
Abstract
Introduction:
Antibiotic use needs to be monitored. Its irrational use causes resistance. Research aims to determine trends in antibiotic use.
Methods:
Observational research with retrospective data collection. Cross-sectional research design. Data about the availability of antibiotics from 2014 to 2017 in hospitals, health offices and PHCs in the city of Manado.
Results:
Trends of antibiotics used in PHC and health office in 2014–2017 were betalactam, macrolide, sulfamethoxazole-trimethoprim, and quinolone groups. Trends in secondary hospital were betalactam, sulfamethoxazole-trimethoprim, and quinolone groups. Trends in tertiary hospital are betalactam, quinolones, and other groups.
Conclusion:
Based on the data of five major antibiotics use in Manado City, there was a change in the pattern of antibiotic use, and this pattern tended to increase.
Introduction
The overuse/misuse of antibiotics has been recognised as a key factor in the emergence of antimicrobial-resistant organisms (Ventola, 2015). Inappropriate antibiotic use also leads to increased medical expenses: unnecessary or duplicative antibiotic use in US hospitals costs an estimated $163 million (Schultz et al., 2014). Hence, many experts have suggested establishing antimicrobial stewardship programs in hospitals as well as in communities (Spellberg et al., 2008).
Antimicrobial resistance is considered a critical public health concern Aaerestrup et al. (2012). The situation in less developed countries is even more challenging. Data on antimicrobial use in India between 2005 and 2009 revealed an increase in consumption of all studied antimicrobial agents (Ganguly et al., 2011). The Antibiotic Resistance Surveillance and Control in the Mediterranean Region (ARMed) study collected data on antimicrobial use from hospitals in seven countries. It found a wide use of broad-spectrum antimicrobial agents and a high prevalence of resistance in common pathogens (Borg et al., 2008).
Current Social Security Agency of Health (BPJS) participants increased. It impacts the number of patients with BPJS in the hospital. Hospital needs strategies, especially strategy about antibiotics using. It is hoped that it will reduce problems while also improving efficiency for BPJS (Mendrofa & Suryawati, 2016). Based on 2011 Permenkes No. 2406 on General Guidelines for the Use of Antibiotics, there were various studies that showed that around 40%–62% of antibiotics were used incorrectly, such as for diseases that actually do not require antibiotics. Studies about the quality of antibiotic use in hospitals found that 30%–80% were not based on indications.
Data show the high use of antibiotics such as penicillin, cephalosporins, and ciprofloxacin in one hospital in Indonesia (Pradipta et al., 2013c). It strongly indicated high resistance to them. Another study was conducted on sepsis patients at two hospitals in Indonesia and showed a high resistance to antibiotics (Pradipta, 2013a; Pradipta et al., 2013b). It becomes more complicated because culture and sensitivity testing of antibiotics show negative results in the majority of patients indicated infection (Pradipta et al., 2012).
The use of antibiotics needs to be monitored. If it use irrationally, it will cause resistance. This has become a global and serious problem. Therefore, it is necessary to conduct research. It aims to determine trends in antibiotic use in the JKN era.
Methods
This research was an observational study with retrospective data. The study design was cross-sectional. The data obtained are secondary data in the form of antibiotic availability during the period 2014–2017. It includes the type, strength, and dosage form of antibiotics. It was processed using descriptive statistics. The data sources are collected from pharmaceutical installations, hospital information systems (SIRS/INSTI), and pharmaceutical warehouses. The sample was chosen purposefully, but it had inclusion and exclusion criteria. Therefore, the place or location of this research was the North Sulawesi Provincial Health Office, Manado City Health Office, Manado Tertiary Hospital, Manado Secondary Hospital, Inpatient Primary Health Center (PHC), and Outpatient PHC.
Results
Table 1 shows percentage of antibiotics used 90% in North Sulawesi Provincial Health Office, Manado City Health Office, inpatient PHC, and outpatient PHC in 2014–2017.
Antibiotics Percentage with Utility 90% in PHC.

In the North Sulawesi Provincial Health Office, the percentage of DU90% items tended to increase from 2014 to 2017. In the Manado City Health Office, the percentage of DU90% items tended to decrease from 2014 to 2016 and fall further in 2017. The percentage pattern of DU90% items in outpatient PHC matched the pattern of the Manado City Health Office. The DU90% inpatient PHC percentage pattern followed the saw pattern.
Based on Table 2, in 2014–2017, the percentage pattern of DU90% items in secondary hospitals tended to decrease. While the pattern of item percentage DU90% in tertiary hospitals tended to rise. There are more DU90% items in tertiary hospitals than in secondary hospitals.
Antibiotics Percentage with Utility 90% in Secondary and Tertiary Hospitals.

Based on the Figure 1, in the Provincial Health Office, antibiotics distributed were more than 46.85%–61.97% from the betalactam group. These antibiotics were Amoxycillin caplet 500 mg and Cefadroksil capsule 500 mg. There were other 3–4 groups included in 90% drug utility, for example, quinolone group, macrolid group, sulfametoxazole–trimethoprim group, and cholamramphenicol group.
Item Antibiotics with Utility 90% in Health Office and Primary Health Care.
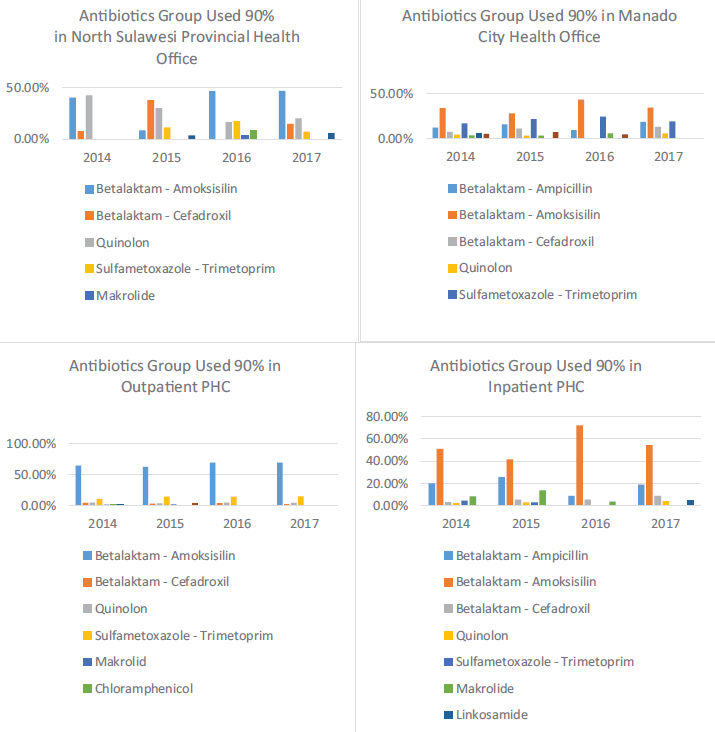
In the Manado City Health Office, the antibiotics distributed were 52.77%–66.12% from the betalactam group. These antibiotics were Amoxycillin 500 mg caplet, Ampicillin 500 mg caplet, and Cefadroksil 500 mg capsule. There were other 2–5 groups included in 90% drug utility, for example, quinolone group, macrolid group, sulfametoxazole–trimethoprim group, cholamramphenicol group, and tetracycline group. There was a tendency for the use of antibiotics in addition to the betalactam class, which has decreased from 2014 to 2017.
In the outpatient health centre, the antibiotics distributed were 65.72–73.59% from the betalactam group. These antibiotics were Amoxycillin 500 mg caplet and Cefadroxil 500 mg capsule. There were other 2–5 groups included in 90% drug utility, for example, quinolone group, macrolid group, sulfametoxazole–trimethoprim group, cholamramphenicol group, linkosamid group, and other groups. There was a tendency for the use of antibiotics except betalactam class had decreased from 2014 to 2017.
In inpatient primary health centre, betalactams are used 72.99% -86.35%. they are Amoxycillin 500 mg caplet, Ampicillin 500 mg caplet and Cefadroxil 500 mg capsule. There are 4 groups that are included in the drug utility 90%, i.e.: quinolones, macrolides, sulfamethoxazole–trimethoprim, lincosamide group. There is a tendency that the use of antibiotics betalactams are increased from 2014–2017.
In the inpatient health centre, the antibiotics used were 72.99–86.35% from the betalactam group. These antibiotics were Amoxycillin 500 mg caplet, Ampicillin 500 mg caplet, and Cefadroxil 500 mg capsule. There were other 1–4 groups included in the 90% drug utility, for example, the quinolone group, the macrolide group, the sulfametoxazole–trimethoprim group, and the linkosamid group. There was a tendency for the use of antibiotics in addition to the betalactam class, which has decreased from 2014 to 2017.
Based on the Figure 2, in level 2 hospitals, the antibiotics used were 67.93–71.29% from the betalactam group. These antibiotics were Amoxycillin 500 mg caplet, Ampicillin caplet 500 mg, Cefadroxil capsule 500 mg, Cefixime 100 mg capsule, Ceftriaxone 1 g injection, Cefixime 200 mg capsule, and Cefotaxime 1 g injection. There were other 3–4 groups included in the 90% drug utility, for example, the quinolone group, the macrolide group, the tetracycline group, the aminoglycoside group, and other groups. There was a tendency for the use of antibiotics in addition to the betalactam class, which has decreased from 2014 to 2017.
Item Antibiotics with Utility 90% in Secondary and Tertiary Hospitals.
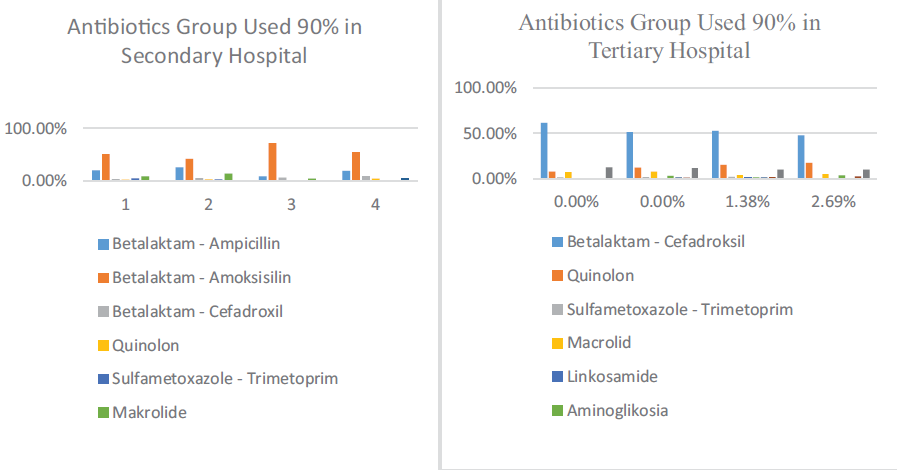
In level 3 hospitals, the antibiotics used were 50.51–61.45% from the betalactam group. These antibiotics were Cefadroxil 500 mg capsule, Cefixime 100 mg capsule, Ceftriaxone 1 g injection, Amoxycillin 500 mg tablet, Cefixime 200 mg capsule, Cefaleksin 500 mg capsule, and Cefotaxime 1 g injection. There were other 4–7 groups included in 90% drug utility, for example, quinolone group, macrolid group, tetracycline group, aminoglycoside group, sulfametoxazole–trimethoprim group, carbapenem group, chloramphenicol group, and other groups. There was a tendency for the use of carbepenem groups to increase in percentage from 2014 to 2017.
Discussion
The 90% drug utilisation (DU90%) method is a method that shows the grouping of drugs that fall into the 90% segment of use. Evaluation of drugs that fall into the 90% segment is needed to emphasise the drug segment in terms of evaluation, control of use, and planning for procurement of drugs (Goossens et al., 2005; Sketris et al., 2004; de With et al., 2009).
Based on Table 1, the most antibiotic use in health office was amoxicillin. Other inline research results were conducted by Pani et al. (2015). It stated that quantitative data analysis using ATC/DDD showed that Amoxicillin (500 mg) was widely used with 2,723 DDD/1,000 patients per day (Pani et al., 2015). Another result of studies of antibiotics used in 2013 amounted to 86.16%, in 2014 amounted to 88.61%, and in 2015 amounted to 82.73%. Amoxycillin is the most used that amounted to 92.76%, Cefadroxil 4.19%, Ciprofloxacin 1.34%, and Cotrimoxazole 1.71% (Putra et al., 2017). In 2015, cefadroxyl was the most used antibiotic in the Provincial Health Office. This might be due to the empty amoxicillin stock at the pharmacy distributor.
The majority of the used antibiotics in inpatient PHC and outpatient PHC from 2014 to 2017 were from the betalactam−penicillin group with oral dosage forms. This was in line with research conducted by Chang et al. (2019), who stated that the main antibiotic group used was penicillins (51.5%) followed by cephalosporins and macrolides (14% each). However, 29% of the antibiotic dosage form used is injection (Chang et al., 2019). Other research states that the overuse of injection antibiotics in PHC has also been observed in other countries such as Vietnam, India, and Korea (Bhartiy, 2008; Choi et al., 2012; Mao et al., 2015). This practice is rarely needed in primary care as most infections can be controlled with oral antibiotics (Dancer, 2004). Injection of drugs is complicated by serious adverse drug reactions and complications such as local infections, bleeding, and nerve injuries (Milder et al., 2012; Ramachandra et al., 2012).
Based on Table 2, Manado Secondary Hospital (Health Facility 2) from 2014 to 2016 used Cefadroxyl 500 mg capsules most. In 2017, it was Cefixime 100 mg capsules. Other studies conducted in India also showed that penicillins and cephalosporins are a class of antibiotics that are widely used and belonged to the DU90% segment (Sholih et al., 2015). Another different research results state that antibiotics used in 2010 was the most widely used penicillin group, 40.2%, which was dominated by amoxicillin, 38.9% (Katarnida et al., 2014). In this study, amoxicillin is an antibiotic that is widely used. This is because this research was conducted in 2010 so that there was a shift in the use of antibiotics from penicillin to cephalosporins.
The most antibiotic used at Manado Tertiary Hospital in 2014 was Cefadroxyl 500 mg capsules and in 2015–2017 was Ceftriaxone 1 g injection. Other inline research results were conducted by Katarnida et al. (2014). It stated that the most widely used antibiotics are cefotaxime 308 (37.3%), ceftriaxone 189 (22.9%), and chloramphenicol 131 (15.9%) (Akter et al., 2012). Other similar research results were conducted in Malaysia. It stated that co-amoxiclav, erythromycin, cefuroxime, ceftriaxone, and ampicillin with sulbactam were the most commonly used antimicrobial agents (Al-Yamani et al., 2016). Another different research result in Tertier Hospital; the most commonly prescribed agent was piperacillin/tazobactam followed by amoxicillin/clavulanic acid and clarithromycin. The most common mode of administration was the intravenous route (Bitterman et al., 2016).
Based on Tables 1 and 2, it is known that there are differences in the patterns of antibiotic use between PHC, secondary hospital, and tertiary hospital. The use of antibiotics in secondary hospital tends to be higher than PHC. The use of antibiotics in tertiary hospital tends to be higher than secondary hospital. These differences due to large differences in antibiotic usage patterns exist, for example, medium-sized, private, and university hospitals use more antibiotics (Katarnida et al., 2014), and additionally, antibiotic usage patterns differ between small and large community hospitals in Korea (Yoon, et al., 2015). Possible reasons for these differences are variations in bacterial epidemiology at the hospital level, the medical staff’s attitude toward prescribing antibiotics, and the antimicrobial stewardship program effectiveness. Hence, if possible, it would be ideal for each hospital to conduct a study of its own (as was done in this paper) to find its own representative antibiotics (Kim et al., 2018).
Conclusion
This study concludes that the most widely used antibiotics from 2014 to 2019 in inpatient PHC and outpatient PHC were Amoxicillin 500 mg tablets. In secondary hospital, the widely used antibiotics from 2014–2016 were Cefadroxil 500 mg capsules. In 2017, there was a change in the pattern of antibiotics used, and the most widely used was Cefixime 100 mg capsules. In tertiary hospital, the most widely used antibiotic in 2014 was Cefadroxyl 500 mg capsules. In 2015–2017, the widely used was Ceftriaxone injection. Based on the data of 5 major antibiotics used in health facilities, there was a change in the pattern of antibiotics used, and this pattern tends to increase.
Footnotes
Acknowledgements
The author would like to thank those who have contributed to this research, Head of Research and Development Center for Humanities and Health Management, Secretary of National Institute for Health Research and Development, and other parties who cannot be mentioned one by one who greatly assisted the process of collecting research data.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.