be included in this sense. 21
Organic Law 10/1995, of 23rd November 1995, of the Penal Code 18 was amended with the aim of decriminalising all Euthanasia related conducts to be carried out in the specific cases established in the law, including all professionals involved, unlike in Holland, Belgium and Luxembourg, where only the doctor is exempt from criminal liability. 21
One of the main problems in the Spanish law is the lack of clarity regarding the role of healthcare professionals in the provision of aid in dying, especially nurses, as is the case with most regulations. 21 The word nurse only appears on two occasions in the entire law, the rest being supposedly included under health professionals or healthcare team. The law only states that the nurse will be informed of the outcome of the deliberation between the patient and the assigned responsible doctor, without clearly defining her/his involvement or the functions she/he will have during the process.
Studies22–27 on the role of the nurse in end-of-life care, including Euthanasia and MAS, point to major shortcomings in both the establishment of the nurse's role and responsibilities.
In the Dutch law, for example, despite the efforts made during the legislative process by nursing associations to include the nurse’s functions throughout the process and also in the modification of the criminal code, only the responsible doctor is referred to; without contemplating or specifying the nurse’s role, whose participation is penalised. However, different studies22,23 show the importance of including the nurse in the regulatory text, as, since the Dutch regulation of Euthanasia in 2002, the nurse has been involved before, during and after the provision of aid in dying, with the legal consequences that may follow.
In the Belgian law, it at least stipulates that requests for Euthanasia must be discussed by the nursing team that has regular contact with the patient. As such, the nurse is expected to play a role during the deliberation stage, but with involvement during the administration of the drug also being penalised. However, as in the Netherlands, there is great variability24,25 in both the nurse’s involvement in the deliberative process (100% nursing homes; 58.6% hospitals; 44.4% homes) and in the process of direct administration of the lethal drug (0% nursing homes; 13.5% hospital; 43% homes).
Therefore, whether the nurse’s role is or is not recognised in the legal norm, the reality is that it is part of the holistic care in the process of caring for people who request Euthanasia, especially in the patient’s need for accompaniment and support throughout the process of their illness.
At the end of a person’s life, they experience a special fragility and care dependency, which, without the recognition of their autonomy, can compromise their dignity. Therefore, when faced with a request for assistance in dying, their care specifically implies establishing a relational link with the patient that guarantees the creation of a context of well-being that allows the patient's values to be explored and their life experience to be addressed. 26
In this sense, there is much that nurses can contribute to the process of aid in dying, as reflected in the Canadian context27,28 including participation in the assessment of the patient’s competence and capacity, providing information on aid in dying, coordinating the process, preparing equipment and intravenous access, coordinating and informing healthcare personnel, documenting, supporting patients and their loved ones, and providing after-care.
It will be essential for nurses to participate actively in the discussions and development of policies involving care during the dying process, especially in the regulation of a practice that has so many ethical, social, legal, deontological and clinical connotations such as Euthanasia and MAS; including the defence of a comprehensive palliative approach and shared care planning as the central axis of health care. The nurse, due to her/his privileged position of continuous contact with the patient and the family, must ensure a correct process of reflection and deliberation, acting as a guarantor of care, carrying out a holistic and comprehensive bio-psycho-social and spiritual approach.
For all these reasons, nurses will play an important role in the process of providing assistance in dying, and it is essential to know their opinion in order to be able to include it in the regulatory text.
Objective
To find out the opinion and attitudes of nurses in the Community of Madrid on the regulation of Euthanasia and MAS in Spain.
Population and methods
Design: an observational, descriptive, cross-sectional study was carried out from September to November 2020.
Study population: all nurses registered in the Official College of Nurses of Madrid.
Inclusion criteria: the nurses surveyed had to be members of the Official College of Nurses of Madrid (Colegio Oficial de Enfermería de Madrid) and agree to participate in the study.
It should be noted that in Spain professional membership is compulsory in order to be able to work as a nurse, so all nurses must be registered in their region’s respective College of Nurses.
Sampling: Non-probabilistic by convenience in order to facilitate the participation of all nurses in the Community of Madrid, given that registration is compulsory, and thus ensure that they could participate and express their opinion on a subject in which nursing is directly involved, and to gather the different sensitivities and ideologies present in the group.
Sample size: The sample size was calculated based on the target population (53,000 registered nurses), under the assumption of maximum uncertainty with an expected proportion of 50%, which was estimated at 382 participants with a confidence level of 95% and a precision of 5%. Taking into account a loss rate of at least 20%, 459 nurses would need to participate.
Measuring instrument: an ad hoc, structured, self-administered questionnaire was designed through the GoogleForms platform, consisting of 34 questions with Likert-type, dichotomous variables, based on studies 29 conducted by other professional associations to compare results, and according to specific aspects included in the legislative proposal. Nine items related to socio-demographic variables were included (sex, age, years of experience, speciality, model in which the main activity is practised, setting, beliefs, training in bioethics and palliative care); and 25 items related to qualitative variables (opinion and attitudes towards Euthanasia and MAS). To avoid bias caused by possible terminological confusion, the accepted definitions of Euthanasia and MAS were included in the informed consent information sheet, on the basis of which the rest of the questions were subsequently developed.
The following procedures were used to validate the questionnaire: - Expert panel consisting of nurses with experience and training in clinical bioethics and palliative care. - Pilot study of a representative sample of the study population.
Data collection process: Through the database of the Official College of Nurses of Madrid, an email was sent to all members informing them of the aim of the study and inviting them to participate voluntarily, together with a link to access the online platform. The link to the survey was kept open throughout the study period on the main CODEM (acronym in Spanish of the Official College of Nurses of Madrid) web page.
Ethical considerations: When send the questionnaire to the participants, they were first informed of the objectives of the study and they were asked for their agreement to participate (informed consent). Each participant was assured maximum confidentiality and anonymity, ensuring the ethical principles set out in the Declaration of Helsinki. All information collected was treated in accordance with Organic Law 3/2018, of December 5th, on Personal Data Protection and guarantee of digital rights. The study was approved by the Ethics Committee of the San Carlos University Hospital.
Statistical analysis: Qualitative variables are described using absolute and relative frequency percentages for each category, and associations were sought using the chi-square test or Fisher’s exact test. To calculate the estimated effect according to the Predominant Reasoning (PR or exponent b) of the predictor variable ‘religious beliefs’, the responses of the different interventions in which nurses would declare themselves Conscientious Objectors were recoded, dichotomising the categories for inclusion in a regression model. For the analysis variables, a confidence interval for 5% alpha error was calculated using SPSS software ver. 22.0.
Results
Characteristics of the participants
A total of 489 surveys were obtained from the nurses in Madrid that participated in the study. A total of 86.3% (422) were women aged between 31 and 40 years (202). A total of 25.8% (126) of the respondents were professionals with more than 20 years of work experience. A total of 78.9% (386) worked in the public health system. Most of them, 68.3% (334) worked in hospital care.
With respect to training, 77.5% (379) did not have a recognised nursing speciality. A total of 60.7% (297) reported having received training in Bioethics during their degree and 48.3% (236) had postgraduate training in palliative care.
Of the nurses surveyed, 52.8% (258) considered themselves to be religious believers, and 77.7% (380) considered that religion influenced their attitude towards Euthanasia in a fairly or very important way.
Participants' opinion on Euthanasia
75.7% (370) and 72.6% (355) of the nurses from Madrid who participated in the study said that both Euthanasia and MAS respectively should be regulated by law in Spain, with 81% (396) stating that each person has the right to decide how they want to live and choose how they want to die.
Likewise, 87.2% (426) said that nurses should participate in guiding and influencing the drafting of the law through the Professional Colleges.
As the main reason that leads a sick person to request to end his/her life, 59.5% (291) indicated the loss of complete physical autonomy and freedom as a person, followed by unbearable physical pain as the second cause in 30.7% (150).
The inferential analysis shows significant statistical relationships between age, years of work experience as a nurse, training, model of care and especially religious beliefs.
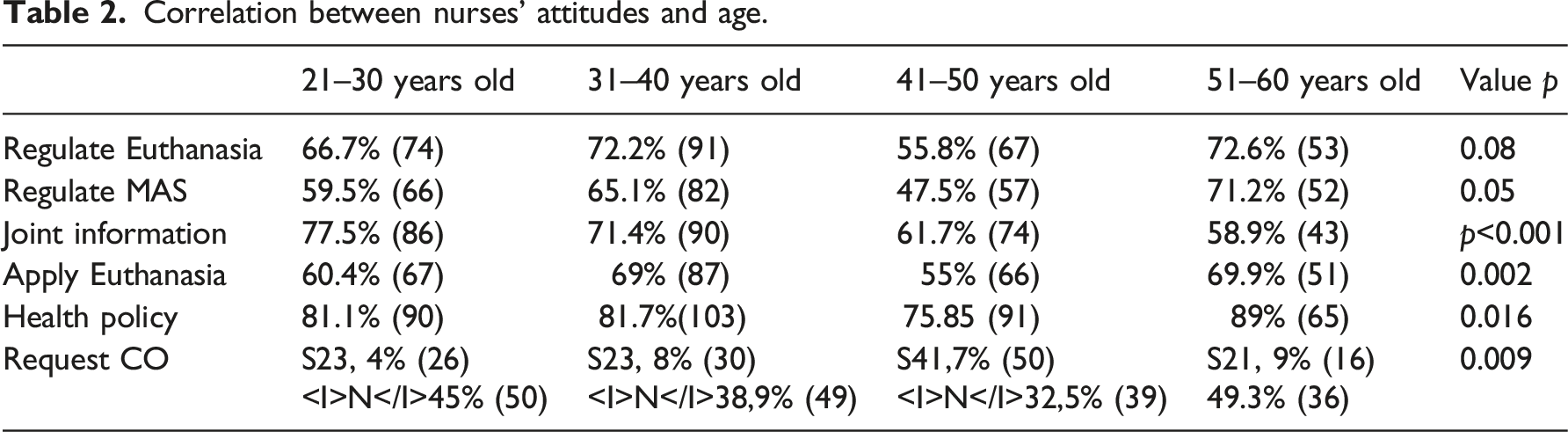
Correlation between nurses’ attitudes and age.
With regard to work experience, respondents with more than 30 years’ experience were more in favour of the regulation of Euthanasia and MAS in Spain (p = 0.05).
In relation to training, nurses from Madrid who participated in the study with postgraduate training in both bioethics (100% PhD and 88.3% courses) and palliative care (83.9%) were more in favour of the need for nurses' participation in health policy through Professional Colleges (p < 0.001).
Correlation between nurses’ attitudes and the healthcare model.

The variable that showed the greatest differences in all categories was religious beliefs, where religious believers were more opposed to the regulation of Euthanasia and MAS, to recognising the right of a person to decide how they want to live and die, and to the need for nurses' participation in health policy (p < 0.001) (Figure 3). Opinion on euthanasia according to religious beliefs.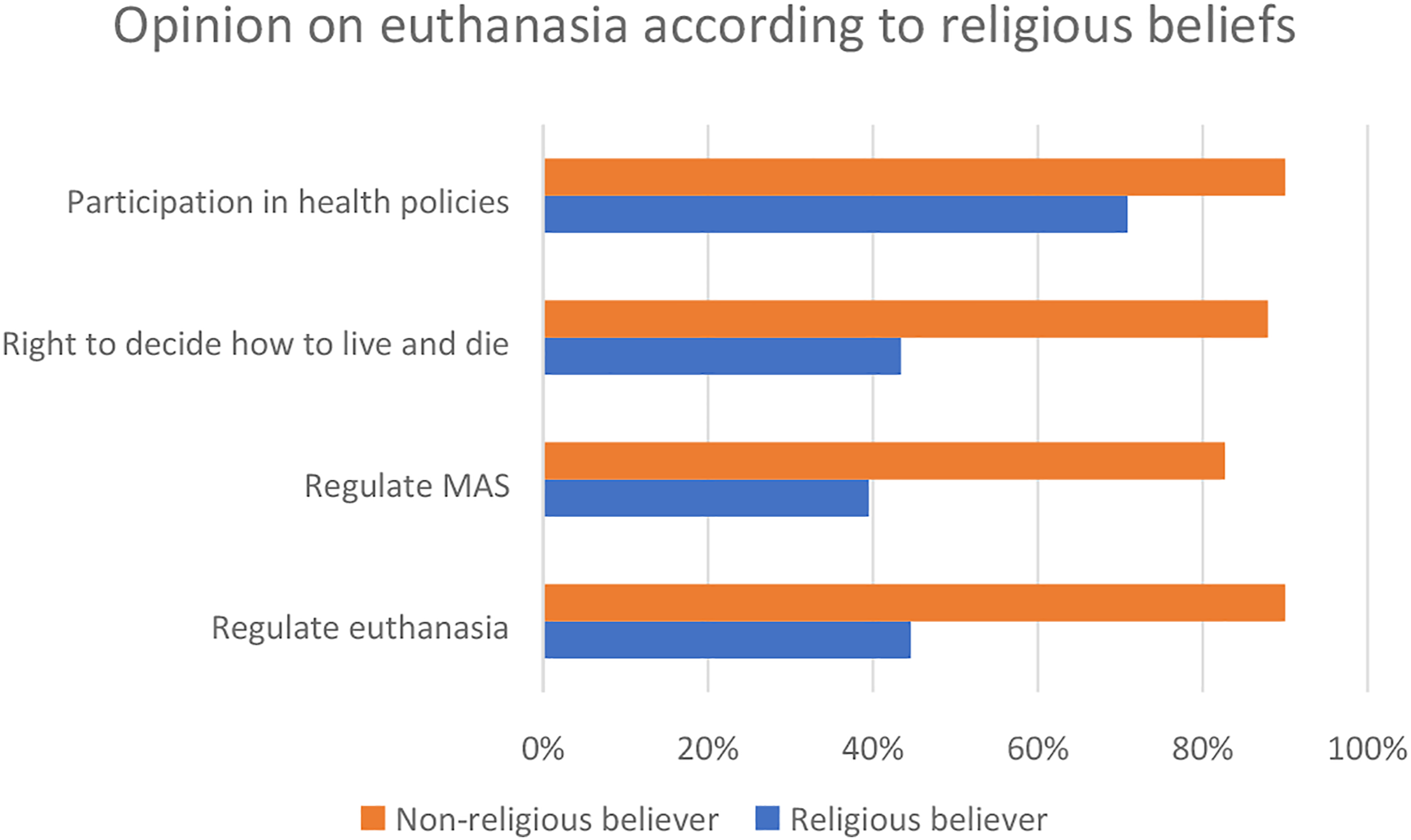
Participants’ opinion of the professionals involved in Euthanasia
When faced with a patient's request for assistance in dying, 66.3% (324) of the nurses from Madrid who participated in the study considered that the information on Euthanasia or MAS should be provided jointly by the doctor and the nurse; as did 42.3% (207) of the nurses that participated regarding the joint doctor/nurse application of Euthanasia.
The inferential analysis shows a significant statistical relationship between age, years of work experience as a nurse, training, model of care and especially religious beliefs.
Respondents over 51 years of age were more in favour of the application of Euthanasia by both nursing and medical professionals, while respondents between 21 and 30 years of age were more in favour of providing joint information rather than applying the service jointly (Table 2).
In this sense, regarding work experience, respondents with 6–10 years of work experience (83.1%) were the most in favour that when a patient requests assistance in dying, information should be provided jointly. Meanwhile, with respect to the application, Madrid nurses who participated in the study with less than 5 years of work experience (55.7%) were the least in favour of it being carried out by both nursing and medical professionals (p = 0.001).
With regard to training, nurses from Madrid who participated in the study with postgraduate training in palliative care (80% Master's degree and 69.9% courses) were more in favour of the need for joint information from the responsible doctor and responsible nurse for the request for Euthanasia (p = 0.06).
Respondents working in public centres were more in favour of the application of Euthanasia by both nursing and medical professionals than those working in private centres (Table 3).
With regard to religious beliefs, non-believing respondents were more in favour of joint information from the doctor and responsible nurse for a request for assistance in dying, as well as of the application of Euthanasia by both nursing and medical professionals (p < 0.001) (Figure 4). Opinion of health professionals involved according to religious beliefs.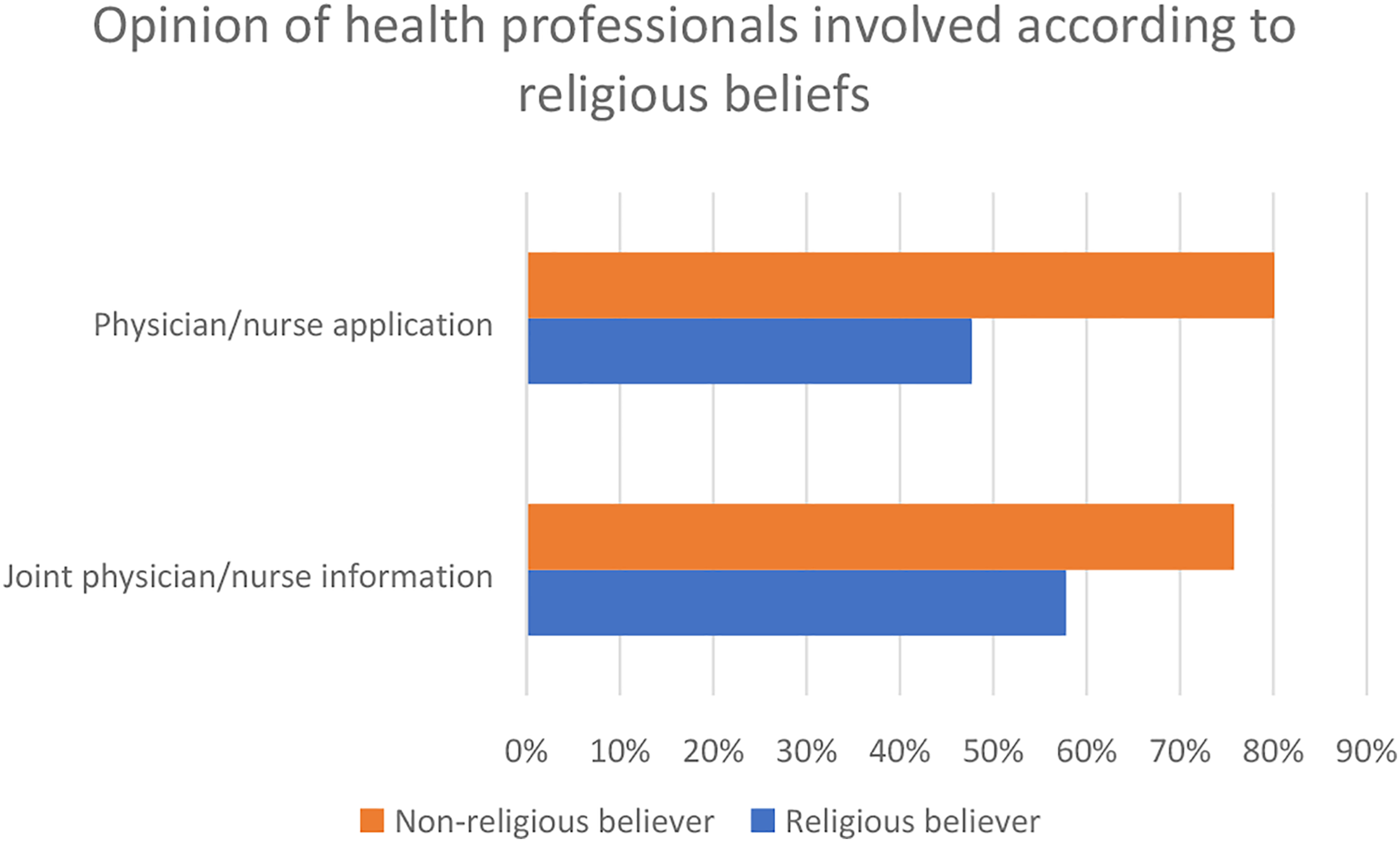
Opinion of the participants on the cases involving Euthanasia to which they would object
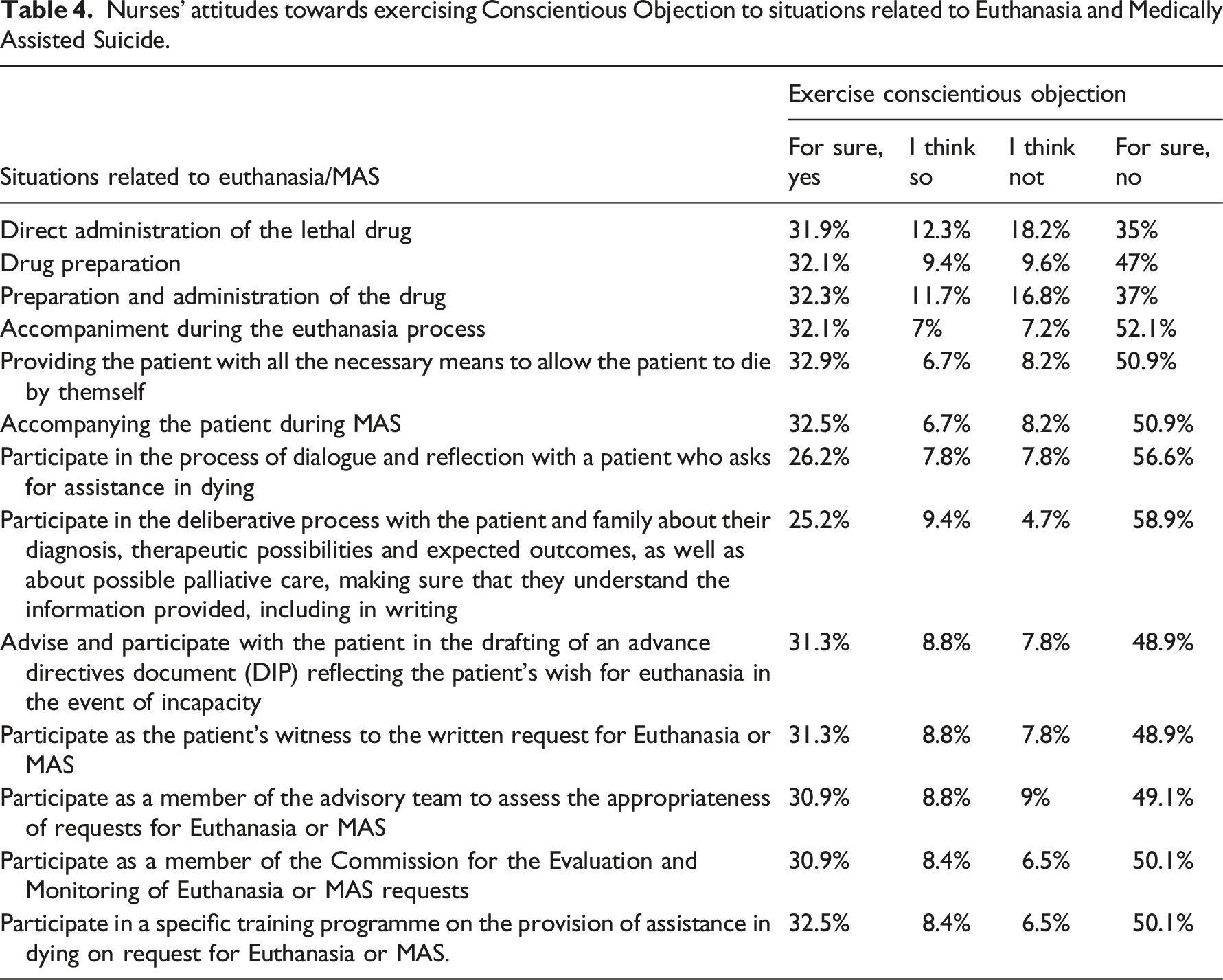
87.5% (428) believed that nurses should have the right to exercise conscientious objection to Euthanasia or MAS, with 35% (171) reflecting that they would request it in the face of possible regulation, compared to 61.9% (303) who would not.
Nurses’ attitudes towards exercising Conscientious Objection to situations related to Euthanasia and Medically Assisted Suicide.
Factors influencing participants' opinions on Euthanasia
Inferential analysis showed significant statistical relationships between age, years of work experience as a nurse, training, model of care and especially religious beliefs.
Those older than 51 years were less favourable to request Conscientious Objection (Table 2).
With regard to work experience, 45.8%(33) of respondents with 16–20 years of nursing experience would definitely apply for Conscientious Objection, compared to 48.1% (50) of those over 30 years of experience and 59.3% between 6 and 10 years of experience, who would not exercise Conscientious Objection (p = 0.002).
Postgraduate training in bioethics (100% Master’s degree, 83.9% master’s degree and 71.9% courses) has a great influence on the knowledge of the right to exercise Conscientious Objection on the part of the nurses from Madrid who participated in the study (55.6% without training, p = 0.005).
Respondents working in private centres were more favourable to declare Conscientious Objection to Euthanasia and MAS than those working in public centres (Table 3).
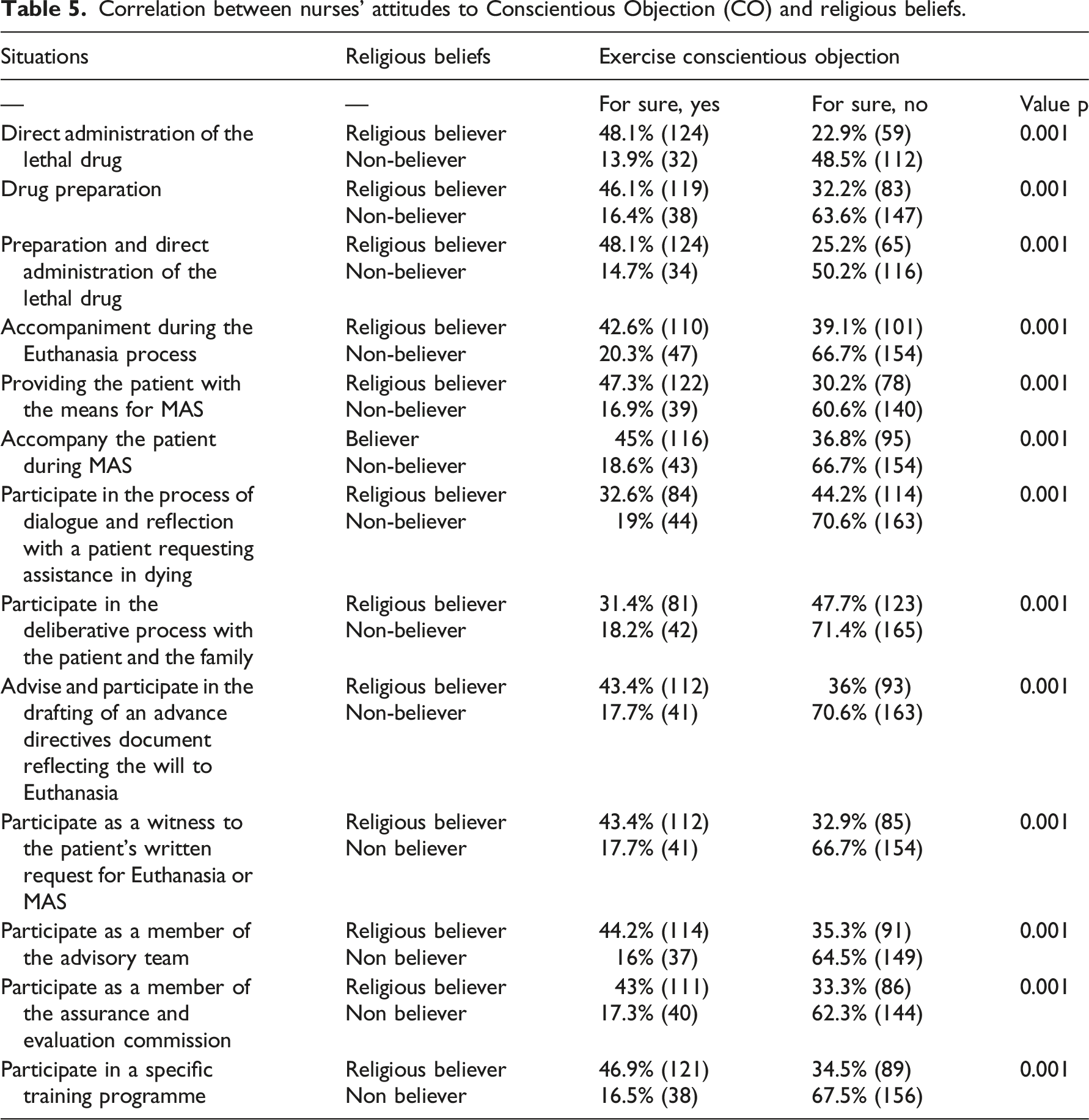
Finally, the greatest differences between variables were found with respect to religious beliefs.
The nurses from Madrid who participated in the study and reported being religious believers were more knowledgeable about the right to exercise CO to Euthanasia requests (85.7%) than non-believers (65.8%), p < 0.001.
Correlation between nurses’ attitudes to Conscientious Objection (CO) and religious beliefs.
Discussion
Few studies29–35 have been carried out in Spain in relation to Euthanasia and MAS in healthcare professionals, possibly because it is a practice that until now has been illegal.36,37 However, like ours, most of them believed that the debate on Euthanasia and MAS was a social debate and not only a clinical or political one. They also agreed that the main reason for requesting Euthanasia was loss of complete physical autonomy and personal freedom. These results coincide with the reports published by the Canadian 38 and Belgian 39 GECs, which show that the main reason for requesting assistance in dying is loss of autonomy.
Our research shows that the nurses from Madrid who participated in the study coincide with the doctors and nurses of the country in a position in favour of regulating both Euthanasia and MAS, as well as the mainly positive attitude towards their regulation at an international level. 36
With regard to doctors, the first study carried out in Spain to specifically address this issue was conducted by the Bizkaya Medical Association 29 (Basque Country) in 2018, showing a majority position in favour of both Euthanasia (82.8%) and MAS (72.4%). This was followed in 2019 by four more Spanish Autonomous Regions with very similar results: Tarragona 30 (91% Euthanasia, 84% MAS), Las Palmas 31 (81.9% Euthanasia, 68.5% MAS) and Madrid 32 (86.49% Euthanasia).
In nursing, a study carried out in 2012 by Tamayo 33 et al. in Andalusia showed that 70% of nurses surveyed were in favour of regulating Euthanasia compared to 65% of regulating MAS. In 2014 a study 34 of primary care nurses in Asturias showed that 87.75% were in favour of regulating Euthanasia compared to 62.06% for MAS, finding that religious beliefs influenced all the questions raised in their research, as in our study.
Finally, in 2019, the Official College of Nurses of La Rioja 35 showed that 83.3% of nurses surveyed were in favour of the regulation of Euthanasia compared to 67.4% for MAS.
Regarding the application of Euthanasia, there are big differences between the opinion of doctors and Spanish nurses.
Thus, 48.6% of doctors in Bizkaya, 29 45% in Tarragona, 30 57.5% in Las Palmas 31 and 64.6% in Madrid, 32 considered that Euthanasia should only be applied by a doctor, compared to 42.3% of nurses in our study who said that it could be applied by any professional in the field of medicine and nursing, as did the nurses in La Rioja. 35
The fact is Spanish legislation 6 does not specify the professional who will carry out the practice; it only refers to it being carried out with the utmost care and professionalism on the part of healthcare professionals, both being supposedly included; which is one of the aspects that may generate the greatest controversy during its application. In this sense, defining the role of the professionals throughout the process, especially nurses, will be essential to identify when and how situations of Conscientious Objection may arise, the percentage of professionals who would exercise it being initially low, both in doctors29–32 (27–37%) and nurses33–35 (26–35%).
Moreover, this present study is the only one that analyses the different situations contemplated by the Spanish law, and therefore the situations in which professionals would declare Conscientious Objection. Knowledge of these situations is key to designing the necessary procedures to safeguard both the right of professionals to exercise Conscientious Objection and the right of patients to receive the requested aid in dying.
As for requests of aid in dying, a study 33 conducted in 2012 in Spain showed that 21.4% of the Andalusian nurses surveyed had had Euthanasia requests, compared to 7.8% for MAS. Another study 40 conducted in 2015 in Belgium also showed that more than half of the participating nurses had been directly confronted with a request for Euthanasia, with more than 80% pointing out the need to allow such requests to be analysed, not only by doctors, considering this way the role of the nurse to be crucial in dealing with them. In this regard, 46% of the nurses who participated in a 2016 study in the Netherlands 41 indicated that the patient is more likely to make a request for Euthanasia to a nurse than to a doctor, claiming this way the need for nurses to be involved in dealing with such a requests and to participate in the decision-making process, as this is not legally recognised for nurses in the Netherlands. Following these lines, in our research most of the nurses surveyed in Madrid would also be willing to participate in the process of reflection and deliberation with the patient when asked for help in dying.
In relation to direct involvement in the implementation of Euthanasia or MAS, there is a growing trend of favourable positioning towards the practice of aid in dying both nationally and internationally. A study carried out in Finland 42 in 2017 showed that 74.7% of the nurses surveyed had a positive attitude towards applying Euthanasia if it were regulated, as did the study carried out in Canada 43 which also showed a favourable stance of 67.3%. In Spain, the predisposition to participate in the application of Euthanasia and MAS in 2012 33 was 54% and 47.3%, respectively, with results very similar to those found almost 10 years later in our research. However, between both practices, the one that generates the highest percentage of Conscientious Objection is the preparation and direct administration of the drug (Euthanasia) as opposed to MAS. This coincides with the study by Zenz 44 et al., which showed that professionals were more willing to participate in MAS than in Euthanasia. On the other hand, it should be noted that Spain is the first European regulation that allows direct administration of the drug by the nurse, unlike Belgium, the Netherlands and Luxembourg, where only the responsible physician can legally do so; although in clinical practice there are situations in which they do also participate in this process.
A systematic review 37 conducted in 2021 on nurses' perceptions and attitudes towards euthanasia showed a number of factors associated with positioning for or against Euthanasia practices. The factors determining the negative attitude and/or lack of support were religion (like the results shown in our research to be one of the most conditioning factors), moral/ethical dilemmas, the role of the health professional’s gender and poor palliative care. In contrast, factors associated with a positive and/or supportive attitude to such practices were unbearable suffering or other distressing experiences of the patient, the legality of euthanasia and the patient's right to die, as were the results found in our research.
Other studies45,46 show that education, age (especially young people) and gender (men) may also influence favourable attitudes towards the provision of Euthanasia. However, in our study statistically significant differences with respect to gender were not found, but there were differences with respect to age. Our findings were, contrary to these publications, the older the age and the longer the work experience as a nurse, the better the attitudes towards Euthanasia; and also with training, with attitudes improving with postgraduate courses in bioethics and palliative care. In this respect, another study 40 shows the need to include specific training in the approach to requests for assistance in dying in order to provide a comprehensive approach, highlighting its inclusion in undergraduate training.
The limitations of this research include the fact that the type of sampling used may make extrapolation to other regions of Spain difficult, although studies have subsequently been carried out in other regions such as Teruel or the Balearic Islands using the same instrument that we developed, obtaining results very similar to those of our research.
Euthanasia and MAS pose a great challenge for nurses in their clinical practice.47,48 Nurses must be informed of the existing legislation, as well as receive the necessary in-depth training to enable them to adopt a position in accordance with their values and have professional guidelines that facilitate the identification of their role. To this end, as our research has shown, it will be key for nurses to participate in guiding and influencing the drafting of the law through the Professional Colleges.
In this sense, with the aim of participating in health policy and exercising representation and positioning in relation to an area in which the nursing profession is directly involved, based on the results obtained in our research, on 14th December 2020 we published a report 49 in which the different nurses’ perspectives for the approval of Euthanasia and MAS were gathered, from an ethical, social, deontological, legal and clinical approach. This report was sent to the government, to all parliamentary groups, along with dissemination to other organisations, the media and the public, with the aim of providing a series of recommendations; not only for legislation, but also for its appropriate implementation in clinical practice. Particular emphasis was placed on the inclusion of the participation of nurses throughout the dialogue process and not merely as specific or instrumental acts, the modification of the Penal Code exempting both doctors and nurses from liability (as initially it only included doctors) and the inclusion of nurses as members of the Guarantee and Evaluation Commissions (as initially it only included doctors and lawyers). It should be noted that some of the proposed recommendations were included in the final regulatory text, 1 such as the modification of the Penal Code and the inclusion of nurses in the GECs.
Following the approval of the law on 24th March 2021, this research team published various documents50,51 on the nurse’s role and CO, in order to bring the regulatory text closer to the nurses’ position in Madrid. An online information day was also held for both nurses and the general public.
Finally, before its entry into force in May 2021, a new document 52 was drafted, following a proposal to do so by the body responsible for the Department of Health of the Community of Madrid, to provide a series of recommendations for the correct application of the law. It emphasised the importance of defining the healthcare team involved in the process, in particular clearly detailing the functions of the different professionals (including the role of the nurse in charge), as well as the need to establish a series of profiles and requirements for the composition of the GECs; and models for how to exercise Conscientious Objection. It should also be noted that some of these recommendations have been included in the implementation of the law in the autonomous region.
Since the law came into force in Spain, it has been possible to observe the great variability in its application between the different autonomous regions, especially in the lack of clarity in the roles of professionals. Also, further research is needed to explore the impact on the emotional well-being of nurses, to identify their roles and to determine the support they need when they participate in the provision of assistance in dying.
Conclusion
Based on the results obtained, the following conclusions can be drawn:
Firstly, the nurses in Madrid who participated in the study are mostly in favour of the regulation of both Euthanasia and MAS, especially those over 50 years of age, with more than 30 years of work experience, who work in the public sector and are not religious believers.
Secondly, attitudes towards the legislative aspects show a greater consensus on the involvement of the deliberative process, joint information, and accompaniment during the provision of aid in dying, than on the direct preparation and administration of the drug; especially among professionals with postgraduate training in palliative care and bioethics, and non-believers.
Thirdly, there is greater agreement on nurses’ involvement in MAS than in Euthanasia, although the nurses from Madrid who participated in the study consider that it can be applied by both a doctor and a nurse.
Finally, there is a low percentage of Conscientious Objection, being related to age, years of work experience, model of care and above all religious beliefs; the key being the protocolisation of the procedure to safeguard both the ideological freedom of the professional, and the legally established patient’s right to this service.
Footnotes
Acknowledgements
The authors thank all the nurses who have completed the questionnaire.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.