
Abstract
The World Health Organization declared the Coronavirus Disease 2019 (COVID-19) pandemic a public health emergency of international concern on 30 January, which caused difficulties among the healthcare professionals (HCPs). Since this pandemic led to strict use of rules and regulations in maintaining physical distancing, a turn was experienced in communication. This study is aimed at assessing communication skills between HCPs and patients before, during and to compare communication skills between them before and during the COVID-19 pandemic. A descriptive cross-sectional study was conducted at Pravara Rural Hospital, Loni, Maharashtra. Samples were included based upon the inclusion and exclusion criteria. Results were obtained with the help of statistical analysis. The present study shows that certain components of communication are changed when comparing before and during the COVID-19 pandemic. To curb the fear of HCP, certain measures can be implemented to reduce anxiety such as informative videos, images, brochures and many more.
Introduction
The World Health Organization (WHO) declared the outbreak of Coronavirus Disease 2019 (COVID-19) a public health emergency of international concern on 30 January (Ratzana et al., 2020). COVID 19 caused by a severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) emerged in China, following the outbreak, declared as a pandemic by WHO on 11 March 2020 and raised an alert due to its spread across the globe (Ratzana et al., 2020). Coronavirus belongs to the Coronaviridae family, has a diameter of 65–125 nm and contains a single strand of ribonucleic acid (RNA) with lengths from 26 to 32 kb comprising of alpha, beta, gamma, SARS coronavirus (SARS-COV), influenza A subtype (H5N1) influenza, H1N1 2009 and Middle East respiratory syndrome coronavirus (MERS-COV).
This pandemic led communication to take a turn between the patient and healthcare professional (HCP). With the limited time clinicians have and the barriers that arise during the pandemic, the need for understanding and using the components of language and communicate effectively is essential (Senicola et al., 2020). Information can be given by telephone, video call or e-mail and physicians aim to compensate for these egregious communication gaps through non-verbal tools such as tone, pause and inflection (Marra et al., 2020).
The integral management is effective communication. Patients who understand their doctors acknowledge health problems, treatment, modify their behaviour and follow medication schedules (Travaline et al., 2005). Many researchers concluded that interaction is vital and essential. The pandemic has generated unsubstantiated rumours and conspiracy theories related to the origin, transmission, preventing and treating and the actions governments have taken to limit its spread (Vraga & Jacobsen, 2005). As a result, appropriate information should be delivered employing interaction.
The physician–patient relationship has proven traditionally to be healthy, which leads to the fast recovery of a patient. In the medical profession, trust is seen as a global attribute of treatment relationships, encompassing satisfaction and has been viewed as vital (Hall et al., 2010). The quality of physician–patient communication in primary care visits is related to patient satisfaction, quality of data collection, utilisation patterns and clinical outcomes (Tallman et al., 2007). Improvement in communication has brought satisfaction for HCP and patients. A patient’s visit involves expectations, trust and hope; similarly, from a doctor’s point of view, empathy and compassion, which are responsible for effectiveness or ineffectiveness in interaction (Benedetti, 2013). The word ‘interaction’ is a Latin word meaning ‘direct reciprocal dialogue and to act upon each other and have influences on’ (Ruler, 2018).
A patient may have heightened expectations due to the current situation, but because of guidelines imposed, it has added an amount of constraint on the HCP (Costaa et al., 2016). The specific restrictions vary between countries, and government policies to handle the COVID-19 outbreak have involved closing schools, non-essential physical shops and businesses, and limiting public transportation and spaces (Nguyen et al., 2020).
The pandemic has encouraged a new phase of real-time, peer-to-peer sharing (Wang et al., 2020). It has led to the use of personal protective equipment (PPE) by the HCP, which acts as a barrier for infection and creates difficulty in communication. Poor health media literacy is common and witnesses the amplification of unverified information, triggering misunderstandings, fear and reduced trust, which inhibit responses to the pandemic (Wang et al., 2020). Wearing masks, goggles and splash shields allows the eyes to be visible, but it conveys commitment and concern as a substitute and paralinguistic help puts meaning and variability into speech, but N-95 masks attenuate sound and amplify speech (Senicola et al., 2020). Thus, this study aims to find out the impact of the COVID-19 pandemic on communication between HCP and patients.
Aims and Objectives
The study was aimed to assess communication skills between HCP and patients before and during and to compare communication skills between them before and during the COVID-19 pandemic.
Methods
A descriptive cross-sectional study was conducted at the Pravara Rural Hospital (PRH), Loni. Samples were included based upon the inclusion and exclusion criteria. HCPs treated patients before and during the COVID-19 pandemic, and both males and females were included. HCPs who were unwilling to consent were excluded. Systematic random sampling was used, and approximately 20% of all HCPs participated (75 physicians and surgeons, 25 dentists, 20 physiotherapists, 80 nurses). Written and informed consent was obtained. Healthcare Professionals Communication Skills questionnaire (HP-CSS) was administered. With the help of descriptive statistics, data were analysed, and results were obtained.
Results
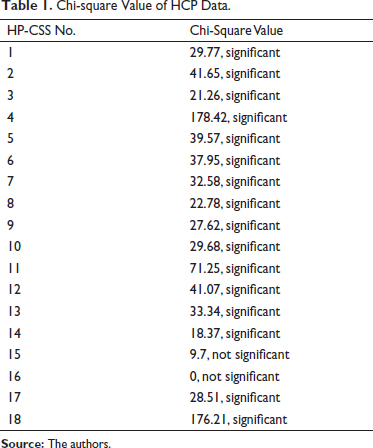
Tables 1, 2 and Figure 1 show data of HCPs. The results showed that there was a significant change in communication, especially in Question 4 ‘When the patient speaks I show interest through body gestures (nodding, eye contact, smile)’ and 18 ‘I find it difficult to ask for information from patient’. The 18th question has a chi-square value of 176.21, which is the highest in the table when compared with the critical value of 11.07. The difference is seen in the values of Question 4, which is 178.42 and is the most significant. The same trend is seen in Questions 11 and 2. Figure 1 presents a graphical representation of the chi-square value across 18 questions. As shown in the Table 1, Question 4 was marked as 5 by 82.5% on the Likert’s scale, while 12.5% marked it as 4 before the pandemic. The same question was marked as 3 by 47.5% during the pandemic. Question 18 was marked as 5 by 86%, which came down to 3 by 68% of HCPs. About 81.5% of the HCPs marked the 11th question as 5, which came down to 43% marking the same question as 5 during the pandemic. The rest of the questions that include 15 and 16 do not show statistical significance.
Chi-square Value of HCP Data.
Percentage Distribution of HP-CSS of HCP Data.
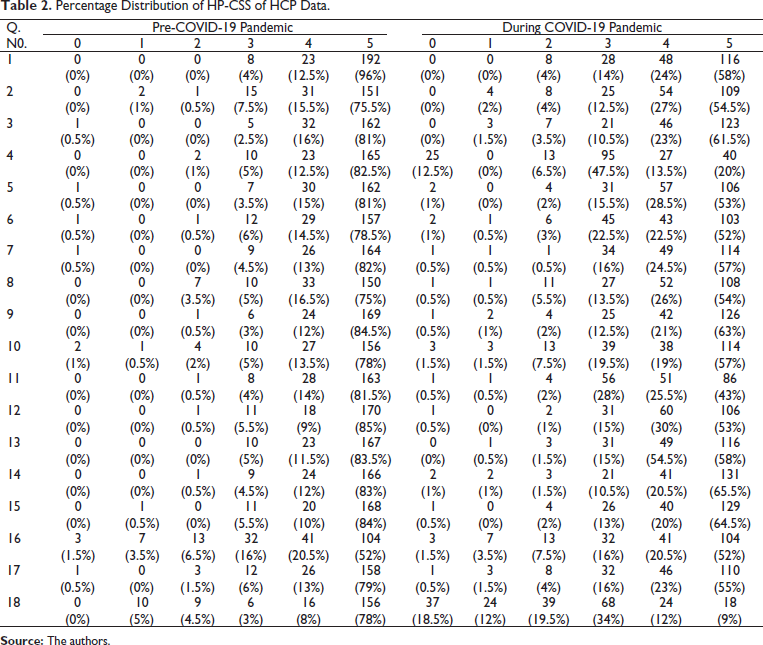

Table 3 shows data of physicians and surgeons (PS). The 18th question ‘I find it difficult to ask for information from patient’ was marked as 5 by 70.2% of the PSs before the pandemic, which came down to 11.7% during the pandemic. The fourth question ‘When the patient speaks, I show interest through body gestures (nodding, eye contact, smile)’ was marked as 5 by 76.7% of the PSs before the pandemic, which came down to 16.9% during the pandemic. The second question ‘I explore the emotions of my patient’ was marked as 5 by 74.1% before the pandemic, which came down to 35.1% during the pandemic. The 10th question ‘When a patient does something that does not seem right, I express my disagreement or discomfort’ was marked as 5 by 77.2% before the pandemic, which came down to 48.1% of the HCPs who marked the same question as 5 during the pandemic.
Percentage Distribution of HP-CSS for PS.
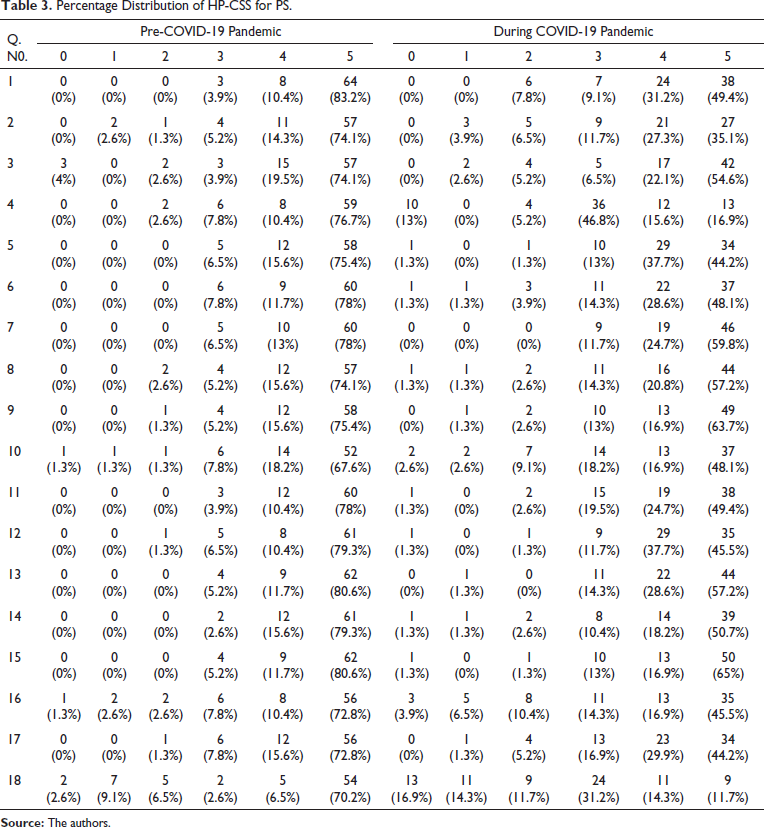
Table 4 presents the data of dentists. In Question 18, ‘I find it difficult to ask for information from patient’, about 80% of the dentists gave the rating of 5 before the pandemic, and the same question was given a rating of 5 by 5% of the dentists. Question 11 was given a rating of 5 by 76% of the dentists before the pandemic, which came down to 44% during the pandemic. The fourth question was given a rating of 5 by 80% of HCPs before the pandemic; this came down to 60% during the pandemic who gave the rating of 5 to the same question.
Percentage Distribution of HP-CSS for Dentists.

Table 5 indicates the data of physiotherapists. Before the pandemic, about 65% of the physiotherapists gave a rating of 5 on the Likert’s scale for the 18th question ‘I find it difficult to ask for information from patient’; this number reduced to 10% during the pandemic. The fourth question ‘When the patient speaks; I show interest through body gestures (nodding, eye contact, smile)’ reduced from 85% to 45% during the pandemic. The eighth question ‘When I give information, I use silence to allow to assimilate what I am saying’ was given a rating of 5 by 60% of the physiotherapists before the pandemic, which came down to 25% during the pandemic. The 12th question ‘I try to understand the feeling of my patient’ was given a rating of 5 by 80% of the physiotherapists before the pandemic, which came down to 35% during the pandemic.
Percentage Distribution of HP-CSS for Physiotherapists.
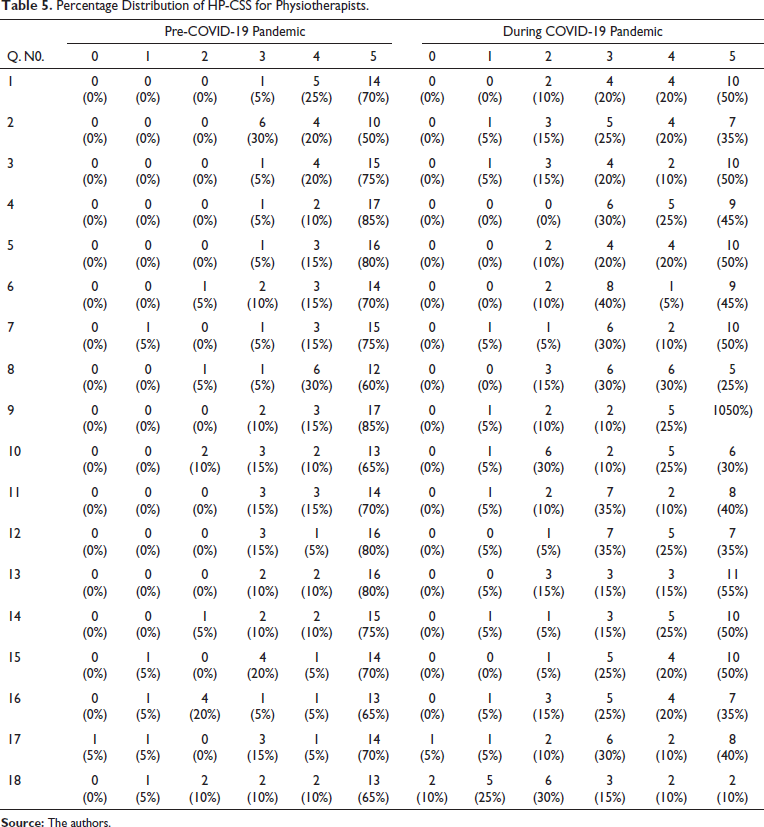
Table 6 presents the data of nurses. The fourth question ‘When the patient speaks; I show interest through body gestures (nodding, eye contact, smile)’ was marked as 5 by 86.25% of the nurses before the pandemic, which came down to 3.75% during the pandemic. The 18th question ‘I find it difficult to ask for information from patient’ was marked as 5 by 86.25% of the nurses, which came down to 7.5% during the pandemic. The 11th question ‘I dedicate time to listen and try to understand the needs of patient’ was given a rating of 5 by 87.5% of the nurses, which came down to 37.5% during the pandemic.
Percentage Distribution of HP-CSS for Nurses.

Discussion
The present study was conducted to evaluate whether there is a change in communication between HCPs and patients before and during the COVID-19 pandemic. Certain HCPs who are in immediate contact with the patients, such as physicians and surgeons, including paediatricians, obstetricians, gynaecologists, general surgeons, dentists, physiotherapists and nurses, were included. A notable change in communication was observed between HCPs and patients in certain components.
When the patient spoke, the HCP showed interest through body gestures (nodding, eye contact, smile) earlier, but a change was observed because the mask does not allow the patient to see the expressions of the HCP, and PPE kits make it difficult for the professional to work. ‘Having a clear voice within government helps avoid a “talking heads” dynamic that undermines the development of a cohesive strategy’ says research on enhancing global health communication during a crisis: lessons from the COVID-19 pandemic (Ratzana et al., 2020).
The HCP finds it difficult to ask for information from a patient because the PPE acts as a barrier making the HCP speak loudly as his voice turns out to be less audible. They try to maintain physical distancing, making it difficult to understand the patient. As a result, it is difficult to ask for information from patients. Researchers say that
Wearing masks, goggles, and splash-shields allow the eyes to be visible, but eye gaze with a patient can convey commitment and concern as a substitute for other facial expressions and paralinguistic (pitch, inflection, tone of voice) help put meaning and variability into speech, but N-95 masks attenuate sound, muffling, or amplifying speech (Senicola et al., 2020).
HCPs find it difficult to respect the patients because they are in a continuous hurry with a constant workload. Exploring the emotions of the patients is now challenging because of reduced conversations with patients. It is difficult to respect the autonomy and freedom of patients. The HCP finds it difficult to dedicate time to listen and try to understand the needs of the patient because there is a fear of the spread of infection and a compulsion to follow hospital protocols.
A change is seen in providing information to patients to reduce contact with the patient; HCPs try to provide quick and important information. The HCP listens to a patient without prejudice, regardless of their physical mannerism and the form of expression before COVID-19, but, at present, if the person is not wearing a mask or maintaining physical distance, then this has changed. HCPs express their opinion and desires clearly to the patients and use silence to allow to assimilate what they say, but it is difficult because of the fear of infection.
Before the pandemic, when a patient did something that did not seem right, the HCP would express disagreement and/or dedicate time to listen and understand the needs of the patient, but because of the high risk of infection and continuous exposure with rising cases, this has changed. Presently, with the increasing COVID-19 cases and increased risk of asymptomatic patients, HCPs provide fewer and only important health information as they find it difficult to request patients.
HCPs have started dedicating less time to listen to patients and try to understand their needs. The reason behind this is the fear of the spread of infection. Although, at present, vaccination drive has been ongoing, the efficacy is not 100%. So, there are chances of infection. As a result, many HCPs said that because of the spread of infection, they try to maintain physical distance and try to reduce the treatment time as a preventive measure. Most of them asserted that although they have reduced spending time with the patient, the treatment has not been affected.
Patients and their families perceive not only the clinical results but also the personal attitudes, closeness and psychological support from the care teams as quoted by researchers (Marra et al., 2020). Working with asymptomatic patients has created a stressful environment among HCPs and patients. Since many patients stay with their families, there is a constant fear of the spread of infection to their loved ones if they are infected. Many workers already have certain comorbidities making them more cautious about themselves.
Physicians and surgeons come in close proximity to the patients. Because of the masks and shields, their expressions are hidden from the HCPs. There is a reduction in the time the HCP usually spends with the patients—the reason could be because of the fear of infection. Due to social scenarios and fear, the patient may hide symptoms, creating undue fear in the minds of HCPs, and the HCPs in turn find it difficult to request information from patients.
Dentists say that they find it difficult to ask for information from the patients. The reason could be because they work in close proximity to patients, which is a requirement for all dental procedures. It requires the patient to remove his/her mask, which increases the potential risk and, as a result, changes the communication. Thus, it is difficult to ask for information from the patients.
Physiotherapists work with the patients for a longer period. The treatment duration may range to about 30–40 min. It has become difficult to respect the autonomy and freedom of the patient because there is a constant risk of infection, and it has become mandatory to make sure that the patient follows all the measures to keep the infection at bay. Certain physical mannerisms like manual contact or standing in close proximity of the patient is reduced from the physiotherapist’s point of view to maintain the norms of social distancing. To reduce the treatment time, a physiotherapist might have reduced the time that they usually give to understand what he/she is saying. Giving instructions clearly usually requires speaking slowly, but due to hectic working hours and facial gear, it has become difficult due to the pandemic. It is difficult to understand the feelings of the patient and ask for information and request the patient because of the pandemic (Marra et al., 2020).
Usually, nurses are in frequent contact with the patients. Because of the constant social pressure of someone being detected as positive and have to undergo quarantine, it has become difficult for HCPs to retrieve information from the patient. Similarly, gestures are also reduced due to the PPE. Research has revealed that professionals in the field of communication, education and health behaviour need to take responsibility for carefully evaluating what is known and insights currently emerging (Finset et al., 2020).
Conclusion
The present study shows that certain components of the HP-CSS are affected when comparing before and during the COVID-19 pandemic. The HCPs have said that it has been difficult to ask for information from the patient. In addition, there are few changes because of the PPE, which hides facial expressions. Rest of the components like understanding and emotions have remained the same.
Key Points
The study aimed to assess communication skills between HCPs and patients before and during and to compare communication skills between them before and during the COVID-19 pandemic.
A notable change in communication was observed between HCPs and patients in certain components.
The HCPs assert that it is difficult to ask for information from the patient.
Exploring the emotions of the patients is now challenging because of the PPE kits and reduced conversation with the patients.
Strengths and Limitations
The major strength of the study is it lies in a 100% response rate during the critical phase of COVID-19 in the rural population. In addition, this was the first of a kind study in this specific geographical area. The survey tool used in the study also helped in improving the existing knowledge of the HCPs and made him/her aware of the components that need to be worked upon.
Certain limitations had to be considered as the study was conducted only in one rural hospital. This survey was conducted on the HCP’s perspective, and the patient’s perspective was not considered.
Recommendations
To curb the fear of HCPs, certain measures can be implemented to reduce anxiety. Information about COVID–19 can be given with the help of videos, images, brochures and many more. COVID-19 screening form can be given so that the fear factor can be reduced, and there can be free interaction as well. For a better understanding of the treatment and precautions, video demonstrations can be carried out. Certain use of hand gestures at this time can be helpful. After vaccination, this scenario may change, but awareness of hygiene and standard precautions should be followed to reduce the risk of infection.
Footnotes
Acknowledgements
Indeed, I am very glad to present this research study. I take this opportunity to thank all the hands that have joined together to make this project a success. It is indeed my privilege to express my sincere gratitude to Dr Tejas Borkar (PT), Dr APJ Abdul Kalam College of Physiotherapy, Loni, for her valuable advice and guidance.
I wish to express my deep gratitude to my parents who have supported me throughout this journey with constant motivation.
I wish to thank all the participants for their cooperation and tolerance towards this project. I would like to bow down to the almighty whose blessings, love and encouragement have always been a catalyst in all walks of my life.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
Ethical permission was obtained from Institutional Ethical Committee held on 16 December 2020 at Dr APJ Abdul Kalam College of Physiotherapy, Pravara Institute of Medical Sciences, Loni , Maharashtra 413736, India.
Abbreviations
WHO: World Health Organization
COVID-19: Coronavirus Disease 2019
HP-CSS: Healthcare Professionals Communication Skills questionnaire
PS: Physicians and surgeons
P: Physiotherapists
D: Dentists
N: Nurses
Fig: Figure
PRH: Pravara Rural Hospital