
Abstract
Groups within the healthcare organisations are widespread subjects of research nowadays. Nevertheless, informal groups are rarely examined in healthcare. This study is a descriptive cross-sectional study aimed to determine the formation of informal groups and its dimensions in Turkey. A survey design was adopted and sample size was 208. The questionnaire was validated using exploratory factor analysis and Cronbach’s alpha coefficient. The study unveiled that the ownership of hospitals are prominent determinants of informal groups. Demographic, social and environmentally proximity are the main factors for public employees to take part in an informal group while intellectual life and closeness are the main factors for private sector employees. The study suggests that managers should assume the most part of responsibility to determine employee’s abilities, preferences and social features to cooperate with informal groups.
Background
One of the most important stages of the human evolutionary process is the development of organised social life. For example, nomadic communities were able to hunt and maintain their lives through teamwork. The industrial revolution, however, led to the simplification of jobs for workers, which reached its peak with Taylorism. Thus, the natural evolution process of the human being has been intervened. On the other hand, Mayo’s research in Western Electric has contributed to the recognition of the importance of formal and informal groups in organisations (Pais & Parente, 2015).
After the industrial revolution, producing methods began to change. Classical approaches to management were the outstanding outcomes of these changes. The theory of Friedrick Taylor suggested scientific organisational functioning and alleged that there is a one best way to do every job (Miller, 2012). In his book that is called ‘The Principles of Scientific Management’, he expresses ‘time and motion’ studies to determine the best way to do jobs. His theory is mostly based on scientifically analysing of jobs, properly selected employees and formal communicating processes (Taylor, 1911). In this classical, the content of communication is explicitly determined. Only formal communication processes is expected and desired in organisations. The main problem of this approach is that the informal and spontaneous aspects in any organisations are unconsidered (Machado & Davim, 2018). The Hawthorne studies carried out between 1927 and 1932 revealed that only formal organisational structure cannot lead to improvement in production but therewithal informal communications and groups must be considered. Elton Mayo found that spontaneous cooperation was supporting the organisation and preventing the breakdown of the society and organisation (Pugh & Hickson, 2007).
Relationships are important in order to fulfil the task successfully in a business. Formal relationships are often defined by job descriptions and organisational charts. Each organisation has also informal groups and these are people who know each other and help each other regardless of rank, function or job title. Significant relationships are also established among people in different institutions. The complex network of relationships within and outside the organisation constitutes the circulation system that carries information and ideas to the employees of the organisation when they need it. The managers of any institution should design the business environment in a way that ensure the development of inter-personal relations. Because it is not possible for managers to force employees to establish positive and close relations with others. Establishing richer, deeper and wider relationships can provide social capital to the individuals working in the organisation and to the organisation. Social capital is defined as a network of relations that provides information, helps problem solving, broadens customer bases, adds value and increases strategic capacity, and it is an undeniable fact that social capital contributes to organisational effectiveness (Lengnick-Hall & Lengnick-Hall, 2003).
Social capital also creates a large recruitment pool as it allows employees to encourage their friends and other professionals to consider working in the organisation. Social capital facilitates the inter-unit resource exchange because employees are more likely to share with people they know and care about (Adler & Kwon, 2002).
Another benefit of groups and communication is that they offer a range of solutions to problems as they involve different perspectives. Researchers have found that effective group discussions allow high-quality decisions (Wanous & Youtz, 1986).
In an organisation, there are groups that can be formed both formally and informally. Formal groups are defined by the organisational structure in order to achieve organisational goals. Informal groups, in contrast, are more natural and formed by social relations and personal preferences (Robbins & Judge, 2013). Each individual can be a member of various formal and informal groups. The communication between members and the structure of groups can differ significantly from formal groups (Certo & Certo, 2016). These factors shape the types and channels of communication which is one of the most important part of a business. On the other hand, communication can be divided into two dimensions as well (Coiera, 2006). Communication is a prominent issue for healthcare. Ineffective communication causes many undesired outcomes in a healthcare institution. Many misdiagnosis, mistreatments, malpractices, patient injuries and deaths can be attributed to the lack of communication or miscommunication. Clinical communication problems are major contributing factors to hospital sentinel events up to 70% (ASQHC, 2012). An effective communication between healthcare teams and their members has been a prominent factor for improving patient safety and outcomes (Milligan et al., 1999).
Informal groups can contribute to success of a business or can be a reason for ineffectiveness. Nevertheless, informal groups can ease the communication within members and organisation. It can also increase the organisational commitment. To manage the informal groups in organisations, the types and formation process of groups need to be identified correctly. With the information on members’ expectations and goals in the formation of an informal organisation, managers can get the ability of motivate staff to develop more value.
In a study examining the factors affecting health insurance acquisition, it was revealed that the information on health insurance products, registration methods or subsidies did not increase the level of acquiring insurance. On the other hand, it has been determined that the introduction of the same information to informal groups increases the acquisition of health insurance by up to 12% and also increases the confidence in and information about the product. In the same study, it was stated that social connections (social networks) play a leading role in the adoption of health insurance. In this sense, it will not be wrong to say that informal groups can play a facilitating role in many areas (Chemin, 2018). In the same study, the statement of an individual who had no previous experience in health insurance was also pointed out. Accordingly, the individual who has no previous health insurance experience has a positive opinion on health insurance because of the positive insurance processes experienced by another friend of the same informal group (Chemin, 2018). To the best of our knowledge, there is a gap in the literature regarding to the formation motives of informal groups in healthcare, despite of many studies searching the effects of informal relations and groups
In this case, healthcare managers should be very careful. In fact, it is possible for individuals in informal groups to influence one another and to be influenced by one another in terms of business processes. For this reason, creating a positive management image in business processes will create a positive perception on the other members of the informal groups. For this reason, inclusion of the formation of informal groups may play an important role in understanding organisational behavior. Therefore, the purpose of this study is to investigate the formation process of informal groups and communication in healthcare and shed light onto proper approaches to manage human resources.
Methods
The main research question of the study is whether there is a significant difference according to demographic features of healthcare staff in terms of the determinants of the informal groups’ formation process. The hypotheses of the study are as given below:
There is/is not a statistically significant difference among profession in terms of the determinants of the informal groups’ formation process. There is/is not a statistically significant difference according to gender in terms of the determinants of the informal groups’ formation process. There is/is not a statistically significant relationship between age and determinants of the informal groups’ formation process. There is/is not a statistically significant difference among year of experience in terms of the determinants of the informal group’s formation process.
The study is a descriptive quantitative study using a questionnaire to collect data from a range of healthcare professionals who work in both private and public hospitals. The data were collected in Istanbul, Turkey. One private and one public hospital were included in the study in order to allow comparison of health staff who works in private and public hospitals. Permissions were obtained from the hospitals for the study. All health staff including patient consultants and administrative staff were included in the study. Non-medical health staff such as, cleaners, repairers, securities, drivers and cookers were not included in the sample. Purposive sampling was chosen as sampling method. Informed consents of the participants were received for the study. The survey has been carried out with the staff who accept to participate in the study. Therefore, the total health staff of hospitals was 300 and 69% of them accepted to participate in the study. The questionnaire was applied at first hand in a hospital. Totally 208 questionnaires were obtained properly.
The questionnaire that was developed by Kabay (2017) used to collect the data. Some modifications were made in line with the aim of the study. Literature was reviewed and experts’ opinions were consulted at the modification process. Exploratory factor analysis and internal consistency analysis has been carried out to determine the structure and reliability of the scale. Then, the tests for hypotheses was carried out.
Results
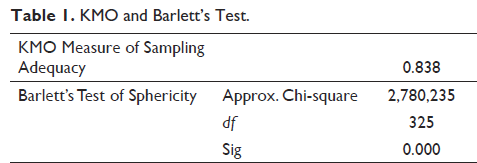
Reliability and validity analyses were conducted to determine the structure and the reliability of the scale. Factor and principle component analyses were carried out in order to reveal the structure and validity of the scale. Cronbach’s alpha coefficients were calculated for each factor and for whole scale in order to ascertain the reliability of the scale. First, Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy was tested and it was found to be 0.838, then, Barlett’s test of sphericity was found to be significant at 0.05. They mean the sample is adequate and suitable to conduct a factor analysis. The table of the analyses are as shown in Table 1.
KMO and Barlett’s Test.
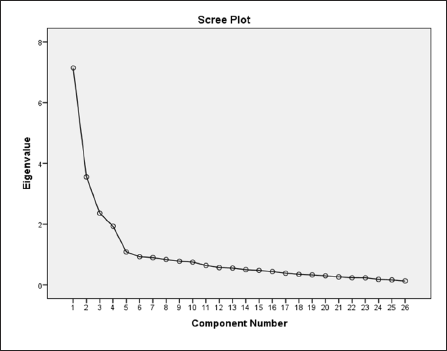
After conducting KMO and Bartlett’s test, factor analysis was conducted. As a result of the test, it was determined that there are two statements should be excluded from the scale and the scale consists of four sub-dimensions. Scree plot graph of the scale is as in Figure 1.
Scree Plot of the Scale.
Varimax was used as rotation method. Rotated component matrix is shown in Table 2. Accordingly, there are four factors and statements collected in each factor and weights of each statement are indicated in the table. Four factors explain 57.62% of the variance.
Structure of the Scale.
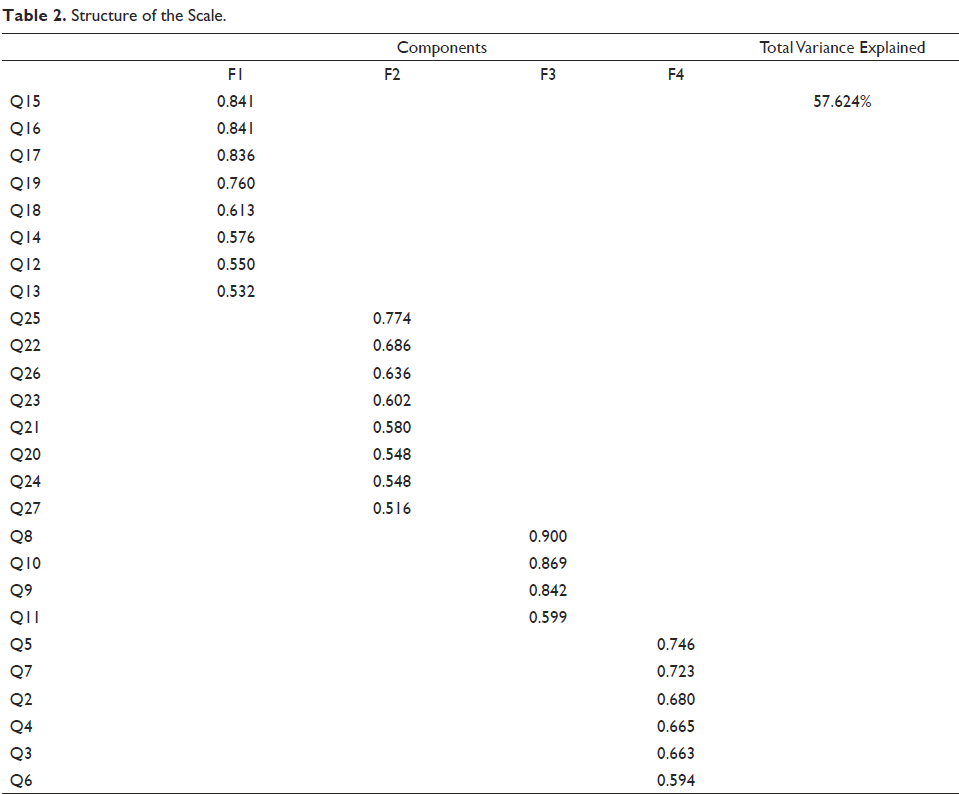
The first and second factors of the scale consist of 8 statements. The third factor consists of four statements. The fourth factor consists of six statements.
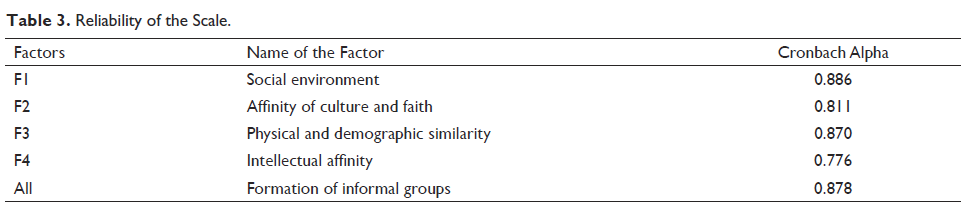
After revealing factor structure of the scale, reliability analysis was conducted. Cronbach’s alpha scores of the sub-dimensions are 0.886, 0.811, 0.870 and 0.776, respectively. Cronbach’s alpha coefficient of the scale as a whole is 0.878, as shown in Table 3. These coefficients mean all scale and each sub-dimension are highly reliable.
Reliability of the Scale.
Descriptive Statistics
After determining the structure and reliability of the scale, first, descriptive statistics were calculated and then hypothesis tests were carried out. Demographic features of the participants are described in Table 4.
Demographic Indicators.
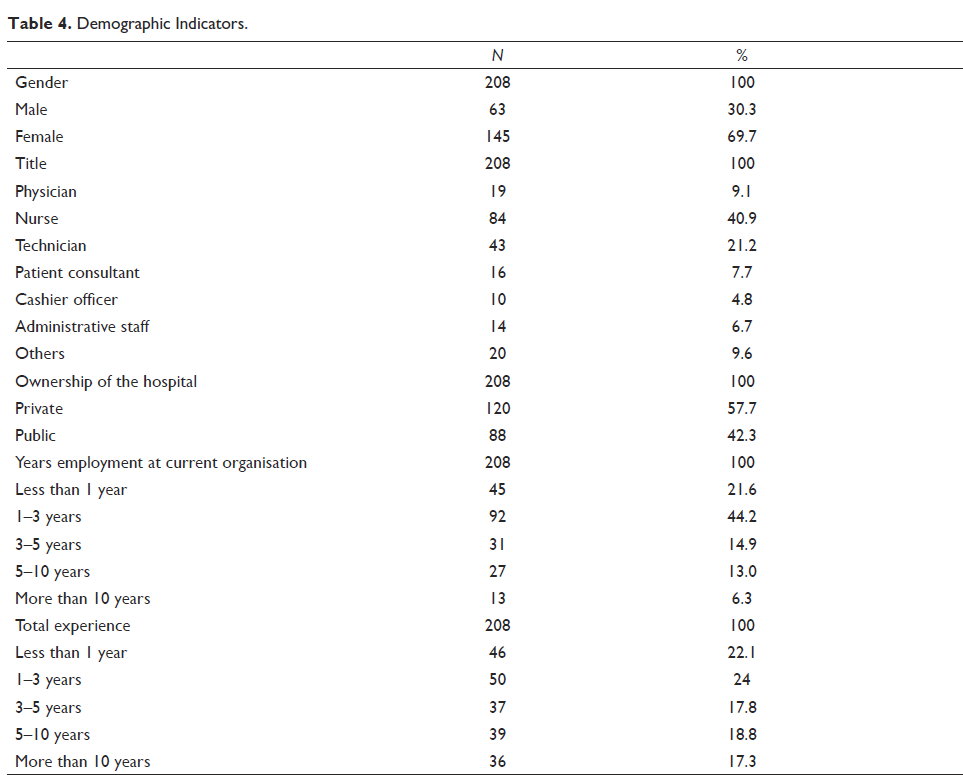
Overall, 69.7% of the participants are woman, 40.9% are nurses, 57.7% are working in a private hospital, 44.2% have 1–3 years of experience in their institution and 22.1% have less than 1 year of total experience.
Mean score of each factor is described in Table 5. The mean scores are 19.6731 ± 5.61, 20.274 ± 4.53, 10.038 ± 3.42 and 15.644 ± 3.48, respectively, and 65.629 ± 11.7 in total.
Mean Scores of the Scale.

Because the dependent variable does not conform to normal distribution, nonparametric hypothesis tests have been used (p < .05).
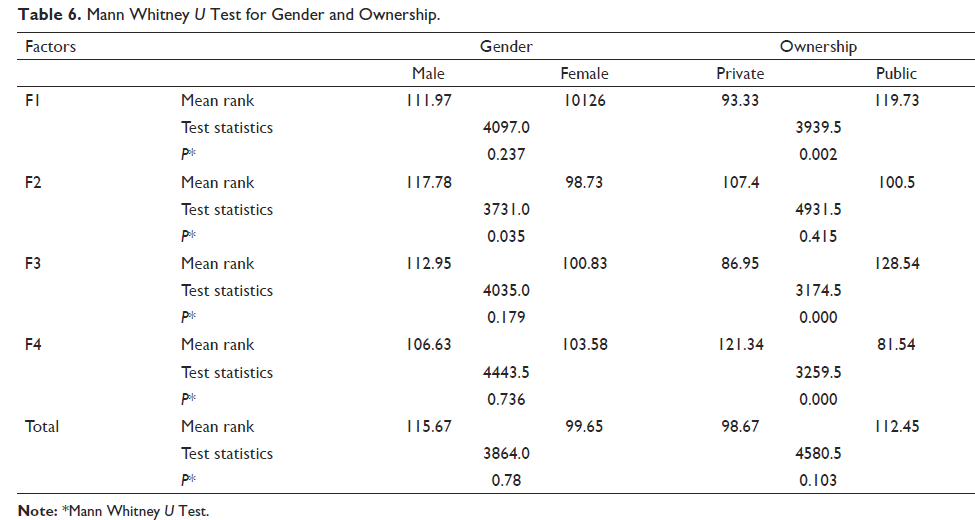
According to the Mann Whitney U, there is a statistically significant difference according to gender in terms of the determinants of the informal groups’ formation process in F2, and, there is a statistically significant difference among ownership in terms of the determinants of the informal groups’ formation process F1, F3 and F4. But there are not statistically significant differences in both variables in total, as shown in Table 6.
Mann Whitney U Test for Gender and Ownership.
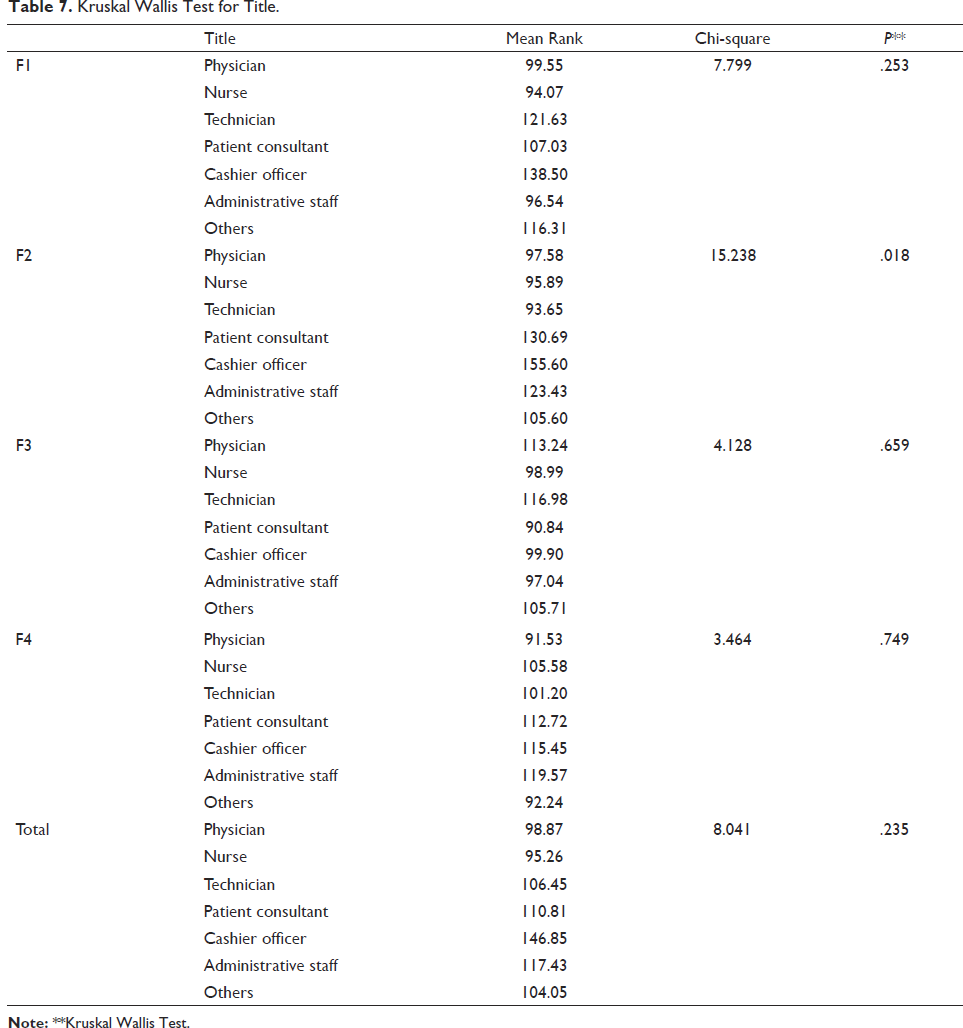
According to the Kruskal Wallis test, there is a statistically significant difference in the formation of informal groups in terms of title only in F2 (p < .05). There are no statistically significant differences in other sub-dimensions and total (p > .05). Cashier officers have the highest mean rank in F2, as shown in Table 7.
Kruskal Wallis Test for Title.
There are no statistically significant differences according to the working year and total experience in formation of informal groups (p > .05), as shown in Table 8.
Kruskal Wallis Test for Experience.

Discussion and Conclusion
Informal groups emerge naturally in organisations in accordance with the common interests and preferences of the individuals. Recently, there has been growing interest in supporting informal groups especially in democratic organisations, with the aim of strengthening the communication and cooperation between individuals. In this kind of organisations, informal groups can take a critical role for organisational learning. There is now much tendency to ease the communication process for the purpose of development of individuals’ abilities and extend the organisational capacity. Many organisations have been supporting the informal groups and communication to prevent or compensate for labour loss. However, the managers can see informal groups as a threat in autocratic organisations. Moreover, it should be noted that informal communication might lead to gossips and controversies.
In recent years, creativity and innovation have become the prominent concepts in the competitive markets. Democratic organisations, free thoughts, taking initiative are the main requirements for creativity and innovation. Many studies have examined the effects of informal groups in formal organisations. These studies have indicated that informal groups and communication can make the work environment more attractive and increase the productivity of employees (Mallett & Wapshott, 2014), it has positive and significant effect on organisational commitment (Gökkaya et al., 2018), and also there is a significant relation between friendship of the employees, organisational commitment and job satisfaction (Lopes, 2004). In a study on medium-sized firms, it was emphasised that informal relations are important in contrast to the widespread belief that informalities should be eliminated and formal relations should be established (Marlow et al., 2010). In another study, which has examined the informal relations in a public–private partnership project it has been found that informal relations could have a significant impact on the success of the project (Zou et al., 2010). In a study which was conducted on local health authorities in Thailand indicated that the informal relationships between local health personnel and non-health organisation personnel could potentially affect local healthcare operations and the development of the local health system (Maneechay & Pongpirul, 2015). In another study on supply chain management, it is concluded that long-term hierarchical relations are effective in creating informal relations and it is possible for stakeholders to trust each other through informal relations (Lu et al., 2015). Priyasad and Weerasinghe (2017) emphasised that the workplace is not only a place where people come together and work but also a complex social system where social needs are met. In this context, it can be stated that informal groups can contribute to efficiency in organisations via strong relations and cooperation. As people are social beings, formation of informal groups are unavoidable. The most important issue is achieving an accordance between organisational and individuals’ objectives (Bekteş & Erdem, 2015). Informal communication will increase with the development and usage of new technologies in organisational processes (Büchel, 2001). Contrary to what is believed by many people, informal groups and communications are not threat for the formal structure and communication. Actually, the informal and formal structures form the organisations as a whole and informal communication has positive effects of the productivity (Gökkaya et al., 2018). Defining the formation of informal groups and having proper information about the structure may enable managers to increase the effectiveness of them.
Accordingly, the primary focus of this article is on examining the formation of informal groups in healthcare and developing suggestions for managers. According to results of the analyses, it has been seen that there is significant difference between participants according to ownership of hospitals. Demographic, social and environmentally proximity are the main factors for public employees to take part in an informal group while intellectual life and closeness are the main factors for private sector employees. The fact that the private sector is in a more competitive environment causes the employees to prefer to take part in groups that can contribute to their abilities and intellectual levels in their perception. Actually, this result indicates the difference between perception of job security of public and private sector employees. The managers who work in public health institutions should know the employees closely to be able to manage the informal groups. The groups that are emerged from demographic and social affinity can threat the authority of managers and the working environment of minority groups. Managers should prevent informal groups being a pressure on other workers and prevent them from hiding the disruptions and errors.
In addition, it has been found that cultural affinity and faiths are considered more important at the point of joining informal groups within men compared to women. Women can be undefended in many organisations due to other informal groups. Managers should ensure women about their position, communication and cooperation process. On the other hand, it has been found that there is no significant difference according to experience of the participants.
Managers should be aware of that informal groups’ relations have significant effects on job commitment, intention to leave, performance and motivation. They should define their employee’s abilities, preferences and social features to cooperate with informal groups. Social, demographic and intellectual features of human resources are the prominent factors, which form informal groups. It is necessary to examine the employees in term of these components and make their expectations and desires in line with aim of the organisation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.