
Abstract
Human serum albumin (HSA) is a commonly used product with high impact on healthcare expenditure. Little is known regarding the appropriateness of HSA use in healthcare system. This study aimed to assess prescriber’s compliance to the approved HSA criteria. Potential cost saving was also estimated. A cross-sectional study was performed in a tertiary care, university hospital in Bangkok in 2019. Prescriptions for HSA for all adult patients along with corresponding medical records were reviewed and assessed against the approved HSA criteria. Deviation from the criteria was used to estimate the potential cost saving. A total of 688 prescriptions were reviewed, 200 prescriptions met the inclusion criteria and were included in the analysis. Among six indications in the approved criteria for HSA, the rates of criteria compliance ranged from 48 to 90%. Hypoalbuminemia was found to be the main reason for inappropriate use. The estimated cost saving from inappropriate HSA use was €3,543 (€59 per prescription). Significant deviation from the approved criteria of HSA use was seen in a Thai hospital and significant cost saving can be made by increasing the compliance to the criteria. A practice improvement initiative to promote rational use of HSA is warranted.
Introduction
Human serum albumin (HSA) is a colloidal solution used in conditions associated with a volume deficit in various indications (Rozga et al., 2013). HSA is one of the top 10 most commonly used products in the healthcare system around the world (Dastan et al., 2018; Somers et al., 2002; Torbic et al., 2020; Zolfagharian et al., 2017). With a high volume of consumption along with its high cost, HSA puts a significant burden on healthcare costs, particularly in developing countries where resources are limited (Aramwit & Kasettratat, 2004). One of the strategies to control the financial impact of HSA is to implement drug use evaluation (DUE) programme to encourage the appropriate use of HSA (Dastan et al., 2018; Farsad et al., 2016; Foroughinia & Mazraie, 2017; Jahangard-Rafsanjani et al., 2011; Shafiee et al., 2016; Somers et al., 2002; Talasaz et al., 2012; Tanzi et al., 2003; Zolfagharian et al., 2017). Through the DUE programme, prescribers are guided by the approved criteria which are aimed to optimise HSA use by selecting patients who will derive benefits and minimising the unnecessary use of HSA. This strategy is important for cost containment in a resource-limited health system (Aramwit & Kasettratat, 2004; Farsad et al., 2016; Foroughinia & Mazraie, 2017; Jahangard-Rafsanjani et al., 2011; Shafiee et al., 2016; Talasaz et al., 2012; Tanzi et al., 2003; Vincent et al., 2014).
Criteria-based evaluation is of utmost importance to create the appropriateness of drug use when making a decision in DUE process (Fanikos et al., 2014). The paucity of solid evidence of HSA in many diseases led to an ambiguous pattern of HSA usage in practice. Several studies investigating HSA utilisation reported varying degrees of appropriateness in HSA usage (Aramwit & Kasettratat, 2004; Foroughinia & Mazraie, 2017; Farsad et al., 2016; Farasatinasab et al., 2018; Jahangard-Rafsanjani et al., 2011; Nejad et al., 2010; Shafiee et al., 2016; Talasaz et al., 2012; Tanzi et al., 2003; Torbic et al., 2020). This may partly derive from the different criteria used to define ‘appropriateness’ in each study. Each geographical area may have different disease patterns, costing system along with healthcare financing schemes. As a result, despite the availability of HSA data from other countries, it may not be feasible to apply data derived from one country to another.
Universal healthcare coverage has been implemented in Thailand since 2002 (Tangcharoensathien et al., 2018). While the initiative has greatly improved access to healthcare services, the financial demand has risen and creates a significant burden on the national healthcare financing system (Tangcharoensathien et al., 2018). Throughout the years, studies have indicated that curbing the overconsumption or inappropriate use of medication may potentially lessen the financial strain on the national healthcare system (Berman et al., 2019). Based on this concept, the policy of promoting rational drug use (RDU) was initiated nationwide and DUE is one mechanism of RDU implementation (Rattanachotphanit & Waleekhachonloet, 2020). Despite a high impact of HSA on healthcare budget and some level of DUE implementation on HSA usage, there was no qualitative assessment on HSA usage in a Thai health system to date. Such information is greatly needed to provide policy makers with the current status of HSA usage in the Thai healthcare environment.
This study aimed to assess the level of prescriber’s compliance to the approved criteria of HSA based on the existing data of the DUE programme in a tertiary care, university-affiliated hospital in Bangkok, Thailand. We also explored the reasons for deviations from the approved HSA criteria along with estimating the potential cost saving if compliance to such criteria can be improved.
Materials and Methods
Ethics Statement
The study protocol was approved by the Institutional Review Boards of Ramathibodi Hospital, Mahidol University, Bangkok, Thailand (reference number: MURA2019/915).
Study Design
A cross-sectional descriptive study was performed at the Ramathibodi Hospital. The hospital is 1,500 beds leading tertiary care, university-affiliated hospital with comprehensive and advanced medical services. There are approximately 200,000 hospital admissions and 1.5 million outpatient visits annually. The hospital also has one of the most advanced clinical pharmacy services in the nation ranging from ambulatory care, acute care, and intensive care settings. There are various specialised pharmacy services ranging from infectious diseases, cardiology, solid and liquid organ transplantation and oncology to name a few. A prospective DUE process of HSA has been implemented since 2016 with the pharmacy department playing the central role in the development, execution and monitoring of the process in collaboration with other health professions. Through the Pharmacy and Therapeutics Committee (PTC), usage criteria of HSA were approved, implemented and revised throughout the years. Starting in 2019, a new set of HSA usage criteria was approved and implemented. The pharmacy department had been collecting data where prescribers were required to provide key information in the structured DUE form. The completed forms were then reviewed by pharmacists prior to dispensing. Once approved, HSA can be used for 3 days and requires additional review if more HSAs were needed. At the time of the study, there were two HSA preparations available at the study site including a 250 mL of 5% HSA injection containing 12.5 g of HSA per vial and a 50 mL of 20% HSA injection containing 10 g of HSA per vial.
DUE Criteria for HSA
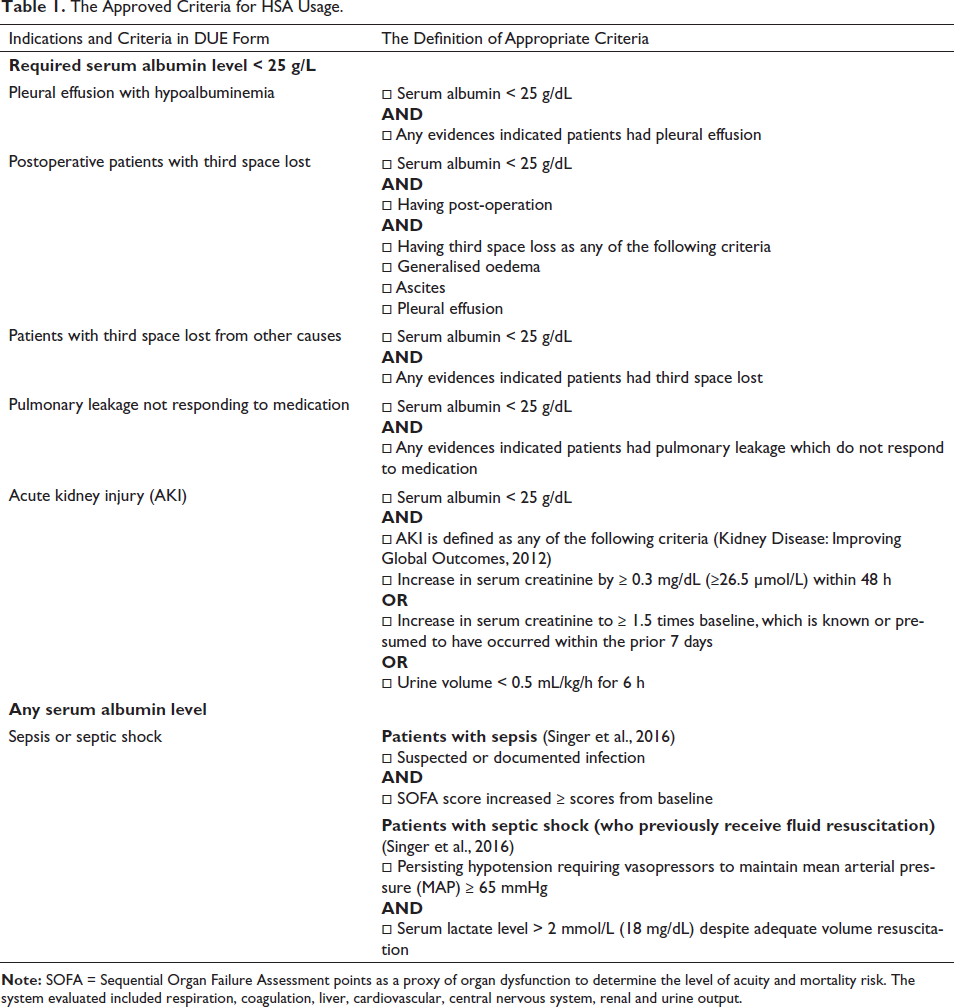
The PTC developed the DUE criteria for approved HSA usage based on the latest clinical evidence and guidelines. There were 32 indications that were approved by the PTC. However, due to the large amount of HSA usage, we included only the most common indications (over 75% of HSA usage) into our investigation. These indications were (a) pleural effusion with hypoalbuminemia, (b) postoperative patients with third space lost, (c) patients with third space lost from other causes, (d) pulmonary leakage not responding to medication, (e) acute kidney injury and (f) patients with sepsis or septic shock.
Study Population
The inclusion criteria were (a) adult patients aged 18 and older (b) admitted to the hospital during September to October 2019 and (c) received 5% or 20% HSA during the hospital stay. Patients whose data were incomplete for data analysis and those receiving HSA for conditions other than six indications of interest were excluded from the study.
Sample Size Calculation
The sample size calculation was based on the following calculation: N = [Z2 α /2 × P(1 − P)]/M2. Where Z = Z-statistic for a level of confidence of 95%, P = The percentage of inappropriate use of HSA of 87.3 (Foroughinia & Mazraie, 2017) and M = Margin of error of ± 0.05. We used a number of prescriptions as a unit of analysis. Therefore, the number of sample size was at least 171 prescriptions.
Data Collection and Data Analysis
Prescriptions of HSA during the study period were screened against the inclusion and exclusion criteria. Patient identification numbers listed on the prescription that met the inclusion criteria were then pooled and searched from the hospital database. The corresponding completed DUE forms of the patients were also pooled. Patient’s baseline characteristics such as age, gender, body weight and comorbidities were then extracted into the structured case record form. Information related to HSA usage including indication, serum albumin level, the prescribed HSA product, amount of use, duration of use, adverse drug reactions and patient outcomes were collected. Continuous data were presented as mean ± SD or median and range. Dichotomous data were presented as proportion or percentages.
Evaluation of HSA Usage Appropriateness
To assess the prescriber’s compliance to the approved usage of HSA, the investigators performed a thorough review of each prescription against the approved criteria set by the PTC. Detail information of the criteria is listed in Table 1. Baseline and clinical information of each patient at each time of HSA use was obtained from medical records and laboratories database and reviewed against the criteria. Any usage that did not meet the criteria was considered as inappropriate use. Reasons for non-compliance were also investigated and tabulated.
The Approved Criteria for HSA Usage.
Cost Analysis
We estimated the potential cost saving based on the deviation from the approved criteria. The cost was calculated using the number of vials of HSA multiply by the cost of unit dose (vial) for each prescription. All costs were reported using British Pound, € (1 Thai Baht = 0.023 British Pound, €). The costs of 5% and 20% HSA product in 2019 were €39 per vial and €24 per vial, respectively.
Results
During the study period, there were a total of 688 prescriptions for HSA. Two-hundred and eighty-two prescriptions were excluded since they were for indications other than the six indications of interest. After screening for all inclusion and exclusion criteria, 206 prescriptions were excluded and 200 prescriptions were included in the final data analysis.
Patient Characteristics
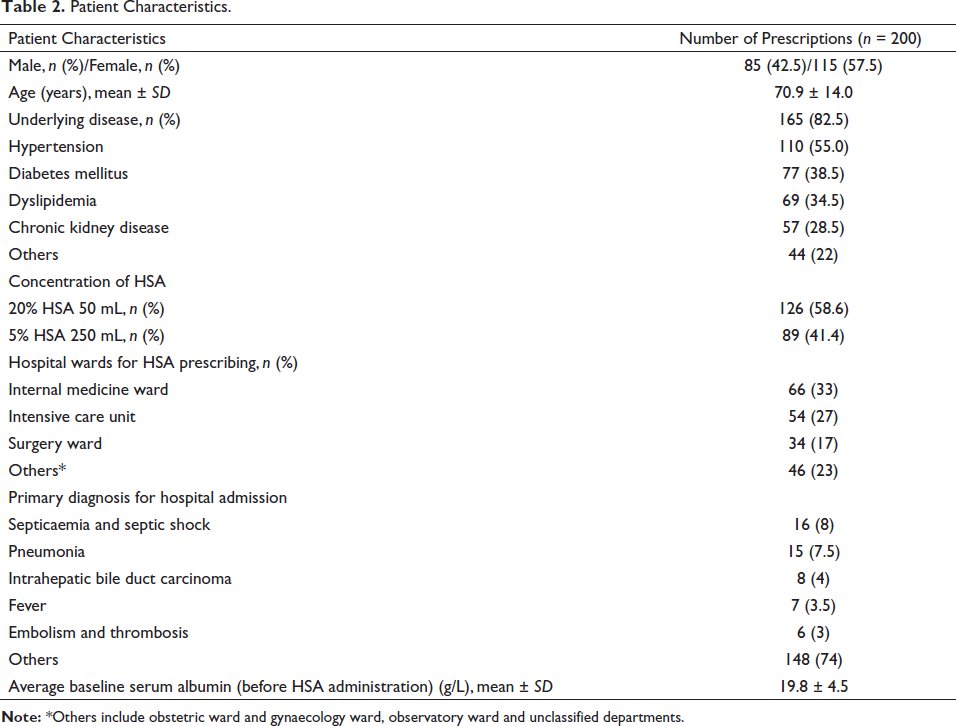
The mean age of patients was 70.9 ± 14.0 years with 57.5% as female. For HSA product, 58.6% and 41.4% of prescriptions were for 20% and 5% HSA, respectively. HSAs were mostly used in the medical wards (33%), intensive care unit (27%) and surgical wards (17%), respectively. The most common reasons for hospital admission were septicaemia and septic shock, followed by pneumonia and intrahepatic bile duct carcinoma, respectively. The mean baseline serum albumin before receiving HSA was 19.8 ± 4.5 g/dL. Baseline patient characteristics are presented in Table 2.
Patient Characteristics.
Indications of HSA and the Evaluation of the Appropriateness of HSA Usage
A total of 200 prescriptions containing 215 indications for HSA were reviewed. Among the six indications investigated, the most common indications were sepsis or septic shock (25.5%), followed by postoperative patients with third space lost (22.3%) and third space lost from the other causes (17.2%), respectively. After reviewing these HSA prescriptions against the approved criteria, 72.1% of prescriptions were classified as ‘appropriate use’. However, 27.9% of the prescriptions were classified as ‘inappropriate’. The appropriate and inappropriate use of HSA for each indication is presented in Figure 1. Overall, HSA usage in sepsis or septic shock had the highest rate of inappropriateness compared to other indications.
The Proportion of Appropriate and Inappropriate Use of HSA According to the Approved Criteria Set by the PTC.

For most indications, inappropriate prescriptions resulted from usage of HSA despite having higher serum albumin level than specified in the criteria. For sepsis or septic shock, a large proportion of inappropriate prescriptions resulted from usage of HSA despite having mean arterial pressure (MAP) above the recommended value (70%) and not meeting the SOFA score as indicated (17%) and lacking evidences of sepsis or septic shock (13%). For AKI, a large proportion of inappropriate prescriptions resulted from not meeting AKI criteria (80%).
There was no report of major adverse drug reaction from HSA use including cardiac failure, pulmonary oedema and hypotension during the study period.
Cost Analysis
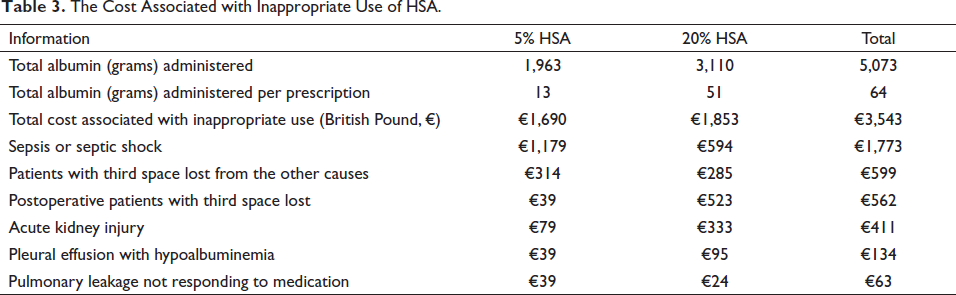
The total cost for inappropriate HSA use was €3,543 (€59 per prescription), which was approximately 26% of the total cost for HSA during the study period (1.5 months) (Table 3). As a result, the estimated annual cost saving if there was a full compliance to the HSA usage criteria for all indications was €28,347 per year. Among these indications, the potential for cost saving through the improvement of DUE compliance was the highest for the indication of sepsis or septic shock.
The Cost Associated with Inappropriate Use of HSA.
Discussion
Due to a lack of definite criteria for use, HSA can potentially be used in several off-label conditions (Caraceni, Domenicali et al., 2013; Caraceni, Tufoni et al., 2013). From a healthcare provider’s perspectives, HSA is a well-known expensive medication requiring a strategy to ensure appropriate usage to avoid unnecessary loss of healthcare resources (Buckley et al., 2021). As a result, the study evaluating the appropriateness of use through the DUE programme may help shed some light on the current situation of HSA use along with providing important information that can be used to design appropriate interventions to improve HSA use in a healthcare institution.
Compared to previous studies from other countries, the most common indications for HSA in our study were different. This may be a result of differences in the patient population, disease epidemiology, types of hospitals investigated in various studies. Interestingly, the rate of the appropriate use of HSA in our study was higher compared to previous studies (9–65%) (Aramwit & Kasettratat, 2004; Farsad et al., 2016; Farasatinasab et al., 2018; Foroughinia & Mazraie, 2017; Jahangard-Rafsanjani et al., 2011; Nejad et al., 2010; Shafiee et al., 2016; Talasaz et al., 2012; Tanzi et al., 2003; Torbic et al., 2020). This may partly be a result of differences in usage criteria from our study that differed from criteria of other studies. Criteria used in other studies were derived from clinical practice guideline (Dastan et al., 2018; Foroughinia & Mazraie, 2017; Farsad et al., 2016; Farasatinasab et al., 2018; Jahangard-Rafsanjani et al., 2011; Nejad et al., 2010; Shafiee et al., 2016; Torbic et al., 2020), primary literature (Dastan et al., 2018; Jahangard-Rafsanjani et al., 2011; Nejad et al., 2010; Torbic et al., 2020), AHFS drug information (Aramwit & Kasettratat, 2004; Talasaz et al., 2012) or institutional guideline (Buckley et al., 2021; Tanzi et al., 2003) at the time when those studies were conducted. For our study, due to the limited resources, we placed emphasis on indications where HSA’s roles were well substantiated with clinical evidence and where justification of use can objectively and easily be measured.
To illustrate the strength of our DUE criteria, HSA use in sepsis was based on the new sepsis definition using various objective parameters such as MAP and SOFA score (Dellinger et al., 2013). HSA has a role in the initial fluid resuscitation of severe sepsis and septic shock when patients already received substantial amounts of crystalloid (Dellinger et al., 2013). As for HSA used for AKI, the definition of AKI was based on the latest KDIGO guideline using serum creatinine and urine output as objective parameters (Kidney Disease: Improving Global Outcomes, 2012). For other indications investigated, serum albumin level was the only objective parameter for evaluation. Other criteria of appropriateness use of HSA were based on criteria associated each specific disease. Based on this approach, the DUE criteria employed in our study reflects the most contemporary evidence-based criteria compared to previous studies, in the setting of a developing country in Asia.
A total of 30% of prescriptions were found to be inappropriate. Among these cases, approximately half of the inappropriate cases were prescribed in sepsis. To improve the compliance to DUE, this can be improved by listing of objective criteria more clearly in the DUE form. In addition, clinical pharmacists’ intervention during ward rounds should be reinforced to help physicians adhering to the HSA criteria of the hospital while dispensing pharmacists should pay particular attention to this indication and perform verification of such order when identified. For other indications, we found that a large proportion of prescriptions were ordered when serum albumin was higher than the level set forth by the criteria. Therefore, one logical intervention to improve compliance was to require physicians to measure and take serum albumin into consideration before prescribing.
From a healthcare provider’s perspectives, significant opportunity for cost saving exists by mitigating HSA inappropriate use and providing cheaper alternatives for HSA. For example, previous studies have indicated that HSA was safe and equally as effective as a 0.9% saline solution for sepsis and septic shock. The Surviving Sepsis Campaign recommended crystalloids as the initial fluid of choice in the resuscitation (Dellinger et al., 2013). In general, 12.5–25 g of HSA was a recommended initial dose. If 2,000 mL of 0.9% saline solution was used instead of HSA, 96% of the cost can be saved when calculating the HSA prescriptions for sepsis or septic shock improperly used in our study (from €1,773 to €63). By using a cheaper alternative, the hospital can realise significant cost saving which will positively impact the hospital budget management. If this can be applied on a wider scale across the nation, it may help lessen the strain on healthcare resources which is extremely beneficial in a developing country like Thailand and most other Southeast Asian nations.
There are several limitations in this study. First, due to the retrospective nature of the study, some information may not be fully documented in the medical records. Second, the study setting was a single-centre and the type of setting was a tertiary care, university-affiliated hospital. As a result, generalisability may be limited to similar settings where have capability to provide HSA treatment. Third, the study duration was relatively short. Based on these limitations, multi-centre studies with a much longer duration may be needed to reduce certain factors such as diverse patient populations and seasonal effect over the entire year. Fourth, the appropriateness of HSA was based on the criteria developed by the study site. As a result, its application can be limited to a setting where patient populations are similar. Despite these limitations, findings from this study at least help shed some light on the scale of the problem of HSA use along with a potential and significant cost saving by promoting compliance to DUE criteria.
Conclusion
Significant deviation from the approved criteria of HSA is common, particularly in the sepsis and septic shock indication, in a Thai university hospital. Hypoalbuminemia was found to be the main reason for inappropriate use. Significant cost saving can be made by increasing the compliance to the criteria. Attempts should be made to improve the rational use of HSA. The cost saving for a proper use may have a huge impact on healthcare financial system of the country.
Footnotes
Acknowledgements
The authors wish to thank all pharmacy and nursing staff who facilitated the data collection and the Pharmacy and Therapeutic Committee of the Ramathibodi Hospital for the support of this project. Special thanks go to Suvatna Chulavatnatol, PhD, and Surakit Nathisuwan, PharmD, BCPS, for their guidance on the project and writing of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study protocol was approved by the Institutional Review Boards of Ramathibodi Hospital, Mahidol University, Bangkok, Thailand (reference number: MURA2019/915).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.