
Abstract
This study sought to examine the internal consistency reliability and underlying factor structure of the Agency of Health Research on Quality Hospital Survey on Patient Safety Culture (AHRQ HSOPSC) in two large acute care hospitals in a developing country setting (Jamaica). A cross-sectional study was done among 328 doctors and nurses. Reliability (internal consistency) analysis was done for each of the 12 composites and the Cronbach’s Alpha coefficients were reported. Principal axis factor analysis (PA) using Varimax rotation was done to identify the underlying factor structure. The Cronbach’s Alpha coefficient was ≥ 0.60 in ten composites. ‘Overall perception of patient safety’ and ‘staffing’ had Cronbach’s Alpha values of 0.585 and 0.553 respectively. A ten-factor solution (34 items) with factor loading of ≥ 0.40 is the best model fit, and composites are now named ‘handoff and transitions/information exchange,’ ‘communication/feedback,’ ‘frequency of events reported,’ ‘management support for patient safety,’ ‘teamwork in unit,’ ‘non-punitive response to errors,’ ‘overall perception of patient safety,’ ‘supervision/management expectations and actions promoting patient safety,’ ‘organizational learning - continuous improvement’ and ‘staffing’. The AHRQ HSOPSC is generally reliable in this developing country setting and the ten-factor structure is consistent with suggested modifications for the emergent AHRQ HSOPSC Version 2 tool.
Introduction
A key strategy in the movement towards safer care is having a positive patient safety culture in institutions. Patient safety culture is the product of attitudes, competencies, values, perceptions and behaviours among individuals and groups, that demonstrate commitment to, and proficiency in the management and assurance of patient safety (Agency of Healthcare Research and Quality, 2018). Safety culture is a concept that emerged from organisations external to the health sector and is a feature of high reliability organisations (Agency of Healthcare Research and Quality, 2019a). Highly reliable organisations (HROs) display five key characteristics (preoccupation with failure, reluctance to simplify, sensitivity to operations, deference to expertise and commitment to resilience) in ensuring that safety and quality goals are achieved (Veazie et al., 2019).
Consequently, organisations should consistently be thinking about the potential for failure, even in the absence of errors, to avoid complacency. Errors should be used as opportunities to learn and understand systems, and to identify areas for improvement. Complex processes exist in the work environment and should be recognised. Oversimplification potentially ignores nuances and increases safety risks. Efforts therefore should be directed to understanding the underlying factors that contribute to complexity. Highly reliable organisations are also sensitive to systems and processes within organisations that could threaten safety. Moreover, HROs value the involvement of all employees (not only senior staff) in openly sharing concerns and speaking up about issues that may impact safety. Commitment to resilience is a hallmark of HROs (Veazie et al., 2019). Such principles foster positive patient safety cultures.
Patient safety culture is influenced by many factors: perception of the importance of safety; communication; information flow and processing; ability to recognise errors and threats to patient safety; organisational learning; leadership; a blame-free environment; non-punitive approach to incident reporting and analysis; staffing; and accreditations requirements (El-Jardali et al., 2011; Sandars & Cook, 2007).
Assessment of patient safety culture helps in the identification of areas of strengths and weaknesses, and may help to tailor quality improvement strategies. Assessments also serve to evaluate and track changes in patient safety culture over time, and in some cases, meet requirements of regulatory bodies (Nieva & Sorra, 2003). Patient safety culture has been assessed using various instruments. The Manchester Patient Safety Assessment Framework (National Patient Safety Agency, 2006), the safety attitudes questionnaire and the Agency of Health Research on Quality Hospital Survey on Patient Safety Culture (AHRQ HSOPSC) are among the most commonly used instruments for assessing patient safety culture (Sexton et al., 2006).
The AHRQ HSOPSC examines 12 domains/composites in the assessment of patient safety culture: communication openness; feedback and communication about error; frequency of events reported; hand-over and transitions; management support for patient safety; non-punitive response to error; organisational learning—continuous improvement; overall perception of patient safety; staffing; supervision/manager expectation and actions promoting patient safety and teamwork across and within unit (Agency of Healthcare Research and Quality, 2018).
The AHRQ HSOPSC has been employed in many studies (Agency of Healthcare Research and Quality, 2018; Chen & Li, 2010; Ebrahimzadeh et al., 2017; Gauld & Horsburgh, 2012, 2015; Hedsköld et al., 2013; Hooshmand et al., 2014; Sorra & Dyer, 2010) and has been translated into many languages (Agency of Healthcare Research and Quality, 2019b). Construct validity of the AHRQ HSOPSC has been assessed using either exploratory or confirmatory factor analysis. Where exploratory factor analysis was used, the optimal factor structure ranged from 8 to 14 factors (Al Salem et al., 2019; Boussat et al., 2017; Gambashidze et al., 2017; Najjar et al., 2013; Pfeiffer & Manser, 2010; Sorra & Dyer, 2010; Tereanu et al., 2018; Waterson et al., 2019), and the same held true for the confirmatory factor analysis (Eiras et al., 2014; Gambashidze et al., 2017; Nordin et al., 2013; Pfeiffer & Manser, 2010; Sorra & Dyer, 2010; Waterson et al., 2019).
Sorra and Dyer (2010) did multilevel psychometric properties examination of the AHRQ HSOPSC on data available from 331 U.S. hospitals and found that the Cronbach’s α (a measure of internal consistency reliability) of the individual composites was greater than 0.7 except for the staffing composite which had a Cronbach’s α value of 0.62 (Sorra & Dyer, 2010). Internal consistency reliability of the AHRQ HSOPSC has also been reported in a systematic review of 62 studies (Waterson et al., 2019). The composite with the highest mean Cronbach’s α was ‘frequency of events reported’ with a value of 0.83. Composites with mean Cronbach’s α values of less 0.70 were ‘communication openness’, ‘staffing’, ‘non-punitive response to error’, ‘organisational learning’ and ‘overall perception of errors’ (Waterson et al., 2019). The use of the tool in its original format has been cited as one reason for variation in its performance in various settings. Other reasons include making modifications/deletion without appropriate guidance, as well as translation of the tool to other languages. Waterson et al. (2019) in a systematic review of the AHRQ HSOPSC equally caution users about the use of the unmodified version of the tool (Waterson et al., 2019). Most studies that attest to the reliability of the AHRQ HSOPSC have been carried out in developed countries (mainly in Europe, North America and Japan) or countries with relatively high per capita income (Waterson et al., 2019).
Hospitals offer a range of complex services and literature points to adverse events and medical errors predominating in this setting (de Vries et al., 2008). A positive patient safety culture is a key element to enhance patient safety. Yet, in the Jamaican context, there is little published, peer-reviewed or grey literature about patient safety culture in large acute care hospitals. Pioneer work (Thompson, 2021) has been done recently assessing patient safety culture in two large acute care hospitals in Jamaica, one of few studies ever done in developing country settings. The use of findings to guide quality improvement initiatives and their application to policy formulation is predicated on the use of a valid and reliable instrument in measuring patient safety culture and its constituent composites. Reliability of an instrument is influenced by the group to which it is applied, and the setting in which it is administered (Dixon-Woods et al., 2014; Wagner et al., 2013). Instruments, whose reliability have been satisfactory in developed country settings are not necessarily reliable when used in developing country settings, due to cultural, linguistic, and organisational differences. It is therefore important to establish the reliability of the AHRQ HSOPSC instrument when used in Jamaica or similar developing country settings. This article examines the internal consistency reliability and the underlying factor structure of the AHRQ’s hospital survey on patient safety culture in a developing country setting (Jamaica). By exploring psychometric properties of the AHRQ HSOPSC, the appropriateness of the instrument in various settings and contexts, can be ascertained.
Methods
In 2019, a cross sectional study was done among 328 doctors and nurses (working in their institutions for 6 months or more) in two Type A hospitals (referred to Institution A and Institution B in this study) in the South-East Regional Health Authority in Jamaica. Type A institutions are large acute care, teaching hospitals, with bed capacity of 300–500. The minimum sample size was determined using data from the AHRQ HSOPSC 2018 report (Agency of Healthcare Research and Quality, 2018). The estimated (November 2018) number of doctors and nurses at the institutions studied was 2257. The weakest composite (‘non-punitive response to errors’) had a positive percent score of 47%; assessment of which is critical in determining patient safety culture, a major objective of this study. Assuming this figure and applying the usual 95% confidence interval, and 5% margin of error, the minimum required sample was 328 (Raosoft, 2004).
A stratified random sampling method was used to select persons for sample and was done proportionate to size of institution (Institution A—37.8% [n = 124] and Institution B—62.2% [n = 204]). Further stratification was done to represent the nurse–doctor composition in each institution (Institution A—64%:36%; Institution B—62%:38%). Informed consent was obtained from all participants and ethical approvals were received from the Mona Campus Research Ethics Committee and the South-East Regional Health Authority Ethics Committee for conduct of the study.
The AHRQ HSOPSC Version 1.0 tool was utilised with permission for collecting data. The AHRQ HSOPSC Version 1.0 consisted of 42 items, which were broken down into 12 composite measures (defined in Table 1). Five-point Likert type responses were used for each question. Each composite consists of three to four items. The tool also consisted of two questions regarding patient safety grade and the number of events reported in the last year.
Definition of AHRQ HSOPSC Composites.

Reliability (internal consistency) analysis was done for each of the 12 composites of the AHRQ HSOPSC and the Cronbach’s α coefficients were reported. Data from the AHRQ HSOPSC tool were subject to principal axis factor analysis (PA) using Varimax rotation; allowing for the distillation of the items into components that convey the main constructs which underlie these items in the Jamaican context. Values for the determinant, Keiser–Meyer–Olkin (KMO) test of sampling adequacy and Bartlett’s test of sphericity were used to confirm that criteria for factor analysis were met. Items correlated with each other without multicollinearity.
Exploratory factor analysis was done. In establishing the underlying simple factor structure of AHRQ HSOPSC tool, factors with primary factor loading or cross-loadings of 0.4 were used. Items were grouped based on their highest loading factor. A scree plot was also used to identify the number of factor components that should be retained in the emergent factor structure by identification of the pattern of eigenvalue decline. Consistent with convention, only components with eigenvalues of one or greater were retained (Field, 2005; James et al., 2004).
Results
Description of Participants
As seen in Table 2, the majority (81.4%) of participants were female. Concerning marital status, almost 60% reported that they were not in union. Most (51.8%) participants were in the age category 26–35 years and registered nurses constituted the majority (53.7%). The plurality (26.5%) of participants was from surgical units. Participants from paediatric units accounted for 6.7%.
Socio-demographic Characteristics of Study Participants.

*‘Other’ included participants from radiology departments and labs.
Descriptive Statistics
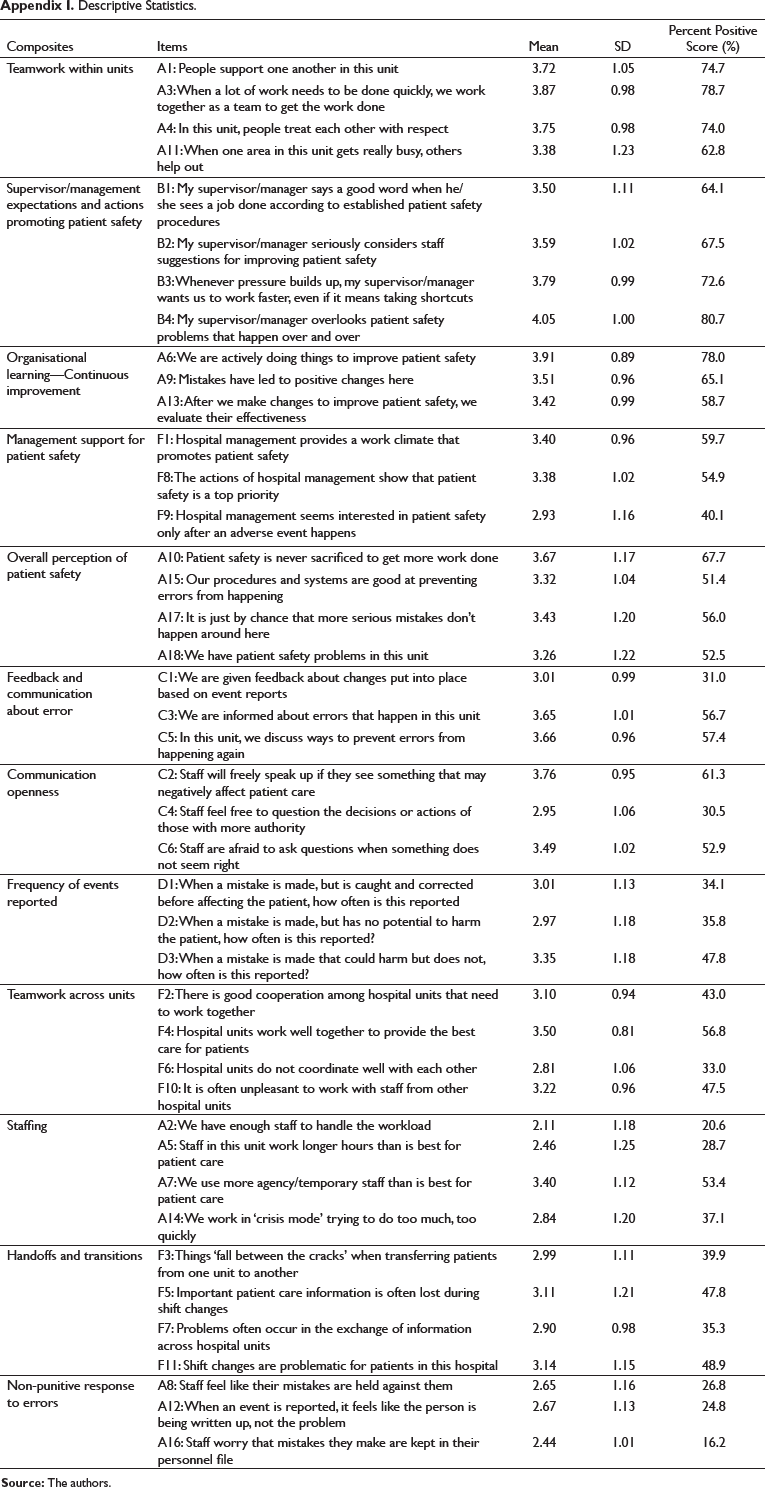
The mean, standard deviation and percent positive score (proportion of positive responses) for each of the 42 items in the tool is reported in Appendix I. Individual items had mean score ranging from 2.11 (SD = 1.18) to 4.05 (SD = 1.0). Positive percent scores ranged from 16.2% to 80.7% for individual items.
Psychometric Properties of the AHRQ Hospital Survey on Patient Safety Culture
Reliability of the Instrument
Cronbach’s α was also derived for the composites, each consisting of three or four items. As seen in Table 3, the Cronbach’s α coefficient was ≥ 0.60 in ten composites. The ‘overall perception of patient safety’ and ‘staffing’ composites had Cronbach’s α values of 0.59 and 0.55 respectively.
Cronbach’s α by Patient Safety Culture Composites.

Exploratory Factor Analysis of the AHRQ Hospital Survey on Patient Safety Culture
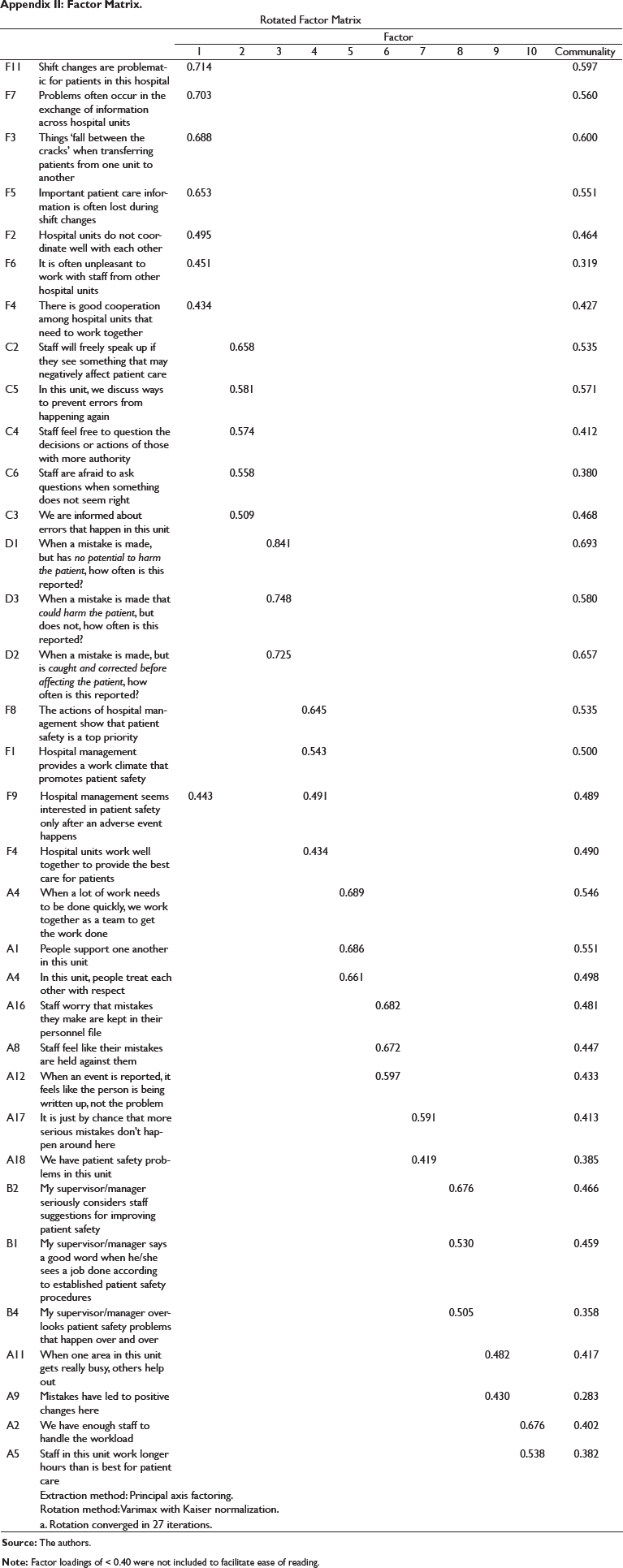
Principal axis factor analysis with Varimax rotation was done to determine the underlying structure of the 42-item AHRQ’s hospital survey on patient safety culture tool in the current study. The KMO measure of sampling adequacy was 0.849 and Bartlett’s Test of Sphericity was χ2 (780) = 4300.02, p ≤ 0.001, indicating suitability of the data for factor analysis. A ten-factor solution with factor loading of ≥ 0.40 showed the best model fit among the population studied (see Appendix I). Eight items were eliminated as they did not meet the criteria of having a factor loading of 0.40 and above (Appendix II). The scree plot for the final model is displayed in Figure 1 with 10 factors having eigenvalues ≥ 1. These ten factors explained 48.31% of variance in patient-safety culture scores.
Scree Plot for the AHRQ Hospital Survey of Patient Safety Culture among Health Workers.

One item (hospital management seems interested in-patient safety only after an adverse event happens) cross-loaded on factor one and factor four. This item was assigned to factor four because the primary loading was higher (0.49) on that factor, compared to factor one (0.44).
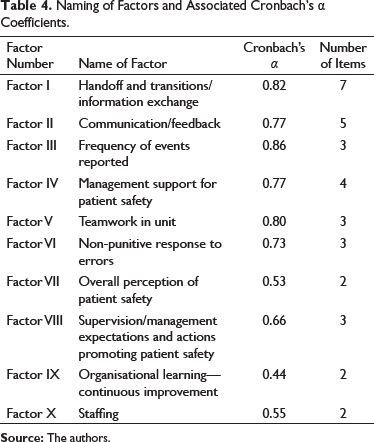
Table 4 summarises and names the 10 factors that were extracted, and provides the associated Cronbach’s α coefficients for each composite. Three of the ten composites (overall perception of patient safety, organisational learning—continuous improvement and staffing) had Cronbach’s α coefficients of less than 0.6. ‘Factor I’ combined items from the composites ‘teamwork across unit’ and ‘handoffs and transition,’ now called ‘handoff and transitions/information exchange.’ Factor II is also a combination of two composites; ‘feedback and communication about error’ and ‘communication openness’ now called/named ‘communication/feedback’.
Naming of Factors and Associated Cronbach’s α Coefficients.
Discussion
Outcomes of patient safety culture assessments are often used as a basis for quality improvement activities/initiatives. It is therefore necessary that the reliability and the validity of standardised instruments be evaluated to ensure that the findings resulting from its use can be appropriately applied. In this study, the internal consistency (reliability) as measured by the Cronbach’s α was done for each of the 12 composites. Cronbach’s α values in this study ranged from approximately 0.6–0.9. Acceptable values for the reliability of instruments vary in the literature, with authors suggesting lower limits of 0.6–0.7 (Field, 2013; George & Mallery, 2019; Taber, 2018; van Griethuijsen et al., 2015). The initial assessment of the HSOPSC instrument used 0.60 as an acceptable value (Sorra & Nieva, 2004).
In this study, all the composites except for staffing and overall perception of patient safety had Cronbach’s α values greater than 0.60. The staffing composite had the lowest Cronbach’s α value of 0.55. This finding is similar to the mean of 0.56 reported in a systematic review of the psychometric properties of the tool by Waterson et al. (2019). Studies have documented very poor internal consistency on this composite (below 0.40), however, in all these studies, the tool was translated in other languages and translation can affect reliability (Waterson et al., 2019). Cronbach’s α of 0.80 or above have been reported in studies done in the USA, where the instrument was in English.
When exploratory factor analysis was done in this study, only two items were loaded on the staffing composite. The Cronbach’s α value for the two-item was similar to the four-item (original tool). Two items did not load on the staffing composite: ‘we use more agency/temporary staff that is best for patient care’ and ‘we work in “crisis mode” trying to do too much, too quickly’. The use of the staffing composite with the four items is therefore questionable and warrants further review to ensure that items have good internal consistency. The composite may have performed poorly in our context because of wording issues. The word ‘agency’ and ‘temporary staff’ may have been interpreted differently. The use of the term ‘sessional staff’ may have been more relevant in our setting. Authors have advocated nuanced modification to the tool to ensure suitability for use (Waterson et al., 2019).
The AHRQ has launched a new version of the tool (late 2019), which is now being used. The new tool has retained the four items for the staffing composite but modification has been done to the wording of the two aforementioned items that were included in the tool. The reported internal consistency reliability for the staffing composite is α = 0.67, and is still the lowest internal consistency reliability value among the composites in the new tool. Assessing ‘staffing’ is important in determining patient safety culture; the constituent items may need to be further adjusted to ensure good internal consistent reliability of the items.
The second composite that had relatively poor internal consistency was overall perception of patient safety, which had Cronbach’s α of 0.59. The average Cronbach’s α coefficient reported by Waterson et al. was 0.60 (Waterson et al., 2019). Reis et al. (2019) purported that the composite ‘overall perception of patient safety’ contains items that are negatively worded, which users have reported a difficulty in interpreting, therefore, threatening the internal consistency reliability of the composite (Reis et al., 2019). All other composites had Cronbach’s α coefficient above 0.70, demonstrating overall good internal consistency of the items used to assess the composites for patient safety culture.
Various factor structures of HSOPSC exist in the literature. This variation can be attributed to the differences among the population studied such as language, methodological techniques and the overall culture of the sample. A recent review conducted by Waterson et al. (2019) revealed that studies in which exploratory factor analysis was performed reported 8–14 factor structures while the majority of those who performed confirmatory factor analysis confirmed a 12-factor structure. In our study, a ten-factor structure was elucidated, and is comparable with that reported by Sarac et al. (2011), Occelli et al. (2013), Perneger et al. (2014) and Bodur and Filiz (2010). The original AHRQ HSOPSC had a 12-factor structure, however, recent factor analysis had resulted in the revamping of the instrument based on a ten-factor structure, consistent with our findings.
While two factors (with its constituent items) were similar to the original composition of the HSOPSC tool (factor III—‘frequency of events reported’, factor VI—‘non-punitive response to error’), there were several deviations. One deviation, though not a unique finding (Perneger et al., 2014), was the combination of items from two composites, as in the case of factors I and II in this study. ‘Factor I’ combined items from ‘teamwork across unit’ and ‘handoffs and transition’. Conceptually, these items together reflect coordination across units and relaying of patient information, and was found to be similar to study done in the Netherlands (Smits et al., 2008). In fact, in the new version (version 2) of the HSOPSC, these two dimensions are now combined, and only three items are used to assess this composite (Agency of Healthcare Research and Quality, 2019c). Factor II is also a combination of two composites; ‘feedback and communication about error’ and ‘communication openness’ now called ‘communication/feedback’. This reveals the important role that feedback plays in facilitating open communication among staff. For example, if staff receive constructive feedback after making a report, it is highly likely that they would be motivated to continue doing so when the need arises (Kroll et al., 2008; O’Connor et al., 2010).
Another deviation is seen in Factor IV called ‘management support for patient safety’ where the item ‘hospital units work well together to provide best care for patients’ (originally a part of teamwork across unit) loaded unto this Factor. One item (‘hospital seems interested in patient safety only after an adverse event happens’) from Factor IV, cross-loaded on Factor I (called ‘handoff and transitions/information exchange’), and illustrates inter-connectedness across domains. This highlights the vital role that management should play in care coordination and information exchange in their support of positive patient safety culture.
‘Factor V’ is concerned with teamwork within unit. All, except one of the original items loaded on to this factor. Unlike the original AHRQ’s tool with composite consisting three or four items, three of the factors extracted in this study had only two items. These were: factor VII—‘overall perception of patient safety’, factor IX—‘organisational learning—continuous improvement’ and factor X—‘staffing’. The Cronbach’s α coefficient for these three factors were 0.53, 0.44 and 0.55 respectively. These results are not surprising as at least three items are needed to obtain valid/good Cronbach’s α scores (Hajjar, 2018).
Overall, eight items did not load unto any factor. Four of the eight items that did not load—‘whenever pressure builds up, my supervisor/manager wants us to work faster, even if it means taking shortcuts’, ‘patient safety is never sacrificed to get more work done’, ‘we use more agency/temporary staff that is best for patient care’ and ‘we work in “crisis mode” trying to do too much, too quickly’—revolve around blatantly unsafe occurrences in the institution. These with their factor loadings all below 0.4, may indicate respondents’ reluctance in highlighting negative viewpoint/perspectives about their institutions. Sorra and Dyer (2010) purport that responses are influenced by both ‘unit and hospital membership’ (Sorra & Dyer, 2010). Three items: ‘we are actively doing things to improve patient safety’; ‘after we make changes to improve patient safety, we evaluate their effectiveness’; and ‘our procedures and systems are good at preventing errors from happening’, may reflect activities that the staff perceive to be management-related activities. They therefore may have removed themselves from the collective ‘we’ or ‘our’ and responses to the questions may have varied greatly by participants.
Our exploration of the factor structure and the loading propensities of the constituent items in the various composites provide insights for the future development of the AHRQ HSOPSC tool. The tool appears to be a relatively reliable one for use in Jamaica, and similar developing country settings. It has the potential to direct hospital leaders and managers to areas of excellence that should be maintained and areas of deficit that should be addressed. Nevertheless, minor weaknesses of the tool should be recognised, and efforts made to improve it.
This study is the first of its kind in Jamaica and the Caribbean. A validated instrument used to assess patient safety culture facilitated comparison of results with those published from other hospitals and other international settings. The sample size in this study was relatively large, however, the study was restricted to two acute care hospitals in a specific geographic region, making it difficult to generalise the findings to other hospitals. Exploratory factor analysis was done in this study, and the results emanated from initial forays pertaining to the factor structure of the AHRQ HSOPSC. Confirmatory factor analysis will be useful in the future to definitively establish in detail, the fit of the data and factor structure observed in the study with theoretically hypothesised models in the psychometric assessment and revision of the emergent AHRQ HSOPSC version 2 instrument.
Conclusion
The instrument was found to be relatively reliable and an underlying 10-factor structure is suggested by our finding. The study provides further evidence and support the use of a 10-factor structure; now being rolled-out by the AHRQ as the HSOPSC tool evolves. It also speaks positively to the applicability of this 10-factor structure in not only developed, but developing country settings. There is need to revise the constituent items for the staffing and overall perception of patient safety which had low internal consistency reliability.
Ethics Review Boards
Mona Campus Research Ethics Committee (ECP 111, 18/19)
South-East Regional Health Authority Ethics Committee
Descriptive Statistics.
Factor Matrix.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.