
Abstract
The Postgraduate Diploma in Public Health Management (PGDPHM) was launched in 2008 to create a cadre of public health managers within the ranks of the public healthcare system. However, limited research exists on this programme and its impact on the health system. This qualitative research study aimed at obtaining in-depth perspectives of PGDPHM graduates from the Indian Institute of Public Health-Gandhinagar (IIPHG). Study participants were selected from a variety of roles across Gujarat. The programme equips healthcare professionals with several competencies essential to the management of public health issues from the community to state levels. However, the health system has yet to fully realise its potential and rationally allocate this human resource. Recognition also has not translated into public health oriented career growth for most graduates, and the duties of medical officers with this qualification continue to have a clinical focus. The PGDPHM programme has the potential to help ensure that India reaches an adequate capacity for health management professionals. It would be beneficial to improve recognition for the programme within the health system, increase focus on public health research and conduct regular evaluations to assess the career trajectories of graduates.
Keywords
Introduction
Public health management is the optimal use of resources in society and health services towards improving the health experience of the population (Negandhi et al., 2015). Public health qualifications provide health functionaries with an in-depth understanding of health systems required to design, implement, monitor and evaluate health programmes, supervise the public health workforce, assess public health issues and develop appropriate strategies to address emerging challenges (Angood & Birk, 2014).
The Indian health system recognised the importance of a public health perspective in medical and health education as early as the 1940s in the Bhore Committee Report, which discussed the lack of focus on preventive and public aspects in medical education at the time (Chauhan, 2011). Specifically, the need for doctors in the public healthcare system to have public health skills was highlighted by the Kartar Singh Committee in 1973 (Singh, 1973). Further, in 1999 under the ‘Calcutta Declaration on Public Health’, a need to rearchitect public health education was expressed to strengthen the health workforce and the health system (Sharma & Zodpey, 2011). At the same time as the launch of the National Rural Health Mission, it was stated by the National Commission of Macroeconomics and Health that the lack of public health training for doctors in the government healthcare system had severely impacted progress in health in India (Zodpey et al., 2015). Even today, among all cadres of the health workforce, public health professionals are in acute shortage in India. The landscape of public health education in India has traditionally focused on medical professionals through Doctor of Medicine programmes in community medicine, and more recently, graduate-level programmes for those from a non-medical background (Sharma & Zodpey, 2011). While these strides potentially contribute a trained public health workforce to the country, there is a need for a specialised public health cadre, to be drawn from within the ranks of in-service physicians in the government healthcare system. This could ensure that public health programmes and policies would be helmed by professionals trained in public health management, monitoring and evaluation, as well as in-depth knowledge of the challenges in implementation.
Since its launch in 2005, the National Health Mission (NHM) included a focus on education and training initiatives for health functionaries in order to keep their skills up-to-date and provide them with a broad swathe of knowledge necessary for public health management (Negandhi et al., 2015). Even today only two states, Maharashtra and Tamil Nadu, have a dedicated and active state infrastructure for public health (Kumar et al., 2016). In Maharashtra, this has taken the form of a distinct department of public health that functions in an intersectoral manner to address disease outbreaks and measures for ensuring a clean environment in communities and vector control. In Tamil Nadu, the Directorate of Public Health works alongside other sub-departments in health to ensure good quality and low-cost public healthcare, disaster anticipation and disease management (Kumar et al., 2016).
The Postgraduate Diploma in Public Health Management (PGDPHM) programme, launched in 2008 allowed doctors serving within the public healthcare system to become interface professionals (Angood & Birk, 2014). By offering a management curriculum specific to public health, the programme also remedied a previous trend where health sector organisations were staffed with traditional management professionals with little public health knowledge (Tiwari et al., 2018). The programme was designed to enhance candidates’ knowledge about public health issues and their management, through both classroom-based learning and practical experience (Zodpey et al., 2012). According to the health workforce literature, the Indian health system will need to add nearly 45,000 public health management professionals to reach the target of 2.97 health managers per 100,000 by 2030 (Tiwari et al., 2018). The PGDPHM programme has the potential to achieve this goal. It is, therefore, necessary to evaluate the experiences of programme graduates in order to create a body of evidence that can contribute to the growth and development of this programme.
Objectives
The aims of this research were to evaluate in detail the professional journey of its graduates, their learnings from the programme and the response of the health system to public health managers so trained.
Methods
A qualitative study design is highly appropriate to assess the impact of such a programme, as it helps the researcher to obtain a deeper understanding of issues, and the perceptions and experiences of study subjects (Negandhi et al., 2015). A semi-structured in-depth interview guide was prepared after a review of the literature on the PGDPHM programme (Zodpey et al., 2012) and other public health education programmes.
Twenty-five government-nominated medical officers (MO) who graduated from the PGDPHM programme at the Indian Institute of Public Health Gandhinagar (IIPHG) between 2008–2009 and 2018–2019 were purposively sampled. To obtain a variety of perspectives, respondents were selected across Gujarat, from various levels in the public healthcare system, including rural primary care providers, and health officers in various state-level programmes.
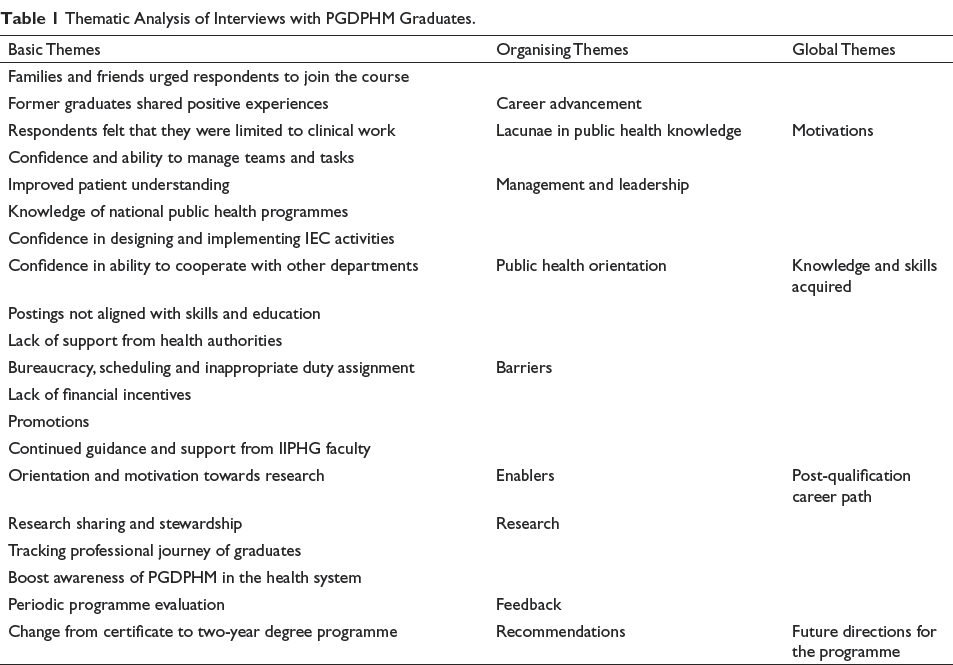
Informed verbal consent was obtained. All interviews were conducted verbally in English and Gujarati, with note-taking preferred by the respondents over audio recording (Sharma et al., 2014). Each interview lasted from about 30–90 minutes. Notes were compiled into coherent transcripts for qualitative analysis. Codes were ascribed to significant statements and then compared across transcripts to identify similar constructs and generate basic themes. This was repeated to create a thematic network which described the fundamental structure of the findings. Table 1 describes the basic, organising and global themes.
Thematic Analysis of Interviews with PGDPHM Graduates.
Results
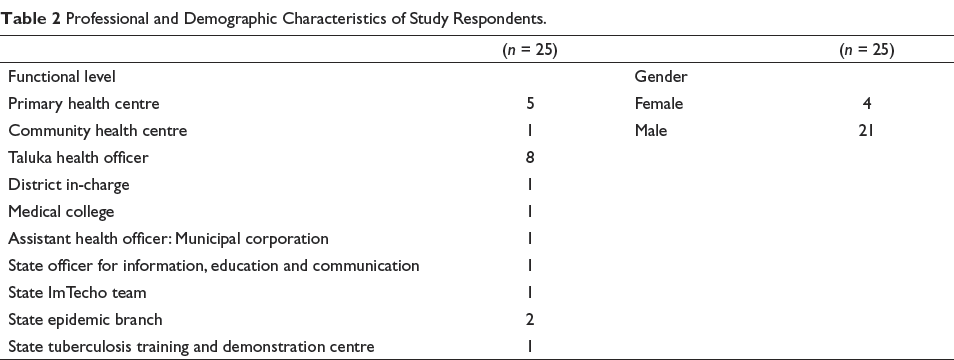
Twenty-five MO practising in various districts of Gujarat were interviewed. Table 2 provides a distribution of the gender and functional role of the respondents, before enrolment into the programme.
Professional and Demographic Characteristics of Study Respondents.
Motivations
Respondents showcased a passion for public health and felt that this programme would help them serve their communities better.
I am passionate about public health and to serve at grassroots level. I felt that this program would give me the skills to improve overall health for my community. (MO 5)
Knowledge and Skills Acquired
Respondents noted that operational skills, such as team management, delegation and programme implementation, enhanced their confidence and enabled them to make streamlined decisions, as physicians and public health managers. Increased facility with digital platforms was perceived to be helpful with work planning, visualisation and analysis of data, which subsequently helped them identify public health issues in their communities and implement relevant solutions.
The program was highly suited to my needs as a government care provider in a rural facility. Epidemiological concepts have helped me to identify disease patterns in my community and take swift preventive action. (MO 1) The program helped me to improve micro-planning skills, I don’t feel lost while preparing the Program Implementation Plan (PIP) now. I understand the finer points of health financing, and how to utilize the budget under various programs. (MO 4)
The programme was also deemed beneficial in imparting a public health perspective. Improved understanding of various national health programmes and their implementation at the community level were reported:
Earlier, I had difficulty understanding how to implement the various national programs for the benefit of my community. Now I am able to plan health education and health promotion events in my community, in collaboration with Accredited Social Health Activists (ASHA), Anganwadi Worker (AWW), and Panchayat members and help care-seekers obtain the exact services they need. (MO 3)
The programme was highly aligned with their work within the health system. More importantly, respondents felt that they could view themselves as public health managers with a broad ambit and the ability to work across disciplines and sectors to ensure good health in their communities. An important improvement in decision space was reported as a result of the knowledge and skills acquired in the PGDPHM programme.
When I create a PIP now, it is not just a document, I have a vision for improving health in my community. I coordinate with my colleagues in other sectors to create a holistic and realistic plan to achieve good community health. (MO 15)
Post-qualification Career Path
A mixed experience was reported when respondents returned to work in the health system after completing the PGDPHM programme. Several barriers and enablers were identified.
Barriers
A majority of respondents returned to their duties as MOs and experienced a gap between their newly acquired skills and their practice.
I went back to my old job as a Medical Officer without a promotion. This could be due to a lack of knowledge among the high-level officials about this program. (MO 9)
Many noted that the system continued to direct them into curative and clinical duties, rather than involving them in roles oriented towards public health management. Even after the PGDPHM qualification, they were perceived only as care providers, and promotions to techno-managerial positions were determined by factors other than an appropriate skillset. Respondents also did not see expected financial benefits and pay scale revisions. Advancement opportunities were few and far in between.
Ideally we should be considered for regional and state level program management positions. Rather than conducting deliveries, I can improve maternal health on a broader level but I have not been given this opportunity. (MO 17) I had expected a pay rise, but that has not happened, which is quite demotivating. (MO 16) I applied for the position of Regional Medical Officer which requires considerable public health know-how, but I was told that while my qualification was ‘good to have’, eligibility was determined only by seniority. (MO 10)
Respondents also noted obstacles in testing and implementing innovations and conducting research, which had been an integral part of the PGDPHM programme.
I want to conduct meetings with the CHWs to improve several aspects of community health but I have no support from the Block Health Officer. My attempts to carry out operational research in order to streamline program implementation in my community were thwarted due to several obstacles including data use permissions from various departments. (MO 13)
Enablers
Many respondents pointed out that their knowledge and input were acknowledged by their superiors in public health matters.
My superiors recognised the skills I had acquired and supported me in running a program. I was given the space to take my own decisions and the necessary resources and logistical support was made available. (MO 2)
Financial, logistics and human resource management were seen as the most valuable skills which enhanced objective thinking and even clinical decision-making.
I am now able to delegate work and set results-oriented targets for my team. Even as a clinician, I feel I can provide more precise care now. (MO 3)
Respondents also reflected positively on the support they received from IIPHG after graduating. They received advice and counsel from the faculty on their projects and routine work.
IIPHG has been very helpful after the program. I discuss field-level issues with the faculty and they also encourage me to carry out small research projects and give me ideas for innovative solutions. (MO 12)
Future Directions for the Programme
Respondents shared that cited follow-up training, regular feedback collection and career growth mapping would be beneficial for them, and measures would keep their knowledge up-to-date and ensure rational human resource allocation. It was also suggested that research produced by academic institutions be shared with programme graduates.
IIPHG should share their research with us so that we can apply the same in the field. Most of the time we are too busy to publish our own papers. Follow-up training sessions should be conducted to upgrade knowledge. (MO 2) I am concerned about why there is no regular monitoring of the graduates of this program. Our career progress should be evaluated regularly. (MO 1)
Some respondents felt that PGDPHM should change from a certification to a degree programme with the duration of two years in order to extend its usefulness beyond the government.
The program should be at least 2 years long, and there should be an on-the-job training component, so that we can learn in the real world. (MO 7)
Discussion
Human resources are a critical component of health systems and a public health orientation, and requisite skills are essential for healthcare practitioners in low- and middle-income countries. A health system is a complex adaptive system with various interconnected inputs (Khan et al., 2018) and outputs; however, the individuals who serve within it often tend not to operate in a perfectly collaborative manner (Kuziemsky, 2016). As of 2017, a ratio of only 11 public health professionals per 100,000 population had been estimated (Tiwari et al., 2019) based on projections from clinical human resource shortages. Further, while the National Health Policy 2017 proposed the development of a public health management cadre at the block, district and state levels, very few states have initiated the process of creating the pathway for this workforce (Tiwari et al., 2019). Maharashtra and Tamil Nadu are the only states that have had an active cadre of public health professionals within the public healthcare system for some time, while Karnataka has made strides in the form of a committee to analyse the state’s needs in this area (Babu et al., 2014).
Since its launch in 2008, research on the PGDPHM programme has been limited with this being only the third study to evaluate the programme by assessing the career paths of its graduates (Negandhi et al., 2015; Tiwari et al., 2014). As noted by a large number of respondents in this study, the advantage of a public health-focused programme designed specifically for health system functionaries inculcates a transdisciplinary approach, breaks professional silos (Sharma & Zodpey, 2017) and helps build horizontal system-wide capacities in the health workforce. The findings of this indicate that there is significant support for programme continuation. It was a widely held opinion that this programme had the potential to contribute to the strengthening of the health system. It was also felt that a longer programme, similar in design to other graduate programmes, would allow for in-depth training in various public health disciplines. Several respondents noted a lack of adequate recognition for the PGDPHM qualification within the bureaucratic hierarchy of the public healthcare system. Issues were also seen with resistance against the application of a public health perspective in the field and stymieing of innovative approaches by higher level functionaries in the health department. Even among states making concrete efforts towards instituting a public health cadre, it has been reported that while a public health qualification was among the eligibility criteria, dated strictures such as service tenure were given more importance (Babu et al., 2014).
This represents a lost opportunity as PGDPHM graduates are in-service practising physicians trained in public health management. Further, as public healthcare functionaries, mainly at the primary level, they bring a wealth of knowledge and experience of actual community needs and are acutely acquainted with how the chips of health policy fall at the grassroots level. When realised to their full potential, they have the ability to serve as a driving force in both the formulation and implementation of public health policy and enabling the system to adequately address healthcare access at the last mile. Therefore, it can be argued that increasing recognition of the qualification is another step towards signal boosting and legitimising qualifications such as the PGDPHM within the health system it was created to benefit.
Policy Implications
As some respondents pointed out, the programme may be served by increasing application-based learning preferably with examples from the candidates’ work settings (Nurmala, 2014). The findings of this study with respect to the course and pedagogy covered in the PGDPHM programme are in line with previous research, where respondents commented that while the course structure was adequate, an increase in duration would be beneficial (Negandhi et al., 2015). To accomplish this, pedagogical approaches such as practice-based teaching would be highly beneficial. They not only allow candidates to learn through exposure to real projects with deliverables and the complete organisational landscape of public health but also have the potential to generate collaborative opportunities and funding for the academic institution, thereby contributing to increased recognition for the qualification itself (Greece et al., 2019). While the PGDPHM programme on its own may be insufficient to address the 2030 target of nearly 45,000 public health professionals per 100,000 population, it is an important initiative in reaching this goal. In order to meet the directives of the National Health Policy of 2017 (Ministry of Health and Family Welfare Government of India, 2017), initiatives should be set up at high levels of the NHM and the state health cadres to increase recognition of the programme and ensure that so-trained public health managers are employed and compensated appropriately. Both of these can be accomplished by the creation of a separate and empowered Public Health Council (Tiwari et al., 2018). Moreover, there is a need for periodic monitoring and evaluation of the programme itself in order to determine whether it has been evolving in terms of curriculum, governance and organisational changes in the health system and emerging public health concerns. As pointed out by many respondents, knowledge and perception about the programme within the health system is still young. This calls for research studies into how the PGDPHM qualification is perceived by high and mid-level health functionaries.
The PGDPHM should also include a mandatory research component to create a culture of evidence-based practice in day-to-day public health management, policy-making and clinical practice (Jansen et al., 2010). This will help inculcate a strong practice-based research ethos in the public health workforce and the healthcare system. Moreover, since the programme was launched as a capacity-building initiative to infuse the health system with a much-needed public health workforce, it is perfectly placed to build systemic capacity for the incorporation of scientific evidence in population health improvement endeavours (Brownson et al., 2018).
Strengths and Weaknesses of the Study
These findings can potentially inform changes in programme design and implementation and can be of use to the Gujarat government in implementing a public health cadre. Since the respondent pool for this study consisted of programme graduates from one institution, care should be taken while generalising the findings. Moreover, this study was conducted in Gujarat, a state that does not have a dedicated cadre of public health professionals. Replicating the same in another state with an active cadre may lead to enriched results. Further, it would also be useful to situate research in the context of state policy on placement within public health programmes.
Conclusion
The PGDPHM is a qualification aimed at increasing the public health management capacities of in-service healthcare professionals on a broad array of public health issues. It was launched in response to a need for public health managers across the country. While this programme has been supplying public health managers to the country since 2008, few evaluations have been conducted of its performance. This made an in-depth assessment of the perspectives of programme graduates employed across Gujarat. The programme has been successful and has resulted in a generally positive impact on the health system. However, in order to achieve India’s need for a cadre of trained public health management professionals, the programme requires greater recognition within the healthcare community and regular evaluation.
Footnotes
Acknowledgements
We are very grateful to all the doctors who participated in this study.
Ethics Approval
This study was conducted according to the principles of the Declaration of Helsinki (Cho et al., 2016) and approved by the Institutional Ethics Committee of IIPHG, India. Participation was voluntary in nature, and all participants were informed that they could stop or refuse at any time. Confidentiality was ensured by anonymising all data.
Declaration of Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.