
Abstract
Background
Research has shown that moral distress negatively impacts nurses, patients, and organizations; however, several scholars have argued that it can be an opportunity for positive outcomes. Thus, factors that may mitigate moral distress and catalyze positive change need to be explored.
Research aim
The purpose of this study was to explore the relationships among structural and psychological empowerment, psychiatric staff nurses’ experience of moral distress, and strategies for coping with moral distress.
Research design
A descriptive cross-sectional correlational study.
Participants and research context
A total of 180 registered nurses working in psychiatric hospitals in Japan participated. This study examined relationships among key variables using four questionnaires to assess structural and psychological empowerment, moral distress for psychiatric nurses, and coping strategies. Statistical analyses of correlations and multiple regressions were conducted.
Ethical considerations
The study was approved by the institutional review board at the author’s affiliated university.
Findings
Psychiatric nurses perceived moderate levels of structural and psychological empowerment, and their experiences of moral distress were related to low staffing. Structural empowerment was negatively related to the frequency of moral distress but not the intensity. Contrary to expectations, psychological empowerment was not found to mitigate nurses’ moral distress. Multivariate regression analyses revealed that the significant predictors of moral distress were the leaving issues unresolved coping style, the problem-solving coping style, and a lack of formal power, which explained 35% and 22% of the variance in the frequency and intensity of moral distress, respectively.
Conclusions
In psychiatric hospitals in Japan, nurses experience moral distress that compromises the quality of care they provide. Therefore, formal support for nurses in voicing and investigating their moral concerns is required to bestow formal power by establishing a ward culture that includes shared governance.
Keywords
Introduction
Nursing is a profession inextricably intertwined with ethics. In particular, psychiatric nurses face unique moral issues while caring for patients, especially those who have destructive thoughts and behaviors with concomitant diminished decisional capacity and autonomy. Many patients commonly experience forced treatment that may include seclusion, restraint, and involuntary medication, as well as face conflicts with their families or medical staff arising from differing priorities. 1
In Japan, psychiatric nurses typically strive to facilitate the early discharge of acute and long-term patients from hospitals into the community and provide care for aging inpatients with medical complications under circumstances such as chronic inadequate staffing, lack of community resources, and inadequate funding. 2 Moreover, the average length of hospital stay for psychiatric patients in Japan is 275.1 days. 3 This long duration has drawn international attention and criticism. 4 Over the last two decades, the Japanese government has instituted and shown its commitment to multiple mental healthcare reforms to move toward community-based care; however, this process continues to face difficulties. Psychiatric nurses must prioritize and balance multiple commitments and demands while being accountable to their hierarchical organizational systems, creating circumstances that often lead to stressful moral challenges.
Jameton 5 coined the term moral distress, which refers to an experience in which a nurse is constrained from taking a morally correct course of action due to perceived external or internal barriers and constraints, thereby causing the nurse to experience discomfort and psychological pain. Moral distress threatens nurses’ integrity, has ramifications for organizations, and can compromise the quality of patient care. Previous studies have found that moral distress negatively impacts nurses, patients, and organizations, 6 resulting in burnout,7,8 lower job satisfaction, 9 turnover intentions,10–12 and poor quality of care.13–15
Although the literature mainly focuses on the negative impact of moral distress, several scholars have argued that it can act as a catalyst for positive outcomes for nurses. 16 In particular, moral distress can be an opportunity to initiate learning for professional growth and increase awareness of moral demands and institutional obstacles, which can lead to improved patient care.17,18 These influential positive factors need to be addressed at the critical junctures of moral distress, to prevent creating a vicious circle and instead facilitate further professional growth and the development of specific interventions.
Previous studies found a relationship between moral distress and work environment12,19,20 and its impact on individual nurses.14,21 These findings suggest that nurses’ perceptions concerning nurses’ environmental factors related to moral distress need to be considered and that the notion that moral distress merely stems from nurses’ individual attributes is unpersuasive. 22 Considering organizational aspects, a work environment that could enhance work effectiveness and productivity (structural empowerment) may be expected to mitigate nurses’ moral distress. Therefore, it is critical to identify the factors that ameliorate nurses’ moral distress, systematically examine how empowerment factors relate to or mitigate nurses’ moral distress, and determine how those factors affect nurses’ coping strategies.
Background
Structural and psychological empowerment
Previous studies have mostly utilized the concepts of structural and psychological empowerment. From an organizational perspective, Kanter 23 emphasized that “the job makes the person” (p.3); that is, workers’ conscious behaviors and attitudes are shaped by their work environment, not personal attributes or predispositions. The empowering work conditions affect workers’ individual psychological empowerment. Spreitzer 24 conceptualized psychological empowerment as an intrinsic motivational construct, while Laschinger et al.25,26 developed a model in which structural empowerment directly and positively affects psychological empowerment among nurses.
Laschinger et al.’s 26 model posits that empowering work conditions increases nurses’ psychological empowerment. Further, it affects nurses’ strategies to utilize patients’ empowerment in nursing care, resulting in positive patient outcomes. Based on a systematic literature review, Wagner et al. 27 noted a significant association between structural and psychological empowerment. Furthermore, Kanai-Pak 28 tested part of Laschinger et al.’s model 25 in a population of Japanese nurses to investigate whether leadership behaviors mitigated nurse burnout and found that structural empowerment impacts nurses’ psychological empowerment in acute care settings. Another study reported similar results by demonstrating that the work environment was a significant predictor of nurses’ perceptions of ward morale. 29
Thus, these two empowerment factors can be applied to mitigate nurses’ moral distress and achieve positive results. Although several studies have been conducted on leadership and leadership types and structural and psychological empowerment, to date, no studies have been conducted using moral distress and the concept of empowerment in psychiatric settings.
Moral distress and coping in general and psychiatric settings
Schaefer and Vieira 30 performed an integrative literature review on research conducted in several healthcare settings and found that some nurses cope with moral distress in positive ways, such as by communicating with colleagues or reflecting on care, while others cope with it in negative ways, such as by changing jobs, avoiding involvement in ethically challenging situations, or not reflecting on the case at hand. Pavlish et al. 31 examined the factors that perpetuate a culture of avoidance of ethical issues (i.e., healthcare providers remaining silent until a crisis occurs and ethical questions become unavoidable) in oncology settings and identified four factors at the individual, interactional, and system levels: fear of harming relationships, the intellectual and emotional toll of addressing ethics, inconsistencies in perceptions of good caregiving, and system processes that entrench avoidance care.
Ando and Kawano 32 reported that, among psychiatric nurses in Japan, common responses to ethical problems include “lack of action,” “consulting,” and “searching for evidence-based care.” Musto and Schreiber 33 found that moral distress occurs when nurses become involved in incidents that impact patients’ physical, emotional, and environmental safety and encompasses both patients and staff. In that study, participants mostly found someone to talk to and began an iterative process; they engaged in a dialog, experienced a shift in perspective, and eventually moved toward a resolution. Furthermore, the authors emphasized the relational aspects of moral distress alongside its contextual and situational aspects. They also found that when nurses had a positive experience of dialog and found that their answer to the question “Is this the best I can do?” was satisfactory, they continued to work at the unit. In contrast, nurses who had a negative experience of dialog either left the unit or talked about leaving. Jansen et al. 34 reported that the coping strategies of reappraising and seeking support from colleagues were common among psychiatric nurses, thus emphasizing the importance of colleagues and the work environment. Austin et al. 35 revealed that nurses who experience moral distress typically feel alone, forsaken, and abandoned, and further noted that moral distress occurs when society assigns significant expectations and responsibilities, which often do not come with the necessary power and control. Therefore, it is imperative that professionals have the resources they need to fulfill their commitments.
Based on previous research on moral distress and empowerment, this study will fill the gaps in the literature by examining the effects of moral distress in a population of Japanese psychiatric nurses to address how the factors of structural and psychological empowerment, moral distress, and coping strategies are systematically related. This study provides a better understanding of nurses’ experiences of moral distress from the perspective of person-work environment interaction.
Research aim
The purpose of this study was to explore the relationships among psychiatric nurses’ moral distress, their perceptions of structural and psychological empowerment, and their coping strategies in Japan.
Method
Participants and setting
This study recruited a convenience sample of registered nurses who worked at psychiatric hospitals in the central and western regions of Japan. Out of 27 psychiatric hospitals contacted, the nursing directors of nine agreed to participate in this study. A G* power analysis using the F statistic and multiple regression (power = 0.8, alpha = 0.05) and the number of predictors (including 14 subscales) showed that this study required a sample size of 146. Ultimately, a total of 727 registered nurses from nine psychiatric hospitals were invited to participate in the study.
The inclusion criteria were registered nurses who had worked in a psychiatric emergency, acute, chronic, rehabilitation, or substance use psychiatric unit for at least 6 months. This allowed for homogeneity in the nursing roles and types of care provided in these units. The exclusion criteria were: (1) nurses in administrative positions, (2) practical nurses and care workers, and (3) nurses employed by forensic psychiatric units, severe physical and intellectual disability units, or psychiatric units providing care for aged dementia patients. These criteria allowed for the homogeneity of the study participants, their working environment, and their nursing roles as staff nurses in psychiatric units.
Definitions of study variables
The study variables included the following demographic data: age, educational background, type of psychiatric unit where participants currently worked, years of experience in psychiatric settings, years of experience at the hospital, and whether participants had attended continuing education courses on ethics in the past 5 years. The theoretical definitions for this study included structural empowerment, psychological empowerment, moral distress, and coping strategies.
Structural empowerment
Structural empowerment 26 is defined as the extent to which employees feel they have access to the following six conditions in their work settings: (a) formal power, or the specific job characteristics required to achieve organizational goals; (b) informal power, or the social connections among peers, subordinators, and cross-functional groups; (c) access to opportunity, or the possibility for growth and increased skills; (d) access to resources or the possibility of acquiring materials such as time, supplies, or finances; (e) access to information, or the formal and informal knowledge and understanding of organizational policies and decisions; and (f) access to support or receiving feedback and guidance from colleagues and supervisors.
Structural empowerment was measured using the Japanese version of the Conditions for Work Effectiveness Questionnaire (CWEQ-II).28,36 The CWEQ-II has six constructs of structural empowerment: access to opportunity, access to information, access to support, access to resources, formal power, and informal power. The CWEQ-II has a total of 21 items, measured using a five-point Likert scale (1 = none to 5 = a lot). Kanai-Pak 28 reported the reliability of the six constructs, as measured by Cronbach’s alpha: opportunity (0.84), information (0.87), support (0.92), resources (0.78), formal power (0.66), and informal power (0.67).
Psychological empowerment
Conger and Kanungo 37 define psychological empowerment as “a process whereby an individual’s belief in his or her self-efficacy is enhanced” (p.474). This study utilized the Psychological Empowerment Scale (PES) 24 translated into Japanese by Kanai-Pak. 28 The PES has four components: meaningful work, competence, self-determination, and impact. The PES has a total of 12 items and uses a seven-point Likert scale (1 = very strongly disagree to 7 = very strongly agree). Cronbach’s alpha for the entire PES in the sample was 0.90.
Moral distress
Moral distress “arises when one knows the right thing to do, but institutional constraints make it nearly impossible to pursue the right course of action” (5, p.6). The Moral Distress Scale for Psychiatric nurses (MDS-P) 8 was used to measure moral distress in this study. The MDS-P comprises 15 items and uses seven-point Likert scales to rate frequency (0 = none to 6 = very frequent) and intensity (0 = none to 6 = a great extent). The MDS-P includes three constructs: unethical conduct by caregivers, poor staffing, and acquiescence of patients’ rights violations. The internal consistency reliability based on Cronbach’s alpha was 0.90 for the whole MDS-P and 0.85, 0.82, and 0.79 for unethical conduct by caregivers, poor staffing, and acquiescence to patients’ rights violations, respectively. 8
Coping
Lazarus et al. 38 defined coping as “constantly changing cognitive and behavioral efforts to manage specific and/or internal demands that are appraised as taxing and exceeding the resources of the person” (p. 141).
The Coping Scale from the Job Stress Scale-Revised (JSS-R), originally developed by Kosugi et al. 39 in Japanese, was utilized to measure coping in the study’s sample population. The scale includes 22 items and uses a four-point Likert scale (1 = none to 4 = frequently). This scale has three factors, active problem-solving, seeking social support, and leaving issues unresolved, for which Cronbach’s alpha values are 0.86, 0.71, and 0.77, respectively. In this study, active coping includes problem-solving and seeking social support, whereas non-active coping denotes leaving issues unresolved.
Ethical considerations
The IRBs at the author’s affiliated university and the hospitals used as study sites (when required) approved the study. Participation in this study was voluntary, and all information provided remained confidential. Data were handled statistically and anonymously. By returning the completed survey directly to the investigator by postal mail using the enclosed stamped envelope, it was understood that participants were giving their consent to participate in this study.
Data collection
Data were collected between February and March 2018. After the IRBs at the author’s affiliated university and hospitals approved the study, the investigator visited and held information sessions with nurse managers to explain it. Once the nurse managers’ agreement and cooperation had been secured, they received several questionnaire packages, including a cover letter for the study participants, consent forms, and the questionnaires: the CWEQ-II, PES, MDS-P, and Coping Scale. Nurse managers were asked to leave these materials in their nurses’ lounges, and a flyer was posted near the packets so that potential participants could access them voluntarily. After potential participants examined the questionnaire packet and consented, they completed the questionnaires and returned them using a postage-paid envelope.
Findings
Descriptive statistics
In total, 182 questionnaires were returned for a response rate of 25%. One hundred 80 were valid. Missing data were at random and accounted for less than 5–6% of all responses. Missing data were replaced with the mean of completed items. 40 Although the data were collected in the private sector, given that 90% of psychiatric hospitals in Japan are private, 4 these data are valid and representative of the larger context of psychiatric hospitals. The Statistical Package for the Social Sciences (IBM SPSS version 25) was used to analyze data.
Demographic characteristics of study participants (N = 180).

Descriptive statistics of major study variables.

Note: SE: Structural Empowerment, PE: Psychological Empowerment, MD: Moral Distress.
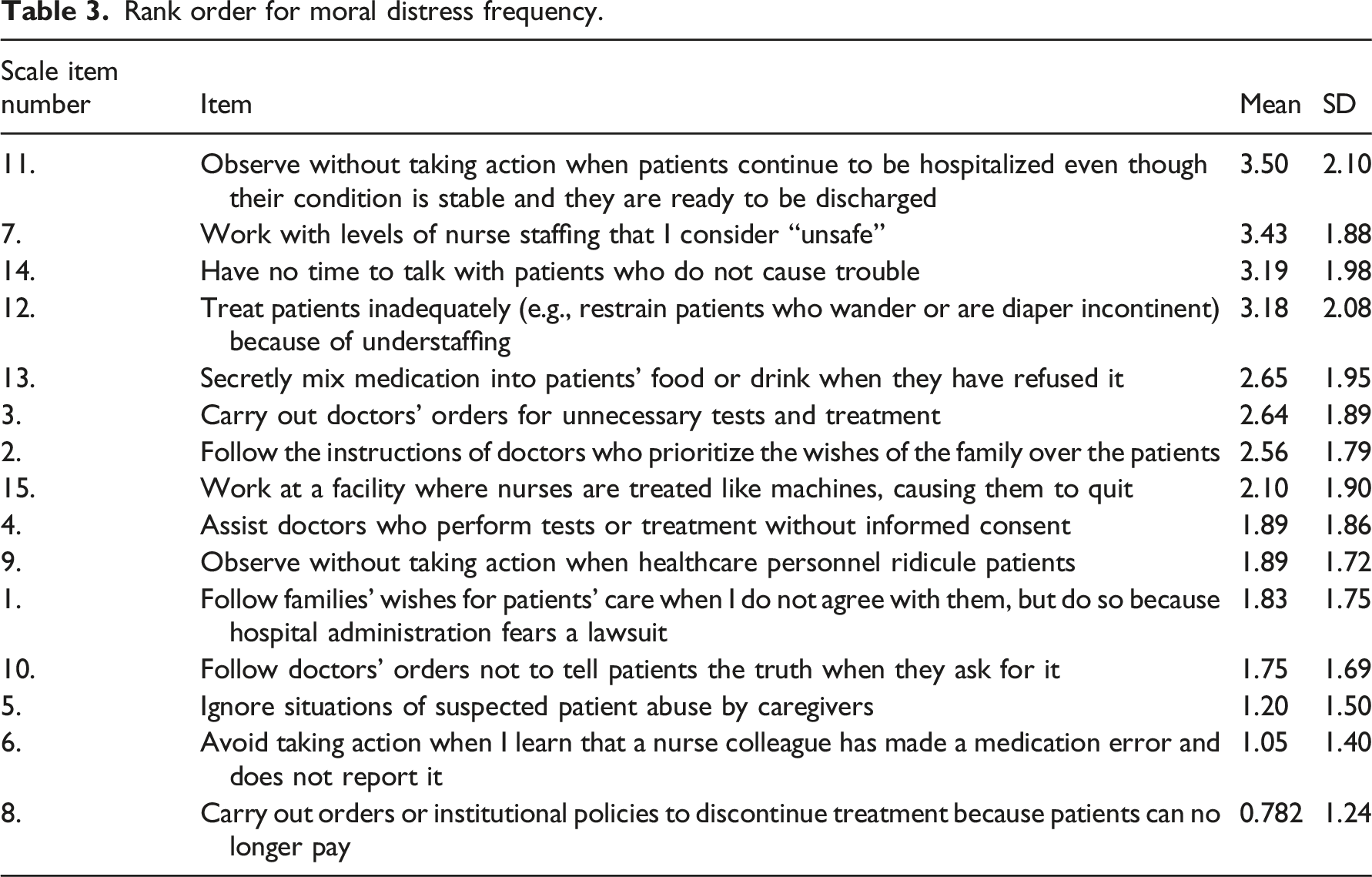
Rank order for moral distress frequency.
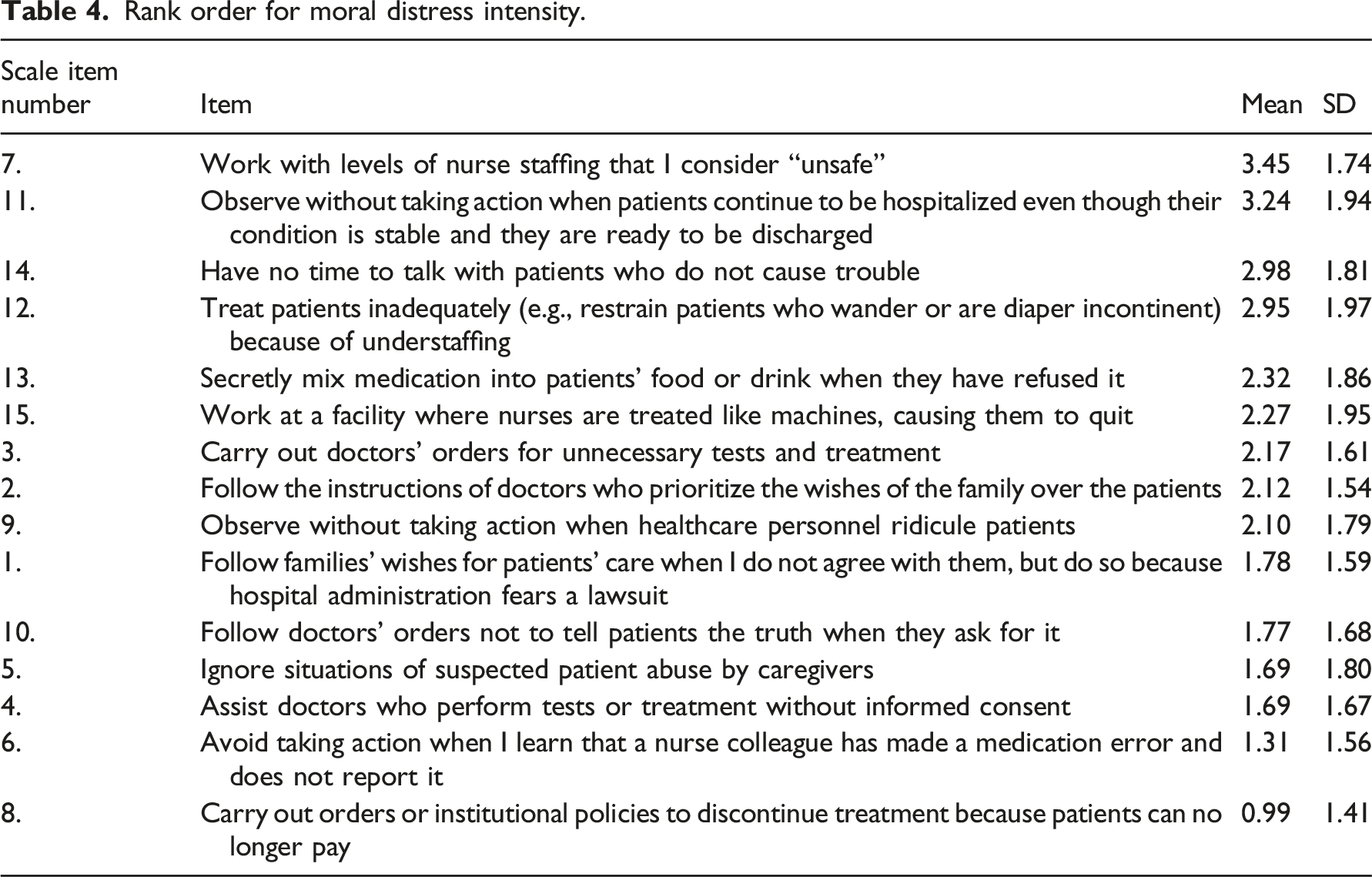
Rank order for moral distress intensity.
Correlations between demographics, empowerment, moral distress, and coping
Correlations between demographic data, structural empowerment, psychological empowerment, moral distress frequency and intensity, and coping (Pearson’s r).

Note: Yrs Psy: years of experience in psychiatric settings. Yrs Hos: years of experience at the current institution, SE: Structural empowerment, PE: Psychological empowerment. Prob solving: Problem solving.
*p < .05, ** p < .01 (2 tailed).
Empowerment, moral distress frequency/intensity, and coping
Correlations between structural empowerment, psychological empowerment, moral distress, and coping (Pearson’s r).
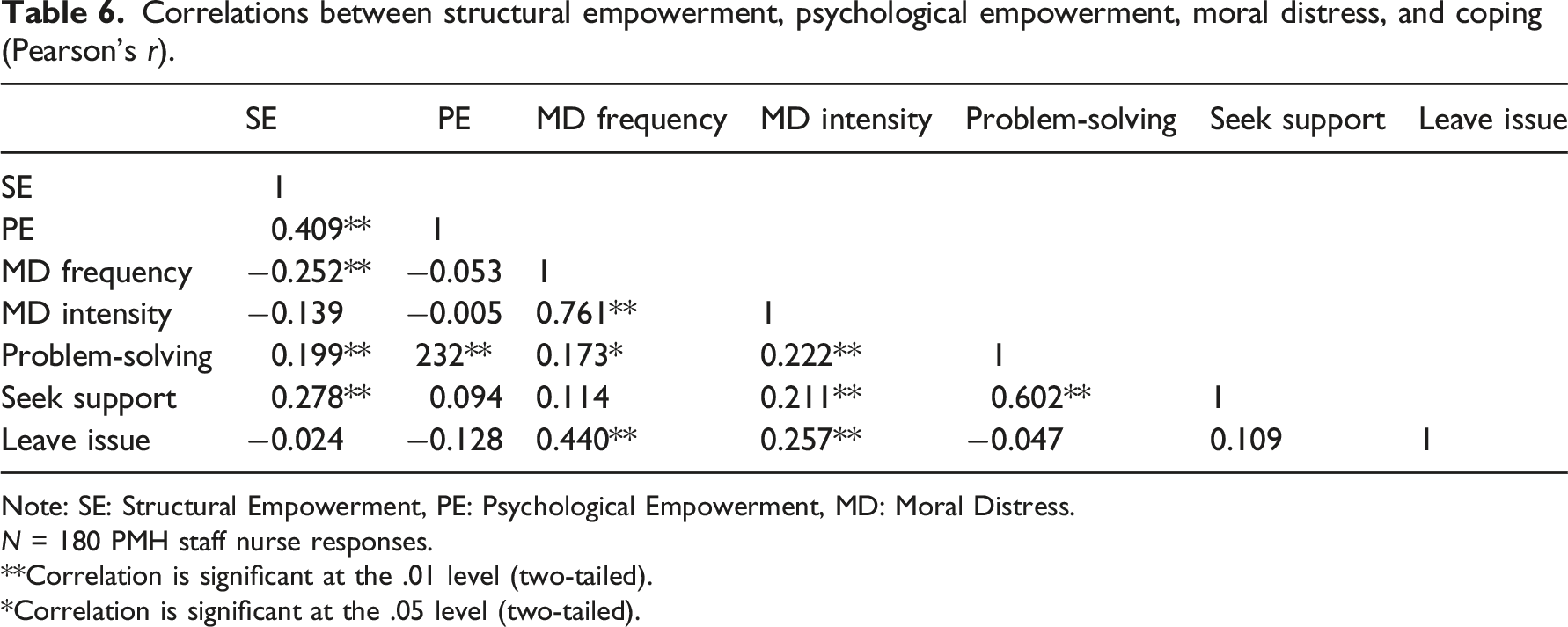
Note: SE: Structural Empowerment, PE: Psychological Empowerment, MD: Moral Distress.
N = 180 PMH staff nurse responses.
**Correlation is significant at the .01 level (two-tailed).
*Correlation is significant at the .05 level (two-tailed).
Structural empowerment and moral distress mediated by psychological empowerment
A significant relationship was found between the total scores for structural empowerment and psychological empowerment; however, no significant relationship was found between the total scores for psychological empowerment and those for moral distress frequency and intensity. Therefore, the assumption was not met to analyze the mediation effect of psychological empowerment.
Factors related to moral distress frequency/intensity in psychiatric nurses
Correlations between demographic data, structural empowerment, psychological empowerment, moral distress frequency, and coping (Pearson’s r).
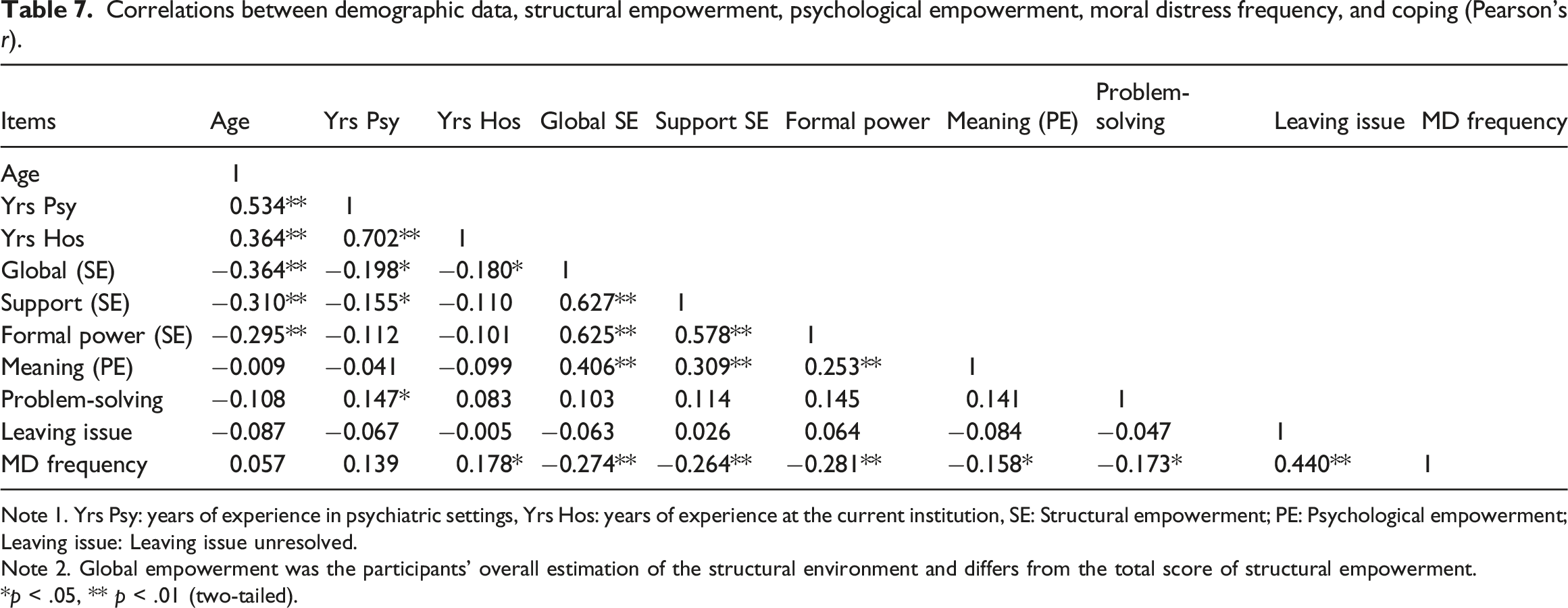
Note 1. Yrs Psy: years of experience in psychiatric settings, Yrs Hos: years of experience at the current institution, SE: Structural empowerment; PE: Psychological empowerment; Leaving issue: Leaving issue unresolved.
Note 2. Global empowerment was the participants’ overall estimation of the structural environment and differs from the total score of structural empowerment.
*p < .05, ** p < .01 (two-tailed).
Multiple linear regression model of moral distress frequency: participant attributes, structural empowerment, psychological empowerment, problem-solving, and leaving issue unresolved coping style.
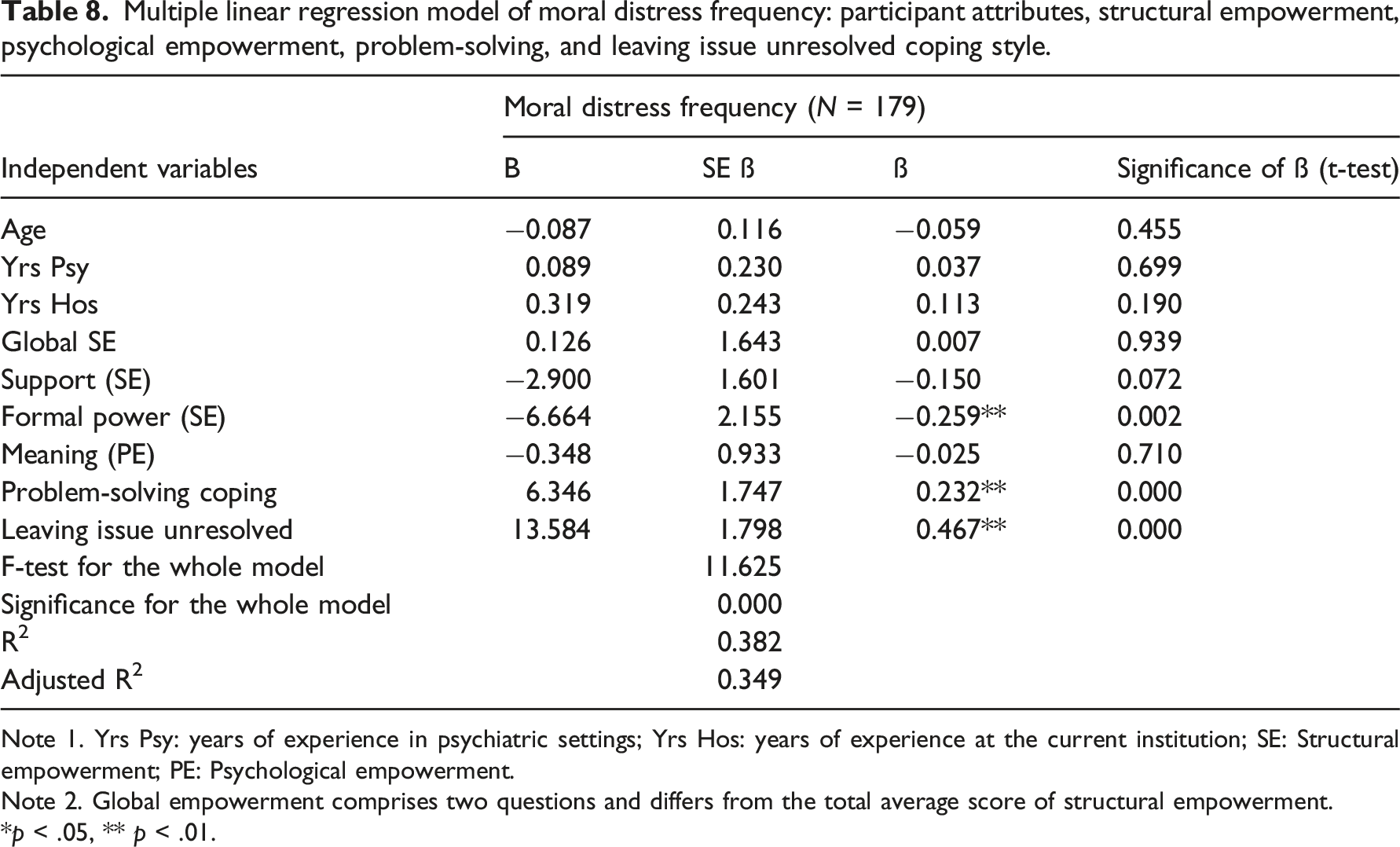
Note 1. Yrs Psy: years of experience in psychiatric settings; Yrs Hos: years of experience at the current institution; SE: Structural empowerment; PE: Psychological empowerment.
Note 2. Global empowerment comprises two questions and differs from the total average score of structural empowerment.
*p < .05, ** p < .01.
Correlations between demographic data, structural empowerment, psychological empowerment, moral distress intensity, and coping.

Note 1. Yrs Psy: years of experience in psychiatric settings, Yrs Hos: years of experience at the current institution, SE: Structural empowerment; MD int: moral distress intensity; PE: Psychological empowerment; Leave issue unresolved: leave issue unresolved coping style.
Note 2. Global empowerment was the participants’ overall estimation of the structural environment and differs from the total score of structural empowerment.
*p < .05, ** p < .01 (two-tailed).
Multiple linear regression model of moral distress intensity: participant attributes, structural empowerment, psychological empowerment, coping.

Note 1. Yrs PHM: years of experience in psychiatric settings; Yrs Hos: years of experience at the current institution; SE: Structural empowerment; PE: Psychological empowerment.
Note 2. Global empowerment comprises two questions and differs from the total average score of structural empowerment.
*p < .05, ** p < .01.
Discussion
In the present study, psychiatric nurses perceived moderate levels of empowerment in the workplace. Furthermore, nurses in this study experienced slightly lower levels of moral distress compared to scores reported in a previous study by Ohnishi et al. 8 Both structural and psychological empowerment were significantly correlated. The study’s findings supported Kanter’s theory and were congruent with previous studies conducted in various non-psychiatric clinical settings.25,41–43
Psychological empowerment and moral distress
This study did not find a significant negative relationship between psychological empowerment and moral distress, indicating that psychological empowerment was not a mitigating factor in moral distress among psychiatric nurses. Hence, the findings showed that psychological empowerment did not mediate the relationship between structural empowerment on moral distress. These findings were incongruent with previous studies that reported a significant relationship between psychological empowerment and moral distress frequency. Browning 44 measured moral distress in critical care settings using Corley’s Moral Distress Scale, 45 which was a different scale from that used in the present study. The researcher reported that psychological empowerment was negatively correlated with and was a significant predictor of moral distress frequency. Similarly, Altaker et al., 46 using a revised version of Corley’s Moral Distress Scale, found a significant negative correlation between psychological empowerment and moral distress frequency. However, the above two studies found no significant relationship between psychological empowerment and moral distress intensity,44,46 which is congruent with the present study.
The discrepancy between this study’s finding that no significant negative relationships exist between psychological empowerment and moral distress frequency, and the findings of other studies, can be explained by the differences in the types of moral problems that nurses often encounter in psychiatric settings compared with critical care/acute care settings. The psychiatric nurses in this study experienced the most frequent and intense moral distress in relation to low staffing. Low staffing is an external cause of moral distress. To explain why this study found no significant relationship between psychological empowerment and moral distress frequency, it could be speculated that moral distress is mostly caused by the external dimension of low staffing, which differs from the intrinsic psychological dimension. Low staffing is an ongoing issue in psychiatric care settings in Japan. The results of this study were congruent with those of Ohnishi et al., 8 in Japan and those of Delfrate et al., 47 in Italy, which showed understaffing to be a common cause of moral distress.
Low staffing occurs at some psychiatric hospitals as Medical Law in Japan permits it exclusively for psychiatric hospitals. The allowed proportions of medical staff are 2/3 of nurses and 1/3 of medical doctors compared to general hospitals. 48 Although mental health professionals have objected to this situation, it is ongoing because Japanese psychiatric care relies heavily on inpatient services. It is predominantly (90%) provided by private not-for-profit hospitals 4 where public funding is not available. 48 Understaffing potentially saves these private hospitals a considerable amount of money.
As Jensen et al. 15 articulated, a lack of staff in acute psychiatric settings leads to inadequate care, including superficial treatment, more disruptive behavior, and coercive measures. Coercive management strategies such as restrictions, seclusions, and restraints due to inadequate staff invoke nurses’ feelings of guilt and uneasiness. However, if nurses are forced to frequently use coercive measures while convincing themselves and others that these are to ensure safety for all, they may begin to use them habitually. While they automatically reassure themselves that coercive measures are unavoidable, a dangerous ethical situation occurs. 49
Moral distress frequency and intensity and moral residue
This study found that structural empowerment was significantly negatively correlated with moral distress frequency but not intensity. This supports Corley et al. 19 and Ganz et al 50 who described moral distress frequency and intensity as different concepts. Nurses’ perceptions of moral distress frequency might be related to their moral sensitivity regarding their environment, whereas moral distress intensity might be based on their experiences and interpretations of moral phenomena.
Epstein and Hamric 51 explained that when nurses encounter a morally distressing situation, although some anguished feelings are alleviated over time, they are not completely eliminated. Hence, the moral distress residuals remain internally, which the researchers termed moral residue. The researchers further explained that, over time, repeated moral distress gradually increases baseline moral distress and moral residue, which was named the crescendo effect of moral distress, and the repeated experiences of moral distress evoke strong negative feelings. Therefore, while moral distress frequency could be an attribute of the environment in which problems were perceived by present study participants as related to low staffing, moral distress intensity could be an internalized attribute influenced by participants’ experiences and environmental factors.
Implications
Participants of this study reported their experiences of moral distress frequency and intensity as being at a moderately lower level than the mid-point score. At first glance, they may not be considered as suffering from the negative impact of moral distress. However, caution must be taken for several reasons. First, as this study showed, having more years of experience in psychiatric units was significantly correlated with higher moral distress intensity. Moral residue and repeated encounters with even minor situations of moral distress can cause accumulated and deleterious effects, such as burnout, turnover intention, and even learned numbness to moral issues. Second, considering the unique ethical issues that arise in psychiatric settings, moral distress situations are often latent and ingrained in daily practice. Ubiquitous moral issues might be easily overlooked in clinical situations. Without numbing their moral sensitivity, psychiatric nurses must carefully examine their daily practices to fulfill their professional obligations to patients and families.
This study found that the coping style of leaving an issue unresolved and lack of formal power are significant predictors of both the frequency and intensity of moral distress. This finding supports Austin et al. 35 who revealed that moral distress arises when professional expectations and responsibilities are not commensurate with a professional’s power and control over a given situation. Additionally, Jansen et al. 15 reported that although nurses are responsible for the quality of care, study participants in acute psychiatric settings reported having limited influence on the decision-making process.
To prevent psychiatric nurses from falling into a vicious cycle of moral distress, restructuring the essence of structural empowerment, which is related to the concept of shared governance, where nurses are involved in the decision-making process, will ameliorate their moral distress in an organization. Staff nurses may have less formal power in a hierarchical organization; however, their proximity to patients and families gives them a pivotal role that affects nursing practice quality.
In Japan, it is common for psychiatrists to be the leaders of the medical team and own private hospitals. In such cases, staff nurses are likely to perceive themselves as lacking formal power to intervene in and control ethically questionable situations. Thus, this perception makes them hesitate to intervene, and they give up examining the issue. Coupled with underlying Japanese cultural norms emphasizing harmony, subtle communication, and an authoritarian work environment, this tendency adds obstacles to open discussion about nurses’ concerns.
Regarding ethics education, more than half of the participants in this study did not pursue continuing education in ethics. One of the possible reasons for this is that nurses’ license does not require renewal, and each hospital has established clinical ladders for nurses’ development. Therefore, an urgent need exists for nurse education. A work environment that promotes collective silence about moral issues among nurses and ignorance about their concerns will diminish the quality of care.
Helmers et al. 52 recommended that formal support be provided and access to bioethics consultations and ethics education should be established. For example, Ohnishi et al. 53 established an online ethics consultation system to support nurses. These services are expected to play an important role. Providing opportunities for nurses to discuss their moral distress freely is crucial to shift their adverse experiences of moral distress into opportunities for constructive personal growth.
Limitations
This study employed a cross-sectional design, which could not identify causal factors. In addition, to increase generalizability, the study participants were recruited from nine different private hospitals from various locations in Japan, including urban and rural areas. However, the results may not be representative of all psychiatric nurses in Japan because participants were not selected at random; thus, the results may have been affected by sampling bias. Although this study conducted a power analysis to secure statistical validity, it was limited by a low response rate of 25%, which may indicate that nurses who were more motivated to discuss the topic may have participated in the study. Moreover, although this study used measures with well-established validity and reliability, response bias, such as social desirability, is inevitable with the use of self-report measures.
Conclusion
This research revealed that psychiatric nurses experience moderately low levels of moral distress and work with moderate levels of empowerment in their work settings. The study found that work-empowering environments are related to nurses’ psychological empowerment, as is evident among various clinical settings and across countries. The significant predictors of moral distress in the workplace were a lack of formal power and using the non-active coping style of leaving issues unresolved. Nurses’ experiences of moral distress were most frequently and intensely caused by low staffing. Contrary to expectations, psychological empowerment did not impact moral distress. To ameliorate psychiatric nurses’ moral distress, which stems from leaving issues unresolved and a lack of formal power, it is necessary to create a work environment in which nurses’ moral distress is both voiced and heard and where nurses are included in decision-making processes.
Footnotes
Acknowledgements
This manuscript was revised based on the doctoral dissertation submitted to Adelphi University. I would like to thank Dr. Jane White for her guidance and support at every step of my dissertation journey. In addition, I would like to thank all participants in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Research ethics
The study was approved by the Adelphi University Institutional Review Board on January 16, 2018. Approval #120617.