
Abstract
Background
Carpal Tunnel Syndrome (CTS) is the most common entrapment neuropathy, characterised by compression of the median nerve at the wrist. Traditional understanding views CTS as a distal compression issue, but recent evidence suggests potential proximal involvement.
Purpose
This study aimed to assess the prevalence of proximal median nerve conduction velocity (CV) slowing in CTS patients and examine its association with CTS severity.
Methods
In this retrospective observational study, data were analysed from 80 CTS patients and 40 controls from the Electrophysiology Lab at a tertiary care institute. Nerve conduction studies (NCS) evaluated the median nerve’s conduction velocity and latency. Patients were classified by CTS severity, and nerve conduction parameters were statistically compared between groups.
Results
CTS patients exhibited significantly prolonged distal motor latency (DML) (5.2 ± 0.8 ms) and reduced forearm motor conduction velocity (MCV) (55.3 ± 4.1 m/s) compared to controls (P < .01). Approximately 27.45% of CTS hands showed proximal median nerve slowing. The severity classification showed that Grade 3 CTS was the most prevalent (47%), followed by Grade 2 (23%) and Grade 1 (10%). There was a negative correlation between distal latency and forearm conduction velocity, suggesting that as distal latency increases, forearm conduction velocity decreases. Post-operatively, significant improvements were observed in distal latency (mean decrease: 1.2 ± 0.5 ms, P < .01), but median nerve conduction velocity remained unchanged. While there was a trend towards improvement in CMAP amplitude, the difference did not reach statistical significance.
Conclusion
A subset of CTS cases exhibits reduced proximal median nerve conduction velocity, which correlates with CTS severity. This suggests retrograde degeneration may contribute to CTS pathology, challenging the traditional view of CTS as a purely distal compression disorder.
Keywords
Introduction
The symptoms of carpal tunnel syndrome (CTS) are associated with median nerve compression at the wrist. It is the most prevalent type of entrapment neuropathy. 1 Typically, symptoms manifest gradually, beginning with recurrent burning, tingling, and/or numbness in the palm of the hand and fingers, particularly the thumb, index, and middle fingers. A person with CTS may awaken with the desire to shake out their hand or wrist. As symptoms progress, individuals may experience tingling during the day. It may be difficult to create a fist, grab small objects, or execute other manual tasks if grip strength is diminished. Clinical exam reveals hypoesthesia of median nerve distribution in the hand, wasting of the thenar eminence, and/or weakening of thumb abduction and/or opposition. In the diagnosis of CTS, a positive Phalen’s test and Tinel’s sign are also essential.2–4
Although it is known that the area most affected by segmental compression of peripheral nerves is the area directly under the site of compression, followed by the distal segment of the peripheral nerve through Wallerian degeneration proportional to the duration and severity of compression, it was discovered that in the proximal segment there is slowed conduction velocity.5, 6 Retrograde degeneration of the median nerve in CTS has shown pathophysiological alterations affecting the median nerve proximal to the carpal tunnel compression site. 7 Weiss and Hiscoe in their experiment discovered that nerve constriction signals swelling and fluid collection in the region proximal to the injury site. They assert that this is caused by a blockage of the axoplasm within the nerve fibre. Some median nerve fibres in the forearm exhibited irreversible atrophic alterations following the discharge of noxious substances.5, 6
But one study reported that the neurological impairment is confined to the area within the wrist to palm segment in patients with CTS due to compression by the transverse carpel ligament to disease process of terminal segment. 8 Another study reported that there was no association between retrograde degeneration (using median motor NCV of the forearm segment and the forearm median mixed amplitude) and CTS severity. 9 Standard electrodiagnostic testing in individuals with carpal tunnel syndrome (CTS) demonstrate pathophysiological alterations in the median nerve at and below the wrist, with reductions in nerve conduction velocity.5, 10, 11
However, there was no consensus in the scientific literature about the proximal median nerve involvement (conduction velocity slowing) among CTS patients. The present study provides details about the prevalence of proximal median nerve changes to the site of compression in CTS and evaluates whether the change in the proximal median nerve is associated with CTS severity.
Thus, the present study was undertaken to present the proximal median nerve conduction slowing (if any) in CTS patients and to associate proximal median nerve conduction velocity with severity of CTS.
Methods
Study Design
This study is a retrospective observational analysis conducted to evaluate the prevalence of proximal nerve conduction slowing in patients with carpal tunnel syndrome (CTS) and its association with CTS severity. The study commenced after obtaining approval from the Institute Research Committee and the Institute Ethical Committee for Human Studies (AIIMS/MG/IEC/2022-23/246). Participants were contacted via telephone, and the study protocol was explained to them. Those who returned to the hospital for various reasons and resided in close proximity to the hospital provided a written consent.
Study Setting
Data for this study were collected from the Electrophysiology Lab, Department of Physiology, at a tertiary care institute in Andhra Pradesh, India. The study period spanned from March 12, 2020, to October 26, 2022.
Study Population
The study population comprised both male and female patients aged between 18 and 50 years, diagnosed with CTS based on clinical criteria according to the American Academy of Neurology guidelines, and confirmed through electrophysiological findings in the Electrophysiology Lab, Department of Physiology. Individuals with conditions suggestive of cervical radiculopathy (C6, C7, and C8), brachial plexopathy or proximal median neuropathy, as well as those with motor neuron disease, previous hand surgeries, spondylotic neuropathy, syringomyelia, stroke, multiple sclerosis, polyneuropathy or diabetes, were excluded from the study, even if they met the clinical criteria for CTS. A total of 253 subjects of both genders who exhibited symptoms suggestive of CTS were initially considered for the study. After applying specific inclusion and exclusion criteria, the number of eligible subjects was reduced to 132. From this group, 80 subjects (57 males and 23 females) consented to participate in the study. These 80 subjects accounted for a total of 102 hands diagnosed with CTS, indicating that some participants had bilateral CTS (n=22). Unilateral CTS cases were predominantly observed in the dominant hand. This retrospective study also included a control group, with data collected from the department laboratory.
The control group comprised 40 individuals (20 males and 20 females) aged between 18 and 40 years, contributing a total of 80 hands (both hands from each participant). Inclusion criteria for the control group included individuals who were apparently healthy, without any known metabolic or chronic diseases, and with no sensory or motor complaints in the upper limbs. These participants were carefully screened to ensure they did not exhibit any clinical or electrophysiological signs of carpal tunnel syndrome or other peripheral neuropathies. This control group served as the basis for comparison in the study.
Nerve Conduction Technique
For the motor conduction study, an active electrode was placed over the middle portion of the abductor pollicis brevis (APB) muscle, and stimulation was applied at two standardised sites: the wrist (8 cm proximal to the active electrode) and the elbow (medial aspect of the antecubital fossa near the brachial artery). 12 Supramaximal stimulation was delivered to elicit the compound muscle action potential (CMAP). The onset latency, CMAP amplitude, and conduction velocity were measured and recorded. Skin temperature was maintained at ≥32°C to ensure the accuracy and reliability of the results. The study was conducted using a 2-channel nerve conduction machine (Model: Aleron, Make: RMS, Recorders and Medicare Systems, India). Same technique was used for all the subjects.
Data Collection
Data were retrospectively collected from patient medical records, including demographics (age, gender) and detailed electrophysiological findings. The electrophysiological assessment of CTS involved nerve conduction studies (NCS) to measure conduction velocity and latency in the median nerve. These studies included sensory nerve conduction velocity (SNCV) and sensory latency measurements, as well as motor nerve conduction velocity (MNCV) and motor latency measurements. Patients were categorised into three grades of CTS severity based on Mackinnon’s classification 13 : (a) Mild, characterised by sensory symptoms such as pain, paresthesias and/or numbness; (b) Moderate, marked by motor symptoms like weakness and (c) Severe, indicated by muscle wasting. All tests were conducted in the Electrophysiology Lab by the principal investigator (PI) and co-principal investigator (Co-PI) during outpatient department (OPD) postings, using standardised procedures.
Statistical Analysis
All data were analysed using IBM SPSS Statistics for Windows (version 26, IBM Corp). The data were tested for normality. Qualitative variables such as CTS grade distribution are presented as frequencies and percentages. Quantitative variables, including nerve conduction parameters, are presented as Mean ± SD or Median (Interquartile Range), depending on the data distribution. A Student’s t-test was used to compare parameters between the two groups (control vs. CTS), and a one-way ANOVA was performed to compare parameters of the three groups (control vs. CTS with proximal median nerve conduction velocity slowing vs. CTS without proximal median nerve conduction velocity slowing), followed by an LSD post hoc test. Pearson correlation was carried out to determine the association between distal latency and forearm median conduction velocity.
Results
Distribution of CTS Severity Classification
The most prevalent severity level is Grade 3, constituting 47% of cases, indicating a significant portion of participants experience severe CTS symptoms. Following this, Grade 2 represents 23% of the cases, while Grade 1 comprises 10%. Notably, Grade 0, representing the absence of CTS, accounts for only 2% of the participants. Table 1 shows comparison of distal motor latency (DML) and forearm motor conduction velocity (MCV) between the control group (n=80) and the CTS group (n=102). The CTS group had a significantly longer DML compared to the control group. Additionally, the CTS group exhibited a significantly lower MCV compared to the control group. These findings indicate delayed motor response and reduced conduction velocity in individuals with CTS. Table 2 reveals that the median nerve CMAP amplitude is decreased in the following order. Control group median nerve CMAP> CTS without slowing > CTS with slowing group.
Comparison of Distal Motor Latency and Forearm Motor Conduction Velocity between Control Group and Carpal Tunnel Syndrome (CTS) Group.

Comparison was done using unpaired student t test. P < .05 is considered statistically significant.
Comparison of Median Nerve CMAP Amplitude Between Control, CTS with Proximal Median Slowing and CTS Without Median Slowing.

Pre-operatively, patients with CTS exhibited a mean distal latency of 5.2 ± 0.8 ms, a mean CMAP amplitude of 8.5 ± 1.2 mV, and a mean forearm median CV of 55.3 ± 4.1 m/s. Post-operatively, there was a significant improvement in distal latency with a mean decrease of 1.2 ± 0.5 ms (P < .01). While there was a trend towards improvement in CMAP amplitude, the difference did not reach statistical significance. No significant changes were observed in the forearm median CV.
Figure 1 shows the relationship between distal latency and forearm nerve conduction velocity. A negative correlation is apparent, suggesting that as distal latency increases, indicating slower nerve conduction, the forearm nerve conduction velocity tends to decrease.
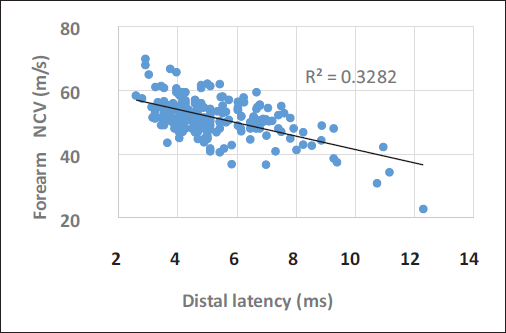
Pearson correlation was used to assess the relationship. P < .005 is considered to be statistically significant.
Discussion
The objective of our study was to assess forearm median CV in CTS patients compared to controls, observing whether there was evidence of proximal median nerve conduction velocity slowing. In this study, the CTS group exhibited a significantly prolonged DML and reduced MCV, underscoring the impact of median nerve compression at the wrist on nerve conduction properties. Buchthal et al. 5 observed that only 2% of patients with carpal tunnel syndrome (CTS) exhibited slowing of conduction from the wrist to the elbow, which was attributed to the high number of cases with mild to moderate CTS in their study. 5 However, in our study, we found that 27.45% of hands showed proximal median nerve slowing. According to our normative data, a conduction velocity below 49 m/sec is deemed abnormal. 13 In our sample, 28 hands out of 102 had conduction velocities below this threshold.
The question arises as to why proximal slowing (i.e., decreased conduction velocity at the level of forearm) occurs when the primary site of compression is distal, at the carpal tunnel. One possible explanation is conduction block, which happens when demyelination is extensive, which can occur at the level of the carpal tunnel during compression.14, 15 In such cases, signals may not only be delayed but also blocked, resulting primarily in decreased CMAP amplitude. Further, the conduction velocity can also be decreased because the motor conduction velocity measurement is indirect in routine studies. The possible explanation is that when nerve compression occurs, as in CTS, the larger fibres are more vulnerable to damage, leaving only the slower-conducting small fibres functional.16–18 As a result, irrespective of the stimulation site, the slow-conducting fibres dominate since the large fibres are compromised, resulting in decreased forearm proximal conduction velocity.
Based on this hypothesis, the decrease in forearm conduction velocity should correlate well with the severity of carpal tunnel syndrome (CTS). Similarly, we observed forearm median conduction velocity slowing with reduced median nerve CMAP amplitude compared to the other two groups (CTS without slowing and control), which is attributed to the loss of nerve fibres. In support of our findings, a previous study has reported that the median forearm NCV reflected chronological changes in retrograde demyelination of the median nerve and that these changes correlated with the clinical severity of CTS. 19
A few studies have argued that the decrease observed in conduction velocity could be primarily due to the indirect method of calculation of CV, and they have employed retrograde mixed nerve conduction study, stimulating at the wrist and recording at the level of the elbow, and observed no reduction in forearm conduction velocity. While others have challenged this hypothesis, stating that a few of the median nerve branches traverse above the carpal tunnel, and during retrograde study, the unaffected nerve fibres traversing above the carpal tunnel could have resulted in normal conduction velocity in the forearm. However, in the present study, we did not perform a retrograde study for CTS. Thus, examining the impact of this approach on our findings is beyond the scope of this article.
In support of the conduction block hypothesis, we observed that CMAP amplitude was decreased in CTS patients with proximal slowing compared to CTS patients without proximal slowing (Table 2). However, among those with slowed conduction, only 12 participants showed a reduction in amplitude, while 16 did not, raising questions about the presence of a true conduction block. If the conduction block is removed, as during surgical relief for CTS, it could shed light on the effect of compression on the nerve conduction parameters.
In our study, seven participants (12 hands) underwent surgical intervention for CTS. Following surgical intervention, improvements were noted: distal latency was corrected, and amplitude increased (Table 3). Despite these changes, the median nerve conduction velocity remained unchanged. This observation suggests that the decrease in distal latency and amplitude may be linked to decreased conduction velocity rather than conduction block. A plausible explanation for the unchanged conduction velocity could be retrograde axonal degeneration and axonal loss, 20 which might have contributed to the observed proximal slowing of the median nerve. This indicates that while distal issues were addressed surgically, underlying proximal nerve pathology due to retrograde degeneration may persist.
Comparison of Pre- and Post-Surgery Median Nerve Motor Conduction Study.
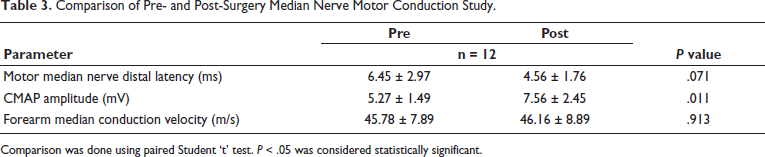
Comparison was done using paired Student ‘t’ test. P < .05 was considered statistically significant.
However, we have not done neuromuscular ultrasound to verify the retrograde axonal degeneration, which would be a logical extension of our study. Our study is limited by its relatively small sample size, which restricts the generalisability of our findings and necessitates larger studies to confirm our observations and provide more robust data. Further, future research should investigate the underlying mechanisms and reasons for retrograde degeneration of the forearm median nerve in a subset of CTS patients. Additionally, exploring the potential reversibility of this degeneration could enhance treatment strategies, providing a broader understanding of therapeutic outcomes.
Conclusion
Forearm median nerve conduction velocity (CV) is decreased in a subset of Carpal Tunnel Syndrome (CTS) cases, correlating with the severity of the condition. The primary cause for this decrease in forearm median nerve CV appears to be retrograde degeneration (axonal atrophy), with conduction block being a secondary factor. This finding challenges the traditional understanding of CTS, which typically focuses on distal compression at the carpal tunnel.
Footnotes
Acknowledgements
We thank all the participants for their cooperation during the study period.
Authors’ Contribution
Dr Senthil Kumar Subramanian, Associate Professor, Department of Physiology, AIIMS, Madurai, Tamil Nadu, India, and Dr Rajathi Rajendran, Assistant Professor, Department of Physiology, AIIMS, Bathinda, Punjab, India, contributed equally to the study’s conceptualisation, methodology design, supervision, data analysis, and manuscript preparation.
Statement of Ethics
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee (IEC) at AIIMS.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Informed Consent
All participants provided informed consent prior to their inclusion in the study, and their confidentiality and anonymity were strictly maintained.
ICMJE Statement
All authors meet the ICMJE criteria for authorship by contributing substantially to the study’s conception, design, data acquisition, analysis, and interpretation. Both authors were involved in drafting and revising the manuscript, have approved the final version, and agree to be accountable for all aspects of the work to ensure integrity and accuracy.