
Abstract
There is limited empirical evidence on the relationship between management and performance of private hospitals in Nepal. We address this gap using de-identified inpatient data from a private hospital in Kathmandu between 2013 and 2017. We consider foreign-born and native-born patients separately, in addition to the full sample. Using a Pabon Lasso model, we assess relationship between hospital management and: (a) bed occupancy rate; (b) bed turnover rate; and (c) average length of stay. To complement the Pabon Lasso model, we use a regression analysis to assess the relationship between hospital management and length of stay in a multivariate framework. Our results indicate that separation between the chief executive officer (CEO) and board may promote better performance, versus CEO duality. However, there are important differences by performance indicator, patient type (i.e., native-born versus foreign-born) and analytical approach. These results comprise new evidence on the relationship between management and performance of private hospitals in a developing context.
Introduction
In developing countries, like Nepal, many people believe the private sector delivers better health care than the public sector (Andaleeb, 2000). This is consistent with a shift in the public-private mix of hospitals across time. Specifically, the share of private hospitals in Nepal has increased from 23% to 78% since 1995. Moreover, the private sector now provides many services that were historically public, like maternal and childcare and infectious disease control (Government of Nepal, 2010). Nevertheless, there is limited empirical evidence on the performance of private hospitals in Nepal, especially as related to management. 1 This is despite the fact that evidence-based decision making is important for the efficient delivery of health care (Liang et al., 2017). We address this gap by examining the relationship between management and performance using Grande International Hospital (GIH) as a case study.
Established in 2010 and providing inpatient services since 2013, GIH is part of the large and growing share of private hospitals in Nepal. It is located in Kathmandu and offers multi-specialty preventative and curative services. GIH complies with patient safety goals of the Joint Commission International, and it has forged a new standard of care in Nepal in terms of improved sanitation, technology and accessibility. For example, compared to public hospitals where the use of new technology is lagging, GIH uses advanced sterilization techniques and a reverse osmosis water purification system (The Himalayan Times, 2017). Moreover, along with 10 operating rooms and 50 critical care units, it has a four-dimensional cardiovascular ultrasound, digital broadband magnetic resonance system, bone densitometer and catheterization laboratory. In terms of accessibility, GIH has an emergency medical team to rescue patients from across the country with an air and road ambulance service. It also provides preventative care, a help desk for foreign-born patients (e.g., for help with insurance and paperwork) and free clinics for those who cannot afford health care. In 2016, Frost & Sullivan named GIH as ‘Hospital of the Year’ (Business360, 2016). Given the importance of GIH to health and health care in Nepal, it is important to assess its performance and drivers thereof. Moreover, as a leading private hospital in Nepal, it is well-positioned to establish best practices for other private hospitals in the country and similar contexts.
GIH Management Strategies.

We use a Pabon Lasso model to compare hospital performance under these very different strategies via bed occupancy rate (BOR), bed turnover rate (BTR) and average length of stay (LOS) (Lasso, 1986). To complement this analysis, we estimate the effect of each strategy on LOS in a regression framework (Aij et al., 2015; Lotfi et al., 2014; Tripathi et al., 2016). Using this multifaceted approach, our goal is to support evidence-based decision making and best practices for private hospitals in Nepal and similar contexts.
Data and Methods
GIH provided us with inpatient data ranging from 2013 to 2017. To our knowledge, we are the only researchers who have access to these data, which contain information about the patient’s country of origin, age, gender, admit and discharge dates, treatment department, diagnosis and surgery procedure. The timeline also includes two external shocks: a major earthquake and a political blockade. 2
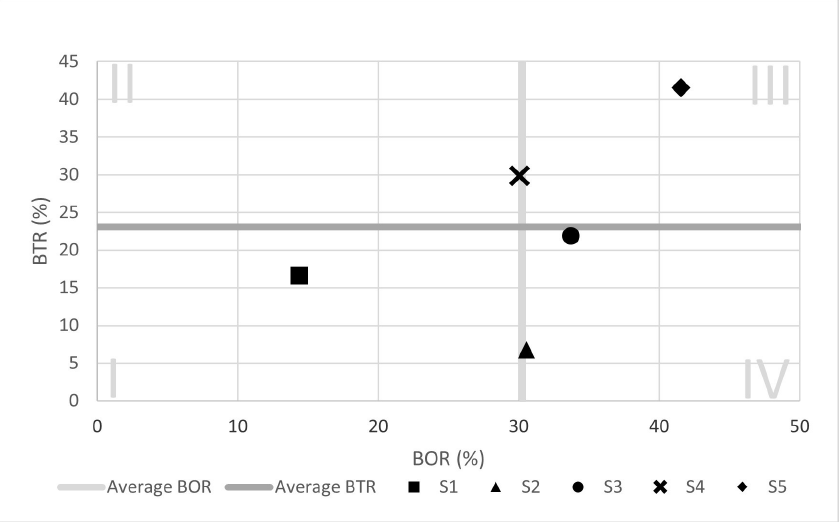
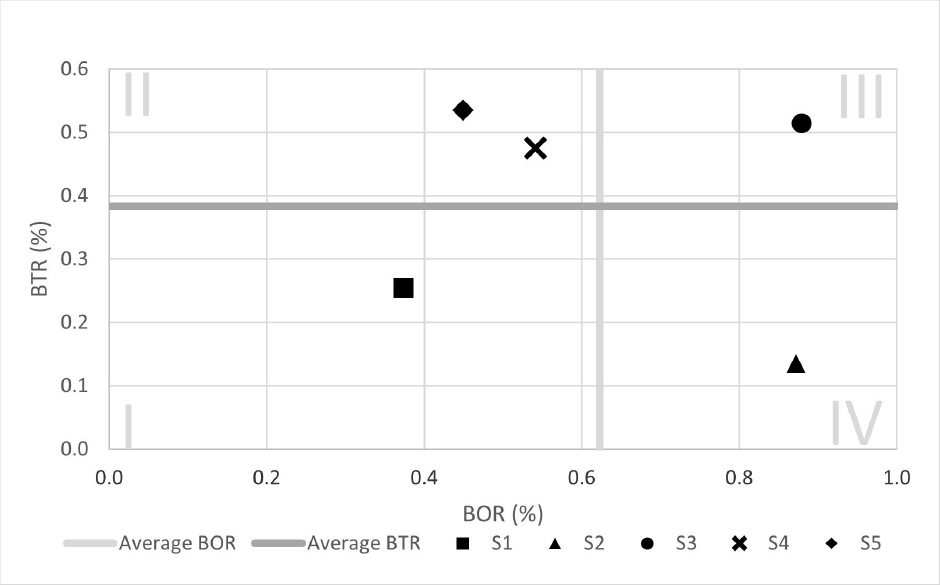
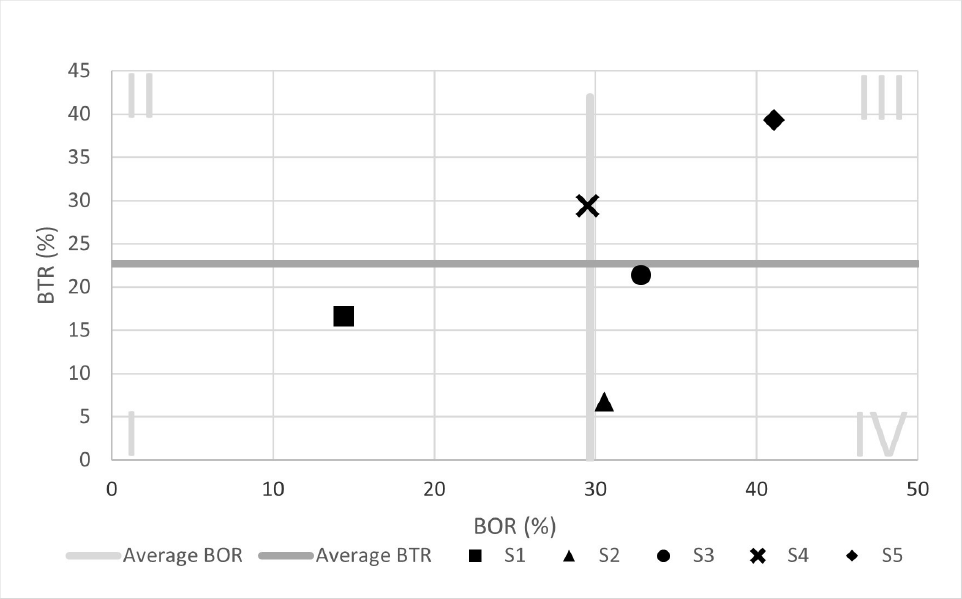
To assess the performance of GIH across the five management strategies, we use a Pabon Lasso model to analyze three indicators: BOR, BTR and average LOS. This graphical approach has been used largely in developing countries such as Iran, Malawi and Philippines (Aeenparast et al., 2015; Ajlouni et al., 2013; Asbu et al., 2012; Gholipuri et al., 2013; Kalhor et al., 2014). For example, Kalhor et al. (2014) use a Pabon Lasso model to assess the performance of six public hospitals in Iran. According to Lasso (1986), researchers should compare across a homogenous group of hospitals since size may affect all three performance indicators. Following this recommendation, we focus only on GIH and compare across the five management strategies.
In our model, BOR is represented on the x-axis and it measures the percentage of beds filled during the strategy. The value is derived by taking the ratio of inpatient days and bed days available (i.e., number of hospital beds × number of days the strategy was in place). BTR is represented on the y-axis and it measures the number of times each bed changes occupants. The value is derived by taking the ratio of the number of discharges during the strategy and the number of beds available, which is 200. The graph is divided into four quadrants where the cutoffs are defined by average BOR and average BTR.
3
The four quadrants are characterized as follows.
Quadrant I—Low BOR and BTR, indicating underutilization of hospital resources. Quadrant II—Low BOR and high BTR. Quadrant III—An ideal situation in which both BOR and BTR are high. Quadrant IV—High BOR and low BTR, representing longer hospital stays with limited changes in bed occupants.
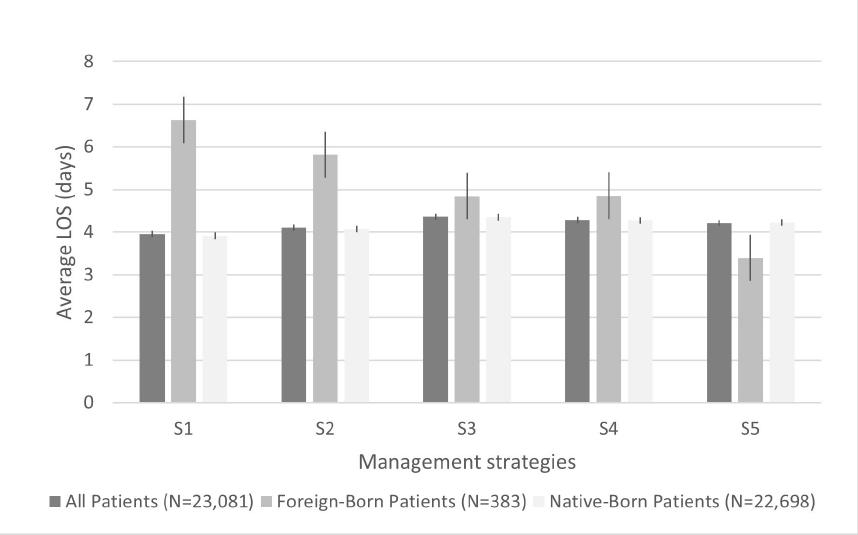
In addition to BOR and BTR, we present average LOS in a separate bar graph. It measures how many days a patient spends in the hospital, on average. 4
To complement the Pabon Lasso model, we estimate the effect of each management strategy on LOS in a regression framework as outlined in Equation (1). Y is LOS in days. βj captures the effect of management strategy Sj on LOS for j = (2, 3, 4, 5). The base group is S1, however we explore alternate base groups in Appendix A. X is a vector of controls for country of origin (i.e., native-born versus foreign-born), dummy variables for age compared to the base group of 25–58, gender, whether the patient had surgery, and treatment department compared to general surgery. We also control for the earthquake and political blockade, as well as time via dummy variables for month and year. α consists of parameters to be estimated and ε is the error term. We estimate Equation 1 using ordinary least squares regressions with robust standard errors.

In both the Pabon Lasso and regression models, we focus on patients who stayed at GIH for less than 39 days since this is the 99th percentile of LOS. 5 We also drop observations that have an obvious data entry error (e.g., a 300-year-old individual) or missing information (e.g., age, gender and treatment department). Our sample consists of 23,081 observations, of whom 383 are foreign-born and 22,698 are native-born. We perform all analyses separately for these groups, as well as the full sample. It is important to distinguish between foreign-born and native-born patients because there are likely differences in the nature of care received. For example, foreign-born patients may be visiting Kathmandu and more likely to seek emergency versus preventative care.
Results
Pabon Lasso Model
Figures 1 to 3 contain results of the Pabon Lasso model, which we use to compare BOR and BTR across the five management strategies. They are given for all patients, then separately for foreign-born and native-born patients. We find that, under S1, GIH was in Quadrant I for all patients. This is characterized by low BOR and BTR, indicating underutilization of hospital resources. BOR increased and BTR declined under S2. Specifically, GIH moved to Quadrant IV, which is characterized by longer hospital stays with limited changes in bed occupants. Under S3, GIH remained in Quadrant IV for native-born patients, but moved to Quadrant III for foreign-born patients. As described above, this is efficient with high BOR and BTR. Next, we find a reduction in BOR under S4, especially for foreign-born patients. Specifically, GIH moved to Quadrant II, which is demonstrative of ‘unnecessary hospitalization, an oversupply of beds or the use of beds for simply observing patients’ (Tripathi et al., 2016). Finally, we find that GIH operated efficiently under S5, especially for native-born patients. BOR and BTR were both high, indicating fewer unused beds and unnecessary hospitalizations.
In addition to BOR and BTR, we consider how average LOS varied by management strategy in Figure 4. For native-born patients, it was lowest under S1 and highest under S3. For foreign-born patients, average LOS was lowest under S5 and highest under S1.
Regression Model
Table 2 contains ordinary least squares estimates of Equation (1), through which we examine the relationship between management strategies and LOS in a multivariate framework. Unlike the Pabon Lasso model, this approach allows us to control for other factors that affect LOS (i.e., patient characteristics, treatment department, earthquake, political blockade and time).
Ordinary Least Squares Estimates of LOS—All, Foreign-born and Native-born Patients.
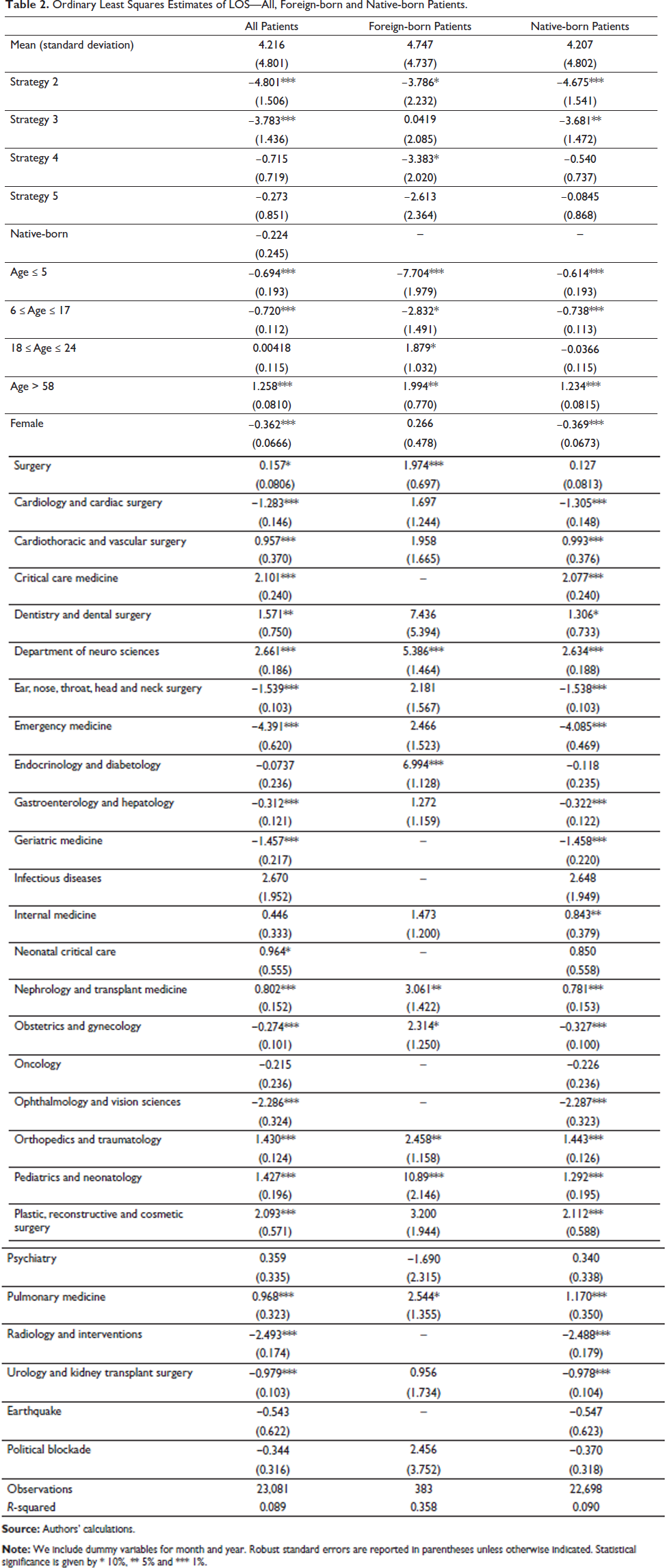
Compared to the base group, S2 had the lowest LOS. 6 Being treated under S2 reduced LOS by 4.8 days, on average, and the effect was slightly larger for native-born versus foreign-born patients. Interestingly, LOS was also shorter under S3 versus S1 for native-born patients (i.e., 3.7 days), but there was no effect on foreign-born patients. On the other hand, LOS was shorter under S4 for foreign-born patients (i.e., 3.4 days), but there was no effect on native-born patients. The difference between S5 and S1 is not statistically significant, regardless of patient type.
In terms of control variables, Table 2 indicates that children and youth (i.e., those younger than 18) stayed in the hospital for fewer days compared to those aged 25 to 58. On the other hand, LOS was 1.25 days longer for older patients, on average. We also find that LOS was marginally shorter for females and longer for individuals who had surgery. Moreover, patients in the following departments had a shorter LOS compared to general surgery: cardiology and cardiac surgery; ear, nose, throat, head and neck surgery; emergency medicine; gastroenterology and hepatology; geriatric medicine; obstetrics and gynecology; ophthalmology and vision sciences; radiology and interventions; urology and kidney transplant surgery. Conversely, LOS was longer for patients in: cardiothoracic and vascular surgery; critical care medicine; dentistry and dental surgery; department of neuro sciences; neonatal critical care; nephrology and transplant medicine; orthopedics and traumatology; pediatrics and neonatology; plastic, reconstructive and cosmetic surgery; and pulmonary medicine. Finally, coefficients related to the earthquake and political blockade are not statistically significant, but they remain in the analysis because, if omitted, they may bias coefficients on management strategies (i.e., these events are plausibly related to both management strategies and LOS).
Discussion
Health care has been changing in Nepal, with a large and growing share of private hospitals (Government of Nepal, 2010). Yet, there is limited empirical evidence on the relationship between management and performance of these hospitals. We address this gap using GIH as a case study. Our goal is to support evidence-based decision making and best practices for private hospitals in Nepal and similar contexts.
Using a Pabon Lasso model, we find that BOR and BTR were low under S1 (i.e., CEO duality), perhaps reflecting the challenges of starting inpatient services. Under S2, in which the board was independent from an experienced CEO, GIH had a high BOR and low BTR. However, with a less experienced CEO under S3, GIH performed better for foreign-born patients. This may be attributed to surrogate mothers from India, a large number of whom came to GIH for labour and delivery and then were discharged during this period. Under S4, during which GIH was managed by the Medical Director, it experienced low BOR and high BTR. This is likely due to the major earthquake and political blockade that occurred during the period; GIH was unable keep adequate records during the earthquake, which could mirror ‘unnecessary hospitalization’ and an ‘oversupply of beds’. Finally, we find that GIH performed best under S5, during which there were two CEOs who were independent from the board of directors. This is consistent with evidence that autonomy allows for expedient decision-making in allocating resources (Gholipuri et al., 2013). However, it is important to note that, while GIH faced challenges under other strategies (i.e., starting inpatient services, earthquake, political blockade), it did not under S5. These differences cannot be addressed in the Pabon Lasso model. Given this limitation, we compare findings from the Pabon Lasso model to those of the regression analysis, in which we control for other factors that affected hospital performance. We find that LOS was lowest under S2. This is inconsistent with the Pabon Lasso model, which suggests it was lowest under S1 for native-born patients and S5 for foreign-born patients.
Taken together, our results highlight important differences in hospital performance by indicator (i.e., BOR, BTR, LOS), patient type (i.e., native-born versus foreign-born) and analytical approach. In terms of the latter, both models are consistent with agency theory, which suggests that separation between the CEO and board promotes better performance. However, results from the Pabon Lasso model also support stewardship theory, which suggests that CEO duality is essential to ‘unify and to remove ambiguity from firm leadership’ (Ramdani & van Witteloostuijn, 2010). We argue that, when it comes to evaluating management strategies, private hospitals in Nepal and similar contexts should consider evidence from more than one analytical approach, as well as important differences by performance indicator and patient type.
Strengths and Weaknesses
A strength of this work is that we use unique data (to our knowledge, we are the only researchers with access) to inform an issue that is not currently well-understood. This is important for the efficient delivery of health care in Nepal and other developing countries where private hospitals are increasingly prominent. Another strength is that we consider contextual differences (e.g., native-born versus foreign-born patients) and we use more than one analytical approach. The latter is important because we cannot control for confounding factors in the Pabon Lasso model. In other words, the Pabon Lasso model is useful for describing differences, but we cannot infer whether they were attributable to management or coinciding factors (e.g., patient characteristics, time, earthquake, political blockade). This is possible to some extent in the regression analysis. Nevertheless, our results are correlational and should be interpreted as such.
In terms of weaknesses, we cannot assess quality of care, and we are missing data related to costs, readmissions and deaths. The latter are required for data envelopment analysis, which is a more common approach to assessing hospital performance; it is used by 48% of studies (Hollingsworth, 2008). This technique would allow us to understand the ‘complex nature of the relations between the multiple inputs and multiple outputs involved in many activities’ (Cooper et al., 2007). Another limitation is that we are missing inpatient data due to the earthquake. This distorts our results. For example, GIH had a low BOR under S4, but the reality was likely quite different. Finally, our analysis pertains to inpatients at a leading hospital in Kathmandu, Nepal. Readers should keep this in mind when generalizing results to other patient types (e.g., outpatients), in less established hospitals, more rural areas and/or other developing countries.
Future Research
Our results indicate that separation between the CEO and board may promote better performance (except the Pabon Lasso model favors CEO duality under S1 for average LOS among native-born patients). Perhaps more importantly, we provide evidence that more than one analytical approach should be used to assess hospital performance. For example, although the Pabon Lasso model is useful for describing differences, we cannot infer whether they are attributable to management or coinciding factors. This is addressed by the regression analysis, to some extent, and hospitals should collect data on confounding factors (i.e., those related to both hospital management and performance). Hospitals should also consider standardization (e.g., current procedural terminology) to enhance the external validity of the analysis.
Conclusions
The importance of private hospitals in Nepal and other developing countries has been growing in recent years. However, there is limited empirical evidence on their performance, especially as related to management. Our results indicate that separation between the CEO and board may promote better performance, but there is variation by indicator (i.e., BOR, BTR, LOS), patient type (i.e., native-born versus foreign-born) and analytical approach. We argue that, when it comes to evaluating management strategies, private hospitals in Nepal and similar contexts should consider these important differences.
Appendix A.
Ordinary Least Squares Estimates with Alternate Base Groups for Management Strategy—All Patients.

Footnotes
Acknowledgements
We thank Grande International Hospital for providing the data and Dr Chakra Raj Pandey for contextual information and feedback. We also thank Dr Ewa Kleczyk and Dr Mario Teisl for helpful comments.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Sujita Pandey declares that she has a financial conflict in terms of stock ownership in Grande International Hospital, as well as a personal relationship with the Medical Director.
Funding
The authors disclosed the receipt of the following financial support for the research, authorship and/or publication of this article: Angela Daley recognizes support from the USDA National Institute of Food and Agriculture, Hatch project 1016011.