
Abstract
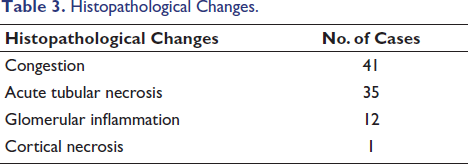
Renal toxicity is a frequent and often fatal complication of snake envenomation. This cross-sectional study aimed to characterize the renal pathological changes in 47 fatal snakebite cases subjected to autopsy at the Institute of Forensic Medicine, Madras Medical College, between 2017 and 2019. Kidney tissues were collected, processed, and H&E-stained for light microscopic examination. The analysis revealed that renal congestion was the most prevalent finding, occurring in 41 cases (87.23%), followed closely by acute tubular necrosis (ATN) in 35 cases (74.46%). Other significant observations included glomerular inflammation in 12 cases and renal cortical necrosis in one instance. These results demonstrate that snakebite nephropathy encompasses a diverse spectrum of pathological alterations, primarily driven by direct venom toxicity and secondary hemodynamic changes. Understanding these specific renal manifestations—ranging from interstitial nephritis to irreversible cortical necrosis—is essential for clinicians in managing acute kidney injury and for forensic experts in framing precise medico-legal opinions regarding the cause of death in envenomation cases.
Introduction
Globally, snakebite envenoming is a neglected tropical disease affecting millions, with India reporting the highest mortality rates. In Tamil Nadu, Viperidae (Russell’s Viper and Saw-scaled Viper) and Elapidae (Cobra and Krait) are the primary species of concern. While neurotoxicity often dominates Elapid bites, renal toxicity is a hallmark of Viperidae envenomation, with acute renal failure (ARF) occurring in 13%–38% of cases in India.
The pathogenesis of snakebite-induced acute kidney injury (AKI) is multifactorial, involving direct nephrotoxicity, hemodynamic instability, and secondary effects like rhabdomyolysis and disseminated intravascular coagulation. Despite its clinical importance, detailed histopathological profiling of fatal cases remains essential for forensic documentation and understanding the mechanisms of death.
Methodology
This cross-sectional study was conducted at the Institute of Forensic Medicine, Madras Medical College, Chennai, from July 2017 to December 2019.
Inclusion criteria: Confirmed snake bite cases with documented clinical progression to AKI. Exclusion criteria: Unknown bites, pre-existing chronic kidney disease, and decomposed bodies. Procedure: Kidneys were collected during autopsy, preserved in 10% buffered formalin, and processed for H&E staining. Slides were evaluated under light microscopy for glomerular, tubular, and tubulo-interstitial changes.
Observations and Results
A total of 47 cases were analyzed.
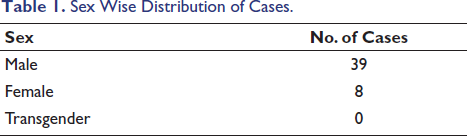
Demographics: Thirty-nine males and eight females. The age range spanned 3–79 years, with the peak incidence between 40 and 60 years (Tables 1 and 2). Histopathology (Table 3): Congestion: Present in 87.23% (n = 41). Acute tubular necrosis (ATN): Observed in 74.46% (n = 35). Glomerular changes: Twelve cases showed inflammatory changes. Cortical necrosis: Observed in one case.
Discussion
Snake venom is a toxic saliva secreted by modified parotid glands. It is a clear, amber-colored fluid when fresh.1, 2 It is a complex mixture containing more than 20 components. The dry weight of venom is constituted by protein, comprising a variety of enzymes, non-enzymatic polypeptide toxins, and non-toxic proteins. It is composed of enzymes (proteases, hydrolases, hyaluronidases, oxidases, phospholipases and esterases), Polypeptide toxins, cytokines and other mediators which cause inflammatory changes and hemodynamic alterations (Figure 1).
Pathogenesis of Snakebite-induced ARF
The kidneys have a rich vascular supply and are hence prone to venom toxicity. 3 Snakebite-induced ARF is usually caused by ATN, but all renal structures may be involved. Clinical renal manifestations include proteinuria, hematuria, pigmenturia, and renal failure. Renal cortical necrosis, acute tubular interstitial nephritis, extracapillary proliferative glomerulonephritis, mesangiolysis, and vasculitis have all been described. The pathogenesis of renal lesions in snakebite is a complex process involving both the direct action of venom on the kidney and the inflammatory effects due to the release of various endogenous cytokines and mediators. Phospholipase A2 stimulates hypothalamus-pituitary and immune axes to increase adrenocorticotropic hormone, corticosteroid, arginine vasopressin and acute phase response. The vasoactive mediators like thromboxane B2, endothelins and other cytokines are important in cellular interaction in a variety of immunological and inflammatory processes. Snake envenoming is a similar inflammatory process as infection or sepsis with roles of cytokines, mediators, complement activation, oxidation and immune response. 4 Hemodynamic alterations play a significant role in snake envenomation. Effects of direct nephrotoxicity are also observed in our findings, which is consistent with Kanjanabuch T. 5
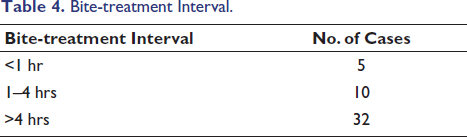
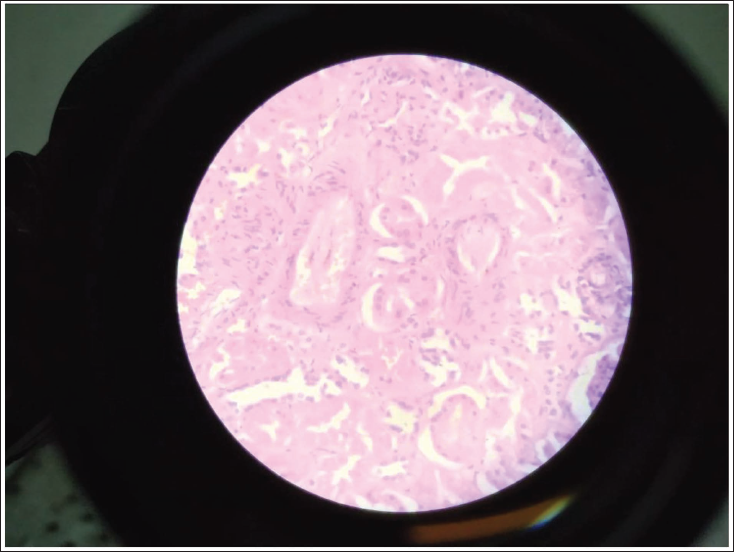
The bite-treatment interval was prolonged in the majority of cases (Table 4). This is owing to the fact that most of the victims are from rural areas and have limited access to hospitals. These findings are observed in a study by Al Lavati et al. 6 The findings observed in the histopathological study were congested blood vessels in the interstitium, focal necrosis of glomeruli, ATN, interstitial edema with inflammatory cell infiltration and fibrin thrombus in arterioles. Glomerular changes included enlargement of the glomerulus with hypercellularity. Ballooning degeneration with endothelial cell swelling was also noted. The findings are consistent with those of Pal et al. and Sitprija V (Figures 2 and 3). 7
The findings of this study align with the broader landscape of snakebite research in India. The predominance of males (83%) reflects the occupational risk associated with agricultural activities in rural India, consistent with studies by Pal et al. and others in the Journal of Indian Academy of Forensic Medicine (JIAFM). 8
Renal Pathology in the Indian Context
The high incidence of ATN (74.46%) matches findings across various Indian centers. In a study published in JIAFM, Pal et al. noted that tubular changes are the most consistent finding in poisonous snake bites. Similarly, the presence of glomerular hypercellularity and ballooning degeneration observed in our study mirrors results reported by Sitprija and researchers focusing on South Asian viper species.
The pathogenesis involves complex interactions. Phospholipase A2 and other enzymes in the venom induce systemic inflammatory response syndrome (SIRS), characterized by cytokine release (TNF-α, IL-6), leading to hemodynamic alterations and direct tubular injury. While cortical necrosis was rare in our study (2.12%), it remains a dreaded complication of Russell’s viper bites in India, often leading to permanent renal failure in survivors.
Comparison with Other Indian Studies
Indian forensic literature emphasizes that "bite-to-treatment" intervals are critical. Our observation of delayed treatment due to rural locations is a common theme in JIAFM reports, where authors advocate for regional-specific polyvalent anti-venoms to combat local species variation.
Sex Wise Distribution of Cases.
Age-wise Distribution of Cases.

Histopathological Changes.
Bite-treatment Interval.
Cut Section of Bite Mark Site.

Acute Tubular Injury Scanner [H&E 10×].

Acute Tubular Necrosis [H&E 40×].
Conclusion
Snakebite-induced AKI remains a significant cause of mortality in India. Histopathological examination reveals a spectrum dominated by ATN and congestion. Early administration of anti-snake venom (ASV) is the primary determinant of outcome. From a medico-legal perspective, a detailed histopathologic study is vital for establishing the cause of death when clinical evidence is sparse.
Footnotes
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent not applicable as it was done as a part of medico-legal autopsy.