
Abstract
Background
Moral sensitivity and academic integrity discernment hold paramount importance for healthcare professionals. Owing to distinct undergraduate educational backgrounds, nurses and physicians may exhibit divergent moral perspectives, academic integrity cognisance, and moral sensitivity within clinical environments. A limited number of studies have investigated the disparities and congruencies pertaining to moral sensitivity and academic ethical awareness among nursing and medical students.
Objective
The study compares moral sensitivity and academic ethical awareness of undergraduate nursing and medical students with and without clinical exposure.
Research design
A self-administered cross-sectional survey conducted from January to February 2022 was used to collect data from a medical school in Hong Kong.
Participants and research context
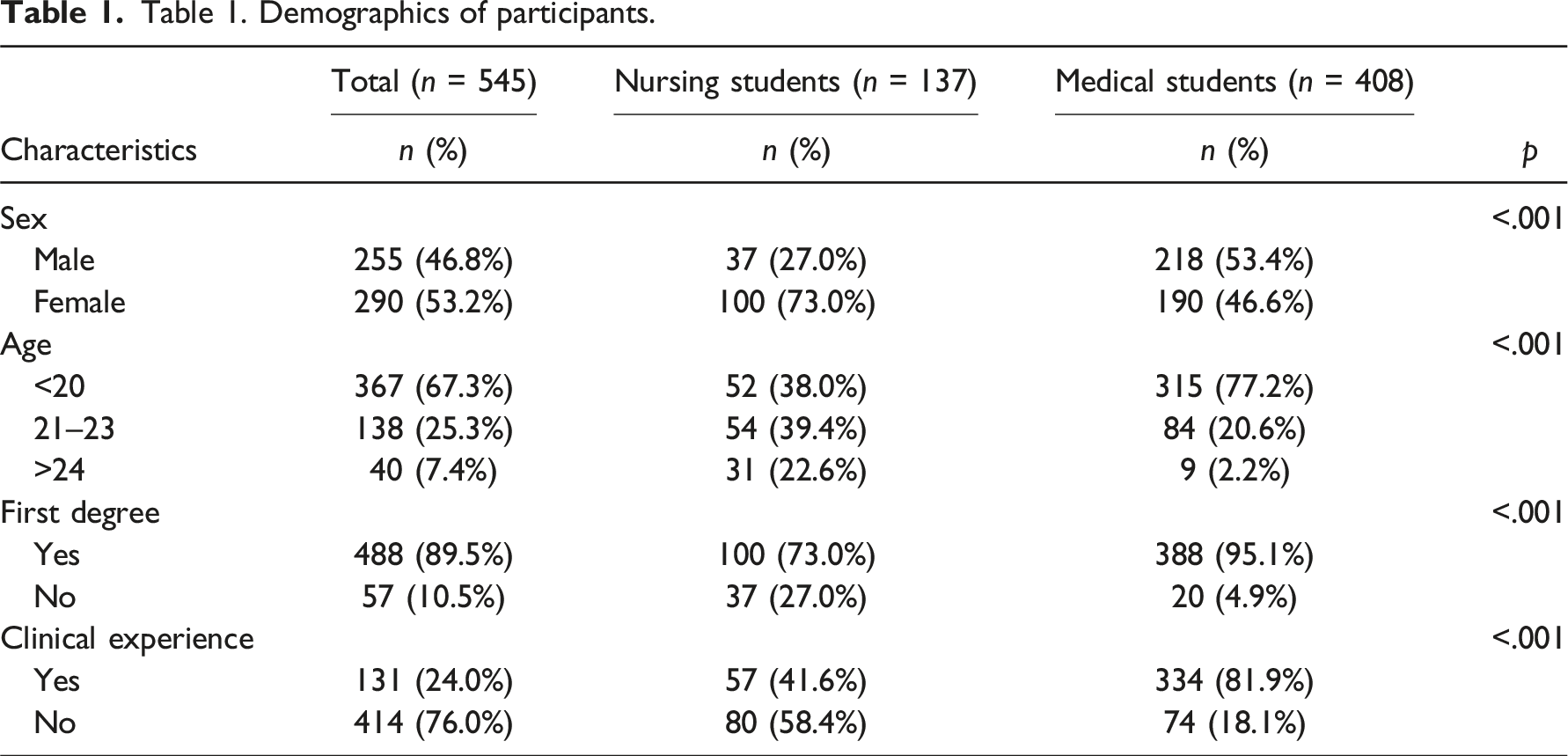
A total of 545 respondents, including 137 nursing students and 408 medical students, completed the questionnaire.
Ethical consideration
Ethics approval of the study was obtained. Written consent was waived to maintain anonymity because completing the questionnaire was considered implied consent.
Findings
Both groups of undergraduates demonstrated a high level of bioethics knowledge. In terms of academic integrity, medical students were found to have a less concerned attitude towards punctuality, attendance, and skipping classes. Regarding moral sensitivity, senior medical students with clinical experience put less emphasis on decision-making involving patient participation, while senior nursing students were more hesitant in withholding treatment for incompetent patients who refused treatment. Both nursing and medical students showed decreased moral sensitivity in the ‘conflicts’ domain with increased clinical exposure.
Conclusion
Study findings contribute to the discussion comparing the ethical attitudes of nursing and medical students. More effort should be made in nursing and medical education to promote practices in line with high academic integrity and to develop the ability to be morally sensitive in professional settings.
Keywords
Introduction
Healthcare systems around the world are becoming increasingly complex due to advancements in technology, changes in healthcare policies, and the diversity of patient populations. As a result, healthcare professionals face various ethical challenges and dilemmas, and must navigate complex ethical situations, govern their practice, and make decisions that prioritise patient well-being.1,2 This requires moral sensitivity and strong academic integrity awareness.3–5 Physicians and nurses, both of whom provide care for patients, are expected to work closely together to achieve these goals in practice, but medical professionals between the two professions may have differences concerning their moral sensitivities and academic integrity awareness due to their different educational programmes and roles in healthcare practice,6–9 which may impact their ethical decision-making in complex situations, integrity, accountability, and responsible conduct. Prospective physicians and nurses begin acquiring knowledge and developing sound moral and ethical judgements during their undergraduate training. Thus, fostering a strong foundation for ethical and moral behaviour starting from the undergraduate level is crucial. This study, therefore, aims to identify and compare the potential differences and similarities in moral sensitivity and academic ethics awareness between undergraduate nursing and medical students in Hong Kong.
Background
Moral sensitivity is a crucial attribute that healthcare professionals must possess to navigate ethical challenges in clinical practice. It is essential as it enables healthcare professionals to identify a moral conflict and respond appropriately to ethical challenges and dilemmas in their clinical practice. 10 It involves being aware of one’s values, understanding the values of others, and recognising the ethical implications of actions and decisions. 11 Lützen et al. developed a theocratical framework for moral sensitivity, highlighting five core components of moral sensitivity that facilitate healthcare professionals in recognising, understanding, and navigating ethical issues: ‘Structural moral meaning’, which refers to the ways used to obtain ethical significance from decisions and actions even if they may restrict patient autonomy; ‘Expressing benevolence’, which refers to a course of action that is in line with the patient’s best interests; ‘Modifying autonomy’, which often occurs in a situation where there is a need to protect the patient from harming himself, herself or others; ‘Experiencing moral conflict’, which requires recognising and acknowledging potential or actual moral dilemmas before putting moral sensitivity into practice; and ‘Confidence in nursing and medical knowledge’, which implies that nursing and medical knowledge is important to resolve ethical conflicts.12–14 In the framework, trust is a fundamental aspect of any relationship, especially in the healthcare setting, where patients rely on healthcare professionals to provide them with competent and ethical care. The connection between building trustworthy relationships with patients and moral sensitivity lies in the importance of ethical awareness and sensitivity in healthcare. When healthcare professionals prioritise building trustworthy relationships with patients, they become more attuned to the ethical dimensions of their interactions and decisions. Studies have found that healthcare professionals with higher levels of moral sensitivity are more likely to engage in ethical behaviour, such as patient-centred decision-making and adherence to ethical principles15–17 They are more attuned to the nuances of patient care and better understand the perspectives and values of the diverse patient population they serve. This, in turn, facilitates a deeper level of empathy, fostering rapport between patient and provider, leading to improved patient outcomes and greater satisfaction.12–14
Academic integrity awareness refers to understanding ethical principles in learning activities, which requires individuals to uphold integrity, honesty, and fairness in their academic pursuits. 18 Even though academic ethics are considered important for most students, some did not view improper behaviours, such as being absent from a class, cheating on exams, and plagiarism, as problematic.19,20 Previous evidence suggests that 54% of nursing students 21 and 67%–90% of medical students 22 admitted to cheating on exams or in otherwise similar situations in their undergraduate studies. Other than academic misconduct, studies also found that some nursing and medical undergraduates have been involved in severe ethical misconduct, such as openly discussing patient information with non-medical staff, recording false information about medical treatments, and deserting the practice site during their assigned duty.20,21,23 Lack of awareness and conducting ethically inappropriate behaviours could affect the capability of undergraduates to make ethical decisions, harm their professionalism, undermine patient trust, and increase the risk to patient safety. 20
Nurses and physicians have unique and complementary roles in patient care. 24 For example, in the end-of-life context, nurses often spend more time in patient care, providing bedside care, administering medications, and monitoring vital signs. They work closely with patients, their families, and other healthcare professionals to coordinate care and ensure patients receive the best possible treatment. Nurses have primarily been prepared to look at the patient as a whole person and evaluate more than the disease process 25 and can become effective patient communication advocates. 26 On the other hand, physicians are responsible for diagnosing and treating patients, making clinical decisions, and prescribing medications. Physicians bear the burden of making treatment decisions. 26 While nurses and physicians have different roles and responsibilities, there is evidence that conflict and confusion occur between nurses and physicians.27,28 Thus, it is crucial to explore the moral sensitivity and academic integrity awareness held by these two groups of healthcare professionals, as their distinct roles and responsibilities can impact the ethical decisions they make in patient care.
As a team, nurses and physicians can integrate diverse perspectives to arrive at more comprehensive and patient-centred ethical decisions by appreciating each other’s strengths. Their mutual goal of patient care can ultimately lead to more effective communication and collaboration. Comparing the moral awareness and sensitivity of nursing and medical students can help us understand how these different roles and responsibilities impact their ethical attitudes and decision-making. It can also help us tailor more targeted ethics curricula and training programmes and develop best practices for ethical decision-making in healthcare. Further, this information can help educators understand how these attributes contribute to students’ overall growth and success in their academic pursuits and future careers. They can also help identify areas where further education and training are needed to foster a culture of integrity and ethical behaviour in healthcare settings.
Contemporary healthcare systems require nurses and physicians to collaborate more closely for comprehensive and holistic patient care. Given that nursing and medical students receive different types of training and education starting from an undergraduate level, 29 it is necessary and appropriate to explore the moral sensitivity and academic integrity awareness held by these two groups of healthcare professionals and identify the differences. Earlier studies have looked into moral sensitivity and academic integrity awareness for nursing and medical students, respectively,8–10,12–20 but very few studies compare the two groups of students.5,6 To the best of our knowledge, there is a lack of information on the attitudes of undergraduate nursing and medical students towards moral sensitivity and academic integrity awareness. The study aims to compare the moral sensitivity and academic integrity awareness of undergraduate nursing and medical students with and without clinical experience.
Methods
Research Context
The study utilised a descriptive cross-sectional correlational research design at one of the two local universities offering undergraduate nursing and medical degree programmes in Hong Kong. The nursing curriculum is a five-year programme, with clinical placements in various specialities spanning from the second to the final year. The medical curriculum is a six-year programme. The first three years are pre-clinical, emphasising interdisciplinary science and humanities training, while the latter three years are clinical clerkships focused on advanced science and clinical medicine. Medical students enter their clinical clerkship having completed several courses in bioethics, resilience, communication, and professionalism, which helps them develop their moral compasses. Nursing students learn bioethical principles and professionalism in the first foundation year and have a specific course on legal and ethical issues related to contemporary practices, such as reproductive health, end-of-life care and clinical research, in the third year. Ethics education is embedded in both curricula throughout the whole programme.
Data Collection
An online self-administered cross-sectional survey was conducted from January to February 2022. The invitation was sent to all nursing and medical students through mass email using convenience sampling. After the initial invitation, two reminder emails were sent to remind participants every two weeks.
Study Instruments
The questionnaire comprises three measures, including perceived knowledge of and attitudes towards bioethics learning, academic ethical awareness, and moral sensitivity. Demographic information, including age, gender, educational background, study programmes, and clinical exposure, was also collected.
Perceived knowledge and attitude towards bioethics learning assesses understanding of the four pillars of bioethics, the Hippocratic Oath, the Nuremberg Code, the Nightingale Pledge, and Healthcare-related Law. Students rated their understanding of various bioethics principles from 0 (know nothing at all) to 10 (very confident in their understanding). They were also asked to rate their level of commitment to learning ethics and science from 1 (lowest) to 10 (highest).
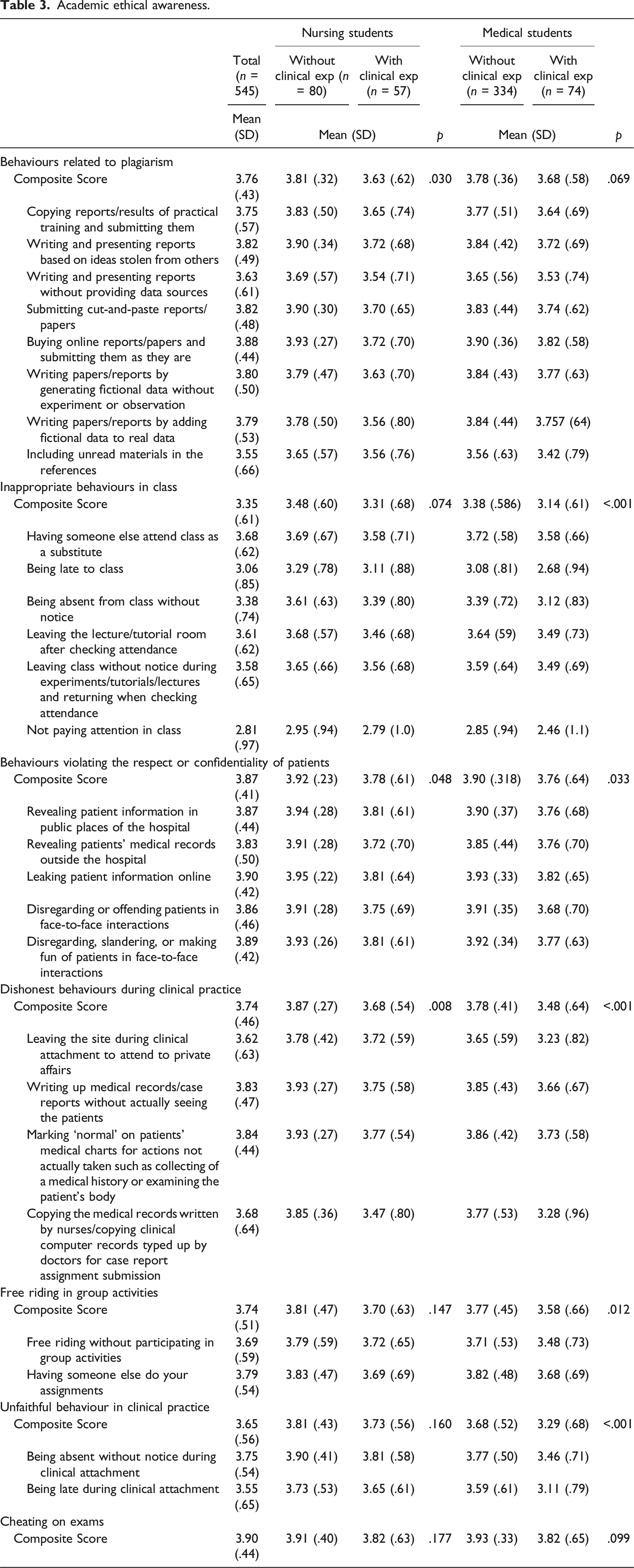
Academic ethical awareness is measured by a validated Academic Ethics Awareness scale developed by Kwon et al. 20 and modified by Cho et al. 18 Amongst the 30 items, two were deleted so that the tool suited both students with and without clinical exposure. The removed items are: ‘Free riding without participating in group projects for clinical practice’ and ‘Asking for answers to exam questions during practical exams’. The remaining 28 items were categorised under seven subscales: behaviours related to plagiarism (8 items), inappropriate behaviours in class (6 items), behaviours violating the respect or confidentiality of patients (5 items), dishonest behaviours during clinical practice (4 items), free-riding in group activities (4 items), unfaithful behaviours in clinical practice (2 items), and cheating in exams (1 item). Respondents were asked to use a 4-point Likert scale, ranging from 1 (allowed to do) to 4 (not allowed to do), to indicate the level of agreement with the statements. A higher score indicated a higher level of academic integrity awareness. The Cronbach alpha for the overall scale in the present study is 0.954 and 0.781 to 0.948 for the subscales.
Moral sensitivity is assessed by the validated moral sensitivity questionnaire among registered practising psychiatric 10 or general nurses3,30 and nursing students.7,31 This study adopted the back-translated English version developed by Han et al. 31 with 27 items under five subscales: benevolence, patient-oriented care, moral conflict, moral meaning, and professional responsibility. Some wordings were changed to adjust the applicability of the psychiatry-oriented tool to student populations. For example, references to ‘psychiatrist’ were replaced with regards to either ‘nurse’ or ‘doctor’; the terms ‘psychiatric care’ were rephrased as ‘patient care’; the words ‘psychiatric practice’ were rephrased as ‘nursing or clinical attachment’; and the term ‘patient admitted under the Mental Health Act’ was rephrased to refer to ‘mentally incompetent patient’. Respondents were asked to use a 5-point Likert scale, ranging from 1 (do not agree at all) to 5 (strongly agree), to indicate the level of agreement with the statements. A higher score indicated a demonstration of moral sensitivity to a greater degree. Cronbach’s alpha for the overall scale in the present study is 0.871, and 0.696 to 0.823 for the subscales.
Data Analysis
Data was analysed using the SPSS version 25. Descriptive statistics, such as means, frequencies, and percentages, were employed to summarise demographic characteristics. Students in each nursing and medicine programme were stratified into groups by clinical experience, nursing students with or without clinical experience, and medical students with or without clinical experience. Independent t test was used to compare demographic characteristics between the groups.
Ethical Considerations
According to the institutional guidelines, ethics approval of the study was obtained. Written consent was waived to maintain anonymity because completing the questionnaire was considered implied consent. The research procedures complied with the ethical standards of the institutional research committee and the Declaration of Helsinki. All participants were given detailed information about the purpose and methodology of the study. The confidentiality of the participants’ information and the right to withdraw from the study were explained during the introduction.
Findings
Respondents’ Characteristics
Table 1. Demographics of participants.
Perceived Knowledge and Attitude towards Bioethics Learning
Table 2. Perceived knowledge and attitude towards bioethics learning.
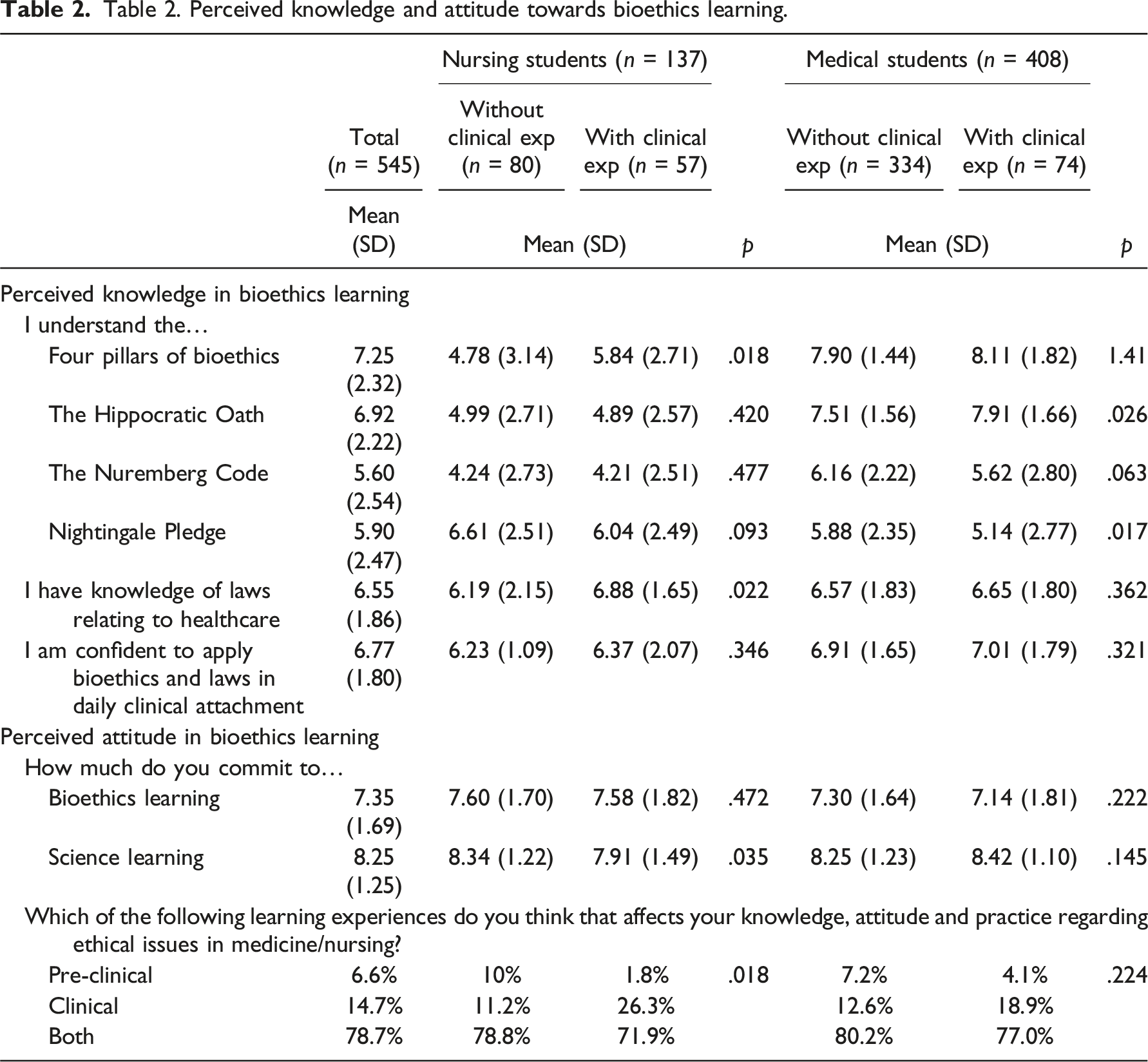
Nursing students who had clinical exposure showed a lower level of commitment towards science learning compared to the pre-clinical environment, with a greater emphasis on learning ethics. There are no other statistical significances among medical students.
Academic Ethical Awareness
Academic ethical awareness.
Moral Sensitivity
Table 4. Moral sensitivity.

Discussion
This study was the first to compare moral sensitivity and academic ethical awareness among undergraduate nursing and medical students with and without clinical experience in Hong Kong.
Our research reveals that nursing students possess a lower awareness than medical students regarding the inclusion of fabricated data in reports and academic papers. This discrepancy could carry over into their professional practices, potentially compromising their future capacity for precise medical incident reporting. Inaccuracy in reporting can jeopardise patient safety, as underreporting of medical incidents is a critical issue that can adversely affect patient care. 32 Notably, physicians typically prioritise incident reporting more than nurses. Barriers to effective reporting include the absence of a robust reporting structure, a culture that emphasises blame, and a punitive environment. Our concerning discovery is that nursing students demonstrate a decline in ethical sensitivity regarding the creation of fictitious data after clinical training. Therefore, it’s imperative to establish a comprehensive, blame-free, and transparent incident reporting system that is readily accessible and accompanied by clear guidelines and constructive feedback. Integrating a robust and efficient reporting system into the early stages of medical and nursing education is essential, with continuous emphasis throughout both pre-clinical and clinical training.
In contrast, medical students in our study were found to have lower awareness than nursing students of being late to class and clinical attachments, being absent without notice during class and clinical attachments, and leaving the site during clinical attachment to attend to private affairs. These differences in attitude between nursing and medical students toward punctuality, attendance, and leaving the clinical site may be due to the different natures of the two professions. Even during training, nursing students spend most of their time in the clinical caring for patients’ day-to-day needs. On the other hand, medical students limit their community activities to short clerking and physical examinations. After graduation from medical school, physicians generally have more autonomy to leave the practice site than nursing staff and do not spend as much time at the bedside as nurses.13,33
Various studies have been conducted based on the concept of moral sensitivity. Previous studies have shown that strong moral sensitivity is crucial in resolving ethical dilemmas, 13 preventing unethical behaviour, 34 and decreasing moral distress.34,35 The relationship between moral sensitivities and clinical experience remained inclusive. In contrast to the belief that moral sensitivity increased as professional expertise increased,36,37 some reported no relationship8,38,39 and others found a negative relationship between the two parameters. 40 Our findings support the latter conclusion, revealing that nursing and medical students with clinical experience had a lower moral sensitivity than their counterparts without clinical experience. Our observation is that senior students with clinical exposure have an overall lower decline in moral sensitivities, suggesting that ethical commitment learning erodes over time. The apparent erosion in academic awareness or moral sensitivity contradicts the generally held idea that moral reasoning and judgement grow with education. However, this may be explained by the fact that individual moral sensitivities may represent a complex interplay of other capacities, such as personal experience, cultural background, significant life events, gender and parental status.
In the local teaching culture, students tend to participate in classroom learning passively rather than proactively participate in ethical dilemmas they encounter. 41 This may limit the impact that formal ethical education has on students. Another possible explanation for the apparent erosion in moral sensitivity in students with clinical experience may be that as students progress into their senior years, they are prone to moral dilemmas. 42 A longitudinal study is needed to elucidate whether students who emphasise ethics learning have a higher moral sensitivity or if intrinsically morally sensitive students would commit to more ethics learning. Medical students’ commitment to ethics learning decreased with the academic year, indicating a need for a review of the curriculum and more rigorous ethical education in senior years. It also suggests a need to instil a sense of the importance of ethics education in senior medical students.
Limitations
Data should be interpreted carefully due to some methodological limitations. Firstly, this study was conducted during the COVID-19 pandemic, when clinical training was suspended in light of strict social distancing measures. The findings may be underreported and not generalisable to the conventional learning environment. Secondly, the study involved a scoping survey using a retrospective design that relied on self-reported, recalled estimates. Thirdly, the respondents were sampled from one tertiary institution, and there was a difference in the number of medical (n = 408) and nursing (n = 137) students who responded to the survey. The limited sample size of nursing students may further limit the generalizability of the results. The majority of the responding students (76.0%) did not have clinical experience; as such, the experience of pre-clinical students may be overrepresented in this sample.
Conclusion
This study has revealed significant differences between nursing and medical students in bioethical knowledge, moral sensitivity, and academic ethical awareness. These findings confirm the existence of variations in ethical attitudes and moral values between nurses and physicians, even during their undergraduate training. Given the community’s demand for morally grounded healthcare professionals, it is crucial for medical educators to foster the moral and character development of nursing and medical students.
The implications of this study on education are noteworthy. Firstly, ethics teaching should be integrated into both nursing and medical programs, with a diverse mix of students, including those with and without clinical experience. Secondly, there should be an increased and sustained emphasis on ethics education during the clinical years. Lastly, there should be a heightened focus on academic honesty, particularly concerning attendance and punctuality for medical students.
Future studies should aim to provide a qualitative understanding of how the experience of moral values evolves as students transition from the pre-clinical to the clinical stage of their education. Additionally, research should explore the implementation of interdisciplinary ethics education and examine how moral sensitivity evolves as students progress into fully-fledged nurses and physicians.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.