
Abstract
Healthy ageing is a new paradigm that describes the possibility of better ageing experience in contrast to the traditional notion of ageing. The aim of this scoping review was to map literature on healthy ageing in the context of low and middle-income countries (LMICs). A five-step scoping review procedure was used to synthesise the conceptualisation of healthy ageing and its measurement approach and to summarise key evidences on healthy ageing. Our descriptive summary analysis shows that the majority of the studies conceptualised healthy ageing under physical capabilities, cognitive functions, metabolic and physiological health and psychological well-being domains with more of objective measurement approach. We identified a number of studies that can be relevant to consider for public health policy. Future research should also focus on neurobiological ageing aspects as such studies were found to be very rare in the review. Our review identified that there is limited number of studies conducted in some LMICs where the growth of population ageing is an emerging concern.
Introduction
Population ageing has become one of the key policy concerns all over the world. The demographic transition was driven by factors such as increasing life expectancy and fall in fertility (Bloom et al., 2010; Bloom & Luca, 2016; World Health Organization, 2015). These two factors were influenced by improvements in living conditions, better health technology, improved education, improved sanitation, the decline in child mortality, accessibility to birth control and family planning measures (Bloom & Luca, 2016) and economic growth (Preston, 1975). It is projected that the number of persons aged above 60 years will increase to almost 2 billion from 600 million by 2050, and which will be 21% of total global population (United Nations, 2002). Researches also projected that the demographic transition would be more rapid in developing countries (Bloom & Luca, 2016; United Nations, 2002). Demographic transition has a clear association with the epidemiological transition (Frenk et al., 1989; Omran, 2005). Major health risk factors in the later stages of the combined demographic and epidemiological transition would be concentrated among the elderly population. Previous studies have observed this concern in different ways such as; the emergence of triple burden of diseases (Ortiz & Abrigo, 2017) health transition (Frenk et al., 1989) and the fourth stage of epidemiological transition (Olshansky & Ault, 1986). Given this high probability of health and non-health risks among the elderly population than any other age cohorts, there is an urge to explore appropriate policy intervention to ensure healthy and productive ageing.
Recent researches have focused on healthy life expectancy (HLE) gained by adding years to life expectancy (LE) at birth. There is evidence for those cohorts entering old age now are relatively healthier than the earlier generations (Bloom et al., 2015). Such an improvement in health or compression of morbidity is possible through managing various intrinsic and extrinsic factors (World Health Organization, 2015). Evidence shows that compression of morbidity is possible by adapting lifestyle-related changes (Fries, 1996, 2012; Hubert et al., 2002), low prevalence of health risks (Fries, 2005) improving socioeconomic health determinants (Head et al., 2018) and better public policy (Islam et al., 2018). Adding health to years will be the most challenging public policy concern in low and middle-income countries (LMICs) as the determinants of health is unfavourable compared to those of high-income countries (World Health Organization, 2015).
Given these transition taking place in LMICs, our scoping review aims to answer the following three objectives.
How do researches conceptualised healthy ageing? How do studies assess or quantified healthy ageing? To summarise the evidence of healthy ageing
Methodology
The methodology for our study was guided by that of Arksey and O’Malley (2005) framework. Accordingly, we included the following steps: (a) identifying the research question; (b) identifying relevant studies; (c) selection of studies; (d) charting the data; and (e) collating, summarising and reporting the results.
Search Strategy
The study used PubMed and Scopus electronic databases to identify relevant studies since these two databases are comparatively better in generating more relevant studies (Falagas et al., 2008). We also accommodated search strategies that minimise errors (Salvador-Oliván et al., 2019). The search results were restricted to English language and published between 2010 and 2019. Three sets of keywords were identified to capture studies from the databases. First, a set of keywords identified that related to healthy ageing based on its conceptualisation in past studies (Fries, 2012). Second and third sets of keywords were used for capturing the elderly population and longitudinal studies, respectively. Finally, all the three groups were linked using Boolean operators (Table 1) and applied in the databases using search for the title and abstract option. We also adjusted for the UK and the US spelling variations and text word synonyms. The search result then screened manually.
Key Words.

Inclusion and Exclusion Criteria
From the search results we considered studies with longitudinal approach since it can help to remove sample selection bias and observe causality, which is considered as the best approach for conducting healthy aging studies (Fries, 1996). Our selected studies for the scoping review includes only studies which reported some form of healthy ageing aspects as a key outcome variable, with a quantitative approach and conducted in LMICs (World Bank classification, June 2019). We excluded studies related to nonhuman species, major chronic diseases, reports, commentary, review studies, conference proceedings, surgery, drug or instrument testing, model verification, Intensive Care Unit (ICU) or emergency clinic, disease projection and protocol explanation, studies with mixed methodology approach and not based on the elderly population. We also excluded studies with mortality as the only outcome variable since the mere expansion of life expectancy is not an indication of healthy ageing (Sadana et al., 2016; Salomon et al., 2012)
Data Extraction and Analysis
We imported all the relevant studies to Mendeley citation software and completed data charting using the Microsoft Word program. We have created three tables; a table with the list of selected studies for the final review which contained information about each article (Supplementary Material, Table 2), and second table for the summary of selected studies, which contained; author(s)’ name(s), year of publication, country/region of the study, study duration, sample size, age, type of study design, measure of healthy ageing (outcome), determinants of healthy ageing (covariates or exposure variable(s)) and key finding of the study (Supplementary Material, Table 3) and a third table to summarise domains of healthy ageing, mode of healthy ageing measurement approach and measurement tools used for assessing health status (Supplementary Material, Table 4).
Our analysis aims to answer each of the objectives discussed above. First, to understand the conceptualisation of healthy ageing we considered the World Health Organisation’s (WHO) framework, which has a more holistic sense that based on life-course and functional perspectives. Accordingly, healthy ageing is defined as the process of developing and maintaining the functional ability that enables well-being in older age. Functional ability refers to the health-related attributes that enable people to be and to do what they have reason to value, which is made up of intrinsic capacity (all the physical and mental capacities) and environments (all the factors in the extrinsic world related to an individual). The framework also considered well-being as a broadest sense of healthy ageing (World Health Organization, 2015). For easy summarisation purpose, we categorised healthy ageing concept into domains such as physical capabilities, cognitive functions, metabolic and physiological health, psychological well-being, social well-being, general health status, security, health behaviours and short-form survey and health indices as indicated earlier (Lu et al., 2019). Second, we aim to look at how does healthy ageing is quantified based on the question that whether functional ability has assessed in subjective or objective measure(s) or both approach and the nature of measurement tools. It is well established that subjective or objective measure(s) of health can be used to assess health changes over time (Cleary, 1997; Fernandez-Ballesteros, 2011). Finally, we aim to highlight research evidence on healthy ageing.
Results
Through the initial search result, 17,425 records were identified. Few articles were accessed by contacting authors. After removing duplicates (391 documents), we ended up with 17,034 documents, which then screened manually based on title and abstract. We further excluded 16,270 documents based on the exclusion criteria, which resulted in 764 documents to be considered for the full-text review. At this stage, we excluded 514 documents with valid reason(s) and thus 250 articles included for the final analysis (Figure 1)

Descriptive and Methodological Characteristics
The review identified studies from 24 countries, of which majority of the studies were conducted in China (106), Brazil (67), and Mexico (25). Few studies were found in Nigeria (9), Iran (8), Malaysia (6), South Africa (5), India (4), Turkey (4), Costa Rica (4) and each study from Cuba, the Democratic Republic of the Congo, Argentina, Tunisia, Chile, Malawi, Indonesia, Romania, Russia, Kenya and Thailand (Figure 2). We also identified one study which is based on multiple country contexts (Cuba, Dominican Republic, Venezuela, Mexico, Peru, India and China) using population-based cohort survey (Jotheeswaran et al., 2015). In terms of the number of study samples, each study varied from each other with relatively less sample size found in Randomised Controlled Trials (RCTs) and other experimental types of studies (See Supplementary Material, Table 3). The study which used the largest sample was 76869, which is a cohort study conducted during 2006–2010 in China (Vaidya et al., 2016). The study which is based on the smallest number of sample was conducted in Brazil, which used 11 months of non-randomised prospective intervention approach in 9 observations (de Oliveira Chachamovitz et al., 2016). Based on the study duration, the longest follow-up study was conducted during 1992–2015 in China (Li et al., 2018), whereas the shortest study period was seven days which was conducted in Brazil (Spina et al., 2019). The oldest study in our review was conducted during 1983–1994 (10 years of cohort study) in China (Liu et al., 2011). Our descriptive data charting shows that the majority of the studies considered the end of middle age or beginning of old age as the baseline criteria for the age of the samples. There are also few studies which considered younger age group as well.
Conceptualisation of Healthy Ageing
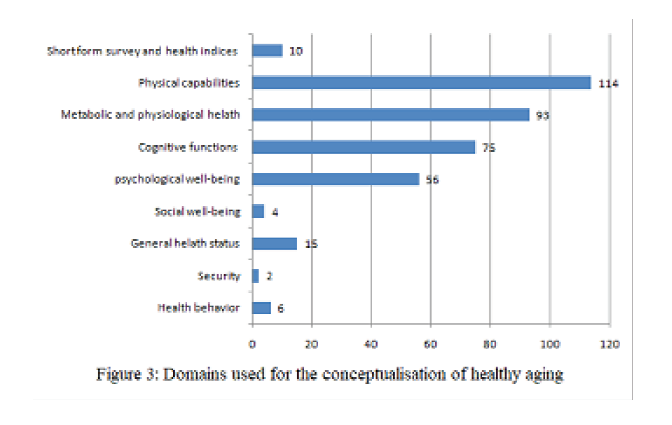
Studies have followed different approaches to conceptualise healthy ageing. The summary of the domains of healthy ageing measurement is provided in Figure 2. A total of 114 studies have considered some form of physical capabilities as a measure of healthy ageing. Most studies used basic/instrumental activities of daily living and disability as the method to assess physical capabilities. We also observed studies which considered other methods to assess physical capabilities including falls, frailty, muscle mass, muscle and grip strength, dependency and autonomy, body balance, mobility, gait strength and speed, sensory impairment and other functional impairments. Metabolic and physiological health domain has considered by 93 studies. Majority of the studies under this domain looked at age-related diseases as the outcome of interest. More specifically such studies considered lifestyle-related diseases (glucose metabolism, systematic blood pressure, Body Mass Index (BMI) and oral health, 3-deoxyglucosone), cardiovascular diseases (stroke, heart disease, angina, myocardial infarction, atherosclerosis), cerebrovascular disease, anaemia, self-reported health status, add power, chronic diseases, multi-morbidity, eye and ear-related diseases and kidney function or glomerular filtration rate (GFR); 75 studies comprised cognitive functions. Cognitive performance was assessed using various standard tools. Broadly, the specific outcome of interest consists of memory testing, assessment of cognitive status and diagnosis of dementia and Alzheimer’s disease; 56 studies included psychological well-being as an indicator of healthy ageing. Methods used to quantify psychological well-being includes assessment of depression, quality of life, life satisfaction, self-perceived uselessness, loneliness, and psychological well-being. Three other domains; social well-being, general health status and security were applied in 4, 15 and 2 studies respectively. All these three domains were quantified based on subjective questions. Health behaviour was assessed in 6 studies based on the quantification of medication intake, smoking and food and dietary habits; 10 studies applied short-form survey and health indices to conceptualise healthy ageing outcome.
The Measure of Healthy Ageing
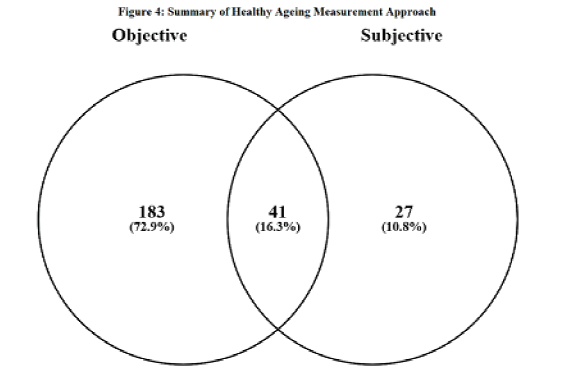
Subjective or objective or mix of both measure of health has been widely used in the literature. The summary of the measure of healthy ageing in our review is depicted in Figure 3. We found that 183 studies measured healthy ageing using objective approach, whereas 27 studies followed subjective approach; 41 studies followed mix of subjective and objective approach. Overall our descriptive analysis shows that objective approaches followed in those studies which primarily used healthy ageing domains such as physical capabilities, cognitive functions, metabolic and physiological health and health behaviours. The subjective approach was widely used in those studies which used domains such as psychological well-being, social well-being, general health status and security.

A word cloud is represented in Figure 4, which shows the most frequently used standard instruments for the assessment of healthy ageing. Two of the most used instruments were Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL), which are traditionally used method for assessing health under the physical capabilities domain. Mini-Mental State Examination (MMSE) is another objective measurement method which has used in most studies and assessed healthy ageing through the domain of cognitive functions. Under the psychological well-being domain, several studies used subjective instruments such as Centre for Epidemiological Studies-Depression scale, Geriatric Depressive Screening (GDS) scale and World Health Organisation Quality of Life (WHO QOL). We observe that other most frequently used health assessment instruments were in objective in nature such as Body Mass Index (BMI), Clinical Dementia Rating (CDR), Timed Up and Go (TUG), Trail Making Test, The Rey Auditory Verbal Learning Test (RAVLT), 10-word Delayed Recall Test, Walk Test and Berg Balance Test. It is to be noted that there are also studies that used multiple instruments to create an overall health index (Carneiro et al., 2019; Chhetri et al., 2017; Doǧan et al., 2012; Fhon et al., 2018; Marchiori & Tavares, 2017; Pérez-Zepeda et al., 2016; Shi et al., 2011; Tang et al., 2013). Our descriptive data shows that these studies have conceptualised healthy ageing with broader sense considering multiple domains with both subjective and objective measurement instruments and thus consists of the most aspects of the healthy ageing definition given by WHO.
Evidence of Healthy Ageing in LMICs
Evidence for healthy ageing is mixed in our review. There is clear evidence for the possibility of healthy ageing through the practice of productive engagement related to cognitive and physical capabilities (see Supplementary Material, Table 3). Majority of these studies applied RCTs or experimental approach and used some form(s) of productive engagement intervention. Studies also proved that lifestyle-related behavioural factors might determine healthy ageing. Some of those behavioural aspects include smoking (Chen et al., 2012; Do Nascimento et al., 2015; Francisco et al., 2010; Hussin et al., 2019; Khalili et al., 2014; Leite et al., 2013; Liu et al., 2012; Liu et al., 2011; Ni et al., 2017; Tian et al., 2011; Wang et al., 2013), poly-pharmacy (de Fátima Rosas Marchiori et al., 2015; Wang et al., 2015), nutrition and dietary habits (Fang et al., 2016; Hussin et al., 2019; Lau et al., 2019; Qiu et al., 2012; Sadeghi et al., 2015) personal hygiene practices (Dos Santos et al., 2013; Saengtipbovorn & Taneepanichskul, 2014) and alcohol intake (Liu et al., 2011). Many studies confirmed the role of socioeconomic factors in the determination of healthy ageing (Supplementary Material, Table 3). Interestingly there are studies which exclusively emphasised the role of childhood or early life background of individuals in the determination of healthy life in the old age (Carrillo-Vega et al., 2019; Castro-Costa et al., 2011; Gao et al., 2017; Goes et al., 2017; Grimard et al., 2010; Gu et al., 2011; Jiang et al., 2019; Mejia-Arango & Gutierrez, 2011; Sadeghi et al., 2015; Saenz & Wong, 2016; Sha et al., 2018; Shen & Zeng, 2014; Torres et al., 2018b). These studies accentuate why considering causality effects is relevant in healthy ageing studies as health in old age is an accumulation of multiple factors influenced over time. Extrinsic factors such as pollution (Wen & Gu, 2012) emotional support (Torres et al., 2018a; Zhang et al., 2018) social support (Brito et al., 2019) community environment (Wang et al., 2018) social isolation and loneliness (Gureje et al., 2011a; Gureje et al., 2011b; Li & Zhang, 2015; Zhong et al., 2017; Zhou et al., 2018) seasonal variations (Elizondo-Montemayor et al., 2017) and other environmental factors (Danielewicz et al., 2018; Lima-Costa et al., 2016) are also found to be the key determinants of healthy ageing. Most of the other evidence identified in our review were connected to age related physiological changes, diseases and fixed characteristics such as gender, urban/rural residency, different age cohorts, and so on. (see Supplementary Material Table 3).
Our review also identified few studies that contradict the possibility of healthy ageing. A study found that even though higher socioeconomic status was associated with the better cognitive performance, it did not help to act as a protective factor against the rate of decline in cognitive functioning (Yang et al., 2016). Another study found that though social engagement helps to improve self-rated health and mental distress, it did not show any impact on chronic health diseases (Liu et al., 2019). Two other studies which experimented with intervention and expected to improve physical strength did not show a positive result (Damasceno et al., 2019; Rica et al., 2013). In short, these contradicting findings show that it is equally important to consider multiple dimensions of healthy ageing outcome without losing the significance of the key determinants.
Discussion
To our knowledge, this is the first systematic scoping review on healthy ageing with a specific focus on LMICs. We summarised study characteristics, methods and key results and thereby examining the extent, range and nature of healthy ageing related researches. Our review highlights evidence of healthy ageing from 24 countries which used different types of longitudinal approach. The descriptive analysis shows that the extent of healthy ageing studies is limited to fewer geographical areas as indicated elsewhere (Preston & Stokes, 2012; World Health Organization, 2015). The number of studies in countries such as India, Russia, Indonesia and Iran was found to be less, and it is a great concern as they will be sharing a significant share of the global elderly population (United Nations, 2017). We noted that there are many studies which used RCTs and other experimental intervention that provided best pieces of evidence, but those were limited to small sample size which may not help for macro-level public policy intervention, especially in large countries. Studies based on larger sample size with relatively longer follow up may provide better public health policy related evidence (Fries, 2012). Most of such studies in our review were conducted in China and has been conducting decades back. It is worthwhile to note that, recently there are efforts on large scale population-based data documentation on elderly related issues at the global level, which may help to conduct further studies by the scientific community in LMICs context (Börsch-Supan et al., 2013). Most of the developed countries consider individuals above 65 years as elderly, whereas it is 60 years in most LMICs. Our review observed that there is no such hard and fast rule for the sample selection on the basis of age. Generally it is highly recommended to consider young age cohorts along with elderly cohorts so that methodologically it can help to provide robust results (Caballero et al., 2017; Moffitt et al., 2017), which was followed by some of the studies in our review.
In comparison to the definition given by the WHO, majority of the studies in our review conceptualised healthy ageing with a narrow viewpoint. We identified only limited number of studies that considered broader aspects of health though many studies conceptualised healthy ageing by combining two or three domains. More specifically, the quantification of extrinsic elements of healthy ageing was limited, especially to those factors related to security and social well-being domains. One of the least studied elements of intrinsic factors includes neurobiological and genetic aspects. This could be because of the difficulty in assessing them over a long period of time. Overall, majority of the studies conceptualised healthy ageing under physical capabilities, metabolic and physiological health, cognitive functions and psychological well-being domains. Conceptualisation of healthy ageing can also be influenced by contextual factors, especially with variations in socioeconomic, environmental and other extrinsic factors which may result in inter-country differences in health status among the elderly. Previous studies have indicated such inter country differences or sub-national level of ageing within countries (Bloom et al., 2011; Rajan et al., 2003).
The method for the measurement of healthy ageing was dominated by the objective approach. We observe that the combined objective and subjective measurement approach could provide better meaning to the health status in the old age as it increases the probability to consider both intrinsic and extrinsic factors. In sum, most of the intrinsic factors were conceptualised under physical functioning, cognitive functions and metabolic and physiological health with objective approach whereas most of the extrinsic factors were conceptualised under security and social well-being with more of subjective approach. Studies that constructed health indices can be considered as a best practice since those studies combined multiple dimensions of health domains with both subjective and objective approach. One of the limiting factors for the measure of healthy ageing with broader meaning is the lack of data documentation in LMICs; still self-rated health status (SRH) could help to provide a better picture as a health assessment tool for measuring health status (Subramanian et al., 2009; Zhao et al., 2014). However, our review identified limited studies that used SRH as a health measurement tool.
Our review identified many evidences of healthy ageing in LMICs despite they have the consequences of epidemiological and demographic transition. The main observation from the review is that the health and non-health related vulnerability could determine healthy ageing, which is consistent with earlier findings such as the role of income status, social support, health problems (Grundy, 2006) lack of care, childlessness, homelessness, inequalities and disempowerment or no access to social protection (Schröder-Butterfill & Marianti, 2006) in determining health and well-being. Thus public policy should focus on these aspects to ensure better ageing.
Our study has strengths and limitations. We used a search strategy that was recommended based on previous review studies, which helped us to optimise search results. We also followed the standard procedure for conducting systematic scoping review as mentioned above. Our study is not free from limitations. Though we have considered the two databases with justification still there is chance for missing out those studies which can be available only through other specific databases. We also did not do grey literature search. Our review considered only studies published in English, thus some of the works, especially from LMICs or regional languages might be missed out. Finally, generally scoping reviews are considered as a precursor for conducting systematic review. Thus it may not take in to account the issues such as the quality of evidence of each study; rather it provides only a narrative or descriptive account of the existing literature (Arksey & O’Malley, 2005; Levac et al., 2010; Peters et al., 2015).
Conclusion
In conclusion, the present scoping review attempted to map literature on healthy ageing studies in LMICs. There is still lack of sufficient studies from most of the LMICs on healthy ageing though many of them are projected to account for a significant share of the elderly population. We observed that most numbers of studies conceptualised healthy ageing based on factors that are related to physical and cognitive change, metabolic and physiological aspects and psychological well-being. Traditionally used health assessment tools were widely used by most of the studies. Our result indicated that there are many study evidence that can be relevant to consider for health policy to achieve healthy ageing for all. Overall, there are extrinsic and intrinsic factors of healthy ageing that can be determined by the interaction of micro (individual) to macro (public policy) level decisive factors. Our descriptive analysis indicates that there is a need for further studies that focus on intrinsic factors such as neurobiological ageing.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for Healthy Ageing in Low and Middle-Income Countries; A Systematic Scoping Review by C. V. Irshad, Umakant Dash, V. R. Muraleedharan, in Journal of Health Management
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or for the publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.