
Abstract
The Indian labour market is dominated by informal workers. Out-of-pocket healthcare payments are the principal source of healthcare financing for those workers. This article will try to investigate the determinants of health expenditures across heterogeneous groups of informal workers in India based on the 68th round of National Sample Survey data on Employment and Unemployment for 2011–2012. Across different types of informal workers, mean health expenditure has been highest among ‘employees of informal sectors’. The determining factors for the health expenditure are social group, household head and the number of dependencies. It is also found that health expenditure is not always catastrophic among informal workers. The result obtained is that health expenditure has been catastrophic for almost 30% of informal workers across various heterogeneous groups. Using the probit model, the influencing factors responsible for the incidence of catastrophic health expenditure are age and sex of the household head, the number of senior citizens in the family, possession of assets and expenditure on fuel and electricity.
Introduction
The Indian labour market is mainly captured by informal employment 1 , and the incidence of it has enhanced rapidly during the post-reform period (Marjit et al., 2007; Sanyal & Bhattacharyya, 2009; Narayana, 2015). This has also witnessed a rapid proliferation of informal employment in both the informal sectors as well as the formal sectors (Sanyal & Bhattacharyya, 2009). Generally, the informal sector also consists of a large number of self-employed (SE) workers (Mukhopadhyay, 1998). Thus informal employment is heterogeneous in nature (Unni, 2005). In this article, the heterogeneity of informal employment is highlighted by subdividing informal employment into three major types 2 , that is, self-employed workers (SE), employees in the informal sector (EIS) and informal employees in the formal sector (IEFS).
The rapid proliferation of informal employment during the post-reform period is a result of labour market flexibility (Unni et al., 2005), resulting in a sufficient reduction in wages to sustain escalated international competitiveness. The deteriorated quality of work during the new policy regime coupled with some major policy shifts in the health sector has caused a disastrous effect on the quality of life of the informal workers. The decline in public investment in health, introduction of the user fees and the new Drug Price Control Order has enhanced the vulnerable condition of the informal workers. The dependency on Out-of-pocket (OOP) 3 health expenditure was thus enhanced during this regime. More specifically, out of total health expenditure, approximately 70% has been OOP private health expenditure (Government of India, 2005) 4 . Being deprived of health benefits, sick leave and working in an unhealthy and deplorable environment for hours, the health of the informal workers is also questionable. In addition to that, income-earning opportunities are also limited among them leading to the impoverishment of a large section of the informal workers (Panneer et al., 2019). Besides, various researchers and economists have opined that not only the incidence of poverty but also wage disparity among them has enhanced during the post-reform period (Papola, 2008; Unni, 2005). Thus it would not be unwise to discuss the extent of health expenditures among the informal workers of India. This article thus aims to discuss private health expenditure among the informal workers of India in the present situation. Furthermore, this article also wants to put some light on the incidence of catastrophic health expenditure among informal workers in India. The issue and nature of health expenditure among the informal workers using NSSO unit-level data have not been addressed in economic literature so far. This article would help to fill up the gap in the literature.
This article is organised as follows: The second section provides a brief discussion of the available literature related to the determinants of OOP health expenditure in India as well as many other developing countries. The research gap and objectives of the study will be spelt out in the third section. The fourth section talks about the source of data used in the study. The fifth section 5 provides estimates of OOP health expenditure among the informal workers in India. Determinants of health expenditure among the informal workers have been discussed in sixth section. The seventh section talks about the extent of catastrophic health expenditure among informal workers. The determinants of catastrophic health expenditure among them are given in the eight section and ninth section 9 summarises the above discussions and concludes.
Brief Review of Literature
Pal (2012) found that the presence of children and elderly members increases the probability of OOP health expenditure in India. Furthermore, OOP health expenditure in India has been higher in the urban area compared to that of the rural area (Sangar et al., 2018). Magazzino and Mele (2012) found that real Gross State Product, the unemployment rate, the number of beds in community hospitals, the urbanisation degree and the percentage of the population with at least a junior high school degree had a direct impact on the real healthcare outlay in Italy. Hooda (2015) found the per capita income and fiscal capacity of a particular state turn positive and have a significant impact on determining the per capita public expenditure on health in India. Mahumud et al. (2017) found that age, sex, marital status, place of residence, and family wealth are significant factors of OOP healthcare expenditures in Bangladesh.
Research Gap and Objective of the Study
The above-mentioned literature only highlighted the OOP, determinants of health expenditures among various countries including India. However, none of the literature has given the focus on the determinants of health among different types of informal workers in India. Worsening financial conditions and hazardous work environments are bound to increase workers’ job insecurity and in turn can create an impact on their mental and physical health (WHO, ILO and Green, 2020). The vulnerability and health hazards among the informal workers are hardly discussed in the economic literature to a great extent. Based on the research gaps, the objectives of the study are listed below:
To investigate the mean health expenditure across different types of informally employed people of India. To find out the determinants of health expenditure among the informal workers in India. To find out whether the health expenditure is catastrophic among the informally employed workers in India or not. To identify the possible factors responsible for the incidence of catastrophic health expenditures among the informal workers of India.
Sources of Data
This study uses the 68th round of NSSO data on Employment and Unemployment for the period 2011–2012 which is the latest available data related to health expenditure among informal workers till date. The extract contains only own account workers (who can also be called Self Employed) (SE), regular salaried workers and casual workers in public and other organisations (indicating IEFS and EIS). To do this we have subtracted all samples whose principal activity status is the employer, student, housewife, beggar, retired and handicapped. Thus the total number of extracted samples is 117,172. Total extracted samples are subdivided into three types of informal workers, SE, EIS and IEFS, and then want to find out the determinants of health expenditure among those chosen types of informal workers. SE workers are their own account workers in our data set. EIS are workers of proprietary enterprises, partnership enterprises, domestic enterprises and other enterprises where the number of workers is less than 10. On the other hand, in our data set, IEFS are workers of public enterprises, private enterprises and cooperative enterprises who hardly get any social security benefits (mainly the benefit of provident fund).
Analysis of Yearly Health Expenditure Among the Informal Workers of India
The mean yearly health expenditure including both formal and informal workers for all types of households is Rs. 6789.65. The following discussion will concentrate on mean health expenditure separately for formal as well as informal workers.
Mean Yearly Total Health Expenditures Among Different Types of Workers
Table 1 has displayed the mean total 5 health expenditures among the formal as well as informal workers where it is found that the mean yearly health expenditure of the formal workers has been considerably higher than that of the informal workers. This is true for both low asset holders 6 as well as high asset holder workers. Our next aim is to look into the OOP health expenditure across heterogeneous groups of informal workers. The rest part of the article, therefore, provides us with information about the health expenditure among informal workers.
Mean Yearly Total Health Expenditure among the Formal and Informal Workers (Rs).

Table 2 gives us information about the OOP yearly mean health expenditures across different types of informal workers. Among them, EIS have the highest mean health expenditures and SE has the lowest mean health expenditures. This is true for both high asset holders as well as for low asset holders.
Yearly Mean Household Level Health Expenditure Across Different Types of the Informal Workers (Rs).

Composition of Total OOP Payments for Healthcare Across Different Types of Informal Workers at the Household Level
Table 3 explains the composition of total OOP payments for healthcare. Total healthcare payments have been sub-divided into two components: (a) institutional expenses and (b) non-institutional expenses. The former refers to hospitalisation expenses while the latter signifies expenses on outpatient services availed by the informal households (NSSO). It is found the lion’s share of the healthcare finances is the non-institutional sources across different types of informal workers. On the other hand, the share of institutional expenses has been below 20% for all the informal workers.
The Composition of Out-of-pocket Payments for Healthcare (in %) Across Informal Workers at the Household Level.

The Share of Out-of-pocket Medical Expenditure Out of Household Consumption Expenditure Among Different Informal Workers at the Household Level
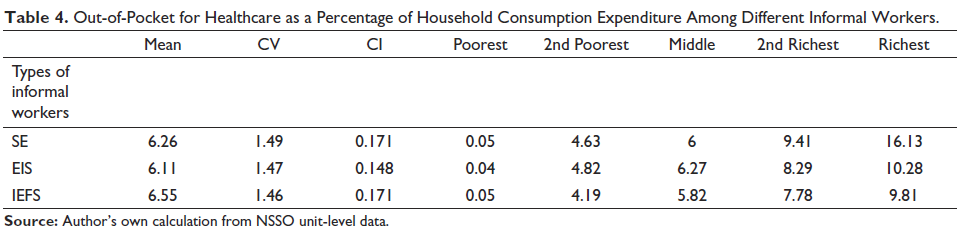
The impact of OOP payments across consumption expenditure quintiles has been analysed among the informal workers and displayed in Table 4. The mean share of household OOP healthcare expenditure in relation to household consumption expenditure is more or less the same across types of informal employment. However, this figure is marginally lowest among the EIS. The coefficient of variation (CV) is very high for all three groups. This is very typical in healthcare expenditure distribution where many people spend little or nothing on healthcare while few households consisting of sick people have large expenditures. The higher the value of CV, the higher the discrepancy in healthcare expenditures among the workers. The concentration index (CI) of OOP payment for healthcare ranks households according to their income on the x-axis and their healthcare expenditure on the y-axis. This indicates to what extent household healthcare payments increases. These indices show whether healthcare payments account for an increasing proportion of income 7 as the latter rises. The CIs are positive indicating that OOP payments on healthcare are disproportionately concentrated among the rich. The quintile 8 specific means of OOP also pay the same result.
Out-of-Pocket for Healthcare as a Percentage of Household Consumption Expenditure Among Different Informal Workers.
Determinants of Yearly Health Expenditure Among the Informal Worker at the Household Level in India
The main objective of this paper is to find out the determining factors of yearly total health expenditures among the informal workers at the household level in India. Here we are considered both household and individual-specific factors. The sample is drawn from the NSSO 68th round where we have the information of both formal and informal workers. But here, we want to identify the factors that play a crucial role in the extent of health expenditures among the informal workers only. Hence there may be some quantitative or qualitative factors responsible for a factor to be informal in nature according to our definition.
So, for this investigation, it is required to take the help of Heckman’s two-step regression model in order to tackle the problem of selectivity bias 9 . To do this, it is required to consider two equations simultaneously; the original equation and the selection equation. In the original equation, the dependent variable is Y i * which is the yearly health expenditure. However, statistical analysis based on non-randomly selected samples consisting of informal workers only can lead to erroneous conclusions and poor policy. Thus we use Heckman corrections which is a two-step statistical approach that provides a means of correcting the non-randomly selected samples and sample selection bias.
This article thus aims to capture the determinants of health expenditure across these different groups of informal workers. Furthermore, wages and educational qualifications among different types of informal workers vary a lot (Abraham, 2019; Dutta, 2005), and health expenditure is bound to vary among them. This article thus aims to capture the determinants of health expenditure across different types of informal workers.
Model 1

Apart from that, our aim is also to capture the determinants of OOP health expenditure in the rural area so that we can put some light on the rural–urban divergence in terms of health expenditure among informal workers. In order to avoid the problem of multi-collinearity, we include rural workers only in a separate model to find out the extent of health expenditure in the rural area compared to that of the urban area.
Model 2

Here ‘age i ’ is considered the age of the ith informal worker. As age increases, health expenditures are supposed to increase because age increases morbidity and illness.
‘hh i ’ represents the household head of the ith informal worker. It is treated as a dummy variable. Gupta and Joe (2013) provided us with the information that health expenditure is considerably higher among male-headed families compared to that of female-headed households. By contrast, in Nigeria female-headed households tend to spend more on health services compared to male-headed households (Ogundari & Abdulai, 2014). This article thus aims to investigate the extent of health expenditures among the workers with female-head where the reference group is male-headed households.
‘assets i ’ represents the total amount of assets possessed by the ith informal workers. According to Gupta and Joe (2013), there has been a positive relationship between the economic status of the people and that of healthcare expenditures. The workers possessing large amounts of assets can be said to be possessing a greater economic status. Thus the workers with large amounts of assets are expected to have larger health expenditures.
‘Caste i ’ represents the social group of the ith informal worker. This article thus seeks to investigate the extent of health expenditure among different social groups. Three dummy variables are separately constructed for the scheduled tribe (ST), the scheduled caste (SC) and other backward classes (OBC). General category worker is considered in the reference group. SC, ST and OBCs are widely considered vulnerable social groups in India (Sengupta et al., 2008) and thus we intend to investigate the extent of health expenditures among them.
‘Youngi’ represents the workers with dependents less than 15 years at the household level. Workers with a higher number of young dependents are expected to spend more on health.
‘Old i ’ represents the workers with dependents greater than 60 at the household level. Workers with senior dependents are also expected to spend larger amounts on health (Gupta & Joe, 2013).
Here ‘Edu i ’ represents years of education among the ith worker. It is assumed that workers with less academic qualifications are less likely to spend on health expenditures (Gupta & Joe, 2013).
‘rural i ’ represents ‘ith’ workers in the rural area. People in rural areas are less intent on seeking healthcare compared to that in urban areas (Gupta & Joe, 2013).
‘Informal workers types i ’ represents of types of informal employment of the ith informal worker. We have constructed dummy variables each for EIS and SE whereas IEFS is the reference. Since the informal worker is not homogeneous, the extent of health expenditure among different groups of informal workers may vary a lot.
Now we present the selection equation that helps to identify the determining factors for the workers to join informal employment. The selection equation is given by

where Ii* represents the type of employment (formal/informal) of the ith worker which is a dummy in nature and is considered as 1 for informal workers, 0 otherwise. Here ‘techi’ represents the technical education of the ith worker. ‘voc i ’ represents the vocational training of the ith worker. ‘rel i ’ represents the religion of the ith worker. All are dummy variables in nature. It is applicable both for Eqs (1) and (2).
Initially, it is required to estimate the selection equation on the basis of the Probit model, On the basis of the estimation, we can have an estimated value of Inverse Mill’s ratio represented by λ of each sample ‘i’. In the Heckman two-step estimation, this λ is to be treated as another explanatory variable of the original equation, mentioned in Model 1 and Model 2. If it is observed that the parameter estimates of λ is statistically significant, then it is obvious that Heckman’s two-step estimation procedure is appropriate to address our research problem. However, the value of λ in the Heckman two-step model has been non-significant even at the 10% level 10 and that proves the non-existent selectivity bias in our model. Now we can take the help of an OLS model to find out the determinants of health expenditure. The models of the OLS are the same as that of the Heckman.
Results and Discussions About Determinants of Health Expenditure Among Informal Workers at the Household Level
The results of the OLS regression have been displayed in Table 5, highlighting the determining factors of yearly health expenditures among the informal workers at the household level in the Indian labour market. The results indicate that the coefficient of EIS, as well as SE, have been significantly higher compared to IEFS which is the reference group. Thus it can be inferred that health expenditures have been significantly highest among EIS followed by SE and the least expenditure has been incurred among IEFS. It is also found that compared to urban workers, rural workers spend significantly lower amounts on health.
Factors Responsible for the Yearly Health Expenditure Among the Informal Workers in India (Using OLS Estimates). Dependent Variable: Yearly Health Expenditure of Each Household.
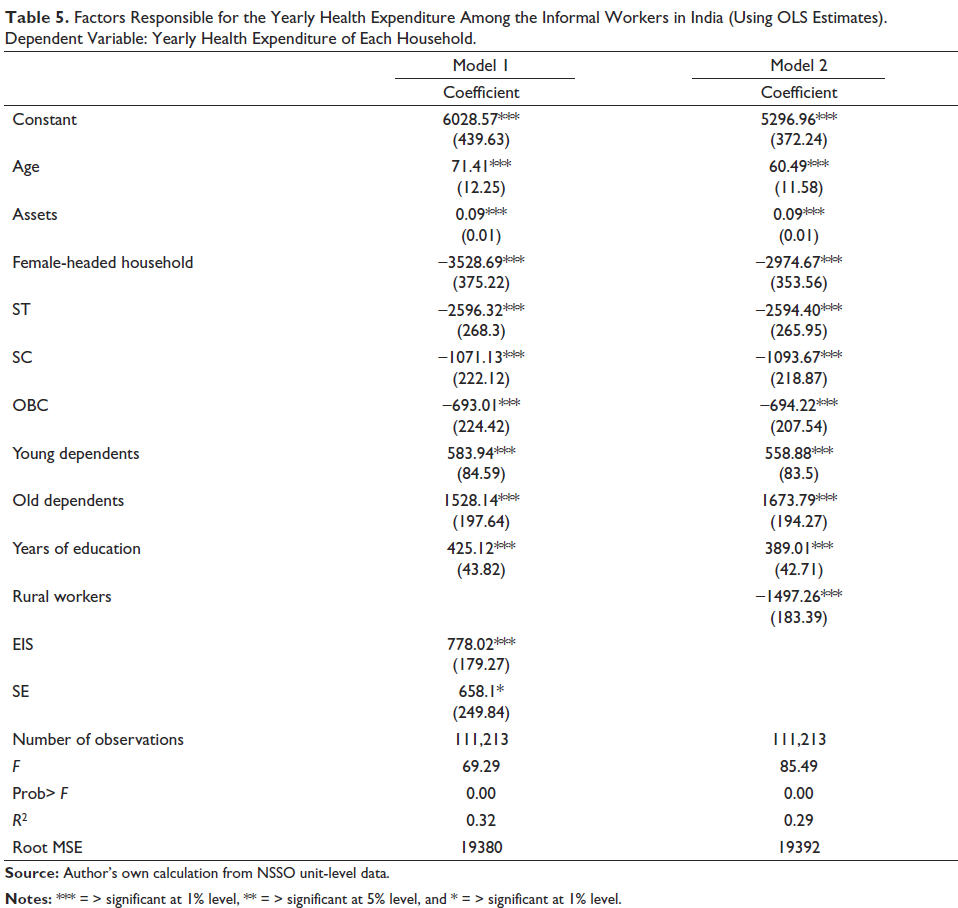
Furthermore, it is found that there has been a positive relationship between the health expenditures of the informal workers and the number of old or children less than 14 years dependent on that household. In fact, the presence of old dependents in the family enhances yearly health expenditure three times more than that of the young dependents. Apart from that, health expenditures are significantly enhanced with the increase in asset holding. Compared to general caste, health expenditure has been significantly lower among the vulnerable social groups like SC, ST as well as OBC workers. The least expenditure on health is observed among the STs. An increase in the years of education increases the expenditures on health significantly. Lastly, compared to that the male-headed household, workers coming from female-headed families tend to spend less on health.
Incidence of Catastrophic Health Expenditure Among the Informal Workers of India
If a household has to reduce its basic expenses over a certain period of time and has to sell assets, or accumulate debts to pay the medical bills of one or more of its members, then the family is said to incur catastrophic payments. Empirical studies confirm that 10% of total expenditure spent on health in a certain reference year is widely accepted as the standard, as this represents an approximate threshold at which the household is forced to cut down on subsistence needs, sell productive assets, incur debts or be impoverished (Ghosh, 2011; van Doorslaer et al., 2006).
Doorslaer (2005) found out that there is a heavy reliance on OOP financing for healthcare in Asia which is one of the major causes of the deterioration of the standard of living. The increased OOP financing for healthcare can only be accommodated through the diversion of resources from other consumption items. The excessive spending on healthcare is explained by the author as negative welfare cost or ‘catastrophic expenditure’ which increases impoverishment among people residing in the low-income countries. Ghosh (2011) found out that new economic policies have significantly enhanced not only the incidence of catastrophic health expenditure but also impoverishment in India. Gupta and Joe (2013) found that the incidence of catastrophic health expenditure is found to be concentrated among high consumption expenditure households in India. Households from SCs are more likely to incur catastrophic health expenditures compare to the households of the general category (Pal, 2012). We use the methodology of calculating the catastrophic payments for healthcare following Wagstaff and van Doorslaer (2003). An OOP payment for healthcare is considered ‘catastrophic’ when the payment exceeds some threshold (Zcat), defined as a fraction of total household consumption or non-food consumption. If T represents OOP payments for healthcare, x represents total household expenditure and f(x) stands for food expenditure, then a household is said to have incurred catastrophic payments when T/x or T/[x−f(x)] exceeds a specified threshold, Zcat. The approach used to measure catastrophic payments in healthcare involves analysing the incidence of catastrophic payments; that is, the percentage of households that spend more in healthcare than the threshold, which can be measured by the headcount (HC). HC is the fraction of the sample whose expenditures as a proportion of total income exceed the threshold Zcat. HG
i
is the ‘catastrophic overshoot’, which equals Ti /xi – Zcat if Ti /xi >Zcat and zero otherwise. The catastrophic overshoot captures the average degree by which payments (as a proportion of total expenditure) exceed the threshold Zcat. If we let Ei = 1 if HG
i
> 0 and Ei = 0 otherwise, then the headcount is given by expression (3):

where N is the sample size and µE is the mean of Ei, while HC captures only the incidence of any catastrophes occurring and O captures the intensity of the occurrence as well.
We have again calculated the concentration index of Ei in order to determine whether poor households incur more catastrophic payments than rich households. If the value of CI for Ei is positive, then there is a greater tendency for rich households to exceed the threshold, while negative values indicate a greater tendency for poor households to exceed the threshold.
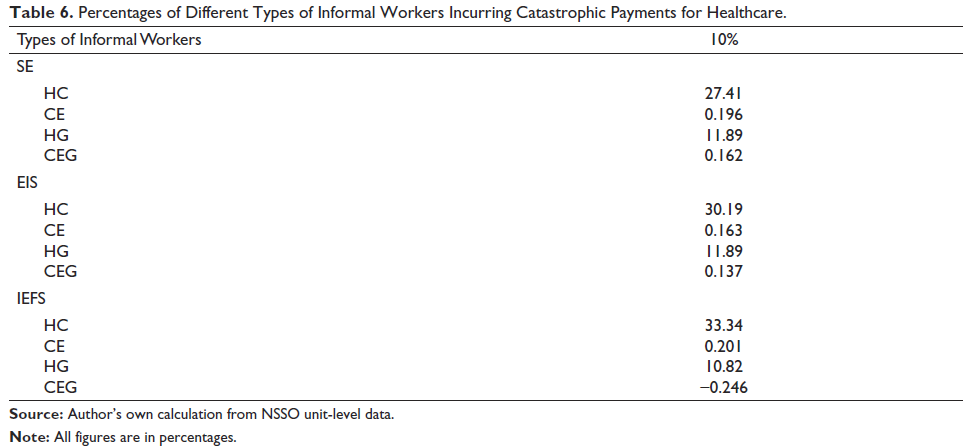
The estimates of HC are calculated on the basis of the 10% threshold only as it is widely accepted as a standard. The OOP payments across different types of informal workers have been displayed in Table 6. Across different types of informal workers, HC has been highest among IEFS followed by EIS and the lowest among SE. However, it is found that HG has been the same across SE and EIS and lower among IEFS. The concentration index of HC (CE) is positive for all types of informal workers indicating that there is inequality in the spending of yearly health expenditure. The Concentration Index for HG (CEG) is also positive for all types of informal workers except IEFS which reflects that inequality in HG has been lower among them.
Percentages of Different Types of Informal Workers Incurring Catastrophic Payments for Healthcare.
Determinants of the Incidence of Catastrophic Health Expenditure Among the Informal Workers in India
It is clear from the above discussion that health expenditure is catastrophic for a large part of the informal workers but not for all. In this section, we would like to explore the possibility of incurring catastrophic health expenditure (yearly) among the informal workers in India. In other words, the initial objective is to identify whether informal workers are subject to catastrophic health expenditure or not. Then we would like to look into the possible determinants of catastrophic health expenditure. Since, selectivity bias hardly exists in our data, so we have used the Probit model to find out the determining factors of the incidence of catastrophic health expenditure (yearly). The catastrophic health expenditure of 10% has only been considered in order to find out the determining factors. The dependent variable Yi* is taking binary values 1 and 0 where 1 indicates that the ith informal worker has to undergo catastrophic expenditure of 10% and above and 0 indicates otherwise. The dependent variable is thus a dummy variable and hence justifies our regression equation. Just like the previous regression, we once again use two different models which are mentioned below.
Model 3
Model 4
It is true that income is one of the most important explanatory variables. As income rises, the ability to pay for healthcare without affecting the consumption of necessary goods will also rise. This possibly can lower the incidence of catastrophic OOP health expenditure in a household. Thus there should be a negative relationship between workers’ income and the ability to pay for OOP healthcare expenditures (Pal, 2012). However, information on income has been unavailable in our data. The wage of the workers might be considered as a proxy of income which is available in our data. Even then we have not considered wage because wage information is not available among the SE. Household assets might be considered as a proxy of income, and in turn, considered as an important explanatory variable for calculating determinants of catastrophic healthcare expenditure. ‘assets i ’ represents the total amount of assets possessed by ith informal workers (Pal, 2012). The Land possessed 11 is also an important explanatory variable among the rural workers (Pal, 2012). Here ‘land i ’ is the total amount of land possessed among the ith informal workers. Furthermore, cooking methods and access to household electricity can also be considered an important explanatory variable of the catastrophic OOP health expenditures. Access to cooking methods and electricity not only is an indicator of workers’ well-being but also these possessions determine workers’ health risks. Long-term exposure to solid cooking fuels enhances the chances of falling ill (Pal, 2012). The extent of exposure to health risk in turn determines the OOP health expenditures. Here ‘fuel i ’ represents the cooking methods and electricity used by ith informal workers.
Years of education are also here considered as a possible determinant of OOP catastrophic health expenditure. Education undoubtedly enhances individuals’ care for their health and thus catastrophic health expenditure among individuals is likely to decline (Cowell, 2006; Grossman, 1999; Pal, 2012). Additionally, according to Cowell (2006), education increases the opportunity cost of getting ill. Furthermore, it can also be said that as income increases, education also increases. Thus an increase in education reduces the likelihood of OOP health expenditure. Therefore, ‘Edu i ’ represents the education of the ith informal worker. Female literacy also plays a very important role in health expenditure and hence catastrophic health expenditure (Gupta & Joe, 2013; Pal, 2012). So, the interaction dummy between education level and gender of the household head has been considered to check this hypothesis. Thus the interactive dummy that is ‘female liti’ and ‘female edu i ’ represent female literacy and years of education of the female member respectively.
Apart from that presence of young family members and senior citizens in the family also enhances the health expenditures and in turn catastrophic health expenditure (Cavagnero et al., 2006). Moreover, a larger household size means a higher probability of being ill. Thus there has been a positive relationship between household size and catastrophic health expenditure (O’Donnell et al., 2005). ‘Young i ’ represents workers with dependents less than 15. ‘Old i ’ represents workers with dependents greater than 60.
Just as the health expenditure, the social background also plays a very important role in determining catastrophic health expenditure. ‘Caste i ’ represents the social group of the ith informal worker. Therefore, three different dummies are considered to represent the deprived social groups. These are scheduled tribe (ST), scheduled caste (SC) as well as other backward workers (OBC). Compared to the others (general), our objective is to investigate the extent of catastrophic health expenditures among the deprived social groups.
The age of the household head also plays a major role in determining the extent of catastrophic health expenditure (Pal, 2012). ‘age i ’ is considered the age of the head of the family. Apart from age of the household head, the gender of the household head also plays a major role in determining catastrophic health expenditure. As explained in Cavagnero et al. (2006), female-headed households have a higher chance of facing catastrophic health expenditure compared to that male-headed households. ‘Hh i ’ represents the household head of the ith informal worker. So female-headed household is considered as a dummy variable and would want to investigate whether catastrophic health expenditure is higher among the female-headed household compared to that of those males.
Besides, it would not be unwise to investigate how far catastrophic health expenditure is different across rural and urban areas. So, we have created a dummy variable for rural areas in order to put some light on this matter in the rural area compared to that the urban area.
Lastly, ‘size i ’ has been considered as an important explanatory variable representing the size of the household. Pal (2012) also considered household size as an important explanatory variable in order to find out the determinants of catastrophic health expenditure. The result obtained in that article is that a higher household size significantly reduces the chances of catastrophic health expenditure.
Just like the health expenditure, ‘Informal workers types i ’ are considered in the explanatory variables in Model 3 to understand the extent of catastrophic health expenditures among informal workers across different heterogeneous groups.
Results and Discussions
The results of the determinants of catastrophic health expenditures (yearly) among the informal workers have been done with the help of the Probit model and are represented in Table 7. Incidence of catastrophic health expenditures is significantly higher among the EIS but lower among the IEFS compared to that of SE. In contrast to that of the OOP health expenditure, we hardly find any significant result in determining catastrophic health expenditures among the rural workers compared to the urban workers.
Factors Responsible for the Incidence of Catastrophic Health Expenditure Among the Informal Workers in India Using a Simple Probit Model.
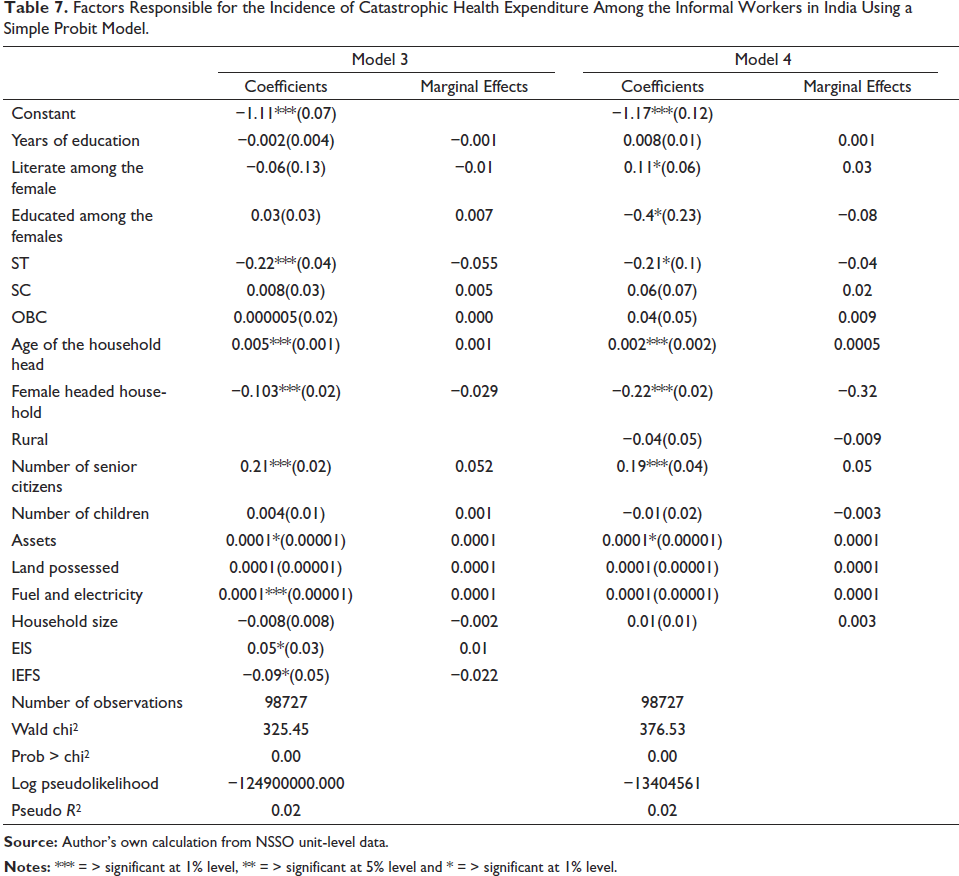
The age of the household head significantly enhances the probability of catastrophic health expenditures. The parameter estimate of the female-headed households is negative and significant which highlights that the chance of catastrophic health expenditure is lower among them compared to the male-headed household. In contrast to the existing theories, years of education are hardly statistically significant in determining catastrophic health expenditures. Not only that, the interaction dummies like female years of education and female literate workers also do not have any impact on catastrophic health expenditure. As far as the economic condition of the informal workers is concerned, it is found that the availability of assets and expenditure on fuel and electricity play a significant role in determining yearly catastrophic health expenditures. However, possession of land hardly has any impact on the catastrophic yearly health expenditure. Apart from that number of senior members in the family increases the chance of yearly catastrophic health expenditures. Lastly, vulnerable social groups such as STs have lower possibility of the incidence on catastrophic health expenditures compared to the non-scheduled social group.
Conclusion
The findings of the present analysis show that the average OOP yearly health expenditure is highest among the EIS compared to SE and IEFS. However, the out of total heath expenditure has been the lowest among them. Thus it is observed that in the group of workers whose mean health expenditure is the highest, the OOP share of healthcare has been the lowest for them. It is also found that assets, household head, social group and types of employment are important determinants of health expenditures. The health expenditures have been highest among the EIS followed by SE while it is least among the IEFS. Compared to IEFS and SE, HC for catastrophic payments has been the highest among EIS. Considering catastrophic health expenditure among the informal workers in India, the determining factors are age and sex of the household head, possession of assets, expenditure on fuel and electricity and the number of senior citizens in the family. However, contrary to the theory, years of education, as well as the interactive dummies like female education and female literacy are not at all determining factors of catastrophic health expenditure. Moreover, compared to SE, the incidence of catastrophic health expenditures has been significantly higher among the EIS but lower among IEFS. Workers in the rural area spend a significantly higher amount on OOP health expenditure compared to those in the urban area. However, this result is insignificant so far as catastrophic health expenditure is concerned. Thus the policy prescription for improving the health situation among the informal workers is to identify them and provide them with better earning opportunities so that their economic condition can be improved.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.