
Abstract
Background
The increasing prevalence of moral distress in the stressful environment of the intensive care unit (ICU) provides grounds for nursing error and endangers patients’ health, safety, and even life. One of the most important reasons for this distress is the treatment team’s second victim syndrome (SVS), especially nurses, following errors in the treatment system.
Objectives
The present study aimed to determine the relationship between moral distress and SVS in ICUs.
Research design
This cross-sectional study involved a sample size of 96 ICU nurses working in hospitals affiliated with Tehran University of Medical Sciences, Iran, in the 2021–2022 period, who were selected via a simple random sampling method. Data were collected using the Demographic Questionnaire, the second victim experience and support tool (SVEST) and Moral Distress Scale-Revised (MDS-R). Descriptive statistics (percentage, frequency, mean, and SD) and analytical tests (Spearman correlation coefficient test, independent t-test, and ANOVA) were employed for data analysis.
Participants and research context
This study used a sample size of 96 intensive care unit nurses working in hospitals affiliated to Tehran University of Medical Sciences selected by simple random sampling.
Ethical considerations
The study obtained research ethics approval, and all participants were informed of the voluntary and anonymous nature of their participation.
Findings
The results showed that 59.4% of nurses suffered a low level of moral distress, and 40.6% suffered from a moderate level of moral distress. The SVS score of 86.5% of the nurses was moderate. There was no significant and direct correlation between moral distress and SVS in nurses; however, there was a significant and inverse correlation between the moral distress intensity and SVS (p = 0.011).
Conclusion
Despite no significant correlation between moral distress and SVS, these variables were at moderate levels. Accordingly, it is suggested to provide a proper ground for expressing morally stressful situations, counseling and training strategies to deal with moral distress, creating support resources for those suffering from SVS, and implementing empowerment programs.
Introduction
The environment of the intensive care unit (ICU) can lead to high levels of stress and moral distress due to high hospitalization and mortality of critically ill patients and numerous ethical challenges and decisions. 1 Moral distress is a complex phenomenon often experienced by ICU nurses. 2 Factors such as keeping pace with technological advances in performance, high workload, and uncertainty about the end-of-life of critically ill patients in ICUs can lead to ethical conflicts among nurses working in the ward, resulting in moral distress. 3 In addition to causing physical and psychological symptoms (anxiety, depression, insomnia and headaches, and nightmares), moral distress can increase stress, burnout, and dissatisfaction with the profession in nurses. 4 This condition is one of the things that can reduce the quality of care, the lack of safe care of the patient, and the ability of people to cope with the existing conditions, followed by absenteeism and leaving the profession. 5 Many factors lead to moral distress, but one of the reasons that can cause moral distress in ICU providers is the second victim syndrome (SVS). 6
The second victim syndrome (SVS) is defined as the healthcare professionals who commit an error and are traumatized by the event manifesting psychological (shame, guilt, anxiety, grief, and depression), cognitive (compassion, dissatisfaction, burnout, and secondary traumatic stress), and/or physical reactions that have a personal negative impact. Generally, the healthcare system has not adequately communicated or implemented effective support mechanisms to address the personal, social, spiritual, and occupational crises experienced by second victims. Although the first victims of medical malpractice are patients and their families harmed, the second victims are nurses who suffer from complex psychological trauma. In addition to the moral distress experienced in caring for a critically ill patient in the ICU, the experience of SVS as a post-traumatic stress disorder (PTSD) impairs the mental health of service providers.7,8 The impact of irreparable mistakes that cause harm to the patient in private life, interaction with professional colleagues, and in the social life of nurses is quite evident. Immediately after identifying an error, intensive care unit nurses often experience stress-related psychological reactions to grief, fear, anger, and shame.9,10 Secondary victims also immediately terrified, manifested by disbelief, shock, high blood pressure and heart rate, muscle tension, rapid breathing, severe sadness, loss of appetite, and difficulty concentrating.
Background
The second victim, while waiting for the error to be investigated, often fears losing his or her job and the financial consequences of unemployment and the fines received by colleagues, their families, and the sick family as incompetence or carelessness, loss of respect for colleagues, loss of professional license, or separation from colleagues and their organization occur. 9 In the first weeks after committing errors, second victims often experience fear of returning to work, loss of confidence, regret, depression, irritability, nervousness, guilt, anxiety, embarrassment, anxiety, humiliation, longing for compensation, frustration, and excessive monitoring. In the months that follow, PTSD symptoms appear as an inability to process successfully, feelings of fear, sadness, and shame. This traumatic event leads to insomnia, other sleep disorders, suicidal ideation, self-harm, and lack of internal security. Grave errors, moreover, can also lead to revoking nursing care licenses or leaving the profession. 9 Moral distress is a prominent issue that harms the performance of ICU nurses. In the meantime, inadequate management and treatment system mechanisms, suffering from no proper training, guidance, and support of the nursing profession at this high level of healthcare, which requires sufficient experience, turn the nurses who caused harm to the patient into second victims. This second victim, if not supported by the healthcare system with training and counseling, the third victim will undoubtedly be the healthcare system itself. 11 Therefore, the present study was conducted to determine the relationship between the SVS and moral distress in ICU nurses so that by identifying this relationship, future studies may provide a solution to reduce it and promote safe patient healthcare.
Methods
Design
This cross-sectional study was conducted on the nurses working in the ICUs of hospitals affiliated with Tehran University of Medical Sciences, Iran, during the 2021–2022 period, who were selected via a simple random sampling method. The region that Tehran University of Medical Sciences, directly through the health and treatment networks of Islamshahr and Ray and South Health Center, is in charge of supervising and providing health services to its people, includes municipal areas 16, 17, 19, and 20. It also includes areas 3 and 4 of the 15th district of Tehran and the cities of Islamshahr and Ray, which are mainly middle and deprived areas of Tehran, with high population density.
Participants
The study population was all nurses working in the intensive care unit. In this study, a sample size of 95% confidence was obtained between the SVS and the moral distress of 96 nurses. Inclusion criteria consisted of having informed consent forms to participate in the study, having at least 1 year of work experience in ICUs, and committing at least one nursing error (based on self-declaration forms). Exclusion criteria were withdrawing from participation in the research and not completing at least 70% of the questionnaire items. The participants were selected through a simple random sampling method using a random number table.
Data collection
To collect the data, the Demographic Questionnaire, the second victim experience and support tool (SVEST) (Burlison et al. 2017), and Moral Distress Scale-Revised (MDS-R) (Hamric et al. 2012) were employed. The Demographic Questionnaire contains items about nurses’ demographic characteristics, including age, gender, marital status, degree of education, place of work, duration of employment, place of employment, type of shift work, organizational position, history of nursing error. The SVEST consists of three parts and 36 items: The first part assesses the medical staff’s experiences of unintentional patient safety incidents. These incidences are not necessarily errors (e.g., incorrect injection of blood or medicine, failure to perform a particular procedure, and incorrect device adjustment). Also, they do not necessarily include the circumstances that led to the injury but the unintentional incidences that did not even reach patients and were prevented or eliminated before they occurred. In the second part, the (non)support of colleagues and organizations for the healthcare providers causing the injury to patients is examined. In the third part of this questionnaire, the healthcare providers’ willingness to obtain different types of support from their organizations in case of unintentional patient safety incidents is measured. Also, two significant consequences of unintentional patient safety incidences for medical personnel (absence from work and tendency to leave the job) are measured by four questionnaire items. This instrument measures the items based on a 5-point Likert scale (strongly disagree, disagree, neither agree nor disagree, agree, and strongly agree). The reliability of the SVEST in Iran was assessed psychometrically by Bagheri et al as 0.79. 12 The MDS-R consists of 21 items rated based on a 5-point Likert scale. A psychometric test in Sharifinia et al. measured its reliability on the Iranian population as 0.71. 13
Data analysis
Data were collected using questionnaires and analyzed via Statistical Package for Social Science (SPSS) version 16.0. Pearson correlation coefficient was employed to examine the correlation between the SVS and moral distress.
Ethical Consideration
This study was conducted after the approval of Tehran University of Medical Sciences and obtaining the code of ethics (IR.TUMS.MEDICINE.REC.1400.751). At the beginning of the study, the objectives of the study and the working method were explained to the participants, and written informed consent was obtained from all the participants. All participants were assured that their information would be kept confidential.
Findings
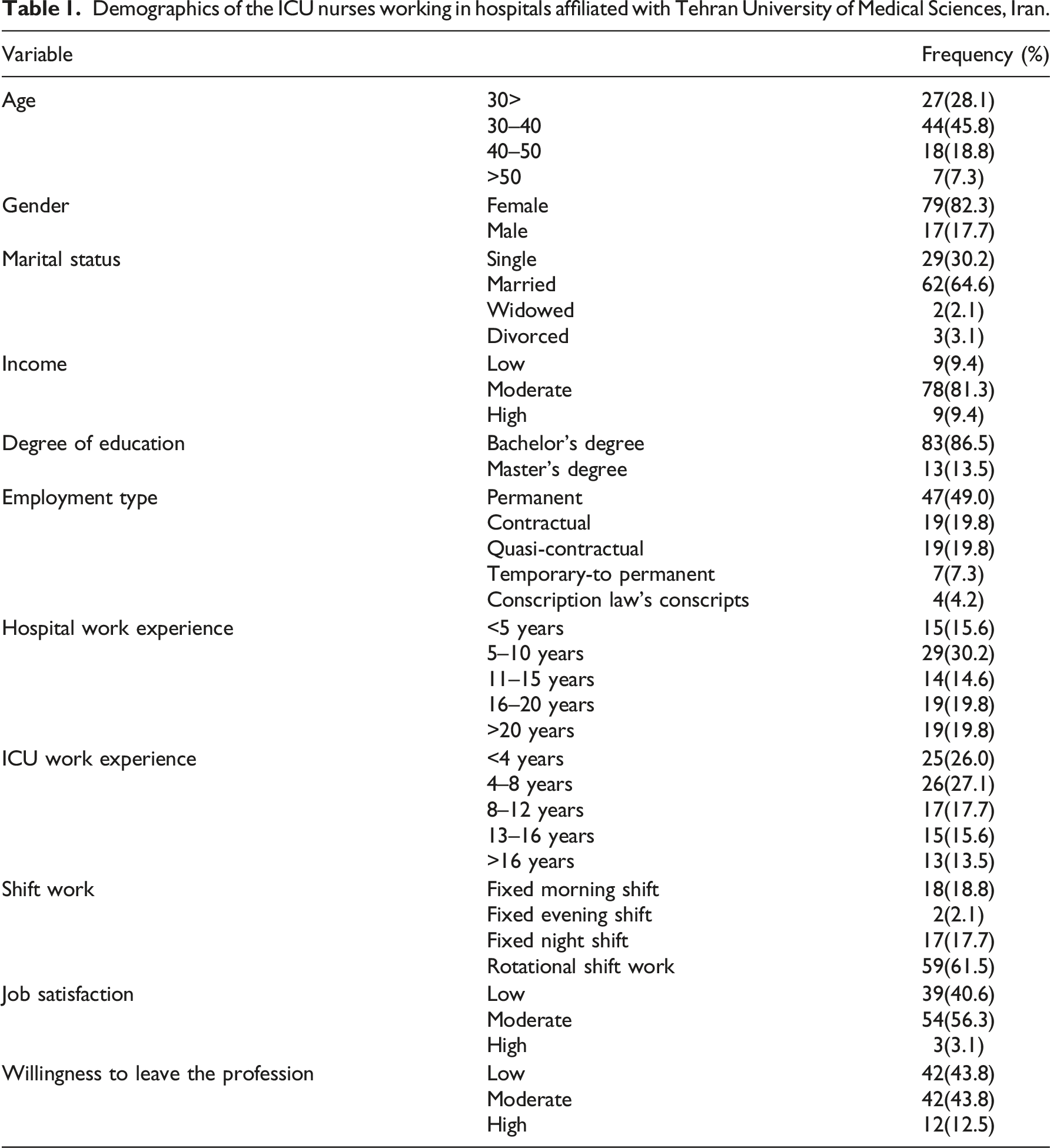
Demographics of the ICU nurses working in hospitals affiliated with Tehran University of Medical Sciences, Iran.
The findings showed that the mean ± SD of the age of the nurses’ moral distress was 68.31 ± 17.98, ranging from 38 to 124. Also, the nurses’ moral distress score classification showed that 59.4% of the scores were at the low level and 40.6% at the moderate level.
The mean ± SD of the moral distress frequency was 38.47 ± 6.91, ranging from 22 to 52. The moral distress frequency score classification showed that 72.9% of the scores were at the moderate level and 27.1% at the high level.
The mean ± SD of the moral distress intensity was 37.17 ± 6.13, ranging from 24 to 50. The moral distress intensity score classification showed that 79.2% of the scores were at the moderate level and 20.8% at the high level.
The mean ± SD of the nurses’ SVS was 121.94 ± 11.62, ranging from 78 to 147. The nurses’ SVS score classification showed that 2.1% of the scores were at the low level, 86.5% at the moderate level, and 11.5% at the high level.
Correlation between moral distress and its subscales with the SVS in the participants (nurses).
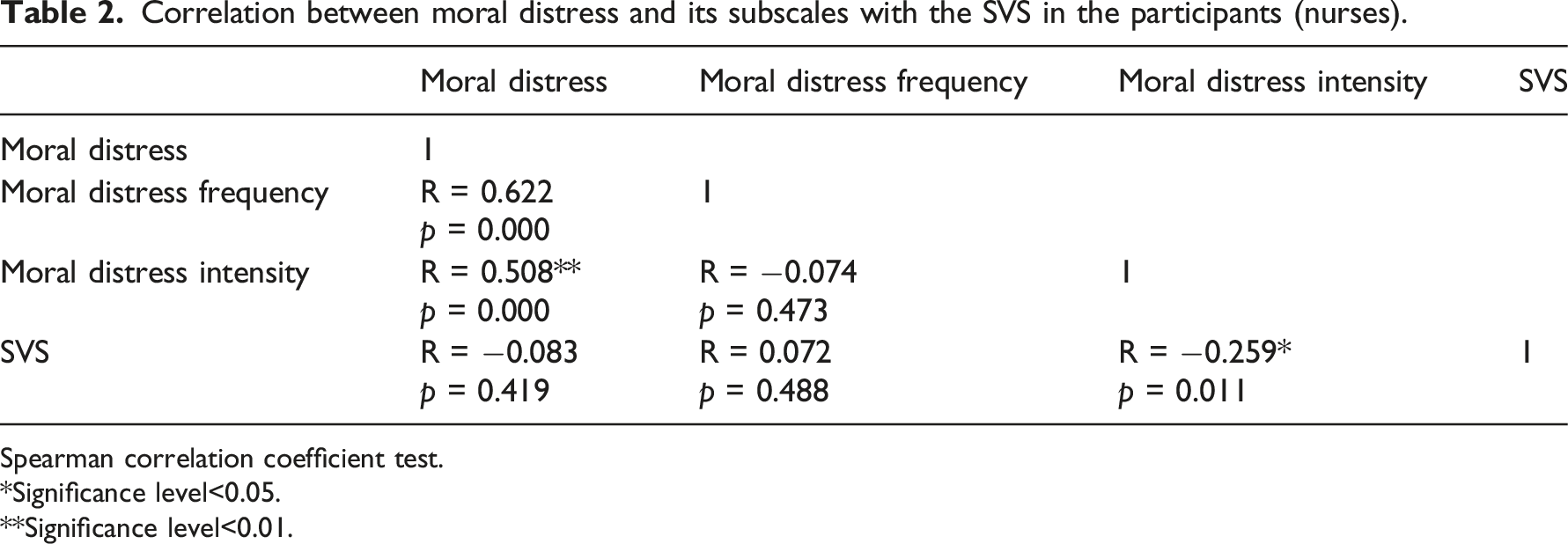
Spearman correlation coefficient test.
*Significance level<0.05.
**Significance level<0.01.
Moral distress and SVS in the ICU nurses by demographic characteristics.

Discussion
The present cross-sectional study aimed to determine the relationship between ICU nurses’ SVS and moral distress. The results showed that most nurses suffered from moderate moral distress frequency and severity. These findings are consistent with Mahdavi Fashtami et al., which showed that the mean ± SD of the moral distress frequency was 1.4 ± 0.58, the mean ± SD of the moral distress severity was 1.7 ± 0.92 out of 4, and its mean effect size was 4±2.38 out of 16. Also found in their study was that emergency nurses suffered moderate-level moral distress. 14 This difference between the two studies can be in the sample sizes, the employed scales, and the wards (emergency and ICU)—it seems that in ICUs and emergency departments, nurses experience more ethical decisions in caring for and treating patients in critical situations than physicians owing to physical work stress and severe psychological stress. Therefore, nurses’ exposure to these stressful conditions increases their moral distress frequency. ICUs have a high mortality rate due to the nature of the disease and the dire condition of patients, which increases the moral distress of nurses in such wards. Also, in E’tebari Asl et al, the ICU nurses’ moral distress mean ± SD was 108.25 ± 24.18. In their study, 118 ICU nurses in educational and medical centers affiliated with Ardabil University of Medical Sciences were surveyed using Corley’s 30-item Moral Distress Scale. Since the scale used in Etebari Asl et al was different from the scale used in the present study, the inconsistency of the results can be explained. 15 In Shafipour et al., the mean±SD of moral distress of nurses working in Mazandaran Burn Center was moderate as 105/65 ± 52/39. Their study was performed on 172 nurses of Mazandaran Burn Center using Corley’s 30-item Moral Distress Scale. The difference between the mean scores of Shafipour et al. and the present study can be in the larger sample size, the employed questionnaire type, and the nurses’ place of employment. 16
In addition, Berhie et al conducted a study on 423 nurses, showing that 83.7% of the nurses suffered from moral distress. Emmamally and Chiyangwa conducted a study on 74 ICU nurses using a 21-item questionnaire and indicated that the mean±SD of moral distress was 112.12 ± 73.21.17,18 These two studies were inconsistent with the results of the present study. It can be inferred that there is some moral distress in nursing and nurses face it daily. This confrontation occurs when a person cannot make the proper connection between his/her moral status and professional beliefs. In these cases, the nurses experience emotional reactions such as crying, anger, sadness, dizziness, nausea, or not doing her job correctly. Eventually, they suffer from a mental imbalance in dealing with morally sensitive situations. Sometimes these stresses are so severe that they do not allow them to behave appropriately. The only thing that remains for the nurses in such difficult conditions is a kind of burnout and job dissatisfaction.
The present study’s findings also showed that most nurses’ SVS scores were moderate. Huang et al. (2021) showed that approximately 2897 (45.26%) nurses were involved in at least one adverse complication that mainly caused psychological distress. They believed that supportive measures with highly high approval among second victims were the possibility of discussing emotional and moral issues, immediate intervention in PTSD, and a safe opportunity to help insights to prevent similar incidents in the future. 19 In general, these traumatic incidents have a high potential impact on the health of the treatment staff and the healthcare they provide. Understanding second victims’ traumatization and the widespread implementation of effective support programs is essential.
The present study’s findings showed no significant correlation between moral distress and SVS in nurses, but there was a significant and negative correlation between the subscale of moral distress severity and SVS. In other words, with the increase in moral distress scores in nurses, the SVS scores decreased. In this regard, the results of Quillivan et al. showed that investigating patient safety culture (non-punitive response to errors) was significantly associated with a reduction in psychological, physical, and professional dimensions of distress in the study of the SVS. 7 Also, Lee et al. (2019) indicated that it is essential to pay attention to the moral dimension in the face of second victims. 20
Mokhtari et al reported that mismanagement, cultural barriers, insufficient information, and legal barriers were the main obstacles to supporting nurses. For this reason, nurses’ training in the SVS and methods for managing the effects of this syndrome recommended support resources and legal issues. 21 Epstein et al stated that healthcare providers have a fundamental commitment to reducing and preventing care costs (such as moral distress and secondary traumatic stress) and strengthening a sense of importance to their staff. 22
Ethical societies that work well have robust support systems, inclusiveness, fairness, open communication, and cooperation and can protect their members. In case of second stress, they should avoid moral distress in their personnel by creating solid moral systems. In this regard, it can be said that the SVS is inevitable in some cases, and the consequences can cause problems for the medical staff, especially those who work in wards with critically ill patients. Healthcare providers have an ethical responsibility to provide and maintain a safe and healthy work environment.
Moral distress is a significant concept in nursing and especially in ICUs. To reduce moral distress in nurses, nursing managers should focus on organizational processes and resources and attempt to reduce the moral distress that leads to nurses’ burnout, frustration, and resignation by reviewing problems and approving solutions in the ethics committee. Furthermore, non-punitive response to errors may reduce the adverse effects of participating in patient safety incidents by encouraging supportive interactions.
Moreover, the perception of distress associated with the SVS may be less severe when a non-punitive response to errors characterizes hospital cultures. Reducing punitive responses to error and encouraging co-workers, supervisors, and organizational interactions may be helpful strategies for managing the severity of SVS experiences, and managers were not responsible for supporting nurses. Since managers are at the center of recognizing and reducing systemic issues, poor management can prevent supporting nurses. Healthcare management is a critical issue in supporting nurses because it plays an essential role in planning the workforce, providing adequate equipment, performing needs assessments, and enforcing supportive laws. Managers can support second victims by identifying organizational errors and other threats that limit their consequences.7,20,22
As a result, moral distress decreases when the necessary support is provided to nurses and all medical staff in the face of medical errors. To this end, it is suggested to provide a proper context for expressing morally stressful situations, counseling and training strategies to deal with moral distress, and creating resources to support second victims and implement empowerment programs. Because the study was performed during the COVID-19 pandemic, the nurses might also be affected by the conditions. Therefore, it is recommended to conduct a study after the COVID-19 pandemic and even conduct a study in this field in nurses working in the COVID-19-specific ICUs. In this study, the relationship between the factors related to the work environment and the main variables of the study was not investigated; therefore, prospective studies are recommended to investigate the factors related to the work environment that may lead to moral distress and symptoms of psychological distress, including secondary victim syndrome. Also, both qualitative and quantitative studies, exploring experiences of moral distress, considering gender inequalities and power relations in healthcare systems, or even the adaptation model in nursing, may provide valuable data.
Conclusion
The results of the research showed that there was no significant correlation between moral distress and SVS in nurses, but there was an inverse significant relationship between the severity of moral distress and SVS in nurses. Therefore, it is recommended that hospital managers, especially nursing managers, create a suitable environment for expressing the morally stressful situations of nurses in the face of SVS and also provide counseling and training programs for dealing with moral distress.
Footnotes
Acknowledgments
We would like to thank the Vice Chancellor for Research of Tehran University of Medical Sciences. We are also grateful to all the nurses who participated in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study is the result of a research project approved by Tehran University of Medical Sciences with the code IR.TUMS.MEDICINE.REC.1400.751.