
Abstract
Science, technology and human values have been the subject of enquiry in the last few years for social scientists and eventually the relationship between science and gender is the subject of an ongoing debate. This is due to the event of globalization which led to the exponential growth of new technologies like assisted reproductive technology (ART). ART, one of the most iconic technological innovations of the twentieth century, has become increasingly a normal social fact of life. Since ART invades multiple human discourses—thereby transforming culture, society and politics—it is important what is sociological about ART as well as what is biological. This article argues in commendation of sociology of technology, which is alert to its democratic potential but does not concurrently conceal the historical and continuing role of technology in legitimizing gender discrimination. The article draws the empirical insights from local articulations (i.e., Odisha state in eastern India) for the understandings of motherhood, freedom and choice, reproductive right and rights over the body to which ART has contributed. Sociologically, the article has been supplemented within the broader perspectives of determinism, compatibilism alongside feminism.
Introduction
Studies in history have told us the developments in society from primitive stage to capitalist stage. These developments have been the outcome of different levels of technology and its use. From the mid-twentieth century and into the 1970s, physics and attendant developments with atom-splitting nuclear power, and later the micro-electronics revolution, commanded the greatest attention. In the past decades, these fields have been rivalled and in some instances eclipsed, at least media attention and the popular imagination, by developments in biology, which has not received even a fraction of the attention from social studies of science. This is something of an idiosyncrasy, given both the current and the potential impact of the advances in reproductive technology on how individuals, members of families, and social groups think about each other.
Assisted reproductive technology (hereafter ART), one of the most iconic technological innovations of the 1970s and 1980s (Steptoe & Edwards, 1978) and since then more than 5 million people have been conceived by ART. Therefore, the ART has been viewed as a normal social fact 1 of life. It focuses on procedures ranging from intrauterine insemination (IUI) to in-vitro fertilization (IVF) 2 that enable couples who have trouble conceiving on their own (genetically linked child) arising from infertility 3 . It is also recognized that technological changes affecting the future of reproduction would require innovation in social, political, religious and ethical life as well. When a new technology emerges, it brings about social change in the society such as culture, the established institutional settings and the value systems. One of the important things which get affected is the established organizational patterns of a society. New technologies often bring major changes in the organizational patterns, which eventually lead to changes in the social relationships. Since the rapid advances in reproductive technology invade multiple human discourses—thereby transforming culture, society and politics—it is important what is sociological about ART as well as what is biological. The article draws the empirical insights from local articulations (i.e., Odisha) in order to the understandings of motherhood, freedom and choice, sense of unease due to rights over the body to which ART has contributed. This article turns out on examination to explore more intimate questions of, say, (in)fertility and identity.
The Anthropology 4 of ART
The event of globalization (Appadurai, 1996) brought a number of trends, especially the increase in international movement of commodities, capital, information, and people, as well as the development of technology (such as in computers, telecommunications, transport and healthcare). If globalization has made reproduction complex almost beyond belief—and its boundaries have been constantly shifting, as everyone searched for the immaculate conception and birth—then global events like United Nations Programme of Action of the International Conference on Population and Development (ICPD) in Cairo in 1994 (United Nations Population Fund, 1995) highlighted issues on future actions on ‘prevention and appropriate treatment of infertility where feasible’.
In fact, reproduction can be imagined as either innately biological or in terms of ‘nuts and bolts’, ‘plumbing’, ‘mechanics’ or ‘giving Nature a helping hand’ indexes a specific pattern of social organization, known anthropologically as a ‘conception model’ (Malinowski, 1927). The conception model presumes that reproduction is a part of Nature, which is later shaped by culture or convention, exposes the social fact that there is always a cultural specificity to how reproductive causality is understood or modelled (Strathern, 1992). Reproduction is universally subjected to elaborate social control and is always modelled in a manner which parallels and complements other social structures (Strathern, 1984). Therefore, reproduction has been considered as both social product and a biological one as well. The rules about who can reproduce with whom are considered to be among the first social proscriptions to mark the emergence of human culture (Levi-Strauss, 1969). This may be the reason which pushed Edward Westermarck (1921) to study the evolution of marriage patterns.
Towards Theoretical Position
Drawing the insights from the anthropological and sociological literature, a few theoretical perspectives around technological innovation guide this article. One is the deterministic perspective which says that technology shapes social reality. The second is the social reductionist perspective that social forces condition the growth of technology. Technologists keep in view the needs and values of potential users before developing new technologies (Callon, 1989). Since the time of invention, technologies are conceived keeping in view the needs of society or social groups and the new social order which the technologies would usher in. These arguments gesture towards third perspective, that is, compatibilism.
The mode of procreation facilitated by the ART creates commodification 5 of new objects (such as ova, sperm, wombs or embryos) and new [historical] subjects (such as women/couples willing to sell or donate their egg or womb, contracting their biological reproduction to another women, willing to donate extra embryos, and so on (Mohanty, 2018). But in modern society, almost everyone accepts the idea that a woman’s labour (for whatever form) can be bought, or that other services skills can be provided in exchange for money (Ibid.) which takes us to feminist perspective on ART. Feminists have long debated the normative status of ART. Two oppositional touchstone positions dominate the feminist perspective concerning ART. Abolitionists adopting a subordination approach are against the ART markets and view ART as a paradigmatic form of violence against women (while reinforcing patriarchal structures on women; Corea et al., 1985; Haraway, 1991; Wajcman, 1991), embodying gender inequality. For them, users (here women) are victims and lack agency in the context of pervasive institutional violence.
Further, ART fails to go beyond hetero-normative framework (Butler, 2002), reinforce the deterministic notion that it is genes that matter most 6 and strengthen traditional patriarchal norms in Indian society. ART advocates, on the other hand, are agnostic to the ART markets per se and, while cognizant of the circumstances under which users resort to it, view users as agents with some ability to negotiate within the ART industry. Therefore, their emphasis is on protecting and promoting the rights of users. It is in this context, one can argue that ART offers a choice of liberation for women (Firestone, 1970). Meanwhile, ART advocates, while cognizant of the role of both capitalism and patriarchy in shaping ART markets, offer more contingent understandings of the circumstances under which women’s reproductive labour enters circuits of economic exchange (Rajan, 2006). Despite the polarized appearance of these caricatured feminist positions, most feminists chart the middle ground between the two camps.
The ‘Field’: Notes on Methodology
Predictably, the most significant challenge was gaining access to ART users. However, in the wake of the ART facilities, several hospitals and clinics in Odisha have begun providing ART-based infertility treatment, with the oldest clinic setting now having worked with infertility couples for more than a decade. An exploratory study was carried out across three cities of Bhubaneswar, Cuttack, and Rourkela in Odisha. A total of 50 (n = 50) 7 in-depth, semi-structured interviews were carried out with 40 women treatment-seekers (hereafter users; see Table 1) and ten treatment-providers (hereafter providers; see Table 2). Interviewees were identified via internet searches of ART treatment clinics, official websites of treatment clinics, personal visits to these clinics, personal contacts. These clinics (as shown in Table 1) are located in busy parts of cities and are well-equipped with state-of-the-art technology to treat infertility.
Distributions of the Users (Women)

Distributions of the Providers (Doctors)

Anthropologists have reflected on what constitutes the ‘field’ and fieldwork, and its significance for the professional identity of anthropologists (Gupta & Ferguson, 1997). Yet given the common understanding of field as ‘the community of human beings who are studied’ (Srinivas et al., 1979). The multi-sited field (Marcus, 1995) visits of the present study used a network of mutual referral (‘snowball’ technique) 8 , to get in touch with providers and [intended] users. Fieldwork in hospitals or clinic settings, perhaps more than in any other area of research, demands from the fieldworker the careful use of the power of empathy (Minocha, 1979). The field work was conducted between 2011 and 2014.
The users were generally referred by the providers (e.g., Table 2). The study sampled providers from eight infertility treatment clinics/hospitals. These clinics were identified based on their involvement in ART treatment practices in Odisha. The interviews with providers and users were carried out at the clinic settings only. Ethical discomforts, particularly with users emerged during the fieldwork. Themes and contents were extracted from the recorded conversations 9 . An additional rich source of data was conferences, scientific and other related meetings.
Findings and Analysis
Infertility and the ART Market
It is said that every human being has a right to the enjoyment of the highest attainable standard of physical and mental health. Individuals/couples have the right to decide the number, timing and spacing of their children. Infertility can negate the realization of these essential human rights. Addressing infertility is therefore an important part of realizing the right of individuals and couples to find a family (Zegers-Hochschild et al., 2013). Infertility affects both sexes across the worldwide. The accurate information regarding the burden of infertility is deeply lacking at global, national and regional scale. However, a recent report (Gerrits et al., 2017) showed that 15% couples of reproductive age encounter infertile worldwide. By contrast, among couples of reproductive age in India, the prevalence of infertility in India was between 3.9% and 6.8% (ICMR, 2016). ICMR (2016) studies showed the regional variation in the prevalence of infertility among Indian states, for instance, 3.7% in Uttar Pradesh, Himachal Pradesh and Maharashtra; 5% in Andhra Pradesh; and 15% in Kashmir. Additionally, the variation may be found in same region across tribes and caste.
A large body of literature describes a trend among females in developed (Schmidt et al., 2012) and even in developing countries of delaying procreation and it is expected that this changing cadence to fertility 10 is becoming a global social fact. ART is one of the management mechanisms of infertility. Global Fortune Services (2020), a corporate analysis and data firm, estimated that ART market to reach USD 45.06 Billion by 2026. The ART market in India is currently growing at 18–19% and estimated to touch ₹25 billion (The Economic Times, 2016). ART clinics in India are now serving a new generation of ART consumers for whom the option of ART has become more routine and the purchase of reproductive services is part of a well-established market (largely private) health care (Mohanty, 2018). Commenting on this new generation of ART consumers, a leading ART consultant in Odisha noted that:
ART patients are changing, and our conversations with these patients are changing. Moreover, ART patients are more organized, more knowledgeable, more determined, and more assertive.
One of the key drivers of the ART market is the need felt by many women/couples to ‘attain motherhood/parenthood’ which includes becoming more discriminating purchasers of ART services.
ART Users: A Brief Profile
The following items were included: age, education level, and age at marriage, duration of marriage, dwelling conditions and caste/religion. The inclusion criteria for women in this study were—(a) being married; and (b) undergoing ART treatment for the past one to five years. Although the gender burden of infertility is particularly pronounced for female, but male factor cannot be ruled out. Male infertility, however, remains invisible in most societies including Odia society, because it is among the most stigmatizing of all male health conditions. However, it was planned before actually conducting the fieldwork to include men but the non-participant nature 11 of them during interviews kept out of the research. The age of the women in the study ranged from 19 to 43 years (see Figure 1). 70% of women were between 22 and 28 years of age (see Figure 1), 35% were high school educated.
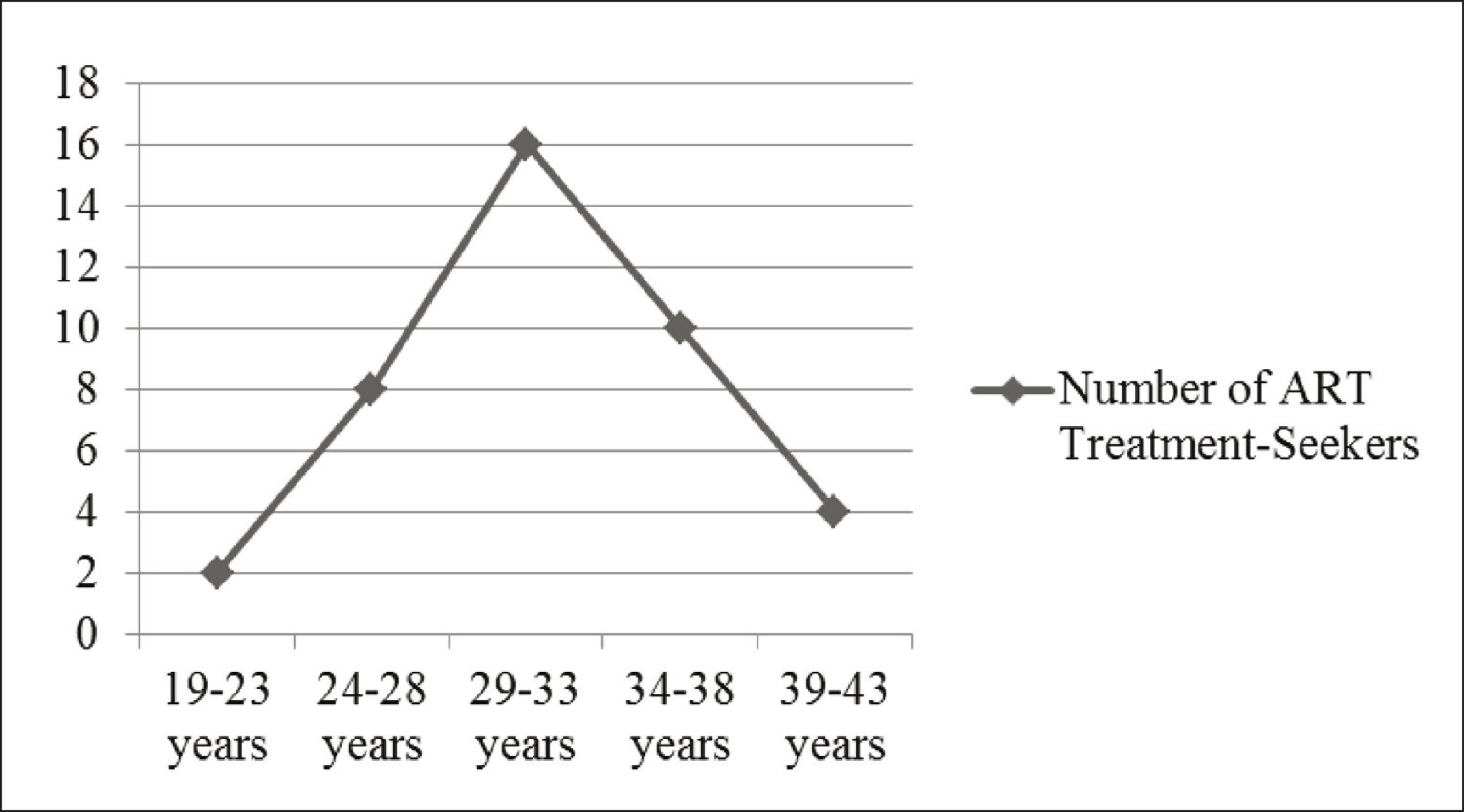
Some of them were married at a very young age, between 16 and 18 years (see Figure 2) and the others after the age of 29 (see Figure 2).

The majority (65%) of women had been married for about 3–5 years. With the number of married years increasing, the aspiration to have a child increased among studied women, for example, it was found that a single treatment site was visited per woman, aged between 19 and 23 years; three treatment sites per woman aged between 24 and 28 years and four treatment sites per woman aged between 29 and 33 years and four to six treatment sites per woman aged between 34 and 43 years. In addition, it was identified that 55% of the women used ART treatment for the last three years, 30% used for four years, and 10% used for five years.

The pre-dominance of Hindus among the users interviewed and/or the absence of other religious groups including Muslims or Christians interviewed, should in no way be interpreted to mean, for example, lower incidence of infertility among these communities, or poor access to treatment. The study was rather keen to include women from diverse religious groups but the absence of data from the clinics/hospitals restricted to the various categories of Hindus only undergoing ART treatment in the selected sites of Odisha.
The caste category that an individual belongs to which often determine their access to information and even their social networks (Desai & Dubey, 2012). Of the 40 treatment-seekers, 21 belonged to upper castes, ten belonged to middle castes and remaining nine belonged to lower castes (see Figure 3).
Revisiting Motherhood
A total of 40 [infertile] women interviewed and their life stories suggest a range of causes for and modes of taking to ART. Mohanty (2018) offers a taxonomy of factors for why and how women resort to ART. One of the causes includes major predisposing factors that cause female frailty. Examples of major predisposing factors are spoiled identity 12 , incompleteness (due to absence of the children of their own), and denial of ‘complete membership’ to biradari/khandaan, everyday suffering, ill treatment by a husband (and other family members), resulting in desertion or separation.
Take the case of a woman who was 24 when interviewed, with a postgraduate degree from Rourkela, an industrial arm of Odisha, shared:
[The] pressure was built within me; I was equally anxious and felt awkward at social gatherings especially when people inquired about ‘where’s the good news?’ (emphasis added) ‘When you are starting a family? You are old enough’ I felt ‘crushed’ being reminded of banjha (barrenness)
13
.
A 30-year-old-woman, native to Bhadrak, a northern city of Odisha state, in her sixth month of an ART-induced pregnancy said:
Without a child a woman has no identity, whether inside or outside a family
14
. Conceiving baby this [ART] way could alleviate [my] suffering.
The study found 80% women equated fertility with a major ‘power’ base through which they negotiate the terms of their existence. Moreover, fertility is a conversation which seeps into the extended family and society at large and the child is seen as a tool in the balancing of power within human relationship. In this study, power base can be understood in terms of strengthening women’s conjugal and affinal relations. Conceiving is their social redeemer, and thenceforth their importance in the family tends to gradually increase even can claim a stake over [family] property or resources. Therefore, they felt compelled by the unspoken pressures from their families to keep their maana-marzyada (honour) in a society. By doing so, not only is the ‘matron’ requirement reaffirmed through the use of ART, but also particular cultural dialogues about gender are also maintained and expanded.
Freedom and Choice
Technology raises the fundamental questions of freedom and choice. Does technology serve a need and offer us greater freedom to choose? Or does technology create new needs and further constrain choices? Such questions strike to mind when we look at ART. The right to be childless is as much a part of the choice as childbearing. The women interviewed went through ART procedures because their ‘hopes’ from the technology. Such hopes could be attracting contributory factor (Ibid.) for the users. A 33-year-old woman from the capital city of Bhubaneswar, told:
If you were successful, you call it a ‘choice’, but if you weren’t, then you would say that one would have been better off without it as ART treatment take long time and [an] economic burden.
Users were supportive of such innovations and moreover, their availability. A 25-year-old woman from Cuttack, a trade arm of Odisha, revealed:
Till now we already spent ₹50,000/. Still the pressure is from within the family. We had sold off our land for continuing the [ART] treatment And, I am the second wife to my husband and the reason for his remarriage was barrenness from the first wife. I fear of desertion!
The above statement implies that fertility has become an important marker of how good the relationship is. It was further observed that both young women (in their early twenties who do not want to wait too long to prove their fertility and fear rejection by their husbands and in-laws, in case they fail to conceive) and older women (10%) were finding their way to ART clinics. The statements also suggested that negotiations around child-bearing are perceived as a benefit made available by the existence of new technological intervention in procreation.
Sense of Unease: Body and Reproductive Right
Reproductive right stands by a woman’s right over her own body 15 for reproductive discipline and birth control, by her right for a truly wanted child through a planned pregnancy. The philosophy of ‘a baby at any cost’ seems to prevail and it has been argued that the right to reproduce has already been enshrined in the document approved in Cairo at the ICPD of 1994 which recognizes the right of access to appropriate health care services that shall provide couples with the best chance of having a healthy infant (UNFPA, 2004). At the same time, it is difficult to imagine that the ‘right to have a baby’ can include the right to have babies that are not biologically the offspring of the couple involved.
ART in a globalized market creates a reproductivized image to sell to users especially true for women, making their [fertile] bodies (Mohanty, 2018). The product [child] obviously plays a part in constructing the image of the self, resulting in an objectified body (Ibid.). ART is invasive as it entraps women into a medical ‘machine’ for certain period of time. Medical machines portray themselves as possessing agentic capacities to discipline bodies. A 28-year-old woman from Rourkela was battling infertility for five years narrated:
I took this [ART] treatment which costed me ₹1,00,000. The procedure was very painful. I felt a great pain after taking this injection… after consuming medicines, pain in the lower abdomen, nausea, feel tiresome, lack of adequate sleep at night…
Similar expression came from a 39-year-old woman from Cuttack:
The experience of going through this entire treatment process has been a constant negotiation of hope, frustration and desperation till you get the result. Sometimes there has been frustration at ‘nothing happening’, at failed cycles, at wrong diagnosis.
Providers, however, had a different view:
It is not harmful to undergo repeated stimulation cycles when the prescribed gap is followed. A few women develop ovarian hyper-stimulation syndrome, which is completely treatable and poses little risk. (emphasis added). These hormones are already being produced in the body in minimal doses. So, they do not have major side-effects. Some women may complain of breast tenderness and bloating, which are self-limiting and resolve once the injections are stopped. For those who want a baby at any cost these are minor issues. (emphasis added). They (risks) resurface every time there is an advance in reproductive technology.
The above statement showed the gut-feeling of the providers regarding the new technology. Providers further went on to argue that no one can be wholly certain what the biological consequences of this technology will be. In providers’ eyes, risk is a fundamental characteristic of new technology. This is the reason why informed consent and prior information can create appropriate safeguards against the evolutionary nature and foreseeable risks in new technology (Sahoo, 2013).
The Regulatory Backdrop of ART
In 2008, the ICMR developed a draft for ART (Regulation) Bill and sent to the Ministry of Health & Family Welfare, Government of India which was later revised by the Ministry of Law & Justice as ART (Regulation) Bill-2013. In 2016, the ART (Regulation) Bill-2016 came before the Cabinet for consideration. The ART (Regulation) Bill proposed to establish National Board, State Boards and National Registry of (ART) in India for accreditation and supervision of ART clinics and ART Banks, ensuring that services provided by these are ethical and that the medical, social and legal rights of all the concerned are protected with maximum benefit to all the stakeholders within a recognized framework of ethical practices. Finally, in 2020, the ART Regulation Bill has been approved by the cabinet which seeks to establish a national registry and registration authority and that gets applicable to all medical professionals and clinics operating or providing services in the field of ART.
Conclusions
From the above discussion, there are a number of inferences which are consistent with an increasingly large and diverse body of qualitative data and indicate that ART as a new social norm. In an era of scientific advancement ART (re)affirms the ‘conventional’ understandings of ‘motherhood’ and hence, contributes to the strengthening of hetero-patriarchy. Through interviewing users and providers and visiting them at their clinics/hospitals, it was observed that Odia rhetoric revolves around sentiments of salvation and sentiments which see the promise of ART in near millennial terms, often powered by a language of hope-n-hype. The pursuit of ART treatment offers a path forward which is sustained by hope and offers a commitment to a normative ascription, even if it never delivers on its promise. Further, reproductive choices through ART valued highly by Odia women for whom the sum total of benefits (in this case the fertile identity and status in the family) involved in technological intervention were greater than the costs. It leaves open the possibility that some may lose while others benefit, promising only that the magnitude of the latter will be greater.
For the first time reproduction is undergoing drastic change where technological development (i.e., ART), social needs and change are closely connected. If the whole point of ART is in order to facilitate successful human reproduction, then the effort to understand how human reproduction is being changed by the very technologies which enable this bridge to be built must be strengthened. Progress in ART, however, may pay attention to the questions of distributive justice. Done justly, the wellbeing of ‘the women’ is a proper subject of concern. The question of moral importance is not whether this constitutes ART; it is whether it can be done fairly and justly.
Footnotes
Acknowledgements
The authors are grateful to the National Institute of Science Education and Research (NISER), Bhubaneswar and the Jamia Millia Islamia, New Delhi for their support towards this research. Ancestor versions of the article were presented at University of Lucknow (2017); Indian Institute of Management (IIM) Calcutta (2016); the Annual Conference of the Indian Sociological Society at KIIT Bhubaneswar (2015). The authors are beholden to Manish Thakur and Devi Vijay of IIM Calcutta, for their feedback and suggestions; Tulsi Patel and S. C. Mohapatra of Delhi University for their recommendation and advice; Manju Singh of Banasthali Vidyapith (Rajasthan) for her encouragement and hospitality; two anonymous referees for their comments and criticisms. The authors wish to thank the staff of Ratan Tata Library of Delhi School of Economics and the Central Library of Jawaharlal Nehru University, Delhi.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.