
Abstract
Background
Speaking up to safeguard patients is a crucial ethical and moral obligation for nurses, but it is also a difficult and potentially dangerous component of nursing work. Health advocacy is gaining impetus in the medical literature, despite being hampered by barriers resulting in many nurses in Ghana remaining mute when faced with advocacy-required situations. We explored situations that thwart nurses from performing their health advocacy role.
Research question
What would cause nurses to take no action when they witness situations that require them to act as health advocates for their clients or communities?
Research Design
An inductive, descriptive qualitative design was used to collect and analyse data on barriers that prevent nurses from practising their health advocacy role in Ghana. Individual one-on-one in-depth interviews were conducted using a semi-structured interview guide. The data were analysed using qualitative content analysis.
Participants and research context
Twenty-four professional nurses and midwives registered with the Nursing and Midwifery Council were recruited from three regional hospitals in Ghana. These public hospitals were chosen from the upper, middle and coastal regions.
Ethical considerations
The UKZN Ethics Review Committee in South Africa and the GHS Ethics Review Committee in Ghana both gave their approval for this study.
Findings
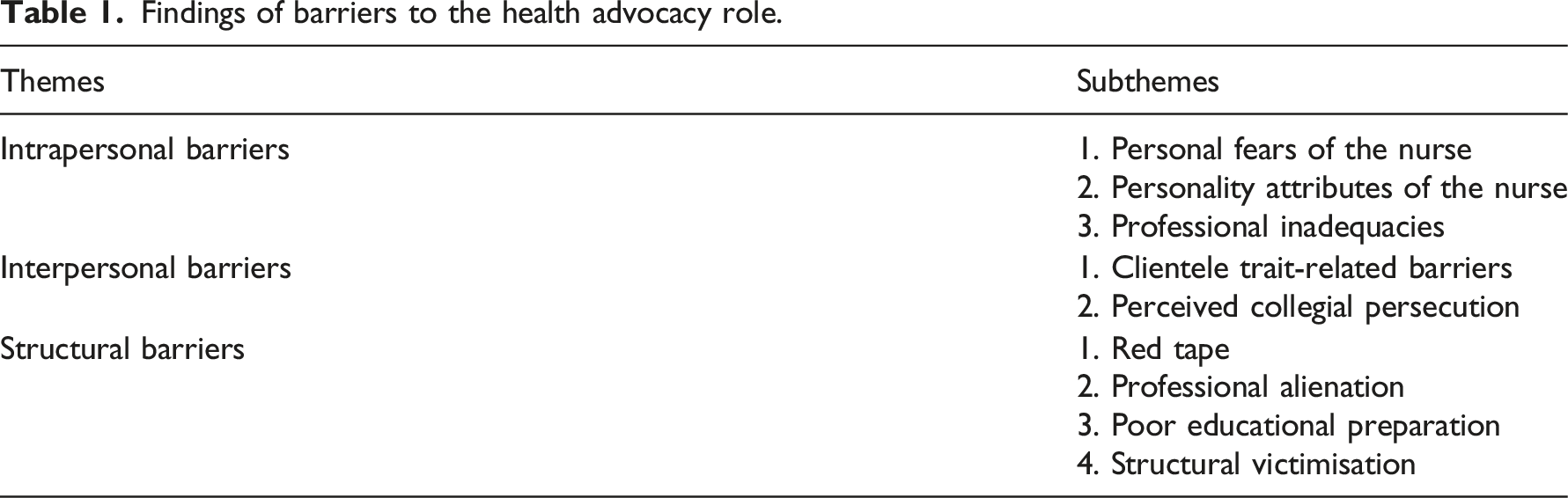
Intrapersonal barriers, interpersonal barriers, and structural barriers emerged as major obstacles that nurses experience when performing their health advocacy role.
Conclusions
Barriers to health advocacy have undermined nurses' ability to function as health advocates and are preventing them from utilising their health advocacy position in nursing practise. Giving nursing students positive role models in the classroom and in the clinic can help them become more effective health advocates.
Introduction
Health advocacy is the act and art of mediating, negotiating, and speaking out to protect the vulnerable and empower the disadvantaged and less privileged about their health. There are contextual barriers to health advocacy, and some nurses view the consequences of advocating for health as a career dilemma, 1 while others perceive it as risk-taking that may lead to castigation. There are nurses who are deontologically focused and are inherently motivated and justified by the ethics and duties of the profession to advocate, 2 but others are consequentialists who consider advocacy in terms of personal or organisational consequences. 3 These barriers prevent nurses from advocating and may lead to perpetuating health disparities and inequities in developing countries where health systems are fractured, 4 leaving clients with little or no voice for assistance. Nurses are in a better position to advocate, but due to barriers that range from personal to structural, they are prevented from being the voices they are meant to be. Our study therefore identified barriers preventing nurses in Ghana from performing their health advocacy role.
Background
Terms such as nursing advocacy,5–7 social advocacy,8,9 patient advocacy10,11 and health advocacy12,13 are but few of the usage of this phrase advocacy in health. Multi-concept usage of the term “advocacy” in health is thwarting the adoption and may create misconceptions associated with the use of this concept of health advocacy.
While health is defined as a state of balance, an equilibrium that an individual has established within and between himself and his social and physical environment, 14 advocacy is thought of as the act of pleading for, supporting, urging by argument, and recommending publicly. 15 Health advocacy is therefore conceived as speaking out on behalf of a particular issue, idea or person regarding health. 16 The concept of health advocacy incorporates patient advocacy, nursing advocacy, and social advocacy because these terms have a direct or indirect link to the concept, health.
The advocacy work of health professionals, especially nurses, goes back several decades. Over the centuries, nurses have advocated for people and communities in need. 17 For instance, Florence Nightingale pursued environmental health advocacy and health reforms, particularly for British soldiers during the Crimean War; 18 Lillian Wald advocated for home health nursing programs, the improvement of child labour practices, and workplace protections in the United States of America; 19 and Margaret Sanger fought for access to birth-control information and services for vulnerable and underserved populations in the United States. 17 These nurses did not only advocate for the vulnerable populations that they worked with (known as nursing advocacy), but they also pushed for policy changes at the health system level (known as social advocacy). The circumstances under which these nurses worked as pioneers were best termed as health advocacy as they mediated, negotiated and literally fought for the rights of the public.12,13 These circumstances that made the nurse health advocates mediate and negotiate have worsened today. In most developing countries, including Ghana, where the healthcare system is fractured 12 and under tremendous underfunding, nurses are required as health advocates for health policy changes. However, most nurses have remained silent due to barriers. 20
Advocating on behalf of clients requires nurses to be knowledgeable about their health advocacy role and the barriers associated with advocating for clients. Mardell 21 warned about these barriers, stating that health advocacy may predispose the nurse to conflict with their medical colleagues and with the management of the organisation which can ultimately lead to the loss of a job. So, nurses willing to function as advocates are bound to experience the chilling effect of threat of retaliation and loss of professional and economic security. 22 But, ‘shying’ away from health advocacy is argued as comparable to medical negligence. 23
Although some nurses know and understand their role as health advocates, most studies show that advocating in the health environment is complex and is a controversial and risky component of nursing practice. 24 The reluctance of nurses to engage in advocacy has been reported in some developing countries. 24 Barriers such as lack of advocacy training; failure to strategically frame advocacy issues; lack of organisational support for health employees to pursue advocacy; unwillingness on the part of health organisations to engage in public controversy; insufficient data; lack of interdisciplinary collaboration and lack of policy analysis capacity in the health sector have been reported as reasons nurses are unable to perform their health advocacy role.25–27
In Iran, a study conducted to identify barriers to advocacy, reported powerlessness, lack of law and a Code of Ethics, lack of support for nurses and physicians as leaders, time constraints forcing nursing to revise work patterns to complete many tasks in a limited time, and limited communication skills as barriers in health advocacy. 24 Other studies in the United Kingdom and the United States of America have reported loyalty to peers and lack of motivation as barriers to the nurses’ practice of the health advocacy role. 28
In Ghana, a study conducted on advocacy characteristics reported that nurses’ states of fatigue and frustration were hampering their performance in the health advocacy role. 29 Similarly, reports from the United States of America suggest stress, fatigue and depression to be associated with health advocacy role performance. 30 These barriers apart, some nurses view the consequences of health advocacy as a career dilemma, 31 while others perceive it as risk-taking that may lead to castigation. There are nurses that are deontologically focused and are inherently motivated and justified by ethics and duties of the profession to advocate, 32 but others are consequentialists who consider advocacy in terms of personal or organisational consequences. 33 Effective advocacy is sometimes conceived to be associated with feelings of frustration, anger and disruption of peer relationships, with some health advocates being labelled as disruptive. 27
Some of these barriers may also result from inadequate advocacy preparation during training. According to Poulton and Rose, 34 the health advocate role is considered among the least relevant to clinical practice by educators and learners and among the most challenging to teach and assess. The authors reported that learners feel their educational needs are not being met in this area and that there is limited published material on the subject, a lack of clarity within the role, insufficient explicit role modelling in practice and a lack of a gold standard for assessment. 34 These are just some of the barriers that are justified in the literature as reasons why nurses do not perform their health advocacy roles. From the literature, barriers to the health advocacy role appear to be contextual. As such, the current study seeks to explore and describe barriers to nurses using their health advocacy role in nursing practice in Ghana.
Methods
Design
A qualitative inductive descriptive design by Creswell and Poth 35 was used to gather and analyse qualitative data on barriers that prevent nurses in Ghana from utilising their health advocacy role in nursing practice. It was determined that a descriptive design was the most appropriate way to allow Ghanaian nurses to share their perspectives on the barriers that prevent them from fulfilling their professional and ethical responsibilities as health advocates. A qualitative descriptive study was used because it could give more detailed information about the problems that were found.
Study setting
To ensure cultural diversity in both the opinions of the nurses and the outcomes, the research was conducted in three Ghanaian regional hospitals that were chosen purposively. These hospitals serve as referral, research, and teaching facilities for nurses and other health professionals. These hospitals were chosen from various geographical locations throughout Ghana’s 16 regions, with one hospital from each of the upper, middle and coastal sectors.
Participants and sampling
A sample of 24 participants, seven male and 17 female professional nurses, were interviewed. Their level of education ranged from a Diploma in Nursing to a PhD level. The age of the participants ranged from 31 to 51 years. Their years of clinical nursing experience ranged between five and 15 years.
Purposive sampling was used to sample the 24 nurses. During the initial stages of the data collection, we recruited professional nurses who met the inclusion criteria in each of the regional hospitals. These nurses were recruited based on their previous involvement in the health advocacy role. The size of the sample was based on what Morse 36 called the ‘data saturation principle’. This means that sampling stopped when no new information was found.
Data collection
Data collection and data analysis were conducted concurrently. The individual interviews were conducted using a semi-structured interview guide, which was developed by the researchers according to the objectives of the study. The following research questions facilitated this interview: (1) what caused you to take no action when you witnessed actions that required you to act as a health advocate for your client or community? (2) What, in your opinion, would cause a nurse to take no action on behalf of her patients or community when health disparities are observed? Probes were generated based on the answers of the participants. For instance, ‘Others mentioned red tape as a barrier; what is your opinion?’ Using the semi-structured interview approach mentioned allowed for in-depth probing while permitting the interviewer to keep the interview within the parameters outlined out by the objective of the study. The interviews were conducted by the first author in English, the formal communication language in healthcare in Ghana. This also assisted in the transcription and analysis of data. The interviews were audio-recorded, and field notes were made during the interviews as part of data collection. Each interview was carried out in the nurses’ office and lasted between 50 and 90 min.
Data analysis
Using the qualitative content analysis approach by Graneheim and Lundman, 37 the transcripts were analysed. This approach involves searching for both concrete and abstract patterns in the different ways the data from the participants is the same and different. 37
The interview transcripts were read through by both authors and compared with the recorded interviews. The first author again read through the interviews several times to obtain a sense of the whole in order to grasp the unit of analysis. When a sense of the whole had emerged, meaning units, that is, statements that uncovered something related to the aim, were highlighted, detached from the text, and pasted into a separate MS Word document. Then, each meaning unit was summed up and given a code, which was a short description of what it meant.
Before abstracting the subthemes into themes, the authors discussed the variations on them by moving back and forth between the parts. Then, the authors discussed the content of the derived codes and grouped them into themes and identified subthemes based on the relationship between their similarities and differences. Based on Graneheim and Lundman 37 approach of abstraction of subthemes and themes, three main themes emerged, with nine total subthemes.
Ethical considerations
This study was approved by the University of KwaZulu Natal (UKZN) Ethics Review Committee in South Africa and the Ghana Health Services (GHS) Ethics Review Committee in Ghana, with approval numbers HSS/0289/018D and GHS-ERC 007/05/18, respectively. These are research ethics committees; however, permission letters were also obtained from data collection sites. Participation was voluntary and participants’ rights were ensured during this study. In a meeting organised with the assistance of the administrator of nursing services, the selected participants were given the information sheet, and those who agreed to participate were recruited and asked to sign the informed consent forms before interviews. During and after collecting data, the study adhered to the principles of anonymity and confidentiality.
Rigour
To establish trustworthiness, member checking and validation were conducted by returning to 12 of the participants and allowing them to read their interview transcripts. For confirmability, the co-author, an expert in qualitative content analysis, evaluated and confirmed the codes derived from the raw data. Precise data, including field notes, was maintained to facilitate an audit trail that details the decisions taken throughout the research process. The audit trail also gives a justification for the researchers’ methodology and interpretive judgement, which may aid in transferability. To assure dependability, qualitative content analysis and processes were applied accurately.
Findings
Findings of barriers to the health advocacy role.
Parts of this article in a draft form are in preprint. 38
Intrapersonal barriers
Intrapersonal barriers refer to the inherent characteristics of the individual that impede the nurse from fulfilling the function of health advocate. The three subthemes making up this theme were the professional nurse’s personality attributes, the professional nurse’s fears, and professional inadequacies.
For professional nurses' fears, participants reported fears of real and/or perceived punishment for using health advocacy roles. This real or perceived fear hindered them from practising their health advocacy role. Some cited fear of being labelled as ‘knowing too much’, fear of getting in trouble with superiors or the organisation, and fear of being victimised as barriers to performing their health advocacy role.
“They have labelled some of us as being too knowing because we speak out for our clients” (PN02, female).
“I am not able to speak for my clients. I wouldn’t speak out. I fear getting into trouble because I have been labelled by my superiors” (PN15, female).
“Well, if it is a very sensitive issue, I might not be bold enough to come out because I fear that people will lambaste or victimise me. I have been victimised before because I spoke out for a client that was treated unjustly” (PN23, male).
Some personality attributes of the professional nurses also prevented them from practising their health advocacy role. These are innate traits of nurses that prevent them from performing the health advocacy role. Being timid, being unassertive, lack of boldness and lack of bravery were discovered as reasons most nurses did not perform the health advocacy role as demonstrated in the following extracts:
“Most of us are timid. We are not able to speak for our clients if we know it might go against a colleague or the facility. I will not speak out. I would prefer someone brave enough to speak up” (PN11, male).
“I don’t speak out because my boldness level is low. (laughs) I have seen nurses who spoke out to support clients and the outcome was not what we expected. The facility side-lined him until he went on transfer” (PN23, male).
Inadequacies that are professionally related were noted as barriers that prevented some nurses from practising their health advocacy role. Lack of experience and professional incompetence were suggestive in some instances when some nurses did not perform the health advocacy role.
“I don’t try to speak out because my confidence and my knowledge level are just to do what I have been assigned. Professionally, if I have these two things, I can advocate very well” (PN01, male).
“I am limited in what I can do as a professional.” “I have the desire to speak for my clients when their rights are violated, but I am limited in terms of experience” (PN16, female).
Interpersonal barriers
Relationships between the nurse and others, including patients and other health workers, were cited as challenging. Barriers stemming from clientele characteristics and the perception of collegial persecution were revealed as the primary factors preventing nurses from fulfilling their health advocacy responsibilities. As exemplified in the following excerpts, participants identified inconsiderate client behaviours, such as inattention to the nurse’s professional advice and ungratefulness for what the nurse does, as client trait-related barriers.
“Clients themselves are part of it. You will stand up for them, and at the end of the day, some of them will behave in a way that will make it difficult to advocate for them in the future” (PN16, female).
“I recall a child who was discharged from the ward and whose mother was unable to pay the bill. I advocated on her behalf, and when she returned home, we never saw her again, and when we tracked the address in the records, it was incorrect” (PN01, male).
“Some of the patients are ungrateful. I have spoken for them severally. I see they don’t appreciate it, so I don’t even have the zeal to do it for somebody else” (PN02, female).
Also recognised as behaviours of other professional colleagues that deter nurses from advocating is the perception of collegial persecution. As reflected in the comments that follow, the activities of collegial persecution were described as intimidation from other professionals, intimidation from senior colleagues, name-calling from colleagues and victimisation by colleagues.
“Our colleague nurses have intimidated us just because we stand up for client rights, especially if it is against another professional colleague” (PN01, male).
“They have given some of us names because we speak for the less privileged clients” (PN04, female).
“What I am saying is, as a nurse, I may know or would have seen that it is right to be a health advocate, but may not want any trouble, or want other people to sabotage me. So, I keep quiet to prevent victimisation from others, including my colleagues, and seniors” (PN22, male).
Structural barriers
The structural barriers are organisational and institutional issues that prevent nurses from practising their health advocacy role. Red tape, professional alienation, poor educational preparation and structural victimisation were discovered. Participants believe that red tape is an excessive and rigid conformity to redundant formal rules and processes within health organisations. They think that barriers come up when institutions have policies that don’t help and when they take too long to act on things that are brought up during advocacy.
“It’s the dysfunctional chain that we go through that impedes our desire to advocate” (PN11, male).
“Some policies in this institution are just not favourable for nurses to work as advocates” (PN19, female).
‘’Sometimes too we go to the authority because some of the things might involve policies or rules that are hard to break and can lead to unfair treatment of our clients, for instance, deposit before treatment” (PN19, female).
Professional alienation, an isolation and division that sidelines some nurses from their professional colleagues and prevents them from interacting with colleagues, was noted. The ‘keep quiet and obey syndrome’, professional snobbery and negative professional socialisation are barriers reported to have prevented nurses from advocating.
“You have to keep quiet and obey; when you step behind the nurse-in-charge to take any action, you may be in trouble” (PN11, male).
“We are not able to advocate because the seniors snub us if we try to suggest or initiate any action of advocacy” (PN18, female).
Inadequate educational preparation due to the absence of health advocacy in the nursing curriculum and educators’ failure to empower students to advocate during training was reported. Also, the inadequacy of the curriculum on health advocacy and inadequate instruction on student preparation on health advocacy from school were seen as barriers that prevented the nurses from advocating.
“The content in the curriculum did not adequately prepare us to be serious health advocates [or to advocate for health]” (PN23, male).
“I hold a view that our training from the nursing schools, particularly the nurses’ training [Diploma Certificate], most of the time, doesn’t empower us as health advocates” (PN14, female).
In addition to the poor educational preparation, the nurses reported an inadequate description of health advocacy in the curriculum and little attention paid to it by instructors as a barrier to its success. They stated that instead of tutors cultivating assertiveness during training, they would rather encourage timidity. Tutors prefer students to submit in all instances, without consideration of the situation.
“It starts with the training schools. In school, you don’t want to be seen as someone who speaks out or stands up for your rights, because all those that do that, the tutors will have their eyes on them and they will frustrate them with their grades” (PN20, male).
“There is something going on that you don’t like, but you can’t talk for fear that in the final exams they will fail you” (PN15, female).
“So sometimes we see problems as nurses and are unable to voice them because of the way we were trained at nursing school” (PN21, male).
Structural victimisation was reported as direct or indirect victimisation of the nurse, both at the training institutions and clinical facilities that hindered nurses from performing the health advocacy role. Participants noted that fear of punishment from the institution and fear of victimisation during training have culminated in their inability to perform the health advocacy role.
“We fear that the authorities will lambaste us or victimise us. So the victimisation is a hindrance to some of us " (PN23, male).
“The principal had to report him to XXX and every year he failed his exams." Every year he failed in his exams until about six years before he passed. The intimidation is real during training, so how can you speak out when you qualify?” (PN20, male).
Discussion
This qualitative study explored barriers to nurses using their health advocacy role in nursing practice. Participants talked about a number of barriers, from the nurses' own personalities to barriers caused by the way the system is set up. As a result, many nurses don’t speak up when they should. These findings are useful to both clinical and nursing education because they provide information on scenarios that inhibit nurses from speaking up to protect patients whose rights are violated by health facilities or health professionals.
To begin, our findings revealed that perceived or real fears of being labelled as knowing too much could hinder a nurse from doing the right thing in an environment. Fear of colleagues and superiors in nursing is hindering nurses from initiating and performing some professional roles. In Zimbabwe, a study reported that nurses’ under-reporting of the adverse effects of immunisation was found to be due to fear of their superiors. 39 Personality attributes such as timidity are barriers that prevent nurses from practising the health advocacy role in Ghana. This appears to have been reported more from the diploma-trained nurses, as they say the educators make them obey in all circumstances without consideration of the situation. Educators are encouraged to treat trainees as junior colleagues and allow more class discussions and student presentation to build their self-confidence. 40 The lack of courage and confidence of some nurses, which made them timid, prevented them from speaking out whenever issues of health advocacy came up. Others have reported that timidity makes nurses lack courage and boldness to initiate the health advocacy role on their own.24,41 Choosing students with the right character and constitution for modern nursing practice may be a challenge but will not only protect the public, but will also improve professionalism and contribute to the flourishing of individuals, families and communities. 42
In addition, our findings suggest professional inadequacies due to lack of experience, lack of current knowledge and practical experience in health advocacy. This intrapersonal barriers to nurses using their health advocacy role are reported in both Ghana and the United States of America.29,43 Also, professional inadequacies have been reported in the teaching field in a previous study by Lindqvist, Weurlander, 44 where newly qualified teachers reportedly felt professionally inadequate during emotional stress. Even as these do not come as a surprise that nurses in Ghana reportedly felt professionally insufficient when confronted with health advocacy issues, it suggests little exposure to health advocacy issues during their clinical sessions on training. An exposure to simulations and real clinical advocacy issues during training would arm and equip them with adequate knowledge on health advocacy in practice. 45
A study in Ghana by Dadzie, Aziato 29 reported that being empathetic, nurturing, ethical, assertive, persistent and compassionate are keys to advocating. This is contrary to what our participants reported, as they held that clients had to be considerate for nurses to advocate. Clients’ inconsiderate behaviours and lack of appreciation of what the nurses do for them were reported as barriers that prevent nurses from using their health advocacy role to assist their clients. Unlike the norm of thanking a patient after a procedure, it was reported that a nurse instead expects a thank you from the patient. This suggests that speaking out for a disadvantaged patient is misconceived as a favour rendered by the nurse and hence the expectation for appreciation.
Also, the current study discovered that fear of victimisation of nurses from their seniors, their colleagues and other health professionals were barriers preventing a lot of nurses from speaking out. The victimisation was reported to come in the form of rejection from colleagues who disapproved of nurses speaking out for clients. Our findings confirm previous studies that say health advocates are perceived in some situations by their colleagues as disruptive and stubborn.27,31 This reveals that even though health advocacy is a moral and ethical obligation, nurses would rather not advocate for their patients than be rejected by their colleagues. This notion leaves some nurses in a divided devotion as to who to offer their loyalty to.
Red tape, the excessive and rigid conformity to redundant formal rules within the health organisations, is hindering nurses from using their health advocacy role. The delays to receive response from management and the unfavourable institutional policies prevented some nurses from performing their health advocacy role in Ghana. Orderly and systematic management of issues in health institutions is necessary, but when it becomes rigid and excessive without consideration of the involvement of human lives, the repercussions these delays bring, retard progress and productivity. This supports previous studies where participants lamented that institutional policies and delays from management were blocking and frustrating nurses’ efforts to advocate.46,47
Structurally, red tape aside, professional alienation, professional snobbery and ‘nurses eating their young’ was reported. Junior nurses who were known to be vocal or to stand up on behalf of poor client care or poor working conditions were alienated by their colleagues and those in senior nursing management positions instead of standing together in solidarity. These demotivated nurses from performing the health advocacy role,48,49 and suggested poor professional solidarity observed in other health professionals who stand together to fight for their rights. Poor professional socialisation in nursing, identified by a participant as the ‘keep quiet and obey syndrome’ is to blame. The keep quit and obey syndrome is a cultural phenomenon. Most African cultures and traditions seem to promote the ‘keep quiet and obey syndrome’ in where the young are not expected to have a say but to obey and do whatever they are told. Participants viewed the keep quiet and obey as very frustrating leading to feelings of powerlessness and lack of enthusiasm to intervene on behalf of clients.24,25,29
Although professional alienation has been identified as a structural barrier to the practice of health advocacy in other countries,48,49 we found that it was entrenched in the cultural socialisation of children through the ‘keep quiet and obey syndrome’. This cultural socialisation behaviour thrives in the nursing profession in Ghana for many reasons including, the elder is always right, children do not contribute when elders are talking, and children who give an opinion contrary to that of the elder are considered disobedient.
As reported by Poulton and Rose 34 many of our participants stated that health advocacy is not taught or is poorly taught in most nursing schools in Ghana and where health advocacy is shown, there are no positive role models for nurses to emulate in clinical settings. Instead, it was reported that what they experienced in clinical settings was the opposite of what they were taught because students and junior nurses are not allowed to speak out at work; they are only expected to keep quiet and obey what they are told to do. The absence of health advocacy role models in the clinical settings has been reported by others as a hindrance to nurses performing their health advocacy role.34,50 Nurse educators have many opportunities to prepare nurses as health advocates, but these opportunities are missed when nurse educators fail to nurture assertiveness among student nurses, fail to be role models for students and perpetuate professional timidity by silencing those students who are seen to be confrontational and vocal in raising critical issues affecting their lives or the patients lives in the learning environment. 51 Our participants reported that they had observed situations where student nurses who were vocal in raising issues during training were openly castigated by nurse educators leading to fear and insecurity among students, which germinate as a barrier to health advocacy during training and later in ones’ professional life.
Finally, these barriers to health advocacy propelled a number of nurses to have difficulty performing their roles. The current study revealed that some nurses found themselves in a state of dilemma, wondering who to stand for. Although nurses' primary responsibilities are to their patients, before the institution or other healthcare workers, 27 due to the barriers many have remained silent. 20
Conclusion
Unlike in Western countries, barriers to nursing performing health advocacy role in Ghana is also entrenched in cultural traditions such as the socialisation of children to keep quiet and obey and do what they are told by adults, and not to question whether anything is wrong or right. This cultural tradition permeates the walls of nursing education and healthcare settings, thus creating an impossible environment for practising health advocacy among nurses. Simulating health advocacy during training may help untangle previously upheld cultural traditions that prevent nurses from using their health advocacy role. Providing nursing students with positive role models both in the classroom and in the clinical setting can help empower nurses as health advocates. Uprooting cultural and professional traditions that enforce timidity and professional alienation in the nursing profession is essential for eliminating the structural barriers to the practice of health advocacy among nurses.
Limitation and further research
This study is limited because its data comes from public regional hospitals. Nurses working in private hospitals were not interviewed, but their data could have revealed problems that prohibit nurses from fulfilling their advocacy duty. Further research is required to comprehend personality traits and nursing role performance.
Footnotes
Acknowledgements
The authors wish to acknowledge the College of Health Sciences of the UKZN Scholarship for funding this study.
Authors contribution
Both LL and SED conceptualised the idea, wrote the proposal, and designed the instruments for data collection. LL collected the data and analysed whiles SED reviewed and made corrections. LL and SED read and approved the manuscript. Both authors contributed to this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.