
Abstract
The study aims to understand the major determinants of infant mortality in infant mortality-prone annual health survey states of India. The study has considered district level infant mortality rate as a dependent variable and household size, sex ratio at birth, female literacy, marriage before the legal age, birth spacing, full antenatal care, Mothers who received post-natal care within 48 hours of delivery, Children within 12 to 23 months who are fully immunised, Breastfeeding within 24 hours of birth, Children aged 6 to 35 months are only breastfed for the initial 6 months, women who are aware of HAF/ORS/ORT, and women who are aware of ARI/Pneumonia as independent variables. The study considered district-level data on the mentioned variables over nine annual health survey states over three years. The results reveal that female literacy, birth spacing, immunisation, only breastfeeding till 6 months, and awareness regarding HAF/ORS/ORT all have a statistically significant negative impact on IMR. On the other hand, post-natal care has a statistically significant positive impact on IMR. This surprising result can have two explanations. First, only those children receiving PNC who are already sick and succumbing to their sickness. Second, the patient death rate owing to hospital infection in India is very high, so it may be that infants are succumbing to this particular aspect. Identification of major determinants of infant mortality will eventually lead to actions against them, and that, in due course of time, will tame the onrush of infant mortality in Annual Health Survey States as well as other parts of India and the world. Quantification and determination of the major determinants of infant mortality for the annual health survey states are missing till date, and from that aspect, the article is novel.
Introduction
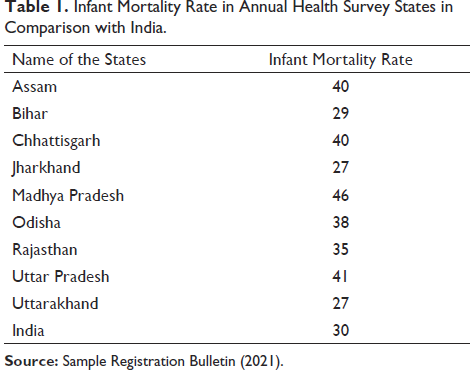
Survival of the infants is one of the most important development indicators. However, India has performed moderately in ensuring their survival. Moreover, the six out of nine Annual Health Survey States of India are lagging far behind the national level regarding infant survival as depicted in Table 1.
Infant Mortality Rate in Annual Health Survey States in Comparison with India.
In this background, it becomes immensely important to identify the major determinants of infant mortality rate (IMR) in the Annual Health Survey States. However, before delving into data analysis, an exhaustive mention of the prime determinants of IMR as documented in the existing literature has been undertaken.
Literature Review
The following literature review has been conducted to pick up the major variables that impact infant mortality.
Sex Ratio at Birth
The relation between IMR and the sex ratio at birth change over time and between countries (Diamond-Smith & Bishai, 2014). Sadly, four million children die within one year of their birth every year. The majority of fatalities are caused by avoidable causes in developing and less developed nations (Perez-Patron & DeSalvo, 2019). There are many incidents in India where a child’s death occurs unexpectedly, with no prior history of disease. The majority of these deaths were in females. The mortality rate for female infants is 1.3 times greater than that of male infants (Khanna et al., 2003). On the other hand, in most nations throughout the world, the mortality rate for male infants is greater than that for females, and males are naturally weaker than females, making them more susceptible to diseases and untimely mortality (Anson & Sun, 2002; Lai, 2005; National Vital Statistics Reports, 2010; Pongou, 2012).
Mothers Who Received Full Antenatal Check-up
Pregnancy-related health-seeking behaviour may have major effects on both the mother and the unborn child’s well-being. Without antenatal care, women have an increased chance of miscarriage, stillbirth, and maternal mortality (Kost et al., 1998). Healthy lifestyle promotion, malnutrition prevention, and raising awareness of gender-based violence are just a few of the ways that an ANC (Antenatal Care Programme) may help reduce mother and infant death rates (Berglund & Lindmark, 2016; Kanyangarara et al., 2017; Khan et al., 2006; Zhou et al., 2019). Women in many poor nations do not attend antenatal care clinics, as a consequence, they are not getting the properantenatal care (Ochako & Gichuhi, 2016). Mothers who have had a full ANC before delivery have a better understanding of the health issues that may occur during and after delivery, as well as a lower risk of maternal, new-born, and infant death (Ochako & Gichuhi, 2016). Kuhnt and Vollmer (2017) discovered that new-born and infant mortality rates are significantly higher in mothers who did not get any antenatal care.
Household Size
The link between the size of a family and IMR is debated. Living in a large family may raise the risk of mortality owing to the ease of transmitting airborne infectious diseases (Beemer et al., 2005; Bernhardt, 1995; Liu et al., 2015; Reid, 2002). Infant survival rates seem to be unaffected by household size, which might be explained by the fact that distinct variables have opposing effects and cancel each other out. Because big houses were more common among the upper socioeconomic classes, babies in these households would have been less prone to poverty as a result of their exposure to sickness (Jaadla & Puur, 2016). On the other hand, Gupta et al. (2016) observed that IMR is adversely correlated with household size.
Female Literacy
Women‘s literacy rate has assisted greatly in decreasing the IMR in the developing world. Zakir and Wunnava (1999) used a cross-sectional model to examine variables impacting IMR in 117 countries in 1993 and identified that female literacy rates have the greatest influence on IMRs. IMR has decreased significantly as a result of the increased literacy of women, and this has improved the health of children (Batool et al., 2019). The advantages of community education, particularly for females, are inversely related to IMR (Barenberg et al., 2016; Ladusingh et al., 2016). Vijayakumar et al. (2016) analysed data from two census years, 2001 and 2011, and discovered the inverse relation between the female literacy, and IMR. Susuman et al. (2014) analysed 2011 census data and discovered that Kerala had the highest female literacy rate (92%) and the lowest IMR in India. Mukherjee et al. (2019) used Sample Registration System (SRS) data of December 2016 to recognise the determinants of IMR in rural India and found, female education is a significant predictor of IMR. A 1% increase in female literacy reduces IMR by 0.763%.
Birth Spacing
To ensure the health and well-being of both mother and child, the WHO advises that women space their pregnancies between 3 and 5 years apart (WHO, 2007). It has been shown that there is a relationship between short birth intervals and mortality repeatedly in a variety of developmental circumstances (Aleni et al., 2020; Cheslack-Postava et al., 2011; Kozuki et al., 2013; Perin & Walker, 2015; Whitworth and Stephenson, 2002). Optimising birth spacing has the capability to minimise the infant mortality rate for both white and black moms by a substantial amount (McKinney et al., 2017). Inadequate birth spacing increases the risk of preterm delivery (Conde-Agudelo et al., 2012), perinatal, neonatal, and infant death (Simmons et al., 2010), as well as illness associated with premature infants and childhood anaemia (Sinha et al., 2017). But some of the authors observed that in the case of developed countries, low weight, the risk of premature births, anaemia, and IMR appear to be unrelated to birth intervals (Ball et al., 2014; Class et al., 2018; Molitoris et al., 2019). On the other hand, current studies on poor communities, however, have indicated that birth intervals continue to be critical for IMR in developing and less developed countries (Baqui et al., 2019; Molitoris et al., 2019; Ogbo et al., 2019).
Children Within 12 to 23 Months Who Are Fully Immunised (IM)
Basic immunisation encompasses all vaccines administered during the first year of life and has served as the benchmark for assessing immunisation programmes (Peck et al., 2019). Immunisation is an important tool for accomplishing the target of reducing under-five mortality (WHO, 2009b). The immunisation of children has resulted in a large decrease in morbidity and death from several illnesses, consequently decreasing the IMR (UNICEF, 2005). It has been shown that childhood vaccines are beneficial in safeguarding children from vaccine-stoppable illnesses, particularly in poor and middle-income countries (Danielsson et al., 2009; Davis & Shah, 2019). Vaccination prevents around 2.5 million new-born deaths each year (WHO, 2009b).
Children Breastfed Within 1 Hour of Birth (BF)
Breastfeeding provides several health advantages for both the mother and the baby, both in the short and long term. It is recommended by both the WHO and UNICEF that breastfeeding should be started immediately after birth and should continue for the first 6 months of life (WHO, 2009a). But fewer than 43% of new-born babies are breastfed during the first hour of life, and less than 40% of infants younger than six months are exclusively breastfed (WHO, 2022). The probability of IMR increases when breastfeeding is not commenced promptly after delivery (Edmond et al., 2006). Breastfeeding exclusively lowers the incidence of diarrhoea, pneumonia, and other infectious illnesses in children (Biks et al., 2015).
Children Aged 6 to 35 Months Only Breast Fed for the Initial 6 Months (BFF)
It is widely accepted that breastfeeding duration is shorter in developed countries compared to developing and less developed countries (Victora et al., 2016). Exclusive breastfeeding is described as ‘providing a baby solely with breast milk during the first six months of life with no additional food’ (UNICEF & World Health Organization, 2003). Breastfeeding stimulates sensory and cognitive growth in infants and protects them from viral and chronic disorders. It also significantly minimises IMR and assists in a faster recovery from sickness (Kasahun et al., 2016). Inadequate breastfeeding within the first six months after birth is a key risk factor for increased IMR, and it also has a protective effect on morbidity and mortality associated with diarrhoea during the first two years after birth (Lamberti et al., 2011). Infants who received breast milk as their major supply of milk until the age of 12 months had fewer gastrointestinal illnesses than infants who were breastfed for a shorter time (Dewey et al., 1995).
Mothers Who Received Post-natal Care Within 48 Hours Delivery
The World Health Organization (WHO) defined ‘post-natal care (PNC) as care given to the mother and her new born baby immediately after the birth of the placenta and for the first 42 days of life’ (WHO, 2008). Care delivered in the postpartum phase allows healthcare professionals to recognise post-delivery disorders and administer remedies quickly (Khanal et al., 2014). The immediate post-natal period, sometimes known as the ‘immediate postpartum period’, accounts for around half of all maternal fatalities and 40% of all new-born deaths (Swain et al., 2017). The WHO recommends that healthy infants delivered naturally in a health institution should be cared for at least 24 hours after their birth. Post-natal care should begin within 24 hours after the baby’s delivery, if possible (WHO, 2013). In less developed nations, fewer than a quarter of neonates get PNC during the first 48 hours after birth (Sines et al., 2007). Mother’s post-natal care within 48 hours of delivery decreases the chance of death of new-borns (Swain et al., 2017).
WAH-Women Who Are Aware of HIV/AIDS, RTI/STI, HAF/ORS/ORTAND ARI/Pneumonia (AWAF)
Gabida et al. (2015) opined that mother-based promotion of awareness regarding diarrhoea is an effective tool to prevent the disease and reduce its days of suffering in Zimbabwe. Higgins-Steele et al. (2017) found that in Afghanistan, infant deaths can be reduced to a great extent through awareness generation among mothers regarding pneumonia and diarrhoea. Freeman et al. (2017) using randomised controlled trials have shown that for some South Asian and sub-Saharan countries, generating awareness regarding diarrhoea, HIV, pneumonia, and malaria can act as a wonder in improving the infant and under 5 mortality rates.
It is apparent from the above literature review that at pan-India level no quantitative analysis has been conducted to determine the major determinants of IMR especially with granular data. In this background, the present article undertakes a district level analysis of the Annual Health Survey states to determine the major determinants of IMR.
Methodology
The present article considers district level data from the Annual Health Survey regarding the above-mentioned variables and runs panel data analysis following the regression equation as mentioned below, after checking for multicollinearity. The concerned analysis encompasses data on the mentioned variables over 271 districts in 9 states for three years (2011–2013). The regression equation might be represented as
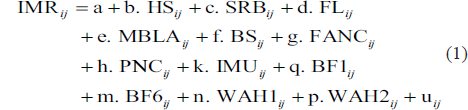
where i = 1,2, …,271 and j = 2011, 2012, 2013
and, IMR = infant mortality rate, HS = household size, SRB = sex ratio at birth, FL = female literacy, MBLA = marriage before legal age, BS = birth spacing, FANC = full ante natal care, PNC = mothers who received post-natal care within 48 hours delivery, IMU = children within 12 to 23 months who are fully immunised, BF1 = breastfeeding within 24 hours of birth, BF6 = children aged 6 to 35 months only breast fed for the initial 6 months, WAF1 = women who are aware on HAF/ORS/ORT, WAF2 = Women who are aware on ARI/Pneumonia. u it represents the stochastic random error.
Data and Analysis
Considering the short panel nature of the data, first multicollinearity, autocorrelation, heteroskedasticity, and contemporaneous correlation have been tested.
As illustrated in Table 1, according to the variance inflation factor, there is no multicollinearity among independent variables. The Wooldridge test (2002) for first-order autocorrelation declared that there is no autocorrelation in the error structure of the data under consideration. The Greene (2000) test for group-wise heteroscedasticity found the presence of heteroscedasticity in the error structure ofthe model. Pesaran (2021) test for contemporaneous correlation, had found cross sectional dependence in the error structure in both the fixed and random effects models. Cameron and Trivedi (2005) had earlier mentioned that ignoring heterogeneity and correlation across units might lead to biased estimation. Again, Chudik et al. (2011) have said that if the number of cross-sectional units (N) is much larger than the time units (T) then cross-sectional dependence should always be taken into account. With the growing financial integration among financial entities, the cross-sectional dependence of banks is becoming obvious, and consideration of the same is becoming important. In cases where the cross-sectional dependence is for unobserved common factors that are uncorrelated with the regressors, fixed effects (FE) or random effects (RE) estimators might be considered, and the standard errors might be corrected following the Driscoll and Kraay (1998) approach. However, if the unobserved common factors responsible for cross sectional dependence are correlated with the regressors, then the Pesaran (2006) method should be used for estimation of the coefficients, as the Driscoll and Kraay (1998) method would not work and FE and RE estimators would be biased and inconsistent (De Hoyos & Sarafidis, 2006). However, if the relationship (correlated or not correlated) among unobserved common factors and regressors is not known, then the choice between Driscoll and Kraay (1998) and Pesaran (2006) is dubious. Beck and Katz (1995) have used Monte Carlo Simulation to explain and favour the use of ordinary least squares, with panel corrected standard errors over more advanced FE and RE models as well as the generalised least squares (GLS) estimator for panel data sets exhibiting both heteroscedasticity and cross-sectional dependence. Ardizzi et al. (2014), encountering a similar problem with the data set, also followed the method proposed by Beck and Katz (1995) but with Prais and Winsten (1954) regression to adjust for autocorrelation. In parlance to Ardizzi et al. (2014), Prais and Winsten (1954) regression have been considered as the data set is with autocorrelation problem along with the other mentioned errors as depicted in Table 2.
Econometric Test Results.

Now Eq. (1) has been estimated following Prais–Winsten regression with PCSE and the result is depicted in Table 3.
Prais–Winsten Regression with PCSE (Dependent Variable: IMR it ).
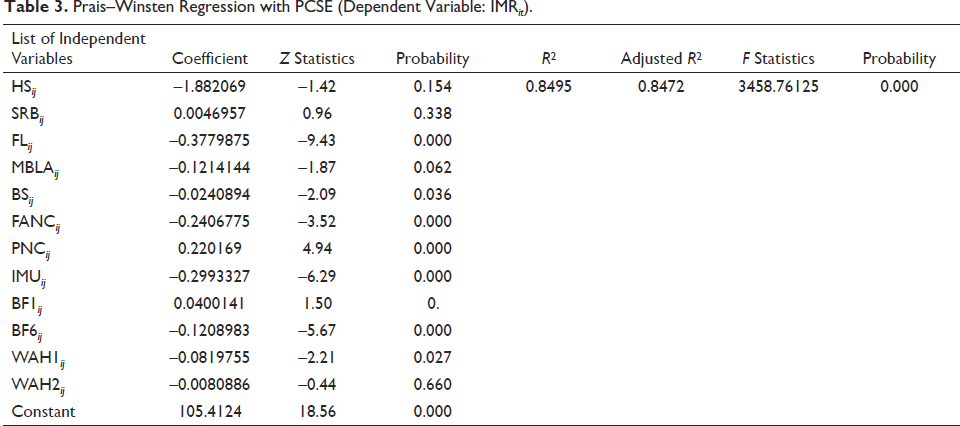
It is apparent from Table 3 that female literacy, birth spacing, full ante-natal care, children within 12 to 23 months who are fully immunised, children aged 6 to 35 months only breast fed for the initial 6 months, women who are aware on HAF/ORS/ORT, all puts a statistically negative impact on infant mortality rate. Ironically, mothers who received post-natal care within 48 hours delivery leave a statistically significant positive impact on infant mortality rate. Two tentative explanations can be forwarded regarding this element of surprise. Following the World Health Organization doctrine, a mother and her baby cannot be discharged of the health facility unless the mother stops bleeding and baby shows no visible infection. It might be that babies undergoing post-natal care within 48 hours of their birth are inherently weak and re succumbing to their already declining health. One more possibility pops up; in India death of patient owing to infection carried from hospital is quite high. The babies who are under the hospital supervision after their birth may be contaminated certain infection and succumbing to them. However, elaborative research in this aspect is required and that is beyond the purview of the present paper at its current state.
Conclusion
The present article devoted itself in identifying the major determinants of IMR in Annual Health Survey States of India. It is apparent that boosting female literacy, birth spacing, immunisation programmes, breastfeeding practices, and awareness of women regarding HAF/ORS/ORT will eventually bring down the IMR to a manageable level. Furthermore, the statistically significant positive relation between infant mortality rate and post-natal care is an eye opener. This might have two explanations. First, the babies that are seeking post-natal care are already sick and succumb to their sickness. Secondly, infection from hospitals is a major issue in India, and each year, many patients who are even cured successfully die of the infection that they carry afterwards. As a policy prescription, spreading awareness regarding breastfeeding, birth spacing, immunisation and awareness regarding specific aforementioned symptoms will do wonders. To turn the dice for post-natal care the health facilities should abide by government-determined protocols and that may eventually turn the impact of post-natal care on infant mortality rate from positive to negative. Children are the bedrock of any society. Their safe survival and, ultimately, their contribution to the socio-economic aspects of a country define the locus of the future growth. India, as an emerging developing country, cannot afford any lax in this aspect and must by any means identify and address the reasons behind its high IMR and, more importantly, the higher IMR of the Annual Health Survey States.
Authors’ Contributions
All the authors have equal and substantial contributions
to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND to drafting the work or revising it critically for important intellectual content; AND in final approval of the version to be published; AND in agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. all authors read and approved the final manuscript.
Availability of Data and Materials
The data sets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.