
Abstract
This article examined the impact of the COVID-19 pandemic on the health financing system in Ghana. The COVID-19 pandemic presents two different crises—a health crisis and an economic crisis, and these have implications for the health financing system in Ghana. The pandemic is likely to have adverse effects on the various sources of healthcare financing, including government support, donor support, national health insurance scheme (NHIS) and out-of-pocket payments, which will impact the general delivery of healthcare in the country. Government support to the health sector in general is likely to be rechannelled into fighting the pandemic considering the declining tax and other non-tax revenues as well as huge expenditure commitment. Donor support is also likely to be scaled down and existing funds redirected into dealing with the COVID-19 pandemic. The NHIS will be affected, as many subscribers are not likely to renew their health insurance policies because of the fear of contracting the coronavirus when they visit health facilities. Also, the non-attendance at health facilities by health consumers will impact out-of-pocket payments and the hospitals’ ability to generate sufficient internal resources for their operations. A number of useful recommendations are proffered with the aim of improving health financing system in Ghana during and post-COVID-19 pandemic.
Introduction
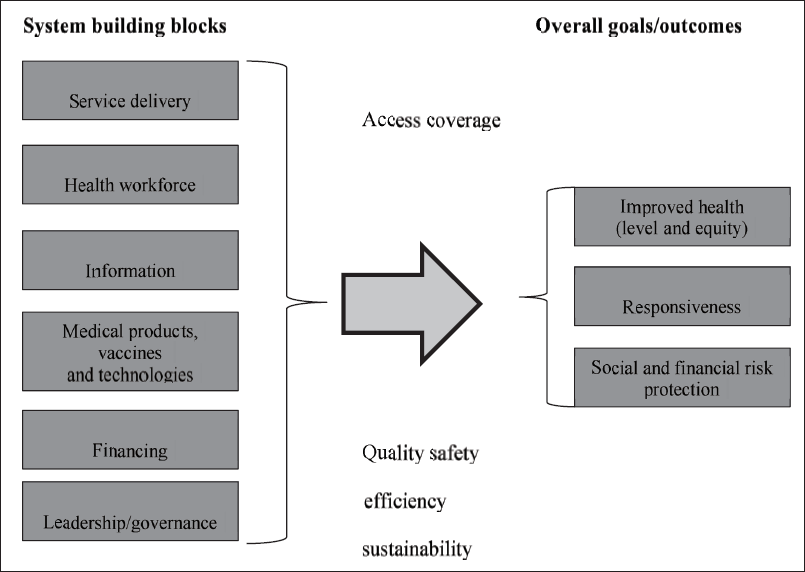
Financing of health systems is an important policy issue in both developed and developing countries, considering the significant role health systems are supposed to play in the delivery of healthcare to the population. The health financing system is one of the six elements of the health system—the remaining elements are service delivery; the healthcare workforce; information; medical products, vaccines and technologies and leadership and governance. The health financing system is supposed to interact with the other elements in order to improve health outcomes, to ensure financial protection, and respond to health consumers in an equitable, efficient and sustainable manner (WHO, 2000). We have, however, witnessed in recent times how the emergence of the novel COVID-19 pandemic is affecting lives. There are concerns and panic regarding the eventual impact of the current pandemic, including health financing system. As at the time of writing, the COVID-19 pandemic was still spreading, and the ultimate weight of the crisis could not be ascertained. The impact of the pandemic is likely to be long lasting, affecting many aspects of human lives with attendant consequences.
Though it is still not clear how the crisis will eventually impact health financing system, it is understandable to anticipate the heightened research interest in the near term on the likely impact of the pandemic on how health systems are financed. We discuss this issue from a developing country context, considering the problem of financing and other challenges confronting the health systems in developing countries like those in sub-Saharan Africa. The problem of health financing in sub-Saharan Africa has been a major limitation to delivering basic healthcare and this is mainly as a result of poor economic performance and very high population growth rates in these countries (Akortsu & Abor, 2011; Mwabu & Vania, 1990). This article examines the ongoing impact of the COVID-19 pandemic on health financing system in Ghana. This article is anticipatory and therefore we also explore the likely implications of the pandemic for financing Ghana’s health system.
The rest of this article is structured as follows: The section ‘Overview of Past Pandemics’ provides an overview of past pandemics in the world. The section ‘COVID-19 Pandemic and Ghana’s Health System’ discusses COVID-19 pandemic and Ghana’s health system. ‘Ghana Government’s General Response to the COVID-19 Pandemic’ section outlines the government’s general response to the COVID-19 pandemic. The section ‘Impact of COVID-19 Pandemic on Ghana’s Economy’ assesses the impact of the pandemic on Ghana’s economy. The section ‘Health Financing System Landscape Prior to the Emergence of COVID-19 Pandemic’ examines the health financing system landscape in Ghana prior to the occurrence of the COVID-19 pandemic. The section ‘Impact of COVID-19 Pandemic on Health Financing System’ discusses the implications of the COVID-19 pandemic for health financing system, and finally, the section ‘Conclusion and Policy Implications’ concludes the article with some policy implications.
Overview of Past Pandemics
In past decades and to a larger extent, wars, natural disasters and predatory animals mainly drove pandemics. It was in the early 1900s that the concept of zoonotic diseases was formed, where it was estimated that about 71% of new diseases and infections were indeed transmitted from animal to human (Burkle, 2020). A pandemic, as described by the WHO, is a disease that has spread worldwide, with little immunity to it, and or no cure for it. Most disease scientists believed a pandemic would occur in the then future and the most common source of it was the influenza virus, which usually starts from a host animal, and can transfer to humans, who have little to no immunity against it. Influenza viruses were hardly on the rise, since most of them did not make humans sick, and did not spread efficiently through human-to-human contact (Reissman et al., 2005).
The first pandemic was the H1N1 influenza pandemic, also known as the ‘Spanish flu’ of 1918. This according to Mills et al. (2004), killed 20–40 million people, and is seen as the worst-case scenario of any pandemic that ever occurred. The Centres for Disease Control and Prevention (CDC), in the United States also estimated that the deaths were hovering around 50 million, and it reduced life expectancy by 12 years (Centers for Disease Control and Prevention, 2019). The peculiar effect regarding this virus was the high death rate amongst healthy adults ageing 15–34, who by natural standards should be able to overcome flu-like symptoms in a short spiral. The case fatality was ten times more than the usual influenza virus epidemic and was particularly high in young adults. This grave death rate was as a result of the inadequate planning of measures to understand and deal with influenza, which later escalated beyond control, leading to a colossal loss of lives within a 2-year period (Mills et al., 2004). As time went on, the reproductive number per infected person transmitability, ‘R’, was estimated to be within 2–3 for the 1918 pandemic, a situation health and disease experts described as dire.
A rudimentary understanding of what caused the virus, animal-to-human transmitability, was not enough, as in 1957, another pandemic ravaged through the world. A/H2N2 influenza, less deadly than the 1918 pandemic, still wreaked havoc worldwide, with the death toll estimated to be around 1.1 million deaths worldwide. The second pandemic happened in the 1957–1958 period, where the H2N2 virus, also known as the ‘Asian’ flu was discovered (Centers for Disease Control and Prevention, 2019). The spread of morbidity of the virus to other countries and continents delayed, allowing for a vaccine to be created in time, to curtail further infections and possible deaths. This opened a window for the study of vaccines to future events of influenza that could lead to a global pandemic (Chowell et al., 2016).
The world was still very much in recovery mode, finding out new ways to combat novel viruses and diseases, when the third pandemic hit, in 1968, the H3N2 virus, which shared similar properties to the H2N2 experienced in 1957. This comprised of two genes from the avian influenza virus. The estimated number of deaths was around 1 million worldwide, with the CDC warning of the threat of antigenic drift, a phenomenon where the genes undergo change due to the influence of the virus in the body. Older people, with specific reference to those above 65, were more susceptible to the virus, and the mortality rate was prevalent amongst them .
It is noteworthy that most of the studies carried out focused more on Europe, Asia and the Americas, with little thought of Africa. Researchers were not able to determine how badly hit African countries were, especially during times where most of the countries were seeking political freedom at the time the pandemic was in full force.
Another pandemic, known as the H1N1 virus struck in 2009. This was a unique virus for the very fact that young people had little immunity to it, but the older folks had antibodies that fought against it. The CDC further estimated it infected about 61 million people with around 13,000 deaths worldwide. It was by far, the least deadly virus, and experts attributed it to preparedness and herd immunity against the strain of influenza as the H1N1 virus (Centers for Disease Control and Prevention, 2019). The WHO (2009) also estimated that this affected 214 countries and killed 18,449 people.
COVID-19 Pandemic and Ghana’s Health System
COVID-19 is considered an infectious disease caused by severe acute respiratory syndrome (SARS). The virus broke out in December 2019 in Wuhan, China, but its effect is still being felt, the world over. The World Health Organization (WHO) pronounced the outbreak of the virus a public health emergency of international concern on the 30 January 2020 and as a pandemic on the 11 March 2020. The COVID-19 pandemic is still spreading as at the time of writing this article with the increasing number of cases being reported daily. As on 3 August 2020, the pandemic had affected 216 countries and territories, with 17,889,134 confirmed cases and 686,145 deaths globally, as reported by the WHO. The pandemic is still spreading in many countries and in Ghana, 37,014 confirmed cases and 182 deaths were recorded as of 3 August 2020 (https://covid19.who.int/). The rise in the number of cases and death will depend on the rate of transmission of the virus and the effectiveness of response in place.
The COVID-19 response in many countries had been hindered by a lack of correct information mouthpiece, a fear-ridden approach used by most countries that created unnecessary panic and fear within the health sector, putting pressure on health resources. Citizens wanted tests to ensure they did not have the virus, and this put pressure on a lot of health systems worldwide. Some of the major problems health systems faced were the lack of accurate research information, knowing very little about the virus and its effect. This made it harder to plan and effectively put in place measures to better deal with the pandemic, curtail the spread and reduce the death rate in most countries (El-Jardali et al., 2020).
Andreea et al. (2020) suggest the need for quick decision making under time and pressure during periods of pandemic and this was key to combatting the virus and controlling the spread during such turbulent times. They advise that positive pressure be put on medical facilities to allow for easier and effective decision making, since there was almost always a clash of social, political, media and economic standpoints regarding how countries are to react during such times. Health systems, which were ready for pandemic breaks usually took steps from the responses of previous pandemics, and were better able to test, quarantine and treat infected people. Education of the citizenry, regarding how the virus works and what it takes to defeat it, was done massively.
In Ghana, the national response to the COVID-19 pandemic was when the first two cases were reported on 12 March 2020. The response by the Ghana Health Service regarding the COVID-19 pandemic, in relation to hospitals has been nothing short of problem-laden. The Director General of the Ghana Health Service at one of the press briefings, regularly held to update Ghanaians on the situation regarding the nation’s response to the virus, insisted that health institutions were going to be funded to adequately prepare for later instances of pandemics and other acute medical problems (Ghana Health Service, 2020). But this statement was not bereft of contempt, as it pointed out the lack of planning and infrastructure in Ghanaian hospitals in general. The lack of resources in Ghanaian hospitals has been identified as a reason for non-adherence to clinical guidelines. The guidelines include a complete and effective human resource capacity to cope with emerging pressures on hospital facilities, the availability of logistics, laboratory testing, equipment and protocols deemed vital in the fight against diseases, stretching to the pandemic (Amoakoh-Coleman et al., 2016).
Ghana’s response has been plagued with a plethora of problems in the health system in the country. This came as no surprise as Amoakoh-Coleman et al. (2016) clearly predicted that the country could face serious crisis soon, if resources were not put in place to correctly deal with the increasing pressure on hospital facilities, especially the lack of medical laboratories in the country, where effective research and placebo testing could be done. In an era where guidelines are of utmost importance, it bodes a vague picture of Ghana’s response to the COVID-19 pandemic.
Ghana Government’s General Response to the COVID-19 Pandemic
The Government of Ghana started responding to the COVID-19 pandemic in Ghana, when the first two cases were reported. The Government’s response to the pandemic was mainly influenced by lessons learnt from some of the countries, which were earlier affected by COVID-19, such as those in Asia and Europe. Developed countries like the United States, Spain and Italy have been heavily hit by the pandemic due to their earlier delays in responding to the outbreak of the virus. Some of the main policy actions the Ghana Government took included: the closure of all the country’s borders, mandatory quarantine and testing of all travellers coming into the country, and the partial lockdown of specific areas recognised as hot spots (i.e., Greater Accra and Kumasi).
The Ghana Government set out five key objectives to fight the COVID-19 pandemic in Ghana, including: (a) limiting and stopping the importation of the virus; (b) containing the spread of the virus; (c) providing adequate healthcare for those who are sick; (d) limiting the social and economic impact of the virus and (e) inspiring the expansion of the country’s domestic capability and deepening self-reliance.
The government implemented a number of measures to lessen the impact of the COVID-19 pandemic on the Ghanaian economy in tandem with measures being adopted worldwide. Some of these measures include: The commitment of a total of GH¢11.2 billion to deal with the pandemic and its social and economic consequences in 2020; About GH¢600 million to be used to support preparedness and response and GH¢10.6 billion for establishing a Coronavirus Alleviation Programme (CAP) to facilitate economic recovery. The establishment of the Coronavirus Alleviation Programme Business Support Scheme (CAP-BuSS), as part of the CAP, designed to specifically support micro, small and medium-sized enterprises (MSMEs). Lowering of the cap on the Ghana Stabilisation Fund (GSF) from the $300 million to $100 million in order to close the fiscal gap due to the pandemic by transferring funds to support the Coronavirus Alleviation Programme. The establishment of $100 million National Emergency Preparedness and Response Plan (EPRP) for COVID-19 to help manage and contain the spread of the virus and strengthen the national capacity for surveillance, diagnosis and case management. Amendment of the Petroleum Revenue Management Act (PRMA), allowing for the withdrawal from the Ghana Heritage Fund to support the fight against COVID-19. Provision of a life insurance package for those directly involved in surveillance, case management, laboratory, and all other health and allied personnel who get infected. Also, provision was made for overtime and risk-based payments for key frontline workers. The provision of temporary subsidy on the consumption of utilities—electricity and water. The cash transfer to the 400,000 most-vulnerable individuals under the Livelihood Empowerment Against Poverty (LEAP) Programme. Also, providing food packs to vulnerable persons within Accra and Kumasi. The reduction in the monetary policy rate by 150 basis points from 16% to 14.5% and a decrease in banks’ reserve requirement from 10% to 8% in March 2020 in order to encourage credit expansion to the private sector. Amendment of the Bank of Ghana Act to enable the government to borrow from the central bank in excess of the stimulated threshold as and when necessary. The engagement of universal banks to provide syndicated loans to support certain key industries. It involves granting a 6-month moratorium on principal repayments for particular businesses, reducing interest rates by 200 basis points, and also increasing the supply of credit to the private sector. The establishment of the National Trust Fund under Act 1013 in April 2020 to mobilise funds from individuals, churches, corporate bodies, staff of organisations, non-governmental organisations, groups, and associations, among others to support the fight against COVID-19. The setting up of the Ghana COVID-19 Private Sector Fund by the private sector to assist in mobilising support from the business community to help Government respond to the pandemic by providing critical interventions to Ghanaians.
The Government also implemented a number of tax measures to curtail the impact of COVID-19 on business and household sectors, including (Deloitte, 2020): Extending due dates for firms and individuals to file their tax returns from the usual four months to 6 months beyond the end of the basis year. Granting of waiver of penalties on principal tax liabilities owed by taxpayers who can redeem their outstanding liabilities by 30 June 2020. Granting of waiver of VAT on donations of stock of goods and equipment for combating the COVID-19 pandemic. Granting of waiver of taxes on certain withdrawals from third-tier pension funds. Granting of deduction against income tax for contributions and donations from the private sector, which are made for tackling the COVID-19 pandemic. Instituting an email filing and direct transfer payment system to enable taxpayers to file and pay their taxes remotely at the different offices of the Ghana Revenue Authority.
Impact of COVID-19 Pandemic on Ghana’s Economy
The COVID-19 pandemic presents two main crises to Ghana—first is a health crisis arising from the effect of the pandemic on public health and second is the economic crisis emanating from the pandemic. Overall real GDP growth was 4.9% in the first quarter of 2020 compared to 6.7% over the same period in 2019. Inflation remained flat between January and March 2020 at 7.8% but increased significantly to 10.6% in April and further to 11.3% in May but declined marginally to 11.2% in June. The sharp surge in inflation from 7.8% in March 2020 to 10.6% in April 2020, reflects the panic buying prior to the market fumigation exercises across the country and the partial lockdown in two main areas—the Greater Accra and Kumasi. Growth in broad money slowed between January and May 2020, while bank credit also fell as the demand and supply for loans dropped as a result of the uncertainties posed by the COVID-19 pandemic. The economy also experienced a decline in interest rates between January and March 2020 following the central bank’s reduction of the monetary policy rate. The economy also witnessed lower
The business and household sectors have also been hit by the pandemic with declining income levels as a result of the lockdown and closure of some business organisations. For instance, the hospitality industry has severely been affected due to the ban on international travel and closure of borders as well as the slowdown in tourism. The closure of most businesses led to staff being laid off, thus increasing the already high unemployment rate.
It is expected that the economic crisis resulting from the pandemic will likely impact on the various sectors of the economy, including the health sector. The article looks at how the current pandemic is likely to impact the financing of Ghana’s heath system. It is our anticipation that the impact of the COVID-19 pandemic will see resources rechannelled to intensify efforts at curbing the impact of the pandemic. This is likely to adversely affect the financing of the entire health system and the delivery of healthcare, especially in areas such as, malaria, tuberculosis, HIV/AIDS, emergency care and diseases related to the top causes of death.
Health Financing System Landscape Prior to the Emergence of COVID-19 Pandemic
As indicated earlier, the health financing system is one of the six elements or building blocks of any health system. The other elements include service delivery; the health care workforce; information; medical products, vaccines and technologies and leadership/governance (see Figure 1). The health financing system is expected to coordinate with the other elements to have a profound improvement on health outcomes, ensuring financial protection, and responding to health consumers in an equitable, efficient, and sustainable manner. In order to achieve these objectives, countries need to effectively execute the three main functions of the health financing system, which include raising revenue, pooling risk and purchasing services (WHO, 2000).
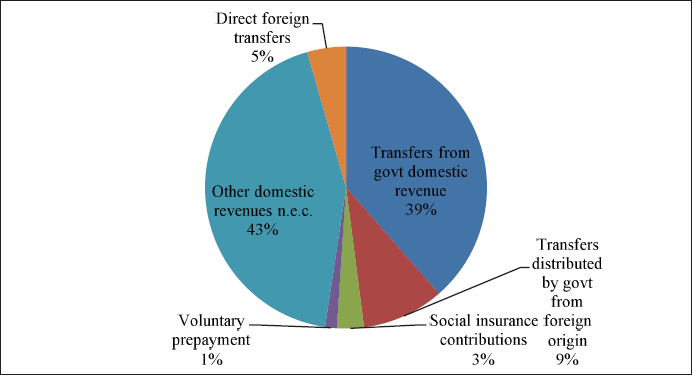
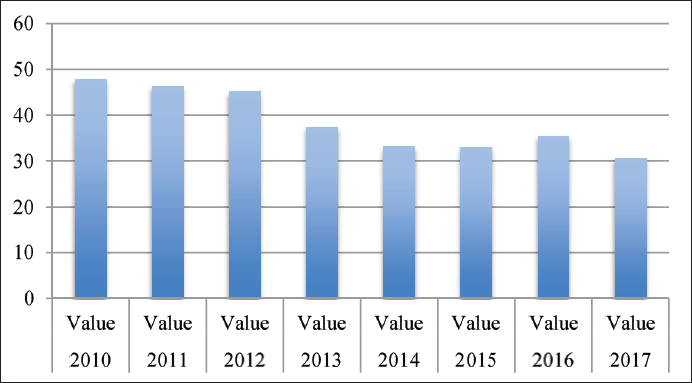
The main sources of Ghana’s health financing system include government support, donor support, National Health Insurance Scheme (NHIS), and out-of-pocket payments. Figure 2a shows the average contribution from the various sources of health financing over the period, 2010–2017. Government’s component of health financing comes from direct and indirect tax revenue (Akortsu & Abor, 2011; Mensah et al., 2010), and it represents about 39% of total health expenditure in the country. Figure 2b shows the trend in transfers from government domestic revenue (allocated to health purposes) as a percentage of health expenditure during the period, 2010–2017. We observe a declining trend of the percentage of government financing of health expenditure over the period. Donor support includes contributions from donor partners, accounting for 14% of health expenditure. The NHIS is made up of premiums paid through the District Health Insurance Scheme by the informal sector and payroll deductions by Social Security and National Insurance Trust and this represents 3% of total financing. Health consumers make out-of-pocket payments, which account for 1% of total health financing in Ghana, personally.
Prior to the outbreak of the COVID-19 pandemic, the Ghana government was initiating reforms aimed at achieving the Universal Health Coverage, but identified financing as a persistent challenge. As part of the strategy, was the need for mobilisation of more domestic resources for health. Another focus was to ensure the efficient utilisation of resources, which underscores the need for improving the purchasing function of health financing, including reviewing the benefits package to guarantee essential service delivery for all Ghanaians.
Impact of COVID-19 Pandemic on Health Financing System
The emergence of the COVID-19 pandemic is beginning to have an impact on the healthcare financing system in Ghana. In the bid to respond to the impact of the pandemic, the government has had to commit resources to support preparedness and response as well as establish the CAP to be used to promote selected industries such as pharmaceutical sector supplying COVID-19 drugs and equipment, support of MSMEs and employment. In order to cater to the huge spending associated with the COVID-19 crisis, the government also reduced spending on goods and services, transfers, and capital expenditure. This situation has implications for the contribution of the government as a source of financing health in general. Government is likely to divert more resources in the fight against the COVID-19 pandemic. Figure 2b shows that the percentage of government financing of health expenditure has been declining since 2010. Already tax and other non-tax revenues are dwindling and with the increased expenditure to boost the economy in response to the pandemic, the fiscal deficit will widen even further, thus increasing debt burden.
The pandemic has also had an impact on donor support. In the immediate term, we observe a number of donors or development partners respond to the pandemic by mobilising resources to finance global efforts at developing a coronavirus vaccine. It is however expected that after the COVID-19 pandemic, donors are likely to scale down on their contributions to health financing in developing countries like Ghana. A typical example was the reduction in donor support to developing countries due to the 2008 global financial and economic crisis (see OECD, 2012). Donor support in other areas such as HIV/AIDS, tuberculosis, and malaria is being rechannelled to fighting the COVID-19 pandemic. For instance, the Global Fund, on the 4 April 2020, issued a guidance note permitting recipient countries to apply grants for HIV/AIDS, tuberculosis, and malaria in their fight against the COVID-19 pandemic through reprogramming up to 5% of savings under existing grants and utilising underused funds (Global Fund, 2020). Also in Zimbabwe, the President’s Emergency Plan for AIDS Relief (PEPFAR) also directed that $150,000 be utilised in acquiring personal protective equipment (PPE) in hospitals (Harris, 2020; Oladele et al., 2020).
The NHIS as the source of financing healthcare in Ghana will also suffer. With the outbreak of the pandemic, many people seem to be shying away from seeking healthcare at the hospitals due to the fear of contracting the virus. Many of these hospitals, especially the public ones are used as isolation centres, which tend to scare non-coronavirus patients from visiting these facilities. Many people prefer doing self-medication at home for certain illnesses because of the fear of getting infected with coronavirus should they visit a health facility. This situation is likely to adversely affect the number of subscribers of the NHIS. Many people may not see the need to renew their NHIS membership if they are not going to visit a health facility and will continue with home treatment.
Similarly, out-of-pocket payment, which constitutes internally generated funds (IGF) of the hospitals, is likely to be affected. Once people begin to opt for self-medication or home treatment, they will avoid paying for certain services including elective surgeries, reproductive health services, amongst others, which they would have received should they visit a hospital. Non-attendance to hospitals will affect IGF of hospitals, thus out-of-pocket payment, as a source of health financing in Ghana will suffer. Also, the COVID-19 pandemic has had an impact on employment, which in turn has affected individual and household incomes. This obviously will affect people’s ability to afford to pay for healthcare, thus reducing IGF of healthcare facilities. A fall in the IGF of these hospitals will certainly affect their ability to acquire consumables for running these facilities.
Conclusion and Policy Implications
This article discussed the impact of the COVID-19 pandemic on the health financing system in Ghana. We observed that the pandemic presents a health crisis and an economic crisis, and these have implications for the health financing system in Ghana. We argue that the pandemic will have adverse effects on the various sources of healthcare financing, including government support, donor support, NHIS and out-of-pocket payments. This will likely impact the general delivery of healthcare in the country. Government support into the health sector in general is likely to be rechannelled into fighting the pandemic, considering the declining tax and other non-tax revenues as well as huge expenditure commitment. Donor support is also likely to be scaled down and existing funds redirected into dealing with the COVID-19 pandemic. It is expected that the contribution from NHIS will be affected, as many people are not likely to renew their health insurance policies due to the fear of contracting the coronavirus when they visit health facilities. Also, the non-attendance at hospitals will impact out-of-pocket payments and the hospitals’ ability to generate sufficient internal funds to support their operations.
Following these observations, we proffer some useful recommendations to improve the health financing system in Ghana. First, the government needs to intensify efforts at increasing tax revenue and increase support to the health sector beyond the current fight against the pandemic. The government needs to ensure compliance in the payment of taxes by roping in those outside the current tax net, especially the informal sector. Improving the level of formality in the country may be useful in increasing the county’s tax revenue generation capacity.
Support from development partners or donors should be targeted at specific priority areas/projects within the health sector with proper coordination instead contributing to general budgetary support. The issue of coordination is necessary to avoid duplication of efforts or multiple donors undertaking the same health-related projects.
To ensure the sustainability of the NHIS, subscribers need to be encouraged to continue renewing their policies. The general education and awareness in this regard are essential. The participation of private health insurance schemes should also be encouraged, especially for the middle to the upper class that can afford it.
The private sector should be encouraged to increase support to the health sector. For instance, the establishment of the Ghana COVID-19 Private Sector Fund to provide a prompt response to the health crisis due to the COVID-19 pandemic is a laudable initiative. The fund, which has support from corporate organisations and some individuals, has put up an infectious disease centre to improve the testing capacity and treatment of infectious diseases in the country. It is expected that similar facilities will be constructed in three other cities—Kumasi, Takoradi and Tamale.
At the facility level, the leadership and management of hospitals need to be proactive in identifying other revenue sources. Ensuring efficiency should be a top priority for hospital management. This requires plugging all the leakages in revenue generation and minimising wastage in the hospitals’ operations. There is also the need for investment into IT infrastructure to promote telemedicine and mHealth. This will help sustain the health facilities’ IGF even in periods when most people will not want to physically visit health facilities.
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship and/or publication of this article.