
Abstract
Background
Moral distress has negative effects on physical and mental health. However, there is little information about nurses’ coping strategies reducing moral distress.
Aim
The purpose of this study was to investigate the coping strategies of intensive care unit nurses reducing moral distress in Iran.
Study design
This is a qualitative study with a content analysis approach.
Participants and research context
The research sample consisted of nurses working in intensive care units of teaching hospitals affiliated to Tehran University of Medical Sciences. Samples were selected among eligible nurses by purposive sampling. Data were obtained through 17 in-depth, individual, and semi-structured interviews with 17 nurses. Graneheim and Lundman’s (2004) 6-step content analysis method was used to analyze the data. Data management was also performed by MAXQDA software version 20. The COREQ checklist was used to report the study.
Ethical considerations
This project was approved by the Ethics Committee of Tehran University of Medical Sciences. All ethical guidelines in research were followed.
Finding
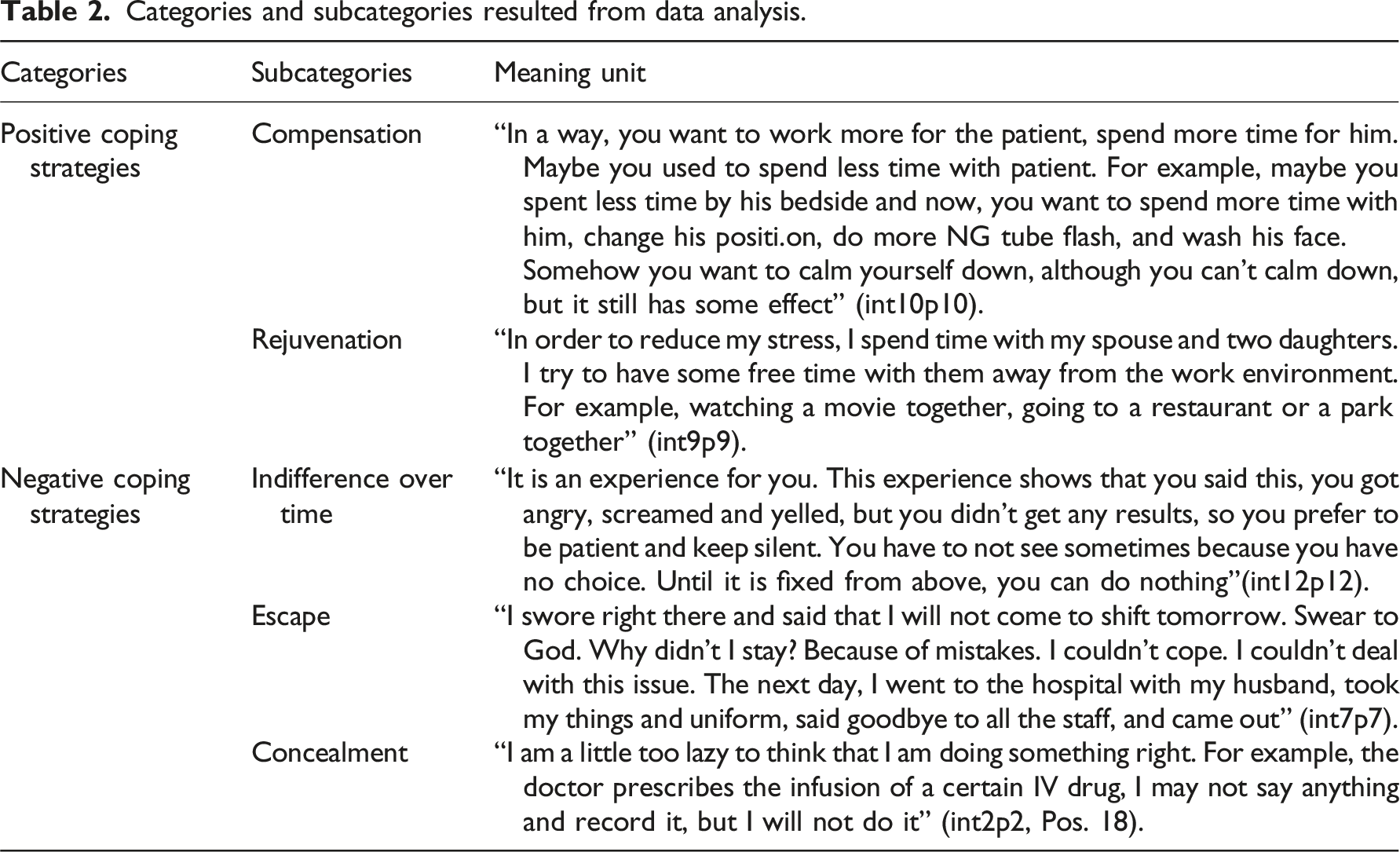
The data analysis resulted in the formation of two main categories of desirable coping strategies (with two subcategories of compensation and rejuvenation) and less desirable coping strategies (with three subclasses of indifference over time, escape and concealment).
Discussion
The intensive care unit nurses in dealing with ethical problems first try to solve the problem through discussion, but when they fail to resolve it peacefully, they resort to several coping strategies. Factors, such as increasing experience, lack of support from hospital managers and officials, poor communication between colleagues, the need to maintain hierarchy, fear of reprimand, and a sense of powerlessness, changed the nurses’ preferred strategies. It is important for managers to provide a blame/punishment-free atmosphere for expression of ethical experiences; a supportive atmosphere in which staff can engage in ethical discussions without fear of punishment. They should also provide opportunities for rest, rejuvenation, and adequate training for their employees.
Introduction
Intensive care unit is a stressful environment 1 due to high mortality 2 and morbidity, 3 and also daily exposure to moral crises. 4 Nurses working in intensive care units have a difficult and complex work environment. They are frequently exposed to work-related stresses such as end-of-life issues, prolongation of life with artificial support devices, and delivery of inadequate or futile care. 2 These nurses, despite recognizing their professional-ethical commitments, cannot comply with these obligations, 3 as a result they face moral distresses. Moral distress standards in intensive care units are significantly higher than in other clinical settings. 4 Healthcare workers working in adult intensive care units experience higher levels of moral distress compared to non-intensive care unit nurses. 5 Studies have shown that more than 80% of intensive care unit nurses experience moral distress, 6 because they often feel involved in the experienced conflict. 7 Moral distress can lead to feeling of hopelessness, anxiety and anger, emotional stress, 7 loss of independence, inability to perform delegated task, invisibility of the self,1,8 fear, failure and demoralization, extreme fatigue, loss of empathy and compassion in providing patient care, and guilt. It also has impact on family dynamism and personal life 9 and leads to loss of identity, insecurity and loss of meaning, and job leave.8,10 As a result, moral distress can have negative effects on nurses, patients and their families, and also can reduce the quality of patient care. 11 In order to have a healthy and sustainable workforce in the future, recognizing moral distresses and providing environments that facilitate the use of coping strategies by employees are important. 9
Over the past three decades, there has been a growing body of literature that describes moral distress as an important and prominent issue, which negatively affects intensive care nurses. These studies believe it is critical to pay attention to how intensive care nurses deal with moral distress.12–14 There have been several studies on ways that intensive care unit nurses deal with moral distress in recent years. In Forozeiya et al.’s 3 study, nurses’ method for coping with moral distress ranged from avoiding the situation by using techniques such as distraction and leaving the ICU, to addressing the problem by using problem solving skill, seeking social support, and performing positive reassessment. Nurses in the study of Henrich et al. 15 to deal with moral distress, used methods such as talking to trusted colleagues, not taking work problems to home, staying away from the causes of moral distress, suppressing emotions and feelings, leaving the ICU, drinking alcohol, exercising, and spending time with children. It should be noted that the majority of these studies have been conducted in developed countries.3,9,16–18 However, it is clear that ethics are influenced by many factors such as culture, religion, upbringing, and individual values and beliefs. These factors shape our ethical perspectives and influence ethical decisions that affect nurses and their patients. 19 This study was conducted to investigate the coping strategies of intensive care nurses reducing moral distress in Iran. The results of this study can be used to design interventions to increase coping ability and positive adjustment of nurses in the face of moral distress, and to promote their moral resilience.
Method
Study design
This is a qualitative-descriptive study with a content analysis approach. In qualitative research, researchers try to create meanings for phenomena and interpret them according to the meanings provided by people in their natural position. Content analysis is the process of systematic classification of data through which codes and themes are revealed.20,21
Research environment and participants
Participants of this study included nurses who worked in intensive care units (CCU and different types of adult ICU units) of teaching hospitals affiliated to Tehran University of Medical Sciences. After obtaining the necessary permissions, purposeful sampling was used to search for participants who had experienced moral distress in their workplace. In the purposeful sampling, the researcher is looking for those who have a rich experience and have the ability and desire to express their personal experiences. Therefore, the researcher visited the hospital and consulted with the head of units to introduce qualified nurses who are well informed and can provide the most complete and comprehensive information. In order to observe maximum variation in sampling, the researchers tried to include participants with diverse characteristics in terms of age, gender, work experience, education, and organizational position in the study. The criteria for entering the study included willing to participate in the study and being employed in intensive care units for at least 1 year.
Data collection method
In order to collect data, in-depth interviews with open-ended and semi-structured questions were used. In order to start the interview, the researcher introduced himself and talked about the purpose of the interview, in order to communicate and gain the trust of the participants. He first obtained their demographic information and then, by asking preliminary questions, establishing proper communication and gaining the participants’ trust, he provided the ground for a better and easier interview. Verbal consent was obtained from the participants to record the interviews. The interviews were conducted individually and in a face-to-face manner at a time and place agreed up on by the participants. Most of the interviews were conducted in person and some through WhatsApp video calls. The duration of interviews varied from 45 min to 120 min depending on the willingness of the nurses to continue the interview. Interviews were conducted by asking general questions such as: “Have you ever been in a situation where you knew something was morally correct but were unable to do it due to limitations?” “Can you describe that situation?” Later on, more specific questions related to the purpose of study were asked such as: “What effects have these situations had on your work and personal life? What was your reaction to these situations? How do you deal with these pressures and moral conflicts?” During the interview, in order to clarify the information and clear any ambiguities, the interviewer asked probing questions such as: “What do you mean by…,” and “Can you explain more about…”. Interviews continued until data saturation was reached. The data was collected between January 2021 and July 2022. The interviews were conducted by the corresponding author (SV), who was a doctoral student in nursing and had previously done qualitative research, before being recorded on a tape recorder and transcribed verbatim after each session. It is worth mentioning that all the interviews, coding, and classification processes were conducted under the supervision of expert professors in the field of qualitative research who have published numerous qualitative articles.
Data analysis
Data management and analysis was performed by MAXQDA software version 20, using Graneheim and Lundman (2004) contract content analysis method. 20 For this purpose, the interviews were first transcribed verbatim in the form of texts. The interviewer then listened to the recorded statements and read the written interview text several times to better understand the participants’ feelings and experiences. Then the parts related to the purpose of this study were extracted and used to form meaning units. Meaning units were then summarized, and codes were generated. The various codes were compared with each other based on differences and similarities and then, were divided into classes and subclasses. Data analysis was performed simultaneously and continuously with data collection. Data collection continued until data saturation was reached (until the collected data was a repetition of previous data and no new code and class was obtained).
Data accuracy and trustworthiness
In order to ensure the data trustworthiness, Lincoln and Guba’s criteria were used. 21 Credibility of the data was achieved by reviewing and confirming a sample of interview texts by participants (Member check) and reviewing the data analysis process by two researchers who were expert in qualitative studies but were not part of the study (Peer check). A long-term engagement with the research process (Prolonged engagement) was also maintained. Data transferability was determined by selecting the samples with maximum variation and accurately describing the details of the study in order to make the study process transparent. Dependability of the data was assessed by continuous comparative analysis of data and the triangulation of data sources. Finally, to achieve confirmability, the documents were recorded over time. Also, in the coding and classification process, in addition to the agreement of research team (peer debriefing), external observers were also asked to examine the coding process, extracted subcategories, and parts of the interviews, to identify similar and different cases than those of researcher’s understanding (External check).
Ethical considerations
All ethical considerations observed in this study included; obtaining permission from the Ethics Committee (IR.TUMS.FNM.REC.1399.182) of the University, providing explanations to participants regarding the purpose and method of study, how to collect information, the advantages and disadvantages of conducting the study, the voluntary participation in the study, recording of the interviews, confidentiality of personal information, the right to withdraw from the study at any time, and, if desired, availability of results to the participants on request. After the participants agreed to cooperate, the interview was conducted individually and with respect to the privacy of the individuals.
Findings
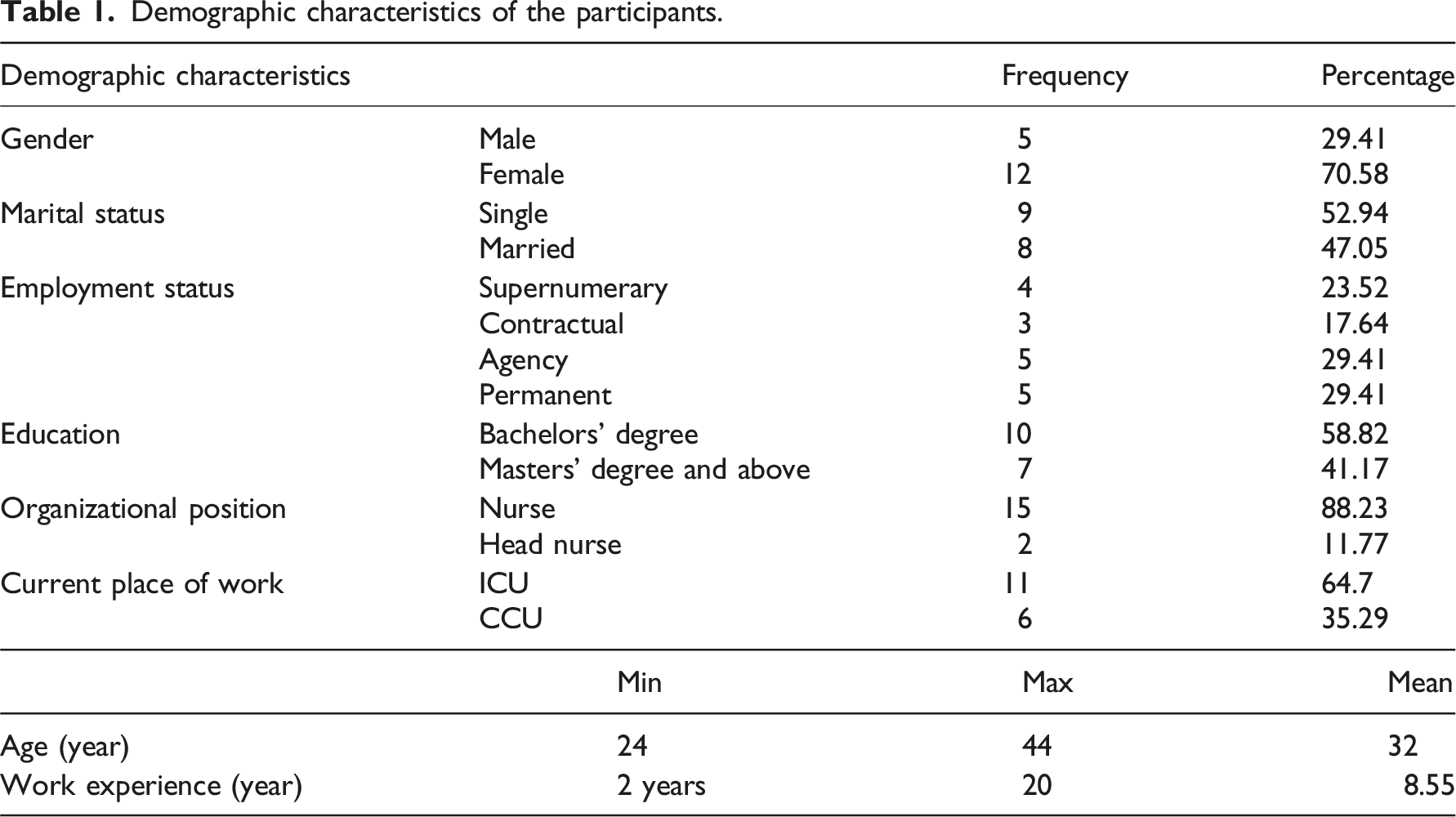
Demographic characteristics of the participants.
Sources of moral distress
In response to the first question of the interview, the nurses referred to some moral situations that had created moral distress in them, including: futile care (including unnecessary tests and surgeries, prescribing expensive drugs for end stage patients, and lack of resource allocation; non-observance of the principle of usefulness), not obtaining informed consent and not being honest with patients in providing information about the disease and treatment (non-observance of the principle of patient autonomy and honesty), discrimination in providing care (non-observance of the principle of justice), negligence and unprincipled care by colleagues (non-observance of the principle of nonmaleficence), and incorrect orders of doctors and confusion in execution (non-observance of the principle of nonmaleficence). Dealing with these ethical issues had disrupted the physical, mental, psychological, and social health of nurses.
Categories and subcategories resulted from data analysis.
The desirable coping strategies
Coping is defined as thoughts and behaviors used to consciously and voluntarily manage internal and external stressors. The desirable coping refers to coping styles or mechanisms that lead to reduced stress, increased well-being, and effective management of problems. 19 In this study, compensation and rejuvenation were two desirable coping strategies used by the nurses in response to moral distress.
Compensation
In this study, nurses used various methods to compensate for their moral shortcomings. They believed that these shortcomings and moral errors were irreparable, but they tried to do their best in other aspects of care and spend more time on patients. This method could give them a sense of relief. Some also tried to compensate for their mistakes by reporting their mistakes and negligence. They believed that by reporting errors and negligence, they could help create solutions and prevent similar errors in future. Some participants believed that due to the doctors-dominant atmosphere, in many ethical situations, their opinions are not taken into account and they are required to follow the doctor’s instructions. In this situation, they asked their patients for forgiveness in order to calm down, even if the patients were unconscious. Participant 2 in this regard stated: “Sometimes I even apologize to the patient. Believe me, there is nothing wrong with that. I say to patient that I had this problem, and I even treated you badly, so I'm sorry. I try to compensate for my mistake.” (Participant 2)
Another method of compensation, which was mostly used by nurses with less work experience, was to inform and give feedback to their supervisor. They felt powerless in the face of more experienced doctors and colleagues, so they tried to use the law and superior power to provide proper moral care in similar situations for patients.
Other participants tried to prevent the repetition of mistakes and compensate for them by increasing their scientific knowledge and learning from their previous unsuccessful experience. Using their past experiences, learning from the experiences of more experienced colleagues, reading scientific books and articles, attending ward rounds and doctors’ visits, and attending hospital trainings, workshops and in-hospital conferences helped them to gain more knowledge about moral distresses and better manage the situation in the next similar situations. Increasing their scientific knowledge assured them that they had done the right thing. “When you know you did not neglect the patient, this in itself can help to regain your spirit. You know that the patient’s low GCS is not your fault, and you have done the doctor’s instructions and what you are required to do and not neglected the patient.” (Participant 6)
Increasing scientific knowledge could also help nurses to reduce their fears and defend their moral beliefs.
Rejuvenation
Rejuvenation is a process of storing lost resources. Nurses in this study stated that multiple experiences of moral distress have made them tired, bored, unmotivated, and low in energy, so they needed to be away from their work environment for a while. However, the shortages of nursing staff in hospitals and high workload in intensive units caused them to even be deprived of sick leave. They tried not to take work issues home and rejuvenate themselves by staying away from the workplace and spending time with family and loved ones, exercising and having fun. They believed that rejuvenation would help them to gain the motivation they need to cope with future moral distresses.
They also calmed down and reduced their moral distress by turning to spirituality and prayer. “By reciting a few chapters of holy Quran or praying for the patient, I calm myself down and feel that God blesses the patient. I also hope that the patient would forgive me if I neglected him/her.” (Participant 15)
In addition to praying to God, talking with a trusted person who was usually a family member or co-worker, and expressing the moral problems in the ward helped to reduce the nurses’ moral distresses and psychological tensions.
Contrary to some nurses who reduced their moral distress by talking to their families, others believed that families do not understand the issues of nursing work and may blame them for their ignorance. They stated that, this not only would not help them to deal with moral distress, but also would escalate the problem, so they tried to leave the work issues in behind in the hospital and not take them home. In other words, they separated their work issues from family issues. Another reason for not taking about work issues at home was that, they did not want to be influenced by family members and their negative emotions.
The less desirable coping strategies
In general, the less desirable coping strategies do not help the healthy and effective management of one’s problems and in fact, lead to more stress, pain, difficulty, and low self-confidence. Some of these strategies may help in the short term, but in a long run, they do not help nurses to deal effectively with their problems or reduce their stress. 19 In this study, nurses used three methods of indifference, escape, and concealment to deal with moral distress. Since these three methods temporarily relieved the nurses’ moral distress but did not eliminate the cause, they were placed in the category of the less desirable coping strategies.
Indifference over time
Some of the nurses participating in this study tried to not interfere in others’ work and remain silent, due to the lack of support, lack of high work position and experience, rejection, retaliation, fear, and sometimes bad and inappropriate responses of those around them when defending the patient in moral situations. The nurses’ previous experience of dealing with such situations had caused them to regret their moral action, so they tried to reduce their sensitivity to moral situations and become indifferent to moral issues in order to protect themselves from moral distresses. “There is someone lower raking than myself at the unit and I knew he is doing something wrong, but when I told him he is doing something wrong, he lifted up his grads and argued with me, and even did not talk to me for couple of days. So, I said leave it, it not my business.” (Participant 1)
The nurses participating in this study believed that having a job position or responsibility gives them more courage to effectively manage moral problems and prevent them from happening again. Experienced nurses and nurses with nursing responsibilities also experienced moral distress.
Some nurses described the indifference as normalizing over time. They believed that the repetition of these situations over time made them stronger and more resilient. They experienced more moral distresses during their supernumerary work, when they had little experience. They said that they have eventually come to terms with these moral distresses over time, and since they could do nothing about them, they tried to ignore moral issues and try not to fix them.
Escape
In this study, some nurses decided to leave their job or department to deal with moral distress and not to experience that moral distress again. In addition to inexperienced nurses, the less desirable coping strategy was also experienced by experienced nurses. For example, participant 14, who had 20 years of experience and was the head nurse of the CCU, stated: “I myself have decided many times to resign from this job. Even now, if the conditions were right and it was possible, assuming that I could retire after 20 years of working as a nurse with difficult working conditions, I would leave right now. So, you can see how difficulties can kill you.”
Sometimes the nurses abdicated their responsibilities in order to relieve themselves of moral distress. For example, seeing a moral issue in the unit, they reported it to others, including the doctor, the superior, and the patient's companion, so that it could no longer be their responsibility. This way they escaped from responsibility.
Sometimes, when seeing that they could not change the situation, the nurses escaped from the moral situations by justifying their moral mistakes. They tried to experience less moral distress by thinking about the positive aspects of their work.
Concealment
Most participants in this study believed that in complex moral situations, no one supports them and also they are the ones who always become convicted, even if they acted ethically in the face of moral issues. Therefore, they believed they have to remain silent and only follow the doctors’ orders. If they thought the doctor’s instructions were useless or even harmful to the patient, they expected the head nurse and other nursing managers to provide them with the support they needed in the face of complex ethical situations. However, due to legal issues, sometimes they did what they felt was right for the patient, but did not record it in the patient’s file, or conversely, they did not do what they did not find useful for the patient, but they recorded it. In this way, they were both safe from legal issues and did not experience a sense of moral distress and its consequences. “... Again, we saw for ourselves whether, God forbid, our own experience really benefited the patient or not. We did it based on our own experience. We did what we thought was best, but in our report, we wrote what was ordered.” (Participant 11)
In this study, nurses used a concealment strategy based on their work experiences in order to help patients.
Discussion
Most nurses in this study believed that they do not have independence and decision-making power. In their opinion, some situations were beyond their power and they could not stand against the organization and doctors, and only carried out doctors’ orders. A strong sense of coping or dominance reduces the risk of moral distress and protects against stress, but a lack of dominance may evoke the sense of helplessness, and possibly affect the way nursing staff experience moral and ethical problems, which increases the stress related to guilty conscience. 22 In this study, when nurses saw the situation as uncontrollable, they used a variety of coping strategies to deal with the situation, so that each nurse had a set of strategies, but sometimes their method changed over time. For example, at first, they tried to solve the moral problem, but when they saw that it was ineffective or their values were ignored, they withdrew from their decision to take moral action. Lievrouw et al. 7 stated that individuals change their methods of managing moral distress depending on personal experiences or perceived work and team culture. Forozeiya et al. 3 instead of the desirable and the less desirable coping strategies, talk about concepts such as Turning away and Turning toward moral distress. She believes that nurses’ coping with moral distress is a dynamic situation between avoiding, communicating, and moving along with it.
One of the desirable coping methods used by the intensive care unit nurses in this study was compensation by eliminating shortcomings, making efforts in other aspects of care, asking for forgiveness from the patient, seeking help from the law and superiors, learning from the past moral situation, and increasing their scientific knowledge. Nurses felt remorse and guilt when they failed in moral situations, so they tried to spend more time in other patient care or seek forgiveness from patient. This coping strategy is not seen in other studies. Asking for forgiveness is one of the tools of compensating for non-pecuniary damages that play an important role in relieving mental pain, improving relationship with the one who caused mental pain, 23 and freeing the wrongdoer from feelings of regret and guilt. 24 Asking for forgiveness is a reflection of society’s culture. 25 Factors such as fear of legal consequences and patient’s negative response to the request of forgiveness make the treatment team cautious about asking for forgiveness. But culture, education, and personality traits are factors that make it easier to ask for forgiveness or receive it. 26 It is therefore essential to create an honest, fear-free, blame-free, and non-judgmental work environment in hospitals that allows expression of mistakes and promotion of forgiveness seeking.
Another way of compensating for moral mistake was to describe the incident to a higher authority to deal with a moral issue. In this study, nurses who thought they do not have power, were mostly younger and less experienced nurses, so they tried to resolve the moral issue through law and superior’s power. They believed that even if they commit negligence and harm the patient, they should inform their superiors in order to help create solutions and prevent these errors from happening again. This is consistent with the findings of Lievrouw et al.’s 7 study, which reported that nurses and young physicians do not always have enough self-confidence to express their moral beliefs, so they delegate independence to the supervisor. In the study of Jansen et al., 22 nurses by delegating their responsibility to supervisors and other healthcare professions, protected themselves from moral conflicts. However, they may later prefer different ways of coping method in their careers or in a different environment.
In this study, most nurses stated that they try to learn from past moral situations and increase their knowledge to prevent the recurrence of moral distress. Increasing their knowledge also helped to alleviate their fears and gave them more courage to express their views and opinions in the face of future moral issues. In addition, increasing knowledge helped them to avoid having a sense of guilt in certain moral dilemmas and reduce moral distress, so they tried to achieve this goal in various ways. In Forozeiya et al.’s 3 study, positive reassessment (i.e., focusing on personal growth to find meaning in situations) was used by more experienced nurses. These nurses re-evaluated the situations and thought about how they could learn, grow, and move forward from moral situation. Most nurses in this study learned from their more experienced colleagues and referred to ward rounds, workshops, and in-hospital conferences as important sources of learning. Nurses in the Helmers et al.’s 27 study also talked about communication with senior team members, and recommended peer support programs for personal learning to novice nurses. The ability to re-describe the event in a group with a structured and guided explanatory framework ensures that each nurse compares his/her feelings and coping strategies with others. This experience can be useful when dealing with moral distress. 17 It seems that providing an atmosphere in which, novice nurses could talk to more experienced nurses and physicians about their moral experiences without being humiliated or blamed can help to prevent or successfully resolve moral distresses.
Another desirable coping strategy used by nurses in this study was to separate work issues from family issues and rejuvenate by using adequate rest and spending time with loved ones having fun activities. Although participants in the present study tried not to think about ethical issues at home, these thoughts were constantly and involuntarily recalled in their minds, even during rest. According to nurses, rejuvenation helped them to temporarily distance themselves from the moral issue and return to work with a more open mind and power. However, due to the current shortage of nursing staff in Iran, 28 they not only are deprived of annual leave, but also they are forced to work overtime, which gives them no time to rejuvenate. In this regard, nursing managers said they were working to restore nurses' lost strength by moving nurses to other wards. Temporary absence from ICU gives nurses time to recover and rejuvenate. Creating a process by which nurses and other healthcare professionals can perform non-clinical tasks in the ICU or work outside the ICU for a short period of time can reduce burnout and stress, improve job satisfaction, and increase mental health. 29 Consistent with our findings, nurses in the study of Boulton et al. 30 to cope with moral distress used methods such as walking in open spaces, breathing fresh air, exercising, and drinking alcohol. Self-care methods such as healthy diet, sleep and rest, spending time in nature, physical activity, meditation, mindfulness, yoga, massage, music, art, and therapy with pets reduce stress and moral tension and promote ethical resilience of health care professionals. 31 Another coping method used by nurses in this study was to turn to prayer, which was in the category of rejuvenation. A close relationship with God can help people cope with stressful situations, including moral distress. 32 People with stronger belief have more access to spiritual and religious coping strategies when faced with stressful situations. These coping strategies can reduce their stress and increase their mental and physical health. 33 In the study of Shamsaei et al., 34 a negative and significant correlation was observed between spiritual health and severity of moral distress in nurses. This means that the higher the nurses' spiritual health is, the lower their moral distress will be. Spiritual health is an effective parameter in reducing nurses' moral distress. Therefore, it is suggested to pay more attention to the spirituality of nurses in promoting nurses’ health and reducing their moral distress.
In this study, nurses expressed differing opinions about talking to co-workers and family members about morally tense situations. They chose someone to talk to who was trustworthy and understanding. Nursing co-workers are often chosen as sources of support, because they can identify and understand the moral distress non-judgmentally. Peer support makes nurses perceive moral distress as a shared experience; an experience that mostly stems from nursing practice in ICU than personal deficiencies or performance. 35 This would be much more beneficial if this support is also provided by nursing managers. 3 Talking to each other, using each other’s experiences and reaching an agreement on certain issues can relieve stress and prevent burnout. This finding is supported by other studies.30,36 In the study of Boulton et al., 30 the most common and valuable of coping strategy in response to moral distress was talking informally with co-workers, such as chatting in the coffee room. The authors of this study mentioned individualized informal support as the most valid, accessible, fastest, and most efficient intervention to reduce moral distress. Fantus et al. (2024) stated that communicating with trusted colleagues and peer support helped enhance novice clinicians’ self-confidence and professional development, and is an effective coping strategy for reducing moral distress. 36
In this study, some nurses, especially less experienced nurses, used the less desirable coping strategies to deal with moral distress. One of these methods was to become indifferent to moral issues that had occurred over time and learn from previous unsuccessful experiences. Hancock et al. 18 also showed that one of the most destructive ways for nurses and physicians to deal with moral distress was to isolate themselves from the patient and stay away from colleagues. In the study of Boulton et al., 9 nurses withdrew from interacting with patients/families to protect themselves. In the study of Henrich et al., 15 nurses also said that in order to cope with moral distress, they invest less in their work and try to distance themselves from the causes of moral distress and hide or suppress their emotions so that they do not look weak. In the present study, nurses concealed their ethics due to lack of support, futility of their efforts to stand up for their values, concern about being condemned, and fear of negative reaction from the other party. They said that in ethical decisions, the final decision is made by doctors, their moral values are often ignored, and whenever they insist upon something they are condemned by the managers, most of them were accustomed to this issue and had come to terms with it. Similar to this result, a study by De Brasi et al. 17 revealed that newly hired nurses avoid engaging with medical staff due to the lack of courage and fear of negative reactions.
Leaving the profession or leaving the intensive care unit was another less desirable coping strategy used by nurses to deal with moral distress. According to literature, negative experience of moral distress affects nurses’ career decisions and causes some nurses to question their future in intensive care unit.27,37,38 In one study, even young staff looking for jobs in intensive care unit changed their carrier after experiencing and trying to cope with moral distress. 9 In this study, nurses stated that, they thought about leaving ICU or their job in order to avoid being in such situations again. In the study of Forozeiya et al., 3 some inexperienced participants stated that they thought about leaving nursing profession or their specialty due to the lack of support from managers. It seems that inability of nursing managers to support their employees is one of the reasons for moral distress in nurses. 9
Some of the less experienced nurses in this study, due to their perceived inability to make ethical decisions, tried to find odd reasons to justify their immoral behavior, and by doing so, tried to calm, convince, and satisfy themselves. Others used a concealment strategy to do what they thought was right without recording it in patient’s file. They stated that they avoid documenting their moral actions due to the fear of legal issues, but keep their conscience clean by doing the right thing. This coping strategy is not found in other texts either, so no comparison could be made in this regard, which highlights the need for more in-depth studies on this topic in the future.
Limitations
Participants in this study were nurses from public hospitals and may not represent the experiences of nurses who work in other settings, such as non-governmental or non-educational hospitals. The findings of this study cannot be generalized to other societies due to its qualitative nature.
Implications and recommendations for practice
The results of this study showed when the desirable coping strategies are not effective, nurses turn to the less desirable coping strategies to deal with moral distress. To prevent moral distress in nurses, it is necessary for managers to provide a supportive atmosphere for discussion about moral experiences without fear of blame and punishment, and also support nurses during inter-professional moral discussions. Strengthening the relationship between physicians and nurses, teaching desirable coping strategies, providing training courses tailored to existing ethical issues, and providing rest times and a place away from the stresses of intensive care unit to recover and rejuvenate can help nurses to effectively deal with moral distress.
Conclusion
The data obtained from this study showed that nurses working in intensive care units in Iran first try to solve moral problems through discussion in the face of moral situation, but when they fail to solve it peacefully, use the desirable and less desirable coping strategies. In this study, nurses’ preferential strategies sometimes changed over time with increasing experience. For example, the unsuccessful experience of solving a moral problem over time led to the indifference of some nurses toward solving such issues. Several coping strategies such as trying the best in other aspects of cares, apologizing to the patient, justifying immorality, and concealing non-ordered but morally right actions are specific to this study and cannot be found in other studies. The less desirable coping strategies often resulted from nurses’ lack of power in the doctor-dominated medical system, the need to adhere to hierarchy, fear, lack of support from officials, and a lack of proper communication between the treatment team. Managers need to first identify nurses’ preferred coping strategies by encouraging nurses to discuss their ethical experiences in a blame and punishment-free atmosphere, and then by teaching desirable and active coping strategies and supporting nurses in ethical discussions, reduce their moral distresses and related harms. In addition, by providing time and space for rejuvenation, managers can help nurses to regain their lost strength. Providing a work environment in which nurses can express their views without fear, offering training courses tailored to existing ethical issues, holding meetings with cordial conversations with colleagues, especially experienced colleagues, and ultimately supporting nurses in ethical issues are among the duties of nursing managers.
Footnotes
Acknowledgements
This article results from a research project approved by the Tehran University of Medical Sciences and Health Services. The authors of this article had no conflict of interest in publishing this article. The authors would also like to thank the Vice-Chancellor for Research and Technology of Tehran University of Medical Sciences for the ethical approval of the plan (Approval ID: IR.TUMS.FNM.REC.1399.182) and the participants who helped us in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.