
Abstract
Background
Stroke survivors typically exhibit sensory and motor deficits, variations in tone and postural dysfunction, which hamper important functional abilities like rising from bed. Research highlights the importance of postural control and balance with such transitions. However, limited research explores the relationship between rise from bed time and quality with trunk control and balance among stroke patients.
Purpose
The aim of this study was to find the correlation of supine-to-stand transition time and quality of bed rise with trunk control and balance among post-stroke patients.
Methods
Fifty-two post-stroke survivors who were able to rise from supine-to-standing independently participated in this cross-sectional study. Supine-to-stand time was recorded using a stopwatch, bed rise quality was assessed using Bed Rise Difficulty Scale (BRDS), trunk control using Trunk Impairment Scale (TIS) and balance using Berg Balance Scale (BBS). The strength of correlation was calculated using Karl Pearson’s correlation coefficient.
Results
Among left hemiparetic participants, a moderate negative correlation was observed between supine-to-stand time and balance. Supine-to-stand time towards the paretic side moderately correlated with trunk control (r = −0.433, p = .013). Bed rise quality and balance showed a moderate negative correlation, irrespective of the side of rising. While rising towards the non-paretic side, the bed rise quality revealed a strong negative correlation with trunk control (r = −0.611, p < .001). For right hemiparetic participants, supine-to-stand time towards the paretic side strongly correlated with balance (r = −0.651, p = .002). Bed rise quality towards the non-paretic side showed a strong correlation with balance (r = −0.653, p = .002).
Conclusion
Post-stroke survivors who took a prolonged time to transition from supine-to-stand and demonstrated poor bed rise quality exhibited reduced trunk control and balance.
Introduction
The central nervous system functions to coordinate movements and postures while keeping the body stable during self-initiated motions. 1 Commonly seen dysfunctions in stroke are impaired motor and sensory function, tone abnormality, perceptual deficits and cognitive limitations. 2 The residual neurological deficits seen in about two-thirds of the stroke survivors 3 lead to disabilities that impair their functions and limit their ability to carry out basic functional activities such as sit-to-stand, standing and walking.4–6
Stroke survivors often exhibit decreased muscle power, loss of coordination, insufficient trunk and limb control, poor alignment and asymmetrical limb loading. These factors impede their functional abilities including bed mobility, sit-to-stand transition and walking.7–9 Trunk control is a complex and dynamic neuromuscular function, and is considered an essential component of postural control. 7 Sub-acute stroke patients, due to impaired trunk control experience prolonged trunk flexion and extension phases, resulting in a longer time to perform sit-to-stand task. 10 The lower trunk and pelvis are crucial for maintaining balance, particularly during standing and many functional mobility tasks during daily activities. 11 Studies have shown that trunk performance is positively correlated with functional ability, balance and gait.12–14 Similarly, task-oriented core activation exercises in sitting have shown to improve trunk control, balance and daily activities in chronic stroke survivors. 15
Rolling and getting out of bed are considered to be the basic movements for the activities of daily living (ADLs) and have been associated with functional improvements.16, 17 The ability to perform supine-to-stand transition is essential to prevent falls and its related complications, ensuring safe transitions. 18 However, stroke survivors typically struggle to get out of bed due to motor weakness, sensory dysfunction, tonal variations and impaired postural adjustments and movement synergies, compromising normal motor strategies, leading to variability in bed rise.17, 19 Bed Rise Difficulty Scale (BRDS) was developed to analyse and describe the movement patterns used by older adults that characterise difficulty in rising from bed. 20 Stroke survivors typically demonstrate multiple push patterns, grasp and push patterns in the arm and asymmetrical lifting of the leg patterns, 21 which are similar to the components used in BRDS. BRDS has also been proven to be a reliable tool to assess bed rise difficulty among post-stroke survivors. 22 Using BRDS, we emphasise on the importance of bed rise quality, as it is an important activity of functional independence.
Previous research has highlighted that the supine-to-stand transition patterns differ between healthy individuals and hemiplegic patients, with the transition time being significantly longer for stroke survivors. 21 The time taken to rise from bed has been correlated with the strength of rectus abdominus, trunk flexibility, sitting balance and ADLs in the older population.23, 24 Supine-to-stand time has also been used as one of the measures to evaluate the basic functional activities among patients with Parkinson’s disease. 25 Additionally, independence in rising from bed and the time taken to perform this task have been associated with improved functioning and ADLs in stroke survivors. 17
Balance impairments impact around 80% of stroke survivors. 26 These impairments result from changes in sensory and motor control, leading to decreased postural stability, dynamic standing balance and weight-bearing symmetry.27, 28 Balance has also been independently associated with the performance of the Five-Times-Sit-To-Stand test. 29 Furthermore, balance ability among post-stroke survivors has been closely related to functional capacity and may serve as a useful predictor of functional outcome. 30 Early sit-to-stand training has also been shown to enhance strength, balance and ADLs in stroke patients. 31 While previous studies have primarily focused on the relationship between sit-to-stand performance and balance, our study aimed to explore the correlation between the more complex supine-to-stand ability and balance.
Predicting functional recovery in the acute stage post-stroke plays a crucial role in successful rehabilitation. 32 Trunk control and postural balance in recumbent, sitting and standing positions have been shown to have predictive validity on functional outcomes in stroke survivors. 12 Impaired trunk control is also known to reduce the ability of maintaining a stable centre of gravity, which compromises gait and overall mobility in stroke survivors. 33 Supine-to-stand transition and bed rise movement, despite its functional importance, is an understudied area in stroke rehabilitation. Though several studies have explored the relationship between sit-to-stand movement, trunk control and balance,10, 29, 31 limited literature exists on the correlation of supine-to-stand transition as a whole and the movement quality or variations with trunk control and balance. This literature gap highlights the need for further research to improve clinical assessment in post-stroke patients. Hence, this study aims to find the correlation of supine-to-stand transition time and quality of bed rise with trunk control and balance among post-stroke patients.
Methods
This cross-sectional study was carried out from December 2016 to April 2018 in a tertiary care hospital in Mangalore. The sample size was estimated to be 52 with the assumed correlation coefficient of 0.6, 95% confidence interval, 90% power and 10% non-response error.
The Scientific Committee and Institutional Ethics Committee of Kasturba Medical College, Mangalore accepted the study protocol (IEC KMC MLR 11-16/293). Stroke patients referred by neurologists and physicians to the physiotherapy department were approached. The purpose of the study was explained to willing patients, who then signed an informed consent form. They were subsequently screened for inclusion and exclusion criteria, and demographic data was collected from eligible participants.
The inclusion criteria were single-episode stroke, Montreal Cognitive Assessment (MoCA) 34 score of ≥ 26, independent supine-to-standing transition and ability to maintain standing for 30 seconds. Individuals with a history of any musculoskeletal, cardiopulmonary or other neurological conditions that could have an impact on the study’s findings were excluded from the study. Following the screening for inclusion and exclusion criteria, using a convenient sampling method, 52 eligible post-stroke survivors were enrolled in the current study. A strengthening the reporting of observational studies in epidemiology (STROBE) flowchart of the participants is presented in Figure 1.
STROBE Flowchart of the Participants.

The principal investigator followed standard protocols for the outcome measurements (supine-to-stand time, BRDS, BBS and Trunk Impairment Scale (TIS)). To reduce potential bias and carryover effects between the outcome measures, the order of the assessment was randomised for each patient using simple randomisation technique with chit method. A camera mounted on a tripod placed at a distance 3 meters away from the side of a standard plinth was used to film the video of the supine-to-stand transition. Each participant was told to recline supine on the plinth, with the arms at their side and head in neutral. The direction of rising (towards the paretic or non-paretic side) was randomised using coin-toss method to minimise the influence of one side’s transition over the other. Each participant was asked to rise from the plinth and come to an erect sitting (towards the right/left side) with legs by the side of the bed, in a manner he/she was comfortable. They were then asked to move into a standing position promptly, ensuring their feet made contact with the ground before standing fully upright. The supine-to-standing transition towards the paretic and non-paretic sides of the bed was recorded individually by adjusting the head position on the plinth. The captured video was utilised to evaluate the bed rise quality towards the paretic and non-paretic side. For clear understanding, two practice trials were provided and the reading from the third trial was used for data analysis. The transition time for supine-to-standing was recorded using a stopwatch.
Measurements
Bed Rise Difficulty Scale
Difficulty in rising from bed was assessed using BRDS. BRDS has 12 components with scores ranging from 0 to 30, with 0 signifying no dependency and 30 signifying complete dependency to rise from bed. It has proved to be a reliable tool to assess bed rise difficulty in stroke patients with a good inter-rater reliability (Intraclass Correlation Coefficient [ICC]= 0.83). 22
Berg Balance Scale
Balance ability was measured using BBS. It is a 14-item performance-based test consisting of common movement tasks. The scores range from 0 to 56, with higher scores indicating greater independence. Excellent internal consistency (Cronbach’s alpha = 0.92–0.98), inter-rater reliability (ICC = 0.95–0.98), intrarater reliability (ICC = 0.97) and test–retest reliability (ICC = 0.98) have been reported with stroke survivors. 35
Trunk Impairment Scale
Trunk control was measured using TIS. TIS evaluates static and dynamic sitting balance and coordination of trunk movements. The scores range from 0 to 23, with higher scores indicating better trunk stability. Good test/retest (ICC = 0.96) and inter-observer reliability (ICC = 0.99) have been reported for TIS with stroke survivors. 36
Data Analysis
The collected data were analysed using IBM SPSS for Windows, Version 25.0 (IBM Corp, Armonk, NY). The data distribution was assessed using the Kolmogorov–Smirnov test for normality, which indicated no significant deviations from a normal distribution. Continuous variables were summarised as mean, standard deviation, median and interquartile range (IQR). Mann–Whitney U test was performed to compare differences between groups. Categorical variables were summarised as frequency tables. Correlations were done by Karl Pearson’s correlation coefficient. Correlation coefficients were generated and graded based on the previous literature. 37 A p value of less than .05 was considered statistically significant.
Results
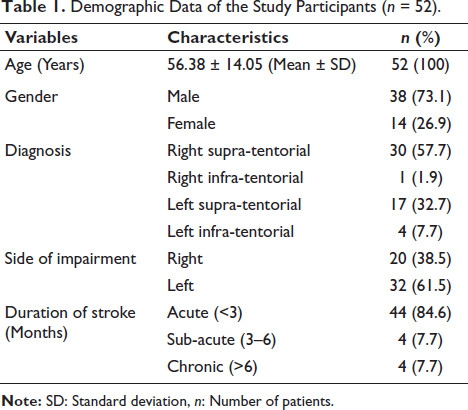
Fifty-two post-stroke survivors participated in the study, of which 38 were male and 14 were female. The mean age of the participants was 56.38 years ± 14.05 years. Among them, 30 patients were diagnosed with supra-tentorial stroke (57.7%), 20 had right-sided involvement (38.5%) and 32 had left-sided involvement (61.5%). All the recruited study participants were right-side dominant. Majority of the study participants had acute onset of stroke (84.6%). The demographic data is depicted in Table 1. The distribution of the study participants with respect to the variables is depicted in Table 2.
Demographic Data of the Study Participants (n = 52).
The Distribution of the Study Participants with Respect to Supine-to-stand Time, Bed Rise Quality, Balance and Trunk Control (n = 52).
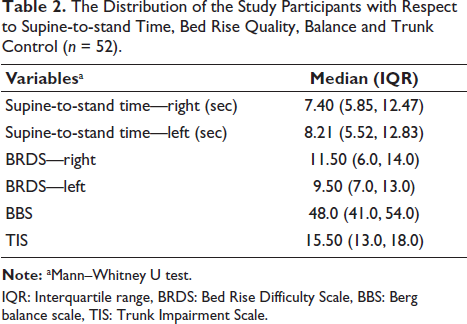
IQR: Interquartile range, BRDS: Bed Rise Difficulty Scale, BBS: Berg balance scale, TIS: Trunk Impairment Scale.
Table 3 depicts the correlation of supine-to-stand time and bed rise quality time with balance and trunk control, irrespective of the side of involvement (right or left hemiplegia). A moderate negative correlation was found between supine-to-stand time and BBS for right-side transition (r = −0.528, p < .0001) and left-side transition (r = −0.519, p < .0001). Similarly, when data was analysed irrespective of the side of involvement for the 52 participants, a significant moderate negative correlation was seen between the supine-to-stand time and trunk control (right side transition (r = −0.452, p < .001); left side transition (r = −0.438, p < .001)). A strong negative correlation was present between bed rise quality towards the left side and balance (r = −0.620, p < .0001), whereas a moderate negative correlation was found between bed rise quality towards the right side and balance (r = −0.499, p < .0001). There was a moderate negative correlation between bed rise quality and trunk control irrespective of the side of transition (right (r = −0.528, p < .0001); left (r = −0.478, p < .0001)).
Correlation of Supine-to-stand Time and Bed Rise Quality with Trunk Control and Balance (n = 52).
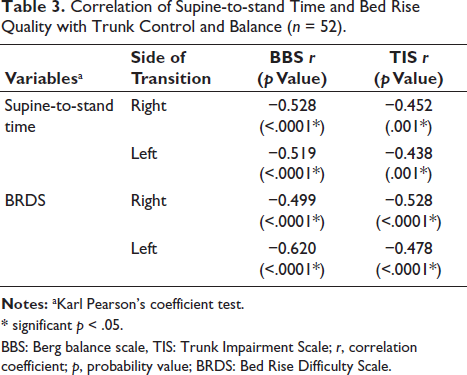
* significant p < .05.
BBS: Berg balance scale, TIS: Trunk Impairment Scale; r, correlation coefficient; p, probability value; BRDS: Bed Rise Difficulty Scale.
Tables 4 and 5 represent the association of supine-to-stand time and bed rise quality with balance and trunk control, respective to the side of involvement (left or right hemiparesis). In the left hemiparetic patients, a significantly moderate negative correlation was found between supine-to-stand time and balance irrespective of the side of transition (non-paretic side transition (r = −0.492, p = .004); paretic side transition (r = −0.521, p = .002)). A weak negative correlation was established between supine-to-stand time towards the non-paretic side and trunk control (r = −0.397, p = .024), whereas a moderate negative correlation was found between supine-to-stand time and trunk control of the paretic side (r = −0.433, p = .013). Bed rise quality and balance were found to have a moderate negative correlation (non-paretic (r = −0.544, p < .001); paretic (r = −0.599, p < .0001)). However, trunk control had a strong negative correlation with bed rise quality towards the non-paretic side (r = −0.611, p < .0001) and a moderate negative correlation with the bed rise quality towards the paretic side (r = −0.561, p < .001).
Correlation of Supine-to-stand Time and Bed Rise Quality with Balance and Trunk Control in Left Hemiparetic Patients (n = 32).
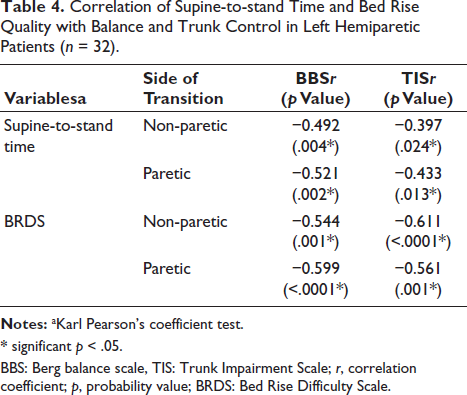
* significant p < .05.
BBS: Berg balance scale, TIS: Trunk Impairment Scale; r, correlation coefficient; p, probability value; BRDS: Bed Rise Difficulty Scale.
Correlation of Supine-to-stand Time and Bed Rise Quality with Balance and Trunk Control in Right Hemiparetic Patients (n = 20).

*significant p < .05.
BBS: Berg balance scale, TIS: Trunk Impairment Scale; r, correlation coefficient; p, probability value; BRDS: Bed Rise Difficulty Scale.
In the right hemiparetic patients (Table 5), a moderate negative correlation was found between supine-to-stand time towards the non-paretic side and balance (r = −0.520, p = .019). A strong negative correlation was found between supine-to-stand time towards the paretic side and balance (r = −0.651, p = .002). Similarly, a moderate negative correlation was established between supine-to-stand time and trunk control (paretic side transition (r = −0.589, p = .006); non-paretic side transition (r = −0.501, p = .024)). Bed rise quality towards the paretic side had a moderate negative correlation with balance (r = −0.501, p = .024), whereas a strong negative correlation was found between bed rise quality towards the non-paretic side and balance (r = −0.653, p = .002). Trunk control had a weak but insignificant negative correlation with bed rise quality towards the paretic side (r = −0.273, p = .244) and a moderate but insignificant negative correlation with bed rise quality towards the non-paretic side (r = −0.418, p = .067).
Discussion
Clinical assessments designed to predict functional abilities post-stroke should be efficient, easy and time saving. The time taken to rise from bed to standing and bed rise quality used in our study is quick, simple and practical. The results demonstrated that an increase in the time taken to transition from supine-to-standing was significantly correlated with impaired trunk control and balance. Likewise, a decrease in the quality of bed rise was correlated with poorer trunk control and balance. This shows the importance of transitional movements in functional recovery post-stroke.
Previous research has correlated rise from bed ability and time taken for the same, on admission, with balance and independent gait on discharge, and found a significant correlation between these measures. 17 These findings are consistent with our study where supine-to-stand time and bed rise quality were better among patients with good balance control. Balance is also considered to be an independent predictor of sit-to-stand ability. 29 The findings of our study reinforce the need to assess transitional movements in stroke patients. While a recent study has examined the relationship between floor-to-stand test with physical performance measures such as balance and gait, 38 it lacks the sit-to-stand component which is a vital ADL. A prolonged time required to transit from supine-to-standing could be due to decreased muscle strength, spasticity and impaired somatosensory function seen in stroke survivors. In addition, age and stroke severity which are known predictors of sitting ability may also be a contributor of increased supine-to-stand transition time due to impaired postural and motor control. 39 These factors hinder their ability to generate adequate muscle force required to shift balance during a transitional movement. The supine-to-stand movement involves transitioning from a broad base of support to a narrower one, primarily centred around the feet. Hence, this transition demands rapid and effective postural reactions to maintain the centre of mass within the base of support, 29 which can explain the correlation of supine-to-stand time and bed rise quality with balance. Since both BBS and supine-to-stand transition involve sit-to-stand components, patients with higher BBS scores appeared to perform supine-to-stand transition more efficiently.
Similarly, transiting from a lower centre of gravity to a higher centre of gravity requires coordination between trunk and limb movements, good postural stability and equilibrium, which are functions often impaired in hemiparetic patients. 40 The findings of the current study show that trunk control is crucial for transitioning from supine-to-standing and bed rise quality. This is in line with previous literature which states that trunk training plays a key role in the improvement of trunk control, dynamic balance and mobility in stroke patients. 41 Bed rise variability among post-stroke participants can be due to several factors including motor weakness, impaired balance and poor inter-joint coordination. 42 Particularly, rolling in bed is affected among stroke survivors due to the impaired activity of trunk muscles. Effective rolling requires coordinated activation of both sides of the trunk, where the agonist muscles facilitate rolling and the contralateral muscles provide stabilisation, enabling smooth movement.43–45 This can explain the prolonged transition time and an increased variability in bed rise among post-stroke survivors, underscoring its association with trunk control.
Interestingly, the results of this study found a significant moderate negative correlation between supine-to-stand time and bed rise quality with trunk control, particularly among left hemiparetic patients. This aligns with the findings of previous research which states that trunk control is found to be more involved among patients with right hemispheric lesions. 46 This could also explain why the correlation between bed rise quality and trunk control was slightly lower in right hemiparetic patients compared to balance.
The limitations of the study were that the results could not be generalised due to the heterogeneous study population with respect to the side of impairment and gender. The study predominantly included supra-tentorial stroke cases and those in the acute phase. There was an underrepresentation of infra-tentorial stroke and chronic stroke patients, which limits the applicability of the findings. Potential confounding factors such as the participants’ prior physical activity levels and rehabilitation history, which were not controlled, may have influenced the outcomes. All the study participants were right-side dominant which may have influenced the supine-to-stand transition performance and quality of bed rise on the dominant side. Additionally, details regarding undiagnosed comorbidities, such as potential visual impairments among participants, were not known, which might have influenced the outcomes. Further research addressing these limitations, including diverse stroke subtypes and phases, is recommended to improve the generalisability of the results.
Conclusion
The supine-to-stand time and bed rise quality assessed in this study may serve as indicators of trunk control and balance ability among post-stroke patients. An increase in time taken to execute supine-to-standing and a reduction in the bed rise quality were found to be closely correlated with poor balance and trunk control among the post-stroke participants. Hence, supine-to-stand time and bed rise quality can be utilised to evaluate and monitor trunk control and balance recovery during stroke rehabilitation.
Footnotes
Acknowledgement
The authors would like to thank all the study participants for their participation and cooperation.
Authors’ Contributions
Manisha Nayak was the principal investigator, who collected the data and critically revised the manuscript.
The study was conceptualised and designed by Abraham M. Joshua and Akshatha Nayak, who also critically edited the text.
Shivanand Pai oversaw the study, and Prasanna Mithra P. evaluated the data.
The paper was prepared with equal contributions from all the authors.
Data Availability Statement
The data supporting the findings of this study are openly available in Figshare at
Statement of Ethics
The study protocol was approved by the Scientific Committee and Institutional Ethics Committee of Kasturba Medical College, Mangalore (IEC KMC MLR 11-16/293).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was obtained from all the study participants before they participated in the study.