
Abstract
In an era where every public health action is expected to be backed by credible evidence, health policy-making has also been increasingly seen to follow the same. The general consensus across the globe is to strengthen health information systems and the decisions of the policy makers are increasingly relying on the information provided to them through such systems. COVID-19 has clearly brought out the need for accurate, timely and relevant information in planning for and responding to public health emergencies that can be equally devastating, if not more. It is crucial for information providers to understand the importance of communicating and disseminating it in a timely manner so that it leads to public health action for the larger good of the population.
Introduction
Health information is the most important element of a health system. It is the basic tool of management and the key input for progress in society (Park, 2019). The availability of data and its conversion to information is the cornerstone of health systems across the world. The information thus obtained is utilised in policy formulation and revising it regularly.
Sound, reliable and timely information is the foundation of decision-making across all health system building blocks, and is essential for health system policy development and implementation, governance and regulation, health research, human resources development, health education and training, and service delivery and financing (WHO, 2008).
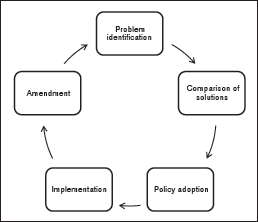
Policy making is a continuous and iterative process. One of the vital factors that drives policy-making and its reform is data. The steps in policy-making include, problem identification, comparison of solutions, policy adoption, implementation and amendment; each of these steps requires information (Figure 1) (Walsh & Simonet, 1995). The field of science is evidence-based; hard facts are what the scientists rely on in making decisions. In a similar way, health policy should not merely be a wish statement, it should be supported by scientific facts and figures. Information is crucial for all management levels of health services, from periphery to centre, implying that not only the policy makers and managers need to make use of information in decision making, but also the healthcare providers.
This article has been written with the objective to explain the importance of health information and its role in policy formulation and its implementation.
Health Information Systems
The WHO expert committee has identified the requirements to be satisfied by the health information systems, and these include that the system be population based, avoid unnecessary agglomeration of data, problem oriented, employ functional and operational terms, system should express information briefly and imaginatively, make provision for feedback of data (Park, 2019).
The health information system provides the underpinnings for decision-making and has four key functions—data generation, compilation, analysis and synthesis, and communication and use. The health information system collects data from the health sector and other relevant sectors, analyses the data and ensures their overall quality, relevance and timeliness, and converts data into information for health-related decision-making (WHO, 2008).
In addition to being essential for monitoring and evaluation, it also aids by providing alerts and early warning signals, supporting patient and health facility management, enabling planning, supporting and stimulating research, permitting health situation and trends analysis, supporting global reporting, and underpinning communication of health challenges to diverse users.
The information is of little value if they are not available in formats that meet the needs of multiple users—policy-makers, planners, managers, health care providers, communities and individuals. Information can influence decisions if it is relevant, reliable and available for decision makers in a timely fashion. Hence, dissemination and communication are essential attributes of the health information system.
Sources of Health Information
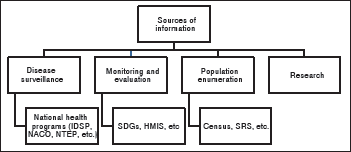
The sources of health information can broadly be classified as (a) disease surveillance, (b) monitoring and evaluation, (c) research and (d) population enumeration (Figure 2). Each of these sources individually and collectively serves as important public health data sets in health planning and health policy making. Disease surveillance is an ongoing, systematic collection, analysis and interpretation of health related data, essential to the planning, implementation and evaluation of public health practice. Surveillance systems help in identifying the early warning signals, investigation and confirmation of cases or outbreaks, guide in public health policy and strategies and pro-dive feedback of information to those providing data. Monitoring and evaluation is important for keeping track of activities and the data thus obtained help in identifying the achievements and the priority area. Population enumeration is more or less the baseline data for planning and implementation of all health related activities. The findings of scientific research most often serve as an aid in health policy making.
The various sources of health information in India are—national health programmes, census, registration of vital events, sample registration system, notification of diseases, hospital records, disease registers, record linkage, epidemiological surveillance, health service record, environmental health data, manpower statistics population surveys and other routine statistics related to health (Park, 2019).
Health Management and Information System (HMIS)
In the year 2008 the Ministry of Health and Family Welfare (MoHFW) launched a government to government web-based monitoring information system. It has since then been in place to monitor the national health programmes and provide key inputs for policy formulation and appropriate programme interventions. The HMIS (n.d.) portal facilitates flow of physical performance from the facility level all the way up till the national level. The data generated through this system has been utilised in assessing performance of health facilities and budget allocation and disbursement. The analytical reports generated through HMIS also provides gap analysis and evidence based course correction. The portal also provides periodic report on the status of the health service performances and human resources and infrastructure services facilities available. HMIS has been capturing facility-wise data pertaining to the following:
Service delivery (reproductive, maternal and child health related, immunisation family planning, vector borne disease, Tuberculosis, morbidity and mortality, OPD, IPD services, surgeries, etc., data) on monthly basis; Training (trainings imparted to medicals and paramedics staff at district and state level data) on quarterly basis; and Infrastructure (manpower, equipment, cleanliness, building, availability of medical services such as surgery, etc., super specialties services such as cardiology, etc., diagnostics, para-medical and clinical services, etc., data) on annual basis.
Integrated Health Information Platform (IHIP)
With the intent to introduce a uniform system for maintenance of electronic health records for every citizen by the hospitals and healthcare providers in the country, the Government of India (GoI) launched IHIP. It provides interoperability of various EHS systems already implemented in the country (National Health Portal, n.d.). IHIP is envisioned to benefit the consumer, health care providers, public health personnel and the policy makers. Currently only two of the many health programmes are active on the IHIP portal. The IDSP module of IHIP was launched in the year 2018 in seven states of the country, and is being launched in phased manner in state/UTs of the India. It is a path breaking initiative and intended to provide case based surveillance data in real time to policy makers for detecting outbreaks, reducing morbidity and mortality, and lessening disease burden in the populations and better health systems (Ministry of Health and Family Welfare, 2018).
Examples of Health Information Systems Driving Public Health Policy: World and India
Sustainable Development Goals (SDG) 2030
The development of SDG 2030 was through a series of deliberations. A post-2015 development agenda was arrived at by broad participation from major groups and other civil society stakeholders of the UN member states. The UN played a facilitating role in the global conversations on the post-2015 development agenda and supported the broad consultations. It had the responsibility of supporting the member states by providing evidence based inputs, analytical thinking and field experience. The sustainable development goals was proposed by the open working group, a result of a three year transparent, participatory process of all stakeholders and people’s voices. The 17 SDGs and its 169 targets was then unanimously adopted by 193 UN member countries (United Nations, 2015a, 2015b).
Cardiovascular Disease
Cardiovascular Disease (CVD) is the leading cause of mortality, responsible for about 30% of deaths worldwide. Framingham heart study, an observational cohort study, was designed to understand the causal relationship between hypertension and other risk factors and coronary heart disease. This study helped to elucidate the major risk factors for CVD and also identify those at highest risk of developing CVD, thus helping in reducing the age adjusted CVD deaths to a half in developed countries. The result of this study was used by the national experts panel to develop guidelines for risk management (Bitton & Gaziano, 2010).
Rare Diseases
Rare disease is a health condition of low prevalence that affects a small number of people compared with other prevalent disease in the general population. This results in limited data being available for the purpose of policy-making in this field. The data available from other countries has to be considered in the local context and at times limited available data has to be used to make larger projections. Evidence suggests that around 80% of the rare diseases are genetic in origin and hence disproportionately affect children. These diseases are serious, chronic, debilitating and life threatening, often requiring long term and specialised treatment/management. The field of rare diseases is complex, heterogenous, continuously evolving, and suffers from a deficit of medical and scientific knowledge. Considering these challenges and making use of the available information, the GoI in the year 2016 appointed three high level committees to work on a policy for rare diseases. The observations and recommendations of these committees and the available data and evidence from other countries, were used in framing the National Policy for Treatment of Rare Diseases in the year 2020 (Ministry of Health and Family Welfare, 2017).
Immunisation
The immunisation programme was introduced in India in 1978 as the expanded programme of immunisation by the Ministry of Health and Family Welfare, GoI. The programme modified as the Universal Immunisation Programme (UIP) in 1985, is one of the largest programmes in the world. The programme makes informed decisions concerning the introduction of new vaccines and strengthening it through the National Technical Advisory Group on Immunisation (NTAGI). The role of NTAGI is mainly to be an advisory body to assist the GoI in developing a nationwide policy framework for vaccines and immunisation, prioritise immunisation activities and set attainable targets, identify critical gaps in policy and programme, and identify studies, assessment and research areas to be addressed; and to review periodic assessment of the national immunisation programme, including performance and disease incidence. Based on the recommendations of the Indian NTAGI the combination pentavalent vaccine was introduced as a part of the UIP (India NHPO, n.d.; Jacob, 2010).
Communicable Disease Surveillance
Disease surveillance gained momentum in India after the 1988 cholera outbreak in Delhi and 1994 plague outbreak in Surat. In response to these events the GoI constituted the National Apical Advisory Committee (NAAC) for national disease surveillance and response systems. Based on the NAAC’s recommendation, GoI launched the National Programme for Communicable Disease in 1997. In November 2004, the integrated disease surveillance project (IDSP) was initiated by GoI with a loan from the World Bank. The IDSP became the key surveillance system in the country and was scaled in three phases to all states and union territories of the country by 2007 (Director General Health Services, 2015).
Since then it has been elevated to a programme and now called integrated disease surveillance programme and is currently a part of the national health mission (NHM), encompassing two sub-missions—the National Rural Health Mission and National Urban Health Mission. There are several programmes and schemes under the NHM. These programmes capture much health information and utilise it in planning, development and implementation of policy.
IDSP is a decentralised surveillance system to detect early warning signals, so that timely and effective public health actions can be initiated. This programme effectively captures data on epidemic prone diseases using an IT based system from all health administrative levels of the country. The surveillance data is analysed to understand the trends and also has a feedback mechanism (NCDC, n.d.).
During the 2009 influenza A H1N1 pandemic and 2014 Ebola crisis, IDSP indicated great potential for surveillance requirements. Heightened surveillance and contact tracing systems were activated rapidly through trained manpower at state and district levels. The data captured by IDSP has been utilised in preparation of outbreak calendar. This has been envisioned as a crucial activity as it provides the states with focus areas and helps them in formulation of policy which are necessary to control and prevent the recurrence of such outbreaks.
In the year 2015, a joint monitoring mission (JMM) was constituted to systematically identify and subsequently fill gaps in surveillance and response, aiming to develop an action plan for strengthening integrated disease surveillance at all levels across the country. A comprehensive mixed method strategy was utilised for the JMM. The strategy included review of key thematic components of the surveillance by subject matter experts, the development of an appropriate tool kit, the processes and timeline review through an internal group, as well as field evaluation of surveillance functions and system attributes. A core group was constituted for consolidating and preparing the final report (Director General Health Services, 2015).
This WHO-led JMM recommended to redesign the IDSP surveillance system, including re-prioritisation of the list of diseases under IDSP and redefining the required surveillance deliverables, upgrading and redesigning the existing IDSP portal system and dashboard for real time visualisation of data and display of key indicators on public domain, ensuring adequate number of trained human resources surveillance both indicator and event based strengthening laboratories, zoonosis, influenza and VPD surveillance systems.
Following the JMM recommendations, the MoHFW, GoI, launched the integrated health information platform (IHIP). This platform is meant to capture real/near real time data. The platform has been designed to capture data and convert to information from all national health programmes in India. The primary objective of IHIP is to enable the creation of standards compliant electronic health records (EHRs) of the citizens on a pan-India basis along with the integration and interoperability of the EHRs through a comprehensive health information exchange (HIE) as part of this centralised accessible platform.
The surveillance mechanism of IDSP through IHIP can be case-based and event-based surveillance. It also includes the diseases which were considered to be important from the surveillance point of view after the disease re-prioritisation exercise. Within the IHIP platform the data captured at the Sub centre level can be immediately visualised at the national level. An epidemiological map is constructed by the platform for every case which acts as an efficient tool in planning the response activities.
In the context of COVID-19, the information of viral pneumonia of unknown aetiology is what triggered the health systems across the world. This information, as soon as available with IDSP, triggered ILI and SARI surveillance within the country and also demanded health infrastructure preparedness for the event when a case occurred within the country.
The information obtained by passenger surveillance activities initiated by the IDSP, helped the policy makers determine, understand and forecast what the country would face in the near future. This helped in strengthening infrastructure, understanding the necessity of a holistic approach and planning the steps ahead by formulating specific policies and guidelines which would respond to it effectively.
With the use of IHIP, case-based data was captured for COVID-19 laboratory confirmed cases. A graphic visualisation of this data was made available on the public domain, which was one of the recommendations of the JMM constituted in 2015 (IDSP, 2019).
Issues and Challenges
The process of data collection and dissemination has been laid out clearly but, ensuring its timeliness and regularity has remained a challenge for most health programmes in the country as well as lack of mechanisms to check the quality of the data being collected and disseminated.
A difference in the priorities of the technical, administrative and political systems. For health information to get converted into a health policy, a synchronisation of the priorities and actions of all the three are essential.
Presence of multiple vertical systems collecting overlapping information on the same individual leading to duplication of efforts and data entries. The non-availability of a unique identification code of each citizen of the country further hamper the health information systems.
In an era when digitalisation of all information, including health information has become unavoidable, data safety and security measures that protect the privacy of the individual should also be an integral part of the health management information systems. The constant threat of hacking of data and personally identifiable information from such systems poses an additional challenge.
Disease surveillance and response programmes such as the IDSP had not received the due attention of policy makers as reflected in the resource and budgetary outlay allocation they receive. COVID-19 has brought out the chasm between the mandate of the programme and the resources allocated for fulfilling the same. The importance of a sound disease surveillance system based on the principles of primary health care and utilising the latest available IT systems has been duly recognised by the health care planners and policy makers.
Way Forward
Evidence informed policy-making is the key for successful and desired health outcomes that in turn accelerates the progress of a country. The data sets generated (big data) in the country are many. Linking the healthcare data sets to facilitate its analysis is equally crucial, and the conversion of data into meaningful information will transform healthcare. The programmes within the government need to be enabled to collate this data and simultaneously maintain the confidentiality. The IHIP is one such platform which collects data and analyses the data fed in to it and generates graphs, trends, geospatial maps, and so on. The implementation of this platform in all state/UTs of the country and its use for all the national health programmes will boost the public health system of the country and also aid in evidence based policy making. IHIP also has the capability to serve as electronic public health observatories, it has been designed to collect and analyse information from various sources. It can be utilised to provide health intelligence (information, data, knowledge and evidence) that can result in local evidence-based action similar to public health observatories.
The WHO in the year 2005 established evidence informed policy network (EVIPNet). This was launched to promote systematic and transparent use of health research evidence in policy-making to strengthen health systems and get right programmes, services and products to those who need them (WHO, n.d.). It has triggered a change in how policy makers view evidence and how researchers engage with policy makers. The experiences of countries which adopted EVIPNet was documented, and it highlighted the five key achievements of its use which included capacity building of policy makers, bringing together communities, researchers, policy makers and decision makers, being able to respond to urgent requests of evidence, affecting change at policy frontline and changing the health policy-making culture (WHO, 2016). EVIPNet is a supportive network that enables working within the time constraints faced by policymakers. A similar mechanism needs to be adopted so as to strengthen the evidence informed policy-making process within our country.
Conclusion
Informed decision making is the cornerstone of a responsive public health system. The health data collection systems should be closely synced to the rapid response system, with both engaged in a continuous feedback loop. Making optimal use of the available technology in the field of health information can greatly augment the capacity of the public health system to take timely action. In developing economies such as India which also has a great potential to provide quality health care and has remained the hub for producing exceptionally trained professionals, an investment in strengthening the health information systems can yield rich dividends. Evidence-informed policy-making strategies must be developed and policy-making should continue to be based on strong health information systems.
Footnotes
Acknowledgements
We would like to express our sincere gratitude to Dr Jai P Narain, former Director, Communicable Diseases, WHO regional office for south-east Asia, for his valuable suggestions.
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship and/or publication of this article.