
Abstract
Introduction
Identifying errors in documentation can improve the quality of medical records, healthcare services and health care systems, and thus provide a good framework for improvements in documentation policies. To this end, the current research systematically examined studies reporting documentation errors and deficiencies in medical records.
Method
The systematic review was conducted based on PRISMA. Original articles, published in English from January 2009 to April 2019, were retrieved using the Web of Science, Scopus, EMBASE, PubMed and Google Scholar.
Results
A total of 7,624 articles were found. After the exclusion of duplicates and irrelevant items from this total, just 48 articles met the requirements of the study, among which 47 had some sorts of incompleteness; inaccuracy, 14 articles; inconsistency, 8 articles; illegibility, 7 articles; unsigned document, 4 articles and irrelevancy, 2 articles. Factors contributing to the incidence of documentation errors included occupational stressors, manual documentation and absence of or a defect in local, national and international standards or guidelines, with 12, 9 and 11 articles, respectively.
Discussion
Incompleteness, inaccuracy and inconsistency are common errors in medical records documentation. Adopting necessary policies for enhancing the quality of documentation, making strides towards electronic documentation equipped with automatic error detection systems, and standardising the documentation process can be of great assistance in minimising documentation errors and deficiencies.
Introduction
Medical records are the main repository of data in healthcare services provided to the patient (Gartee, 2011; Homan, 2007; World Health Organization, 2006). They evolve over time and serve as a valuable reference for legal risk protection, emergency care, research and quality assurance (Gutheil, 2004). It is necessary to pay special attention to the quality of medical record data because of their important roles in healthcare management, providing patient care services, supporting administrative-financial processes and insurance payments, quality assurance and measuring the quality of healthcare services, self-management, education, research, monitoring community health and promoting public health and supporting micro- and macro-policies in the health systems (Department of Health (DH) et al., 2011; Green & Bowie, 2011; Haux et al., 2004; Institute of Medicine (US) Committee on Data Standards for Patient Safety, 2003; Moghaddasi, 2005; Oppenheim, 2012; Wager et al., 2017; World Health Organization, 2003).
The World Health Organization (WHO) has emphasised the importance of the quality of medical record data, which could not only improve the quality of healthcare services but also decrease healthcare costs (World Health Organization, 2006). As also emphasised in the literature, it is important to conduct quality control of medical records in order to enhance the quality of their data (Abdelhak et al., 2007; Huffman, 1994; Moghaddasi, 2005; Skurka, 1998). The quality control process helps healthcare systems to consider and evaluate the documentation patterns of physicians and other healthcare providers and assists administrators in making sure of the presence of data quality (Skurka, 1998). Quality control can also lead to the identification of documentation errors and defects and provide a framework for learning from the errors and deficiencies, thereby improving patient safety (Mitchell, 2008; World Health Organization, 2016).
Improved documentation can lead to the identification of the causes of medical errors and initiation of new ways to prevent them (Chowdhury & Habib, 2015). According to Gurley et al. (2018), after clinical judgment and communication, documentation is one of the most common factors affecting malpractice. According to Gutheil (2004), lack of documentation is a significant breach of and deviation from the standard of care. Jeff (2015) implicitly stated that poor documentation may cause malpractice. Proper documentation can reduce medical errors (Achar & Wu, 2012; Edwards & Moczygemba, 2004; Scott, 2013). Chang et al. (2005), in the Joint Commission on Accreditation of Healthcare Organisations (JCAHO) Patient Safety Event Taxonomy, considered three levels for medical errors, known as communication, patient management and clinical performance. They also implicitly referred to documenting errors and deficiencies under the communication level. Because of the importance of communication in promoting patient safety, communication improvement has always been highlighted in the patient safety goals of the Joint Commission (Rodziewicz & Hipskind, 2019). Therefore, proper documentation of medical records, as the most important communication tool of healthcare teams, can lead to better communication and, consequently, improved patient safety.
Given the importance of documentation errors, the identification of these errors is crucial because error detection can lead to improved quality of medical records, healthcare services and health care systems, and it also provides a good framework for learning and modifying documentation policies. According to WHO, learning from errors, especially if considered at the organisational level, can be very productive (World Health Organization, 2016). To this end, this study attempted to systematically review studies that reported documentation errors by performing quantitative and qualitative analyses of medical record data.
Method and Design
In this study, documentation errors were defined as any error or deficiency in recording data in medical record, which could affect the main aspects of information quality and result in poor documentation.
The Prisma guideline (Page et al., 2021) was utilized for reporting this systematic review.
Data Sources and Searches
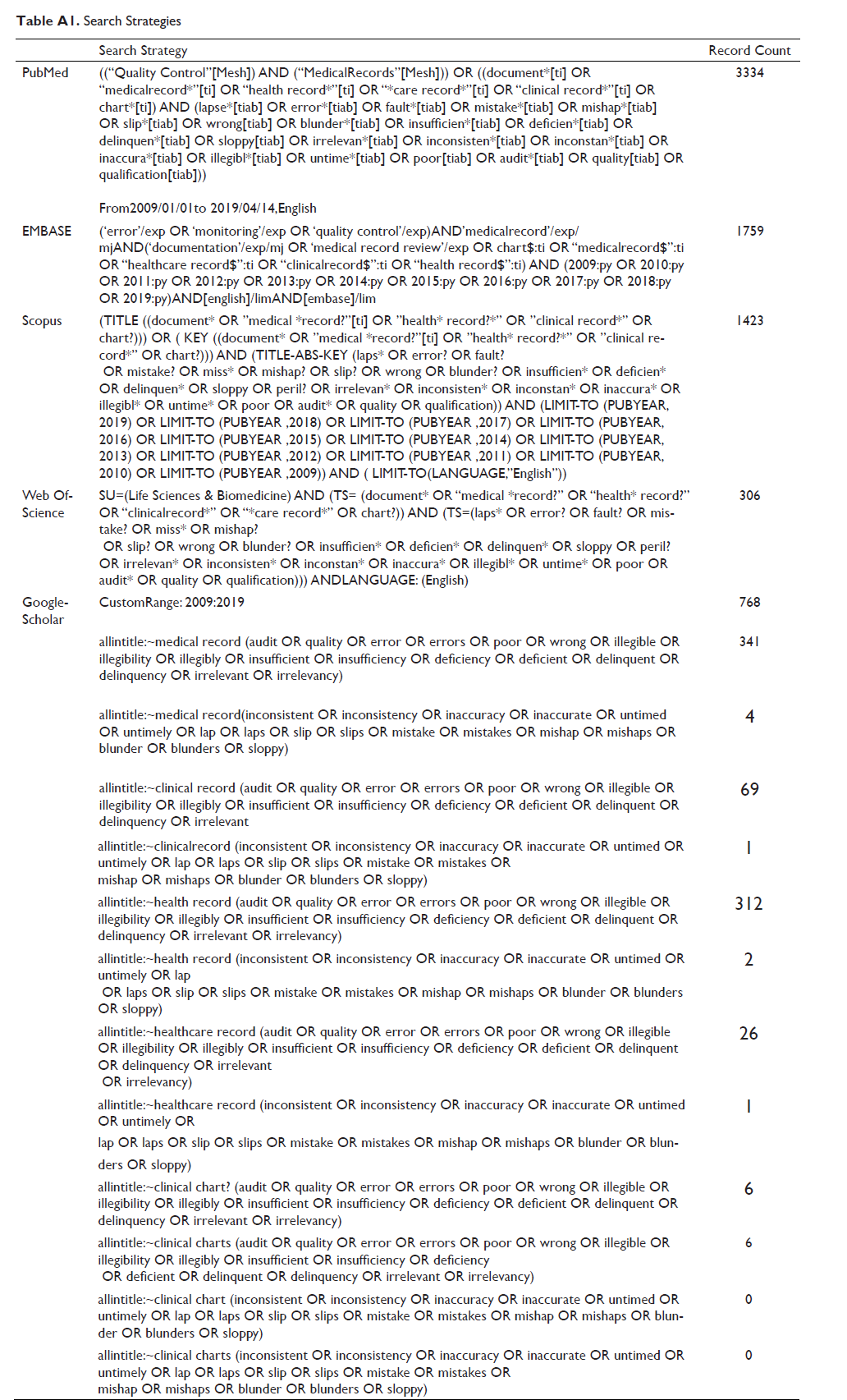
This study used the most popular data sources, that is, Web of Science, Scopus, EMBASE, PubMed and Google Scholar, to retrieve peer-reviewed articles indexed from 2009 to 14/4/2019. In order to formulate a comprehensive search strategy, first, the equivalent terms for the main concepts were identified by referring to the literature and using MeSH and EMTREE thesauri, and consulting with experts. Truncation and wild cards were employed for searching different forms of the words. In order to construct the search strategies, truncation and wild cards, field tags for title, abstract, keyword, MeSH term, EMTREE term, as well as Boolean logical operators, were used according to databases’ instructions. The search strategies for the data sources can be found in Table A1.
Study Selection
The retrieved articles were imported into Mendeley software to identify and remove duplications. Duplicate articles that were not identified by the software in this step were identified and eliminated in the first phase of screening. In the first phase, the articles were screened by title and abstract, and in the second phase, by full text. In the first phase, only original research articles published from 2009 till the time of search time, in the form of journal articles, were included. In the second phase of screening, the full text of articles published in English was selected. In terms of study design, all studies that retrospectively or prospectively reviewed the data of medical records and reported documentation errors with regard to the information quality dimensions of medical records were included. In both phases, two researchers independently screened the documents to identify eligible articles based on the predefined inclusion and exclusion criteria. Disagreements were resolved through the involvement of a third researcher or consensus-based discussion. The quality of the articles was assessed by three researchers on the basis of the STROBE checklist (STROBE Statement, 2007).
Data Extraction
In this stage, the characteristics of the eligible articles and data with regard to the research question were extracted. For each article, the following data elements were extracted and recorded in the two tables designed for this purpose, as follows:
[F]irst author; publication year; the country where the research was conducted; type of study; sample; setting; documentation errors and deficiencies; factors affecting the documentation errors and deficiencies; suggested solutions.
The extracted data were analysed by content and then categorised. In terms of research method, the studies were categorised into classes such as prospective review, retrospective review, goal-based evaluative study and criterion-based evaluative study. In order to categorise the documentation errors and deficiencies, the most common quality dimensions mentioned in the literature were used (Chen, Hailey, et al., 2014; Chen, Yu, et al., 2014; Davoudi et al., 2015; Kahn et al., 2016; Moghaddasi & Rahimi, 2016; Wager et al., 2017; Weiskopf & Weng, 2013). Additional categories were defined and then classified in order to categorise factors contributing to the emergence of errors and to present the suggested solutions for minimising document problems.
Results
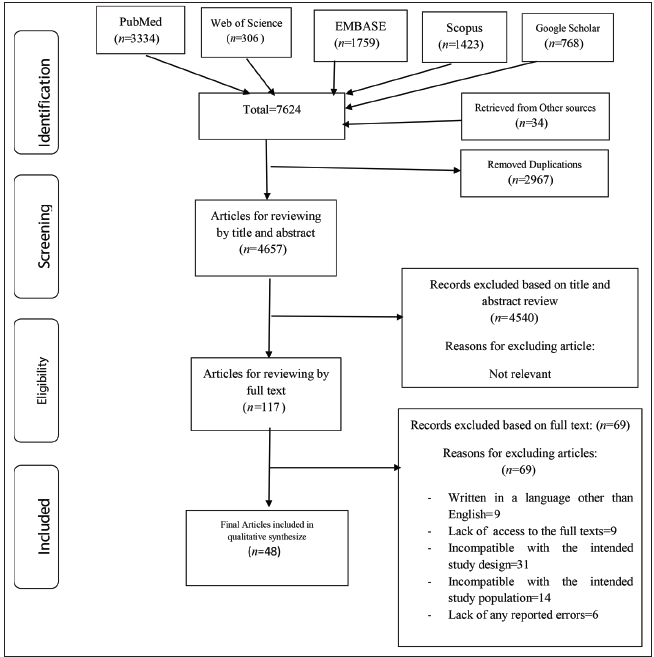
As shown in Figure 1, 7,590 articles were found based on the search strategy. Added to these were 34 additional articles found by conducting a manual search into the articles suggested in the databases and references of the eligible articles. The articles left for analysis, after removing the duplicates, were 4,657 in total. After screening this total (i.e., 4,657 articles) by title and abstract, 117 articles entered the full-text screening phase. By eliminating the unrelated articles and articles that did not meet the inclusion criteria, just 48 eligible articles were left to be analysed.
According to Table 1, showing the characteristics of the studies, 10 (out of 48) articles were conducted in the United States, six in Australia, with one in collaboration with New Zealand; three in Norway and Sweden; two in the Netherlands, Switzerland, Ireland, Iran, Canada and Jamaica; and one article in the United Kingdom, Vietnam, Iceland, Germany, Nigeria, Pakistan, Afghanistan, Finland, Ethiopia, Saudi Arabia, India, Malawi and Ghana.
Characteristics of Included Studies.

In terms of the study type, the majority of the articles derived from evaluative studies: 30 were criterion-based, nine were goal-based and one used both approaches. Five articles were comparative studies, with two of them comparing sample populations and the third comparing manual and electronic documentation. One of the comparative studies compared the current study’s audit with the audit carried out five years ago, and another conducted a before–after study and compared the results prior to and after the implementation of electronic health record (EHR). Also, 41 articles were retrospective reviews, and seven articles were prospective reviews. University hospitals, general hospitals and special hospitals were the settings where 35 articles came from; long-term facilities were the setting of four articles; and clinics, emergency centres and other ambulatory care centres were the setting of six articles. The setting of two articles was both hospitals and ambulatory centres. In one case, the patients’ medical records that were sent from the long-term care centre to the emergency department were reviewed.
The data extracted are presented in Table 2, showing documentation errors and deficiencies, factors contributing to such errors and the recommendations made.
Documentation Errors and Deficiencies, Contributing Factors and Suggested Solutions.
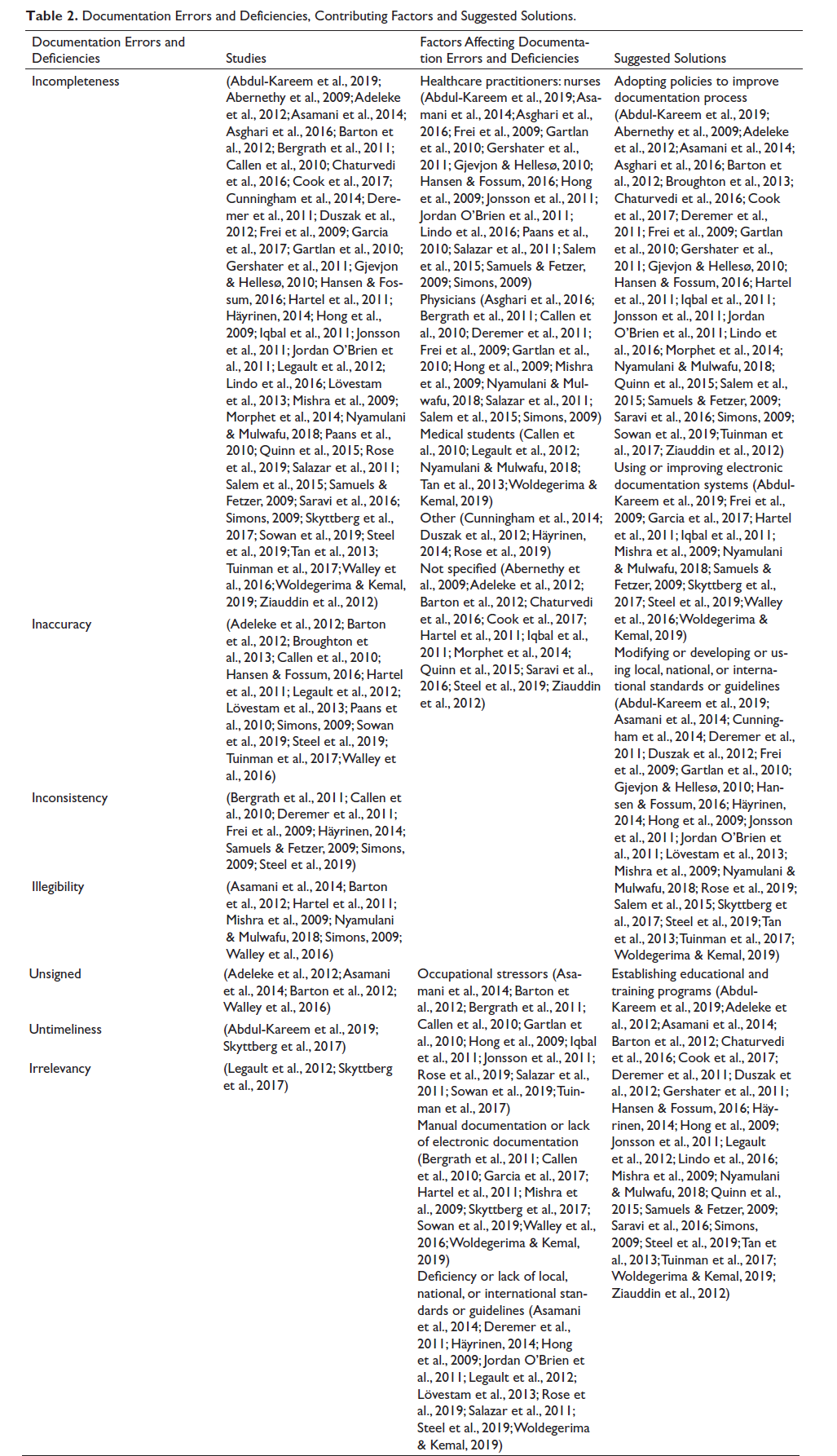
Incompleteness was present in all of the examined articles except for one (Broughton et al., 2013). A closer review of studies evaluating data adequacy and sufficiency revealed recurring issues with incomplete data. Four studies (Gershater et al., 2011; Iqbal et al., 2011; Morphet et al., 2014; Rose et al., 2019) identified gaps in healthcare service data provided to patients. Two studies (Bergrath et al., 2011; Johnson et al., 2015) found problems in calculating indices necessary for patient care, while one study (Abernethy et al., 2009) highlighted issues in computing care quality indices. Additionally, three studies (Cunningham et al., 2014; Duszak et al., 2012; Hong et al., 2009) reported coding-related challenges. In all criterion-based evaluations, data incompleteness was the most common documentation error and the main cause of the incompatibility of medical records with the intended criteria (Abdul-Kareem et al., 2019; Adeleke et al., 2012; Asamani et al., 2014; Asghari et al., 2016; Barton et al., 2012; Broughton et al., 2013; Chaturvedi et al., 2016; Deremer et al., 2011; Garcia et al., 2017; Gartlan et al., 2010; Gjevjon & Hellesø, 2010; Hansen & Fossum, 2016; Hartel et al., 2011; Häyrinen, 2014; Jordan O’Brien et al., 2011; Legault et al., 2012; Lindo et al., 2016; Lövestam et al., 2013; Mishra et al., 2009; Nyamulani & Mulwafu, 2018; Paans et al., 2010; Salazar et al., 2011; Salem et al., 2015; Samuels & Fetzer, 2009; Saravi et al., 2016; Skyttberg et al., 2017; Sowan et al., 2019; Tan et al., 2013; Tuinman et al., 2017; Woldegerima & Kemal, 2019). Inaccuracy was also reported in 14 studies (Adeleke et al., 2012; Barton et al., 2012; Broughton et al., 2013; Callen et al., 2010; Hansen & Fossum, 2016; Hartel et al., 2011; Legault et al., 2012; Lövestam et al., 2013; Paans et al., 2010; Simons, 2009; Sowan et al., 2019; Steel et al., 2019; Tuinman et al., 2017; Walley et al., 2016), inconsistency in eight (Bergrath et al., 2011; Callen et al., 2010; Deremer et al., 2011; Frei et al., 2009; Häyrinen, 2014; Samuels & Fetzer, 2009; Simons, 2009; Steel et al., 2019), illegibility in seven (Asamani et al., 2014; Barton et al., 2012; Hartel et al., 2011; Mishra et al., 2009; Nyamulani & Mulwafu, 2018; Simons, 2009; Walley et al., 2016), unsigned document in four (Adeleke et al., 2012; Asamani et al., 2014; Barton et al., 2012; Walley et al., 2016) and irrelevancy in two studies (Legault et al., 2012; Skyttberg et al., 2017).
In 17 studies, documentation errors and deficiencies were related to nurses (Abdul-Kareem et al., 2019; Asamani et al., 2014; Asghari et al., 2016; Frei et al., 2009; Gartlan et al., 2010; Gershater et al., 2011; Gjevjon & Hellesø, 2010; Hansen & Fossum, 2016; Hong et al., 2009; Jonsson et al., 2011; Jordan O’Brien et al., 2011; Lindo et al., 2016; Paans et al., 2010; Salazar et al., 2011; Salem et al., 2015; Samuels & Fetzer, 2009; Simons, 2009; Sowan et al., 2019; Tuinman et al., 2017), in 12 studies to physicians (Asghari et al., 2016; Bergrath et al., 2011; Callen et al., 2010; Deremer et al., 2011; Frei et al., 2009; Gartlan et al., 2010; Hong et al., 2009; Mishra et al., 2009; Nyamulani & Mulwafu, 2018; Salazar et al., 2011; Salem et al., 2015; Simons, 2009), in five studies to medical students (Callen et al., 2010; Legault et al., 2012; Nyamulani & Mulwafu, 2018; Tan et al., 2013; Woldegerima & Kemal, 2019), and in four studies to other members of the healthcare team (Cunningham et al., 2014; Duszak et al., 2012; Häyrinen, 2014; Rose et al., 2019), while some other studies did not mention any specific healthcare practitioner (Abernethy et al., 2009; Adeleke et al., 2012; Barton et al., 2012; Chaturvedi et al., 2016; Cook et al., 2017; Hartel et al., 2011; Iqbal et al., 2011; Morphet et al., 2014; Quinn et al., 2015; Saravi et al., 2016; Steel et al., 2019; Ziauddin et al., 2012). One study also noted the documentation errors of the patient’s previous healthcare team (nursing home).
Occupational stressors, including workload, shortage/absence of specialised human force, time limitations, shift rotations and communication problems between different units, contributed to the incidence of documentation errors and deficiencies (Asamani et al., 2014; Barton et al., 2012; Bergrath et al., 2011; Callen et al., 2010; Gartlan et al., 2010; Hong et al., 2009; Iqbal et al., 2011; Jonsson et al., 2011; Rose et al., 2019; Salazar et al., 2011; Sowan et al., 2019; Tuinman et al., 2017). Manual documentation or lack of electronic documentation were factors mentioned in these studies as influencing the incidence of documentation errors (Bergrath et al., 2011; Callen et al., 2010; Garcia et al., 2017; Hartel et al., 2011; Mishra et al., 2009; Skyttberg et al., 2017; Sowan et al., 2019; Walley et al., 2016; Woldegerima & Kemal, 2019). Absence of or a defect in local, national and international standards or guidelines was another factor predisposing those in charge of documentation to documentation errors (Asamani et al., 2014; Deremer et al., 2011; Häyrinen, 2014; Hong et al., 2009; Jordan O’Brien et al., 2011; Legault et al., 2012; Lövestam et al., 2013; Rose et al., 2019; Salazar et al., 2011; Steel et al., 2019; Woldegerima & Kemal, 2019).
The examined studies recommended adopting new policies to improve the documentation process (Abdul-Kareem et al., 2019; Abernethy et al., 2009; Adeleke et al., 2012; Asamani et al., 2014; Asghari et al., 2016; Barton et al., 2012; Broughton et al., 2013; Chaturvedi et al., 2016; Cook et al., 2017; Deremer et al., 2011; Frei et al., 2009; Gartlan et al., 2010; Gershater et al., 2011; Gjevjon & Hellesø, 2010; Hansen & Fossum, 2016; Hartel et al., 2011; Iqbal et al., 2011; Jonsson et al., 2011; Jordan O’Brien et al., 2011; Lindo et al., 2016; Morphet et al., 2014; Nyamulani & Mulwafu, 2018; Quinn et al., 2015; Salem et al., 2015; Samuels & Fetzer, 2009; Saravi et al., 2016; Simons, 2009; Sowan et al., 2019; Tuinman et al., 2017; Ziauddin et al., 2012), using electronic documentation systems or improving the existing systems (Abdul-Kareem et al., 2019; Frei et al., 2009; Garcia et al., 2017; Hartel et al., 2011; Iqbal et al., 2011; Mishra et al., 2009; Nyamulani & Mulwafu, 2018; Samuels & Fetzer, 2009; Skyttberg et al., 2017; Steel et al., 2019; Walley et al., 2016; Woldegerima & Kemal, 2019), modifying, creating, or using local, national, and international standards and guidelines (Abdul-Kareem et al., 2019; Asamani et al., 2014; Cunningham et al., 2014; Deremer et al., 2011; Duszak et al., 2012; Frei et al., 2009; Gartlan et al., 2010; Gjevjon & Hellesø, 2010; Hansen & Fossum, 2016; Häyrinen, 2014; Hong et al., 2009; Jonsson et al., 2011; Jordan O’Brien et al., 2011; Lövestam et al., 2013; Mishra et al., 2009; Nyamulani & Mulwafu, 2018; Rose et al., 2019; Salem et al., 2015; Skyttberg et al., 2017; Steel et al., 2019; Tan et al., 2013; Tuinman et al., 2017; Woldegerima & Kemal, 2019) and offering educational courses (Abdul-Kareem et al., 2019; Adeleke et al., 2012; Asamani et al., 2014; Barton et al., 2012; Chaturvedi et al., 2016; Cook et al., 2017; Deremer et al., 2011; Duszak et al., 2012; Gershater et al., 2011; Hansen & Fossum, 2016; Häyrinen, 2014; Hong et al., 2009; Jonsson et al., 2011; Legault et al., 2012; Lindo et al., 2016; Mishra et al., 2009; Nyamulani & Mulwafu, 2018; Quinn et al., 2015; Samuels & Fetzer, 2009; Saravi et al., 2016; Simons, 2009; Steel et al., 2019; Tan et al., 2013; Tuinman et al., 2017; Woldegerima & Kemal, 2019; Ziauddin et al., 2012).
Discussion
Incompleteness in medical records was detected in the majority of the articles examined in this study. Many studies have cast doubt on the generalisability of their results due to, among others, limitations in the studied population (Abernethy et al., 2009; Adeleke et al., 2012; Callen et al., 2010; Cook et al., 2017; Garcia et al., 2017; Gjevjon & Hellesø, 2010; Hansen & Fossum, 2016; Hartel et al., 2011; Legault et al., 2012; Lindo et al., 2016; Mishra et al., 2009; Quinn et al., 2015; Rose et al., 2019; Salazar et al., 2011; Salem et al., 2015; Simons, 2009; Tan et al., 2013), the retrospective review nature of the studies (Abernethy et al., 2009; Bergrath et al., 2011; Deremer et al., 2011; Duszak et al., 2012; Hartel et al., 2011; Jonsson et al., 2011; Mishra et al., 2009; Morphet et al., 2014; Salazar et al., 2011; Simons, 2009; Skyttberg et al., 2017; Sowan et al., 2019), and shortcomings in methods, data collection procedures and research instruments (Abdul-Kareem et al., 2019; Duszak et al., 2012; Frei et al., 2009; Garcia et al., 2017; Gershater et al., 2011; Hartel et al., 2011; Häyrinen, 2014; Jordan O’Brien et al., 2011; Legault et al., 2012; Mishra et al., 2009; Tuinman et al., 2017). Yet, incomplete documentation is doubtless a major problem in the patient medical record documentation process (Asakura et al., 2014). Lack/absence of documentation, insufficient documentation in justifying the need for the delivered healthcare services, incorrect coding and other errors are the main error categories of the CERT program cited by The Centers for Medicare & Medicaid Services (2016). According to Karp et al. (2008), many lawsuits related to medical errors were lost due to the low quality of medical records, insufficiency of data and indefensibility of the records, even when appropriate healthcare services have been offered to the patient. Edwards believes that ‘better documentation can reduce medical errors’ (Edwards & Moczygemba, 2004).
Unsigned document and unspecified identification of the healthcare provider, observed in four studies, may be due to the healthcare providers’ reluctance to take full responsibility for care (Adeleke et al., 2012). Still, they pose major problems for healthcare service organisations and teams. In an examination developed by the Centers for Medicare & Medicaid Services, unreliable medical records, due to lack of necessary signatures or illegible signatures and incomplete medical records, were the most important documentation errors leading to loss of payment lawsuits (The Medicare Learning Network, 2017). Illegibility of the contents of the medical records, especially the illegibility of doctors’ handwriting, could also contribute to the incidence of medical errors (Edwards & Moczygemba, 2004). Edwards believes that diagnosing and ordering errors can be caused by unavailable patient healthcare data and illegible handwriting (Edwards & Moczygemba, 2004).
Identification of incompleteness, illegibility and unsigned documentation requires quantitative analyses. Since some errors related to incompleteness, illegibility and unsigned documentation can be resolved, it seems that simultaneous quantitative analyses may help in the timely identification of these errors, thereby improving the patient’s medical records and preventing unfavourable outcomes (Abdelhak et al., 2007; Huffman, 1994; Moghaddasi, 2005; Skurka, 1998; World Health Organization, 2003).
Clarity and accuracy have the highest degree of importance for effective communication between healthcare team members and patients (Abdelrahman & Abdelmageed, 2014). Therefore, the accuracy of medical record data in any healthcare centre is a necessity for the provision of care to patients (Lindh et al., 2013). As a result, the inaccuracy reported in 14 studies disrupted effective communication between healthcare teams, thereby threatening the process of patient care. The inconsistency reported in eight articles demonstrates heterogeneity in data. Documentation errors such as inaccuracy, inconsistency and irrelevancy can be identified in the process of medical record qualitative analysis but cannot always be resolved, especially because qualitative analysis is often performed after quantitative analysis and in a retrospective manner (Abdelhak et al., 2007; Huffman, 1994; Moghaddasi, 2005; Skurka, 1998).
According to Ross Koppel, 70% of medical records contain errors (Farr, 2018). Errors in medical records may lead to medical errors (Adane et al., 2019). Lack of recording or erroneous recording of necessary data in medical records can have adverse consequences, especially if this leads to an inaccurate diagnosis or inappropriate treatment plan (Lippincott Nursing Education, 2018). Many common medical documentation errors may be disastrous, sometimes leading to patient mortality. Poor documentation may affect budget distribution, epidemiological variables, research and research investment, communication among the healthcare team members, care quality evaluation, ranking of hospitals, services, and individuals, and even hospital bills (Asakura et al., 2014). Therefore, it is essential to identify factors contributing to documentation errors.
Human factors are important factors in the incidence of medical errors (Rodziewicz & Hipskind, 2019). In some of the examined studies, documentation errors were the result of a lack of knowledge and awareness (Barton et al., 2012; Deremer et al., 2011; Hong et al., 2009), low priority in the documentation (Bergrath et al., 2011; Gartlan et al., 2010), evasion of responsibility (Adeleke et al., 2012) and lack of physical well-being of the person in charge of documentation (Callen et al., 2010). However, one must not overlook the share of difficulties related to systems and processes in providing the conditions for documentation errors.
Manual documentation and absence of electronic documentation systems (Bergrath et al., 2011; Callen et al., 2010; Garcia et al., 2017; Hartel et al., 2011; Mishra et al., 2009; Skyttberg et al., 2017; Sowan et al., 2019; Walley et al., 2016; Woldegerima & Kemal, 2019), absence, deficiency or non-use of standards and guidelines (Asamani et al., 2014; Deremer et al., 2011; Häyrinen, 2014; Hong et al., 2009; Jordan O’Brien et al., 2011; Legault et al., 2012; Lövestam et al., 2013; Rose et al., 2019; Salazar et al., 2011; Steel et al., 2019; Woldegerima & Kemal, 2019), and factors such as workload, shortage of or absence of specialised human force, with time limitations (Asamani et al., 2014; Barton et al., 2012; Bergrath et al., 2011; Callen et al., 2010; Hong et al., 2009; Jonsson et al., 2011; Rose et al., 2019; Salazar et al., 2011; Sowan et al., 2019; Woldegerima & Kemal, 2019), shift rotations (Tuinman et al., 2017) and lack of effective communication between different units (Gartlan et al., 2010) are referred to in some of the reviewed articles as factors influencing the incidence of documentation errors. These factors could lead not only to documentation errors but also medical errors if they are not identified and controlled. Therefore, given the effectiveness of Root Causes Analysis tool in the prevention of medical errors (Charles et al., 2016, 2017), this tool can also be used in the case of documentation errors in order to identify the causes of errors and find solutions to resolve these problems.
Calculated policy-making and modification of processes for improving medical record documentation at both small and large scale are solutions recommended by many studied articles (Abdul-Kareem et al., 2019; Abernethy et al., 2009; Adeleke et al., 2012; Asamani et al., 2014; Asghari et al., 2016; Barton et al., 2012; Broughton et al., 2013; Chaturvedi et al., 2016; Cook et al., 2017; Deremer et al., 2011; Frei et al., 2009; Gartlan et al., 2010; Gershater et al., 2011; Gjevjon & Hellesø, 2010; Hansen & Fossum, 2016; Hartel et al., 2011; Iqbal et al., 2011; Jonsson et al., 2011; Jordan O’Brien et al., 2011; Lindo et al., 2016; Morphet et al., 2014; Nyamulani & Mulwafu, 2018; Quinn et al., 2015; Salem et al., 2015; Samuels & Fetzer, 2009; Saravi et al., 2016; Simons, 2009; Sowan et al., 2019; Tuinman et al., 2017; Ziauddin et al., 2012). Using electronic documentation systems (Abdul-Kareem et al., 2019; Frei et al., 2009; Garcia et al., 2017; Hartel et al., 2011; Iqbal et al., 2011; Mishra et al., 2009; Nyamulani & Mulwafu, 2018; Samuels & Fetzer, 2009; Skyttberg et al., 2017; Steel et al., 2019; Walley et al., 2016; Woldegerima & Kemal, 2019) or upgrading the existing systems (Bergrath et al., 2011; Callen et al., 2010; Deremer et al., 2011; Häyrinen, 2014; Paans et al., 2010; Salazar et al., 2011; Simons, 2009; Sowan et al., 2019; Tuinman et al., 2017) are some other solutions proposed in these studies. In a review study, Adane concluded that poor medical data processing systems are the main cause of medical errors (Adane et al., 2019). Edwards believes using integrated computer-based medical records can lead to better documentation and, consequently, reduce medical errors (Edwards & Moczygemba, 2004).
However, as also noted by Frie and Mishra, the use of electronic documentation systems alone is not sufficient for preventing documentation errors (Frei et al., 2009; Mishra et al., 2009). Human force empowerment through education and enhancement of the knowledge and awareness of those in charge of medical documentation can greatly reduce documentation errors (Abdul-Kareem et al., 2019; Adeleke et al., 2012; Asamani et al., 2014; Barton et al., 2012; Chaturvedi et al., 2016; Cook et al., 2017; Deremer et al., 2011; Duszak et al., 2012; Gershater et al., 2011; Hansen & Fossum, 2016; Häyrinen, 2014; Hong et al., 2009; Jonsson et al., 2011; Legault et al., 2012; Lindo et al., 2016; Mishra et al., 2009; Nyamulani & Mulwafu, 2018; Quinn et al., 2015; Samuels & Fetzer, 2009; Saravi et al., 2016; Simons, 2009; Steel et al., 2019; Tan et al., 2013; Tuinman et al., 2017; Woldegerima & Kemal, 2019; Ziauddin et al., 2012). Moreover, development, modification or use of standards or guidelines at a local, national or international scale is another solution that may help prevent documentation errors (Abdul-Kareem et al., 2019; Asamani et al., 2014; Cunningham et al., 2014; Deremer et al., 2011; Duszak et al., 2012; Frei et al., 2009; Gartlan et al., 2010; Gjevjon & Hellesø, 2010; Hansen & Fossum, 2016; Häyrinen, 2014; Hong et al., 2009; Jonsson et al., 2011; Jordan O’Brien et al., 2011; Lövestam et al., 2013; Mishra et al., 2009; Nyamulani & Mulwafu, 2018; Paans et al., 2010; Rose et al., 2019; Salem et al., 2015; Skyttberg et al., 2017; Steel et al., 2019; Tan et al., 2013; Tuinman et al., 2017; Woldegerima & Kemal, 2019).
Conclusion
Documentation errors and deficiencies, especially those that have not been resolved or modified, always threaten the process of healthcare service provision to patients and, consequently, the health of individuals and society. Thus, it is necessary to identify and resolve underlying factors contributing to these errors and empower the human force. To this end, measures such as the adoption of policies for improving documentation at a small and large scale, movement towards electronic documentation equipped with automatic error detection systems and standardisation of the documentation process can be of great assistance.
Appendix
Search Strategies
Author Contributions
A. SH. was responsible for the study design, literature search, data extraction, quality assessment of the selected articles and manuscript preparation.
H. M. and F. A. were responsible for the study design, critically reviewing the manuscript, participating in screening the articles and assessing the quality of the selected articles.
A. H. contributed to assessing the quality of the selected articles and critically reviewing the manuscript.
F. A. was responsible for whole correspondence during the paper submission, handling the revisions and resubmission.
Footnotes
Acknowledgement
The current research has been approved by the ethics committee of Shahid Beheshti University of Medical Sciences (ethics code: IR.SBMU.RETECH.REC.1397.708).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.