
Abstract
This paper examines place-specific factors affecting geographies of innovation, that is, the transfer of research from the laboratory to bedside in the healthcare sector in four European bioscience regions. These regions are Medical Delta (MD; Leiden, Rotterdam and Delft, Netherlands) Oxford and the Thames Valley (OTV; UK), Biocat (Catalonia, Spain) and Life Science Zurich (LSZ; Switzerland). Evidence is drawn from the European Union-funded Healthcare Technology and Innovation for Economic Success (HealthTIES) project (2010–2013). The analytical framework, the HealthTIES Innovation Cycle, is organised into resources (inputs), innovation system elements and outcomes. The paper shows that each region represents different positions within international value chains of innovation in the healthcare sector. They range from the highly research intensive but with relatively less in the way of commercial exploitation location (OTV) to the less research intensive but with more commercialisation (LSZ).
Introduction
In the study of innovation geographies, place-specific factors come together to enable firms and other kinds of organisation to undertake radical, new and/or incremental product, service and process development. As Feldman (2014) points out, while investments in innovation in certain places yield jobs, growth and prosperity, similar investments in others fail to produce the desired local effects. The focus in this paper is on how innovation is organised at the local level in the healthcare 1 field. In so doing, we identify the elements of innovation cycles and the resulting outcomes in often internationally organised innovation value chains, where value is realised in these locales.
Our study draws on data from a recently completed European Union (EU) FP7 funded study (2010–2013) – Healthcare Technology and Innovation for Economic Success (HealthTIES). The organising framework for analysis used is the ‘Healthcare Technology Innovation cycle’. The study is based on four European regions: Medical Delta (MD; Leiden, Rotterdam and Delft, Netherlands) Oxford and the Thames Valley, (OTV; UK), Biocat (Catalonia, Spain) and Life Science Zurich (LSZ; Switzerland), along with an emerging region, Debrecen (Hungary). 2 The regions are all leading centres in healthcare innovation in their own country.
However, ‘regions’ are complex entities differing in scale; they are not only administrative entities but can also be functional regions built for a particular purpose. The EU’s own concept of ‘region’ is flexible. ‘Regions’ are defined in the broader sense, such as Länder, communities, autonomous communities, departments, provinces, counties, metropolitan regions and any other political entity with relevant competences to accomplish their engagements. 3 Our ‘regions’ vary in size and in the composition of their research and industrial bases, as well as in their administrative and functional status. Therefore in the analysis, we consider all parallel developments in order to reflect on diversities of value chain development at a given moment in time, rather than on systematic comparisons.
Within this varied geographic context, we address the following research question: how has the innovation cycle in the healthcare sector developed in each of the four regions? We argue that it is necessary to look beyond just universities and the biomedical industry sector to map the elements of the cycle in order to account for individual regions’ differing strengths, weaknesses and prospects. To contextualise the research question, we define the innovation cycle and examine explanations for particular geographies of innovation. This is followed by the profile of each of the four regions, the methodology used to assess performance and the data analysis. Finally, some conclusions are drawn on what has been learned about regional differences and the implications for prospects for future developments.
Innovation cycles and innovation systems in healthcare at the local level
The Healthcare Technology Innovation cycle connects engineers and medical professionals, scientists and entrepreneurs, and developers and end-users (medical doctors and patients; Figure 1). The concept of an innovation cycle implies a virtuous circle of interaction. The European Alliance for Innovation defines an innovation cycle as representing a framework for classifying the different stages of innovation and the stakeholders related to the development of innovation. 4
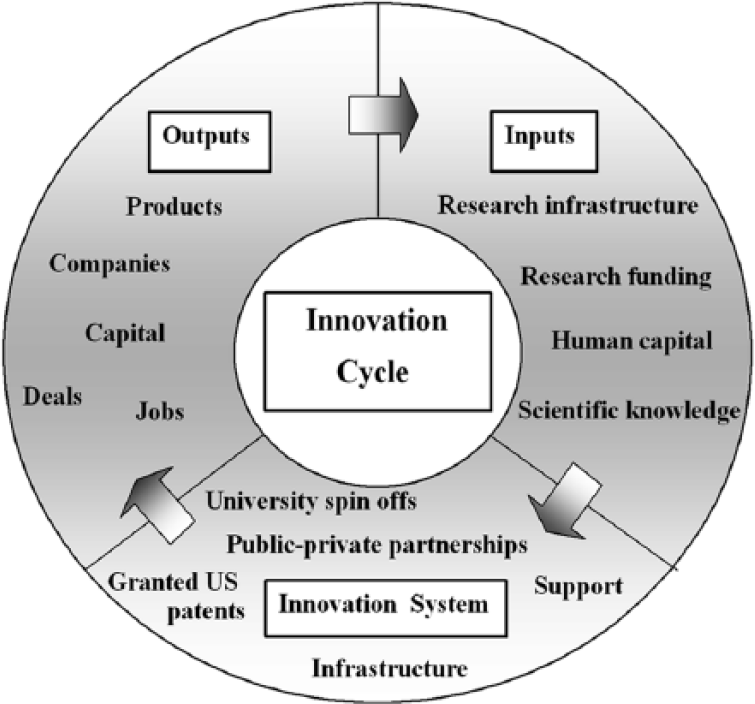
Healthcare Technology and Innovation for Economic Success Innovation Cycle.
The healthcare innovation cycle contains three stages and numerous stakeholders. The first specifies resources (inputs) (e.g., the science in the research base, research funding, human capital). Central to this is the national context. In the second, the innovation systems most closely resemble that of a sectoral innovation system (SIS) (Malerba, 2002, 2005). It includes technology transfer capacity building (e.g., infrastructure and support for technology transfer). The third stage includes outcomes (e.g., new firms, jobs, drug developments advances in diagnostics, therapeutic and other technologies) rather than production capabilities and links to customers, which are elements in ‘global’ commodity chains that concern interconnections within and across varied geographical scales (see Birch, 2008).
Within each element of the innovation cycle are stakeholders – governments, universities and various other private sector organisations. However, as it is a cycle, this process is not linear. Feedback loops involving interactions between the different elements (Kline and Rosenberg, 1986; Rothwell, 1994) contribute to the vitality of individual cycles.
A limitation of the healthcare innovation cycle concept is the lack of a sense of place and a broader geography of innovation, which Cooke (2005) and Swiss Biotech (2016) refer to as an ‘innovation value chain’ in the sector. The analytical agenda in this paper is that of a place-based analysis taking into account where key components of internationally organised healthcare innovation value chains are located (i.e., the whole spectrum of innovation from resources to outputs). This approach resonates with different typologies of systems involving interconnections between different geographical scales.
Birch (2017) applies the value chain concept to examine where innovation happens in the life sciences, and considers where and how value circulates, and who captures the value produced. This approach is useful because, by implication, the local geographical dimension is where value creation and exploitation takes place. To explore that aspect we draw on research evidence to ‘ground’ the innovation cycle concept.
In the healthcare sector, key inputs are scientific knowledge, research funding, human capital and research infrastructures. Each of these is connected to research universities, which are often the central players in geographies of innovation. A key feature of the bioscience sector is national funding for research, whether it is the National Institutes of Health in the USA (Breznitz and Anderson, 2006), federal/central government agencies in Europe (e.g., Switzerland), the Medical Research Council in the UK or the EU under the Horizon2020 Programme. 5 National is the dominant level of provision of resources for the production of scientific knowledge (e.g., research funding, infrastructure, the education and training of human capital) investing in scientific frontiers (Mazzucato, 2013), as well as determining other property rights to knowledge important in the bioscience sector. 6 In some, the regional level is the primary source of such resources (e.g., Länder in Germany, Cantons in Switzerland). These regional entities facilitate technology transfer through layers of policy linking national and local levels. Other organisations (e.g., firms, research institutes, hospitals) also provide knowledge and support the infrastructure for innovation, such as science parks and incubators.
The starting point of the HealthTIES project was that the chosen regions each had strong science bases (scientific knowledge) that underpinned the development of the healthcare sector. Coenen et al. (2004) find that the dominant knowledge base of the bioscience sector is connected to the science base as a source of knowledge. The sector is characterised by strong spatial concentration around nodes of excellence, such as in the four HealthTIES regions. These are then themselves interconnected through international networks. Inputs are analytic knowledge, while companies use sources of synthetic knowledge such as hospitals, specialised services, suppliers and customers for testing, (re-)designing or commercialising new discoveries and inventions. Knowledge combinations are relevant in both cases.
Different mixes are found in biotech generally in technologies, inputs and demand (Tödtling and Trippl, 2015). Moreover, not all local analytical knowledge bases are the same in healthcare as in the specific case of biotech because of different levels of research funding priorities, specialisations, engagement in research consortia and so on. In addition, synthetic knowledge where innovation takes place mainly through the application of existing knowledge or through the new combination of existing knowledge, for example in public–private partnerships, is also a key element of healthcare innovation value chains. These varieties of innovation pathways are key to understanding our cases.
Implicit in this cycle schema embedded in the concept of resources (inputs) is the idea that there are a variety of knowledge transfer mechanisms in place in a locality. One example is the interaction between individuals and organisations in clusters in spreading knowledge and expertise, while keeping the process spatially bound (Breschi and Lissoni, 2001). Birch (2008: 87) in a critique of cluster approaches cites Malmberg (2003), Malmberg and Power (2005) and Malmberg and Maskell (2006) stating that, ‘it is important to explore both the concentration and dispersal of innovation across multiple scales’. This point is reinforced by Moodysson and Jonsson (2007), who also find that while functional proximity facilitates technology transfer, global knowledge collaboration is indispensable for most dedicated biotech firms. This raises the issue of which actors and under what circumstances local collaborations are important.
A further category of resources in healthcare is high skill human capital. This is particularly associated with innovation-led entrepreneurial activity (Audretsch and Keilbach, 2005), with entrepreneurs being drivers of innovation. Fritsch and Wyrwich (2014) argue that where there are concentrations of the highly skilled, which is often related to a high-quality science base. A local environment has other skill sets including those of intermediaries (Howells, 2006), such as technology transfer officials who mediate in the technology transfer process, for example by supporting the formation of new firms or connecting the researchers to the next stage in the cycle, that of innovation systems.
Basic to the innovation cycle in Figure 1 is the capacity in the second stage for sustaining the development of the local elements in the internationally organised innovation system. The systems literature includes an increasing number of types of system that comprise a broader framework of innovation geographies. In general, the systems concept embraces stakeholders, public and private sector actors, and the networks that link them (see, for example, Coenen et al., 2006; Woolthuis et al., 2005). These include national innovation systems (NISs) (e.g., Freeman, 1995; Lundvall, 1988, 1992; Nelson, 1993), regional innovation systems (RISs) (Cooke, 1992), sectoral systems of innovation (Malerba, 2002, 2005) and varieties of business ecosystems, for example, entrepreneurial ecosystems (Spigel, 2015).
The healthcare sector as it appears in the innovation cycle has some elements of a SIS but is not confined to one product group. Breschi and Malerba (1997: 131, in Coenen et al., 2006) define a SIS as ‘a system (group) of firms active in developing and making a sector’s products and in generating and utilising a sector’s technologies’. Coenen et al. (2006) suggest that the boundaries of a SIS are defined by a certain product group with a dominant knowledge base.
In the SIS concept, policy makers (central government and local authorities) appear as agents of change in the system alongside firms and non-firm organisations (such as universities or financial institutions), as well as organisations at lower (research and development (R&D) department) or higher levels of aggregation (e.g., firms’ consortia) and individuals (Malerba, 2002). The absence of formal administrative boundaries in the concept is relevant to the healthcare sector analysis, as although we discuss evidence of activity at the local level, the overall context is that of an internationally organised field (see Coenen et al., 2004).
While the RIS approach does recognise interconnections at various spatial scales, it is essentially a territorially bounded system (Coenen et al., 2006) but with extra-local linkages. Asheim and Coenen (2005: 1174) define the RIS as ‘interacting knowledge generation and exploitation subsystems linked to global, national and other regional systems’ that may stretch across several sectors in the regional economy. The capacity of the constituents of a regional economy allow for the support of science and technology discoveries and their application, for example through networks between local stakeholders (e.g., entrepreneurs, intermediaries) and infrastructure, for example, science parks (Casper, 2013).
However, a weakness in the HealthTIES innovation cycle, as in other innovation systems approaches, is that entrepreneurs and enterprises appear in the system and output stages of this cycle, rather than in inputs as actors with agency at the local level (Autio et al., 2014; Feldman and Francis, 2006; see also Sternberg and Müller, 2005 on the RIS). Feldman (2014) describes entrepreneurs as a missing element in the discussion of innovative places, while Hekkert et al. (2007: 421) argue, ‘Entrepreneurs are essential for a well functioning innovation system’. Indeed, entrepreneurial activities, together with knowledge development, knowledge diffusion through networks and market formation, are among the key elements of innovation systems. While university spin-offs appear in innovation systems, only a few such companies are in biosciences and many of them remain small. It is often non-university biosciences spin-offs that are more active players in innovation systems (see Cooke, 2005).
System approaches neglect how universities and research establishments change in response to changes in technology, markets, public policy, etc. In countries such as those in the HealthTIES consortium, incentives are put in place to create synergies between various research organisations, firms and individuals. Many have resulted in public–private partnerships designed to exploit commercial opportunities. However, these do not occur at the same rate or in the same form in our four locations.
The need for such critical analysis is made by Carlsson et al. (1999) who asked the following.
What is the appropriate level of analysis?
How is a system delineated and which actors form the components?
What are the key relationships that need to be captured so that the important interaction takes place within the system rather than outside it?
Following from this, further questions arise: how is the performance of the system to be measured? Is this measurement to be at the system level rather than at the component level (in this case at the regional level)? Analysis here takes each element of the innovation cycle in turn.
In summary, the review of innovation systems provides various frameworks to work in evaluating the structure and outcome in different locations. The definition of location, sector and technology is critical but not simple in the healthcare sector. By nature, this field is not bounded – collaborations often transcend local geographic boundaries, firm boundaries, etc. The field is also dependent on multiple disciplines and technologies, including non-science areas such as law, public health, social science and management. Studying this complexity requires rich datasets; often studies focus on one technology (e.g., rDNA), one drug (e.g., Herceptin), one discipline/process (e.g., molecular biology), one firm (e.g., Genentech) and one university (e.g., Stanford).
This paper is an ambitious endeavour to reflect on local regional competitiveness and shortcomings to understand how leading centres in Europe stack up with regards to our understanding of inputs, systems and outputs in the healthcare sector. Direct comparisons are not possible, given the population size of each country and history. However, specialisations of each and common threads that cut across these regions can be noted. These observations imply significant possibilities for policy from organisational, local to regional level in order to target synergies.
Study context: The four European regions
The USA is and has been the leader in translational research in the healthcare sector (Bagchi-Sen et al., 2004; Kenney, 1986a, 1986b). In Europe such work is noticed in the UK, Germany (see, for example, Cooke, 2005, 2013) and Switzerland (Gebhardt, 2015). Other countries (e.g., Israel, India) have strong science bases but are yet to deliver effective support for this process (Breznitz, 2013). Here we consider the national and regional (local) policy contexts in the four European regions.
The four key bioscience regions of the ‘Healthcare Technology Innovation cycle’ – Biocat, Medical Delta (MD), Oxfordshire and the Thames Valley (OTV) and Life Science Zurich (LSZ) – are what Cooke (2005) has described as bioscience megacentres, albeit on a smaller scale than ones in the USA (such as Boston or San Francisco). Their locations are shown in Figure 2.
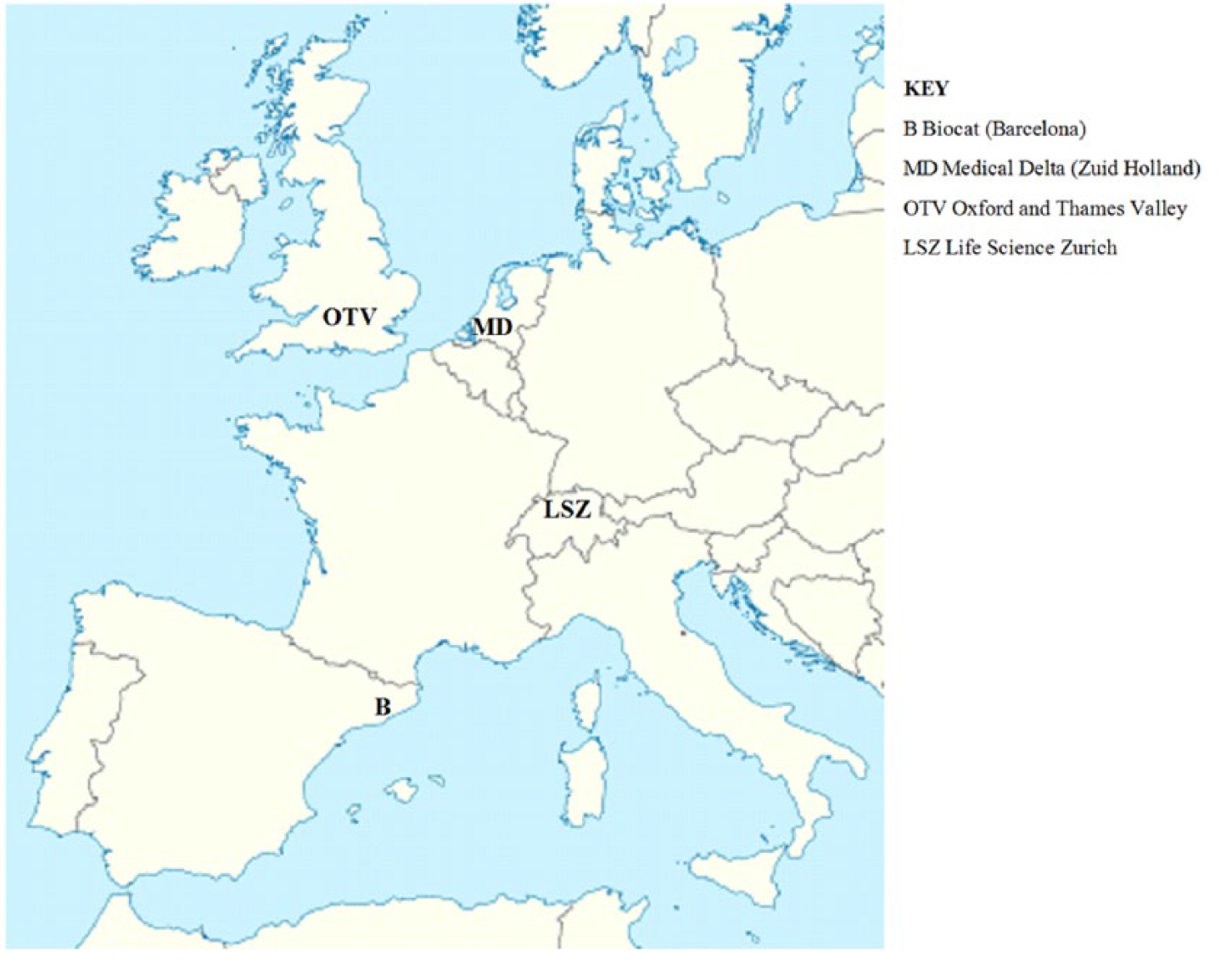
Map of Western Europe showing Healthcare Technology and Innovation for Economic Success regions.
Three are similar in population size. In 2010–2011, Oxfordshire and the Thames Valley (OTV) had a population of 1.1 million, Biocat (Barcelona municipality) 1.6 million, the LSZ canton of Zurich (2010) 1.6 million and MD, the Zuid-Holland region (2011), 3.5 million. 7 MD includes three urban centres (Rotterdam, Leiden and Delft), each with a major hospital. Although a weakness of the HealthTIES methodology is that it is not corrected for population size, in our analysis we do in part use to some indicators factored by population size.
The strengths of the science bases and for translational research are shown in Supplemental Appendix A. This shows the main research institutes in each, confirming the rationale for comparison even though the evidence collected after the regions were chosen suggests that in some respects they represent different positions in more global innovation/value chains (Birch, 2008; Cooke, 2005). MD, OTV and LSZ have their research integrated with hospitals so it is difficult to separate out institutes. The Barcelona list is more truly one of research institutes, as they are less integrated in the region.
MD and LSZ have regional structures created to promote translational medicine and are most obviously where the whole innovation cycle is organised at the regional level. In both, universities work with private sector engagement as a main driving force in economic development. However, while universities are funded regionally by Switzerland’s cantons, they are nationally funded in the Netherlands. They differ in the availability and type of resources, in the key elements of innovation cycles and, as a result, in outputs. They are also dissimilar in the extent to which national governments set sectoral innovation agenda and incentives.
OTV and Biocat have clusters of commercial activities that have grown around their major universities and hospitals. Examples of major national and regional policy initiatives are shown in Table 1.
Recent policy initiatives in each country and region.
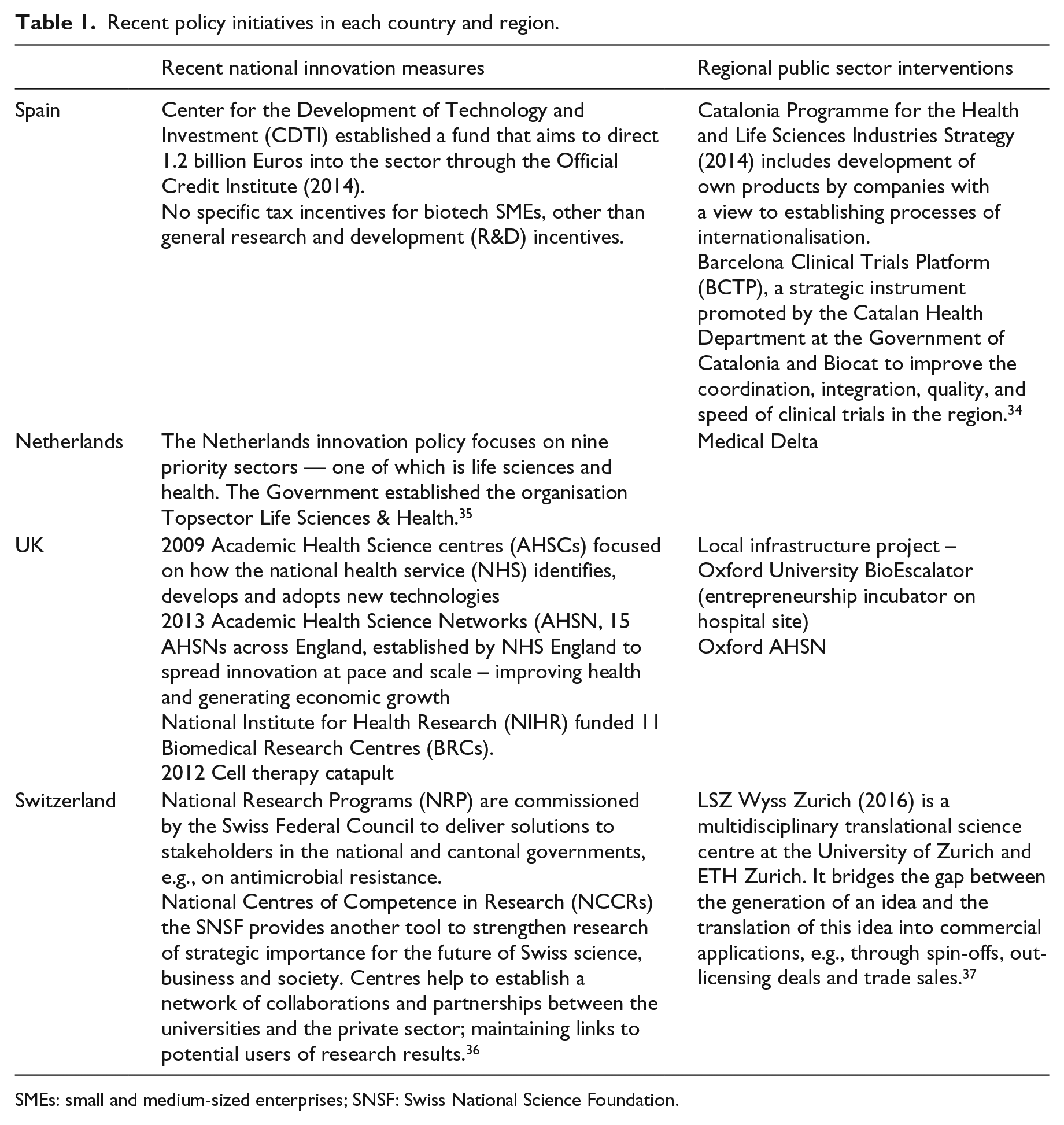
SMEs: small and medium-sized enterprises; SNSF: Swiss National Science Foundation.
Spain
Spain has one of the ‘world’s leading centres of biotechnology research’ but lags behind in its technology transfer system and creation of new firms (Wharton, 2014). 8 Research in the life sciences is funded through the Spanish Research Council, 9 which is one of the largest in Europe. Biology and biomedicine are one of eight target areas. It has commercialisation, transfer of results to the corporate sector and creation of technology-based companies as three of its main functions. While it has a robust science base, there is evidence that it lacks interactions between different organisations.
In 2014, Spain adopted the Israel model for designing an entrepreneurial and business model based on innovation. The country had been losing its position in the world rankings of R&D activity. The sector had been especially hurt by cuts in public subsidies and the shortage of tax incentives for research, which translate, for example, into fewer patent registrations. Comparatively weak policy efforts to incentivise knowledge and technology transfer compared to incentives to foster research have further hindered progress. Spending on R&D (over half by firms) is concentrated in three main centres – Madrid, Catalonia and the Basque country, with Catalonia being one of the country’s national biotechnology hubs, with 20% of all companies in the sector. 10
In Catalonia, the Programme for the Health and Life Sciences Industries 11 is one of Seven Strategic Industrial Sectors, published by the Government of Catalonia. Not explicit in Switzerland or the Netherlands, but increasingly the case in the UK, the strategy sees a key role for the hospital sector driving innovation in pharmaceutical and medical technologies. At the regional level, Biocat is the main organiser of the life science innovation cycle. Biocat was established in 2006 by the Government of Catalonia and Barcelona City Council. Its aim was to facilitate networking among biotech and pharma companies, research institutions/universities and an administration that fosters the biotechnological and biomedical sector in Catalonia. 12 Biocat is led by a biomedical network that monitors what is happening in the sector, but has more resources and works closely with universities and hospitals. Start-up finance is available through ESBAN, an association of business angels.
The Netherlands
Science policy in the Netherlands has an increasingly close relationship with innovation policy. 13 What drives the success of the Dutch Life Science & Health sector is knowledge-sharing and close cooperation and collaboration between companies and research institutions, with full support of the government. 14 The government has ‘actively supported and co-funded a R&D infrastructure based on the concept of open innovation and long-term public–private partnerships’ while investing in the strong research base. These partnerships cover the entire life sciences value chain: they range from basic research to product and business creation. In cases where they address human health, they reach all the way from bench to bedside. They include all Dutch university medical centres, together with their associated universities.
Medical Delta was established in 2006 by the Delft University of Technology (TU Delft), Erasmus Medical Centre, Erasmus University, Leiden University and Leiden University Medical Center, and the City councils of Delft, Leiden and Rotterdam. MD is coordinated through its website. 15 Its aims are to realise breakthroughs in medical sciences and healthcare, to develop novel technologies and to fuel related economic opportunities through university–industry linkages. MD is a medical technology cluster, home to a large number of biotech firms with stakeholders such as companies, business parks and local government.
The United Kingdom
The UK’s strength in life sciences lies in it having ‘4 of the top 10 universities in the world, 19 of the top 100 universities, a stable of quality service providers, world class charitable supporters of the industry and a rich heritage of globally recognized medical research’. 16 The country has one of the strongest biotech industries in Europe. It has a strategic approach to life sciences similar to that of the Netherlands. There is a complex policy structure for funding involving research and innovation in universities, research centres and, increasingly, hospitals. The UK government’s 2011 Strategy for UK Life Sciences supports companies through every stage of the product life cycle. It highlighted weaknesses in the UK healthcare innovation cycle for R&D funding for translational activities or the ‘translational funding gap’ 17 in 2014. 18 The Office for Life Sciences (OLS) is part of the Department of Health and the Department for Business, Energy & Industrial Strategy, and it ‘champions research, innovation and the use of technology to transform health and care service’. 19 The regional level has been abandoned as an organising authority in England with Local Enterprise Partnerships (LEPs) now responsible for sector-specific policy intervention (if any; Lawton Smith and Waters, 2015).
All areas have activity in the medical technology, medical biotechnology, industrial biotechnology and pharmaceutical sectors, but the South East (Thames Valley, Oxfordshire), the East of England (Cambridgeshire) and London together contain 60% of all employment. 20 In OTV, Oxford and particularly Oxford University dominate. Its translational trajectory is predicated on its very strong science base, much of which is funded by national and international research funding bodies (research councils, national charities and currently the EU). The main local sector network is OBN, 21 a membership organisation with some 400 member companies, which has spread its activities beyond Oxfordshire, providing networking, partnership, purchasing and training activities. OBN in practise is not a formal part of a locally organised innovation cycle, as is the case with Biocat.
Switzerland
Switzerland operates ‘a systemic approach to research’. 22 As an established approach in Swiss politics, the division of tasks between the private and the public sector in the field of research and innovation is based on two pillars: the principle of subsidiarity and a liberal economy. Thus, the government becomes only active in areas where it is constitutionally authorised so to do. Under the Research and Innovation Promotion Act (RIPA), the Swiss government is responsible for providing grant funding for research and innovation through the Swiss National Science Foundation (SNSF) and the Commission for Technology and Innovation (CTI). 23 The Federal budget through the SNSF and programmes such as the national centres of Competence in Research (NCCR) for university-based education, research and innovation, is very high.
At the regional level, Swiss cantons also fund universities and especially universities of applied sciences (Gebhardt, 2015). Gebhardt argues that it is not necessary to use innovation policies as developmental measures in Switzerland, since private investment is the key driving force. In the pharmaceutical sector, Switzerland is now leveraging that strength for broader biomedical sciences and the creation of its national biotech innovation chain. 24
The Zurich life science (LSZ) cluster was established in 2001 by the University of Zurich and the Federal Institute of Technology Zurich (ETHZ), both in the canton of Zurich. 25 It aims to establish co-operation networks bringing together academia, industry and the public sector, and to support science education. Approximately 80% of the cluster activities are related to human health. In addition to promoting networking and communication within the universities and with the general public, two new networking platforms, the LSZ Young Scientist Network and the LSZ Business Network, have been initiated.
Data, methodology and findings
Each HealthTIES project teams collected standardised regional information on universities, research institutes, universities of applied sciences, intermediate vocational education, publications, care and cure providers, government, industry, technology transfer, science parks and incubators. The data, as at 2012, were then benchmarked for each region using a set of indicators that comprise innovation system parameters and best practices, by an analysis of the scientific strengths of the universities and companies by region, together with a Strengths, Weaknesses/limitations, Opportunities and Threats (SWOT) analysis.
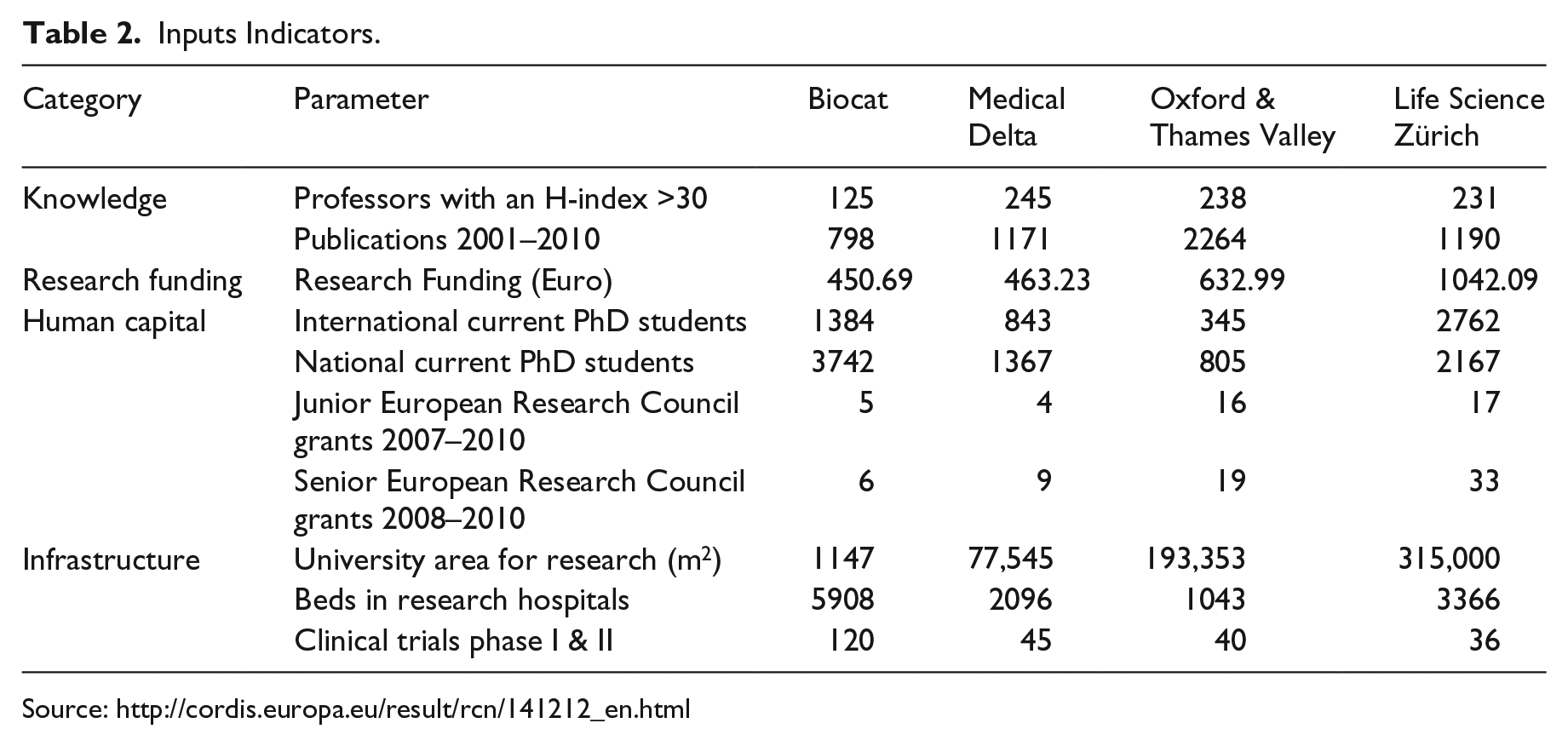
Data in Tables 2–4 are designed to show the innovation cycle at each stage: local resources (inputs), innovation system and output indicators. 26 However, this kind of analysis is fraught with methodological complexities owing to the difficulties in defining what is to be measured and reported indicators of performance (Carlsson et al., 1999).
Inputs Indicators.
Innovation system indicators.

TTO: Technology Transfer Office.
Output indicators.

For example, the EC’s (2011) Economic Performance Indicators (EPIs) for regional biotechnology are categorised under three dimensions: cluster dynamics, enablers and outputs. 27 Cluster dynamics includes the number of jobs created and companies established (including growth and survival rates within the last three years). Cluster enablers are designated as the external environment and include public funds raised, private funds raised, framework conditions and the number of cluster organisations (cluster management/facilitator). Cluster outputs include revenue from marketed biotech products/technologies, revenue from licensing activities on biotechnology products/technologies and numbers of newly developed and marketed biotechnology products/technologies.
Other measures of outputs from universities include numbers of university products such as patents, licenses and collaboration (Lendel, 2010), as well as spin-offs. All offer a range of possible sources of innovation that could be absorbed within a local economy. Measurement by geography and the impact of proximity are important but also problematic. Goldstein (2009), for example, measures universities’ technology transfer by distance, types of research and kinds of universities. He finds spillovers from basic research to be less localised than those from applied research, with spillovers from highly ranked research universities more geographically widespread.
Identifying outputs is problematic, as studies do not necessarily agree as to what is an input or an output. Moreover, whether inputs and outputs can be actually identified as being ‘regional’ is a further complication. For the biotech sector, standard output indicators include the founding rates of firms, size (employment, turnover etc), specialisation as indicated by new products, patents and drugs in development. Collectively, these shape the specialisation of a region from the private sector and universities (BIS, 2013).
In keeping with the suggested metrics above, the HealthTIES project developed a set of innovation indicators that were grouped into the three innovation phases: Resources (Input), Innovation System and Outputs. 28 Data were collected by teams from each of the partners. In Oxford, MD and Zurich, the teams comprised academics working with local organisations. In Biocat, data were collected by the Biocat team. The criteria adopted for the study across the regions for innovation indicator datasets were that the data should be relevant to the HealthTIES disciplines – biotech, medtech, life sciences, engineering and medical sciences, and that discrimination between regional performances should be supported. This illustrates that within the healthcare sector a number of disciplines are involved (Tödtling and Trippl, 2015).
The datasets needed to be quantitative in order to identify the impact of local expertise and conduct regional SWOT analyses. Our focus is on capacity building and exploitation of existing capacity, that is, the system and its existing strengths and opportunities. We accept that there are limitations to the chosen proxy variables, for example a large number of patents are non-performing, and a great many spin-offs do not deliver significant new products based on research (Balas and Elkin, 2013). However, these indicators are believed to be the best available.
The regions differ in the scale of activity, both geographically and in component elements of the innovation cycle. In turn, these have reinforcing effects and implications for pathways of development because they influence what future developments are possible. Key organisational differences lie in whether the regions exist as virtual, functional or administratively defined regions, in the lead organisations and major players, in the composition of the resource, systemic elements of the cycle and, thence, in the scale of outputs, and in relation to the size of population and resources. In the analysis we examine where each region occupies different positions in international innovation/value chains, identifying place-based issues.
Existing resources, strengths and opportunities
The differences between each region at Stage 1 of the innovation cycle are illustrated in Table 2. The four regions are specialised in different areas of research and commercialisation activities. For example, OTV is a leading region regarding its research activities and capabilities in the health-related research sectors and lags in commercialisation. An indicator of the region’s strength in knowledge is the number of professors with an H-index of 30 and above. 29 MD, OTV and LSZ have at least 100 more than Biocat. Per number of professors, however, Biocat has a higher rate of publications (6.4) than MD (4.8) and LSZ (5.2). Oxford’s professors’ publication rates far exceed all of these (9.5). Other European countries do not yet have an equivalent of the Research Excellence Framework (REF). This is a system for assessing the quality of research in higher education institutions on their research outputs, research environment and impact. It strongly drives academics to publish and obtain research funding. Impact relates to ‘an effect on, change or benefit to the economy, society, culture, public policy or services, health, the environment or quality of life, beyond academia’. 30 Academics can also apply for grants to encourage knowledge exchange.
Oxford University’s academics have had a primary focus on publishing in top journals in order to maintain global reputation. Rather than this being associated negatively with commercialisation, perhaps peer-reviewed publications are an important means through which dissemination to industry takes place. Grimshaw et al. (2012) (in Balas and Elkin, 2013) argue that most clinical research arises through scientific reviews that synthesise knowledge for practical implementation. It is therefore possible that UK government policy on the REF is supporting key future elements of the healthcare innovation system, as well as in specific knowledge transfer initiatives in life sciences.
On overall levels of external research funding, LSZ is ahead of OTV. OTV matches that region in the number of ERC junior research grants but lags behind in the number of senior ERC grants. This might indicate that the innovation cycle in OTV is at a comparatively early stage and is focused more on science than translational medicine when compared with LSZ. However, the strength of the research base overall illustrates the primary UK position held by Oxford University and its teaching and medical research functions in local National Health Service hospitals. 31
MD, LSZ and Biocat outperform OTV in human capital, particularly in the ability to attract more overseas as well as national MSc/PhD students. LSZ has more international PhD students and graduated MSc students, both national and international, suggesting that it has a younger profile than the other regions. However, it is Biocat that has by far the most PhD students and OTV has by far the least. Taken together, per head of population Biocat has the highest percentage of 0.7%, next is LSZ, 0.4%, followed by Oxford, 0.13%, and MD, 0.1%. This is an indicator that the regional environment (Casper, 2013) in OTV and MD is less favourable. This suggests that the local labour market might be attractive to local and inward investors, whereas a lack of skilled professionals in OTV and MD might be bottlenecks for a growing industry.
Biocat is the strongest region for translational medicine overall with respect to the number of both research and general hospital beds in its much higher number of hospitals, and in the number of clinical trials for its population size (0.3%). This with its smaller number of professors with high H-indexes, lower levels of publications, research income and much smaller research infrastructure indicates that its position in an internationally organised healthcare innovation value chain is that of teaching and applied research. There are potentially greater opportunities for stakeholder engagement and agency at the local level to develop translational research activities, given the high level of regional funding.
In contrast, the small number of research hospital beds at OTV might hamper the development of advances achieved through the interaction between research and patients, thus limiting experimental capacities. This is in spite of institutional capacity in the form of a regional clinical trials consortium.
Innovation systems
In Stage 2 of the innovation cycle, one of the main differences in the respective innovation systems relates to the size of the physical infrastructure (Table 3). Biocat far outperforms the other regions in the space provided in its science parks and has stronger institutional capacities in the form of a vastly higher number of technology transfer officers both in the science parks and in the universities.
However, this does not translate into significant differences in the numerical value of commercialisation in an innovation value chain in the form of the number of spin-off companies. Biocat does have the most spin-offs, nearly double the number in OTV and LSZ, but not that many more than MD. The greater number might mean that the agency of entrepreneurs in creating institutions and building capacity (Feldman, 2014) is stronger than in the others. It is the case, therefore, that entrepreneurship is necessary for innovation in the healthcare sector, but this study also illustrates that this is not sufficient to drive forward innovation, whereas the state is necessary but not sufficient by itself and needs other system elements to interact.
Biocat’s place in an international healthcare innovation value chain differs from that in MD and OTV, particularly. MD and OTV have the largest public–private partnerships, which are internationally organised (Birch, 2008). What is seen here is a hybrid domain of important technology advances – a combination of analytic and synthetic knowledge (Coenen et al., 2004). However, the number of granted US patents of potential value realisation tells a different story, as there is a fairly uniform number across three regions, with LSZ having fewer.
OTV has the second largest provision of space but its infrastructure for incubation of new and growing biotech firms is weak. SQW (2013) also identified a lack of available premises inhibiting the location of Big Pharma and a lack of linkages between Oxford University and local firms. Oxford University has now started building the Bioescalator (an incubator) amongst other research institutes, next to the Churchill Hospital. This eventually will be ‘a hub for the commercialisation of bioscience and medical research and innovation in Oxford’. 32 Three other bioincubators are planned in Oxfordshire. 33
Where the evidence is lacking is on local inter-linkages, which the cluster literature suggests are drivers of innovation (but see Birch, 2008; Malmberg and Power, 2005) and central contributors to innovation. The evidence suggests that local intervention is important. Specifically organised innovation systems can produce better performance.
Outputs
One of the major differences is in the value realised by commercial activity or outputs in the regions if employment is taken as a proxy (Table 4). LSZ dominates the number of larger biotech companies, which is over twice that of MD, while Biocat and OTV are way behind. LSZ also has many more jobs than two of the other three in the smaller biotech companies. Biocat comes close to LSZ in jobs, mainly employed in its smaller firms.
In spite of OTV’s strong research base, its ability to commercialise research seems to be limited. Employment in the biotech sector is half that of Biocat and somewhat over a third that of LSZ. Its poor performance might indicate that despite the very strong scientific labour market, which is associated with high levels of entrepreneurship (Fritsch and Schindele, 2011), the area appears to lack people and capabilities for supporting commercialisation or fostering entrepreneurship, which seem to be present in all the others. This is consistent with the finding that OTV has a weaker regional environment (Casper, 2013). This could also be related to the lack of a local interventionist policy for the sector. This may be a short-term problem: OTV was able to attract throughout Europe the largest amount of investments between 2007 and 2010 with 420.75 million Euro (followed by MD with 215.38). This indicates a perceived (scientific/economic) potential for further growth by investors and this has the potential to increase the output of the region over time.
Another prime indicator of commercialisation is in the number of products on the market. Here LSZ scores most highly, followed by Biocat. This suggests that in Switzerland it is the private sector that is driving developments, a characteristic of the NIS, while in Biocat the government policy of collaboration is having an impact. However, OTV has the highest number of products in clinical trials, but is third highest in products at the discovery stage. This shows that there are no clear cut patterns to translational research across the board, rather there are indicators of where different kinds of agency are being felt in producing outcomes.
What the data in the three tables cannot show are direct outcomes in innovative healthcare. Other indicators, such as new therapy and healthcare structures, efficacy and effectiveness indexes, could be more appropriately constructed as outcome indicators. These indicators would be a first step in identifying national, regional and local conditions that underpin potential advances in healthcare and, hence, can be used to identify appropriate policy responses.
Conclusions
In this paper, the concept of an innovation cycle has been used to examine the healthcare sector in four leading regions in Europe. Data collected at one point in time are used to reflect on our main research question: how has the innovation cycle in the healthcare sector developed in each of the four regions? A related question is also examined: what do the elements of innovation cycles tell us about the location of value in international value chains? This question is asked in economic development and policy cycles given the importance of local–international networks for innovation.
To answer our question, we use data from HealthTIES supplemented with discussion on the place-specific contexts within which the data are meant to be analysed. From this analysis the development paths can be seen and comparisons across places made to show the relative positioning of the regions within internationally organised innovation value chains. Moreover, this sector provides both economic and social benefits. Past studies recognise that a thriving innovation-oriented healthcare sector is seldom inward looking, and collaborations abound. Although comprehensive data on collaboration across value chains do not exist, capacity data are available to some extent for parts of the value chain in different regions.
Data on the three stages of the innovation cycle (resources/inputs, systems and outputs) give information on those differences. The resources tell us about capacities, the innovation system tells us about interactions and the outputs provide indicators of the effectiveness of commercialisation process in each. Although we do not have time series data, we can use the cross-sectional data to show the outcome of investment, utilisation of resources and provide implications for the broader impact through a presentation of policy needs and data needs.
We show that with respect to resources, the four regions are specialised in different areas of the innovation cycle. OTV is clearly an outlier, being dominated by analytic rather than synthetic knowledge (Coenen et al., 2004) but not in all respects, particularly in human capital. While MD and LSZ are similar to OTV in the number of research professors, this does not translate into the same level of publications. All three other regions have far higher student numbers than OTV, both at Master’s and PhD levels. Three regions (but not OTV) are converging in the inputs to support commercialisation. OTV lags behind the others, especially Biocat, in the number of hospital beds and clinical trials, which represent later stages of the innovation process.
Biocat, however, is well behind the others in the availability of university infrastructure for research. LSZ is well ahead of the others with respect to research funding and associated university research areas. We note how public policy and private sector involvement have produced distinctive characteristics either through enabling or not enabling processes needed for translational research.
In ‘innovation systems’, Biocat is the leader, particularly for physical infrastructure, especially in the number of full-time technology transfer office (TTO) employees. It has more university spin-offs than the others but there is an imbalance between the resources devoted to commercialisation and the resulting extent (spin-offs and patents). Similarly, the evidence suggests that OTV’s TTO resources are relatively inefficient as they have not resulted in as many university spin-offs pro rata. A strength of MD’s innovation system is in the number of large public–private projects that have an applied commercialisation element (synthetic knowledge, Coenen et al., 2004).
The evidence suggests that it is in systemic features where MD, LSZ and Biocat are converging, but not necessarily through the same kinds of public policy intervention (Table 1). Where Oxfordshire’s LEP celebrates the strength of the life sciences research base, its policy priorities are more to do with creating a favourable environment with strategic interventions linked to infrastructure. It is considerably behind LSZ and Biocat in the commercialisation of research over a wide range of resources, innovation systems and output indicators.
OTV is an outlier in other ways. It lacks the range of infrastructural support that is present in other regions, such as incubators and technology transfer support. It has a comparatively low number of young academics graduating but has a high capacity to import. A serious weakness is its apparent low capability to create spin-offs and to profit from its strong research as well as patent base. This might indicate insufficient capabilities regarding the commercialisation process as well as insufficient entrepreneurial education.
It is ‘outputs’ where there is most obvious evidence of divergence across a range of indicators, indicating that the trajectories of the region in translational medicine are different. This is particularly the case with respect to the roles of entrepreneurs in driving innovation systems rather than being merely outputs. MD is the leading region in the number of companies but less so in the number of larger companies (those with more than 20 employees). Hence, there are limitations to its overall SIS (Malerba, 2002, 2005). LSZ is the most efficient in generating the largest number of successful firms, as is also indicated by the number of products on the market. OTV again diverges from the other three regions in translational activity in the number of biotech companies of all sizes. However, OTV has the highest number of products in clinical trials and total investments, indicating its specialist position in the healthcare innovation chain, that of a developer of potential innovations.
In our case, holistic analysis does not provide answers to who is doing what to achieve better results. What these frameworks do tell us is what data we need. Furthermore, the organisation of the healthcare sector in each region is different and the national contexts are dissimilar so data really are often non-comparable and somewhat unreliable. At the same time the absolute values (not per capita) tell us about potential policy agenda.
We have used the concepts of innovation cycle for the framework of analysis. This has also drawn on the SIS and innovation value systems rather than with boundaries (NIS and RIS) to better analyse our cycle. It sets out elements that at different stages in innovation processes produce outcomes in a circle of interaction. In principle this circle is virtuous, but where key elements at each stage are lacking, opportunities for certain pathways of development are limited.
An implication for policy is that as nations move towards knowledge-based economic development, universities are a necessary but not sufficient condition for scientific research to create profitable and socially valuable innovations. There is scope for public policy to identify how the local infrastructure might be improved and, hence, feed into stronger internationally organised innovation systems. The strength of the science base does not necessarily result in new firms and applied projects, even though a normative policy agenda might suggest that it should. However, downplaying scientific publications could underestimate their importance in innovation value chains. As Balas and Elkin (2013) suggest, better understanding is needed on the scientific publication pathway in innovation success.
Footnotes
Acknowledgements
The authors thank John Slater for his comments on earlier versions of this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research leading to these results has received funding from the EU’s Seventh Framework Programme (FP7/2007-2013) under Grant Agreement No 26555.
Supplemental material
Supplemental material is available for this article online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.