
Abstract
Background
Depression is a prevalent mental health disorder and a significant contributor to disability adjusted life years. It is also associated with increased cardiovascular risk, often not adequately addressed by current treatments, leading to significant gaps in the treatment. Yoga practices like Vamana Dhauti could be a potential adjunct therapy to standard treatments by balancing doshas and positively influencing vagal tone.
Objective
This pilot randomised controlled trial aimed to assess the feasibility and tolerability of Vamana Dhauti in depression patients and its effects on Heart Rate Variability (HRV). Clinical changes were evaluated using the Hamilton Rating Scale for Depression (HAM-D).
Methods
The study was conducted at the Department of Integrative Medicine, NIMHANS, Bengaluru. Patients with depression, aged 18–50 years, both genders, and no contraindications to Vamana Dhauti, were randomly assigned to Vamana Dhauti + Shavasana (n = 12) or Shavasana rest only (n = 12) groups using online software, which also included allocation concealment. Outcome measures include feasibility (acceptability, demand, practicality, adaptation, integration, perceived ease, and difficulty), tolerability (adverse events), HRV and HAM-D.
Results
Vamana Dhauti was found feasible and tolerable in patients diagnosed with depression. Vamana Dhauti was well-accepted, could be completed within the given setting and time, and was found to be easy to practice by participants (VAS = 2 ± 1.65; 0 being very easy and 10 being very difficult) with few mild adverse events (n = 2/12). Notably, a significant group × time interaction was observed in HRV, low-frequency measures [F (1,22) = 8.168; p = .009)]. Both groups saw an increase in Low-frequency during the first 10 minutes of Shavasana (control > intervention), but after 20 minutes, only the intervention group returned to baseline values, showing improved resilience. Clinical outcomes measured by HAM-D showed a significant improvement in both groups.
Conclusion
Vamana Dhauti is feasible and well-tolerated by patients diagnosed with depression, suggesting its potential integration into depression-focused Yoga modules.
Introduction
Depression is a common mood disorder, 1 and a leading cause of disability adjusted life years (DALYs) in Asia, with a prevalence ranging from 3.2% to 4.7%.2, 3 It can start early in life and continue into adulthood, generally affecting women more than men and, if not treated, adversely impacting education, work, and relationships.1, 4 Stressful life events and genetic susceptibility influence the onset of depression, prognosis, and relapse likelihood. 5 Some underlying mechanisms include deficiency of norepinephrine, serotonin, and dopamine, and abnormal levels of endocrine factors, including growth hormone (GH). The Vagus nerve mediates two-way communication between the gut and the brain, regulates the anti-inflammatory reflex, and maintains the gut barrier. Stress-induced vagal tone reduction triggers inflammation and gut barrier disturbances, further deteriorating depression.6, 7 Guidelines recommend a combination of second-generation antidepressants and psychotherapy interventions, with measurement-based care and maintenance therapy for depression. 8 However, low remission rates, higher relapse, drug intolerance, and reduction in Heart Rate Variability (HRV) associated with antidepressants9, 10 make it essential to find an alternative treatment that can augment the effects of antidepressants.
Mind-body interventions like Yoga enhance HRV, potentially reducing both depressive symptoms and cardiovascular risks. 11 Not all Yoga practices have similar effects on HRV. Kapalbhati, high-frequency yogic breathing (at the rate of 2.0 Hz for 15 minutes), and breath awareness increase sympathetic activity and reduce vagal tone when done alone. In contrast, very slow breathing and meditation have the opposite effect. Thus, a more comprehensive Yoga module with relaxation techniques preceded by more dynamic practices could improve cardiac health and autonomic system balance.12–14 While the exact mechanisms of Yoga’s benefits for depression remain unclear, studies suggest that changes in cortisol levels, HRV, Brain-Derived Neurotrophic Factor (BDNF), modulation of synaptic plasticity through plasma C1q, Factor H and Properdin, along with changes in inflammatory markers such as IL-6, DHEAS, Sirtuin 1, and telomerase activity may contribute to its therapeutic effects on Major Depressive Disorder (MDD).7, 15, 16 There is preliminary evidence of its efficacy as a standalone treatment for mild to moderate depression. 17
Among the Sharirik doshas (pathogenic factors of the body) vata, pitta and kapha; depression is associated with vata vitiation with kapha avarna (covering/obstruction) and imbalance of tamas among the manasika doshas (pathogenic factors of the mind, i.e., rajas, tamas and sattva); thus, treatment of depression involves addressing kapha followed by vata. 18 Hatha Yoga includes asana (Yoga postures), shatkarmas (six yogic cleansing techniques) and pranayama (breath control), mudras (Yoga gestures) and bandhas (energy locks), and samadhi (enlightenment). Shatkarmas in traditional texts such as Hatha Yoga Pradipika and Gheranda Samhita are advised when the body’s tridoshas (Vata, Pitta, Kapha) are imbalanced before asana and pranayama practice for better outcomes. Dhauti (yogic cleansing of the digestive tract, respiratory tract) is particularly mentioned to help with kapha and pitta disorders.19, 20 However, current scientific research primarily focuses on Yoga programmes with asanas and pranayama only. 21
The procedure of Vamana Dhauti (therapeutic self-induced emesis) includes drinking saline water and vomiting it out under the guidance of a Yoga expert. Thus, the Vagus nerve may be stimulated during Vamana Dhauti via chemical (saline water), mechanical (distension of the stomach), and reflex (gag and vomiting) mechanisms. This stimulation may lead to improved vagal tone and enhanced resilience. According to yogic texts, balancing doshas through practices like Vamana Dhauti can enhance the effects of subsequent asanas and pranayama.19, 20 Therefore, incorporating Vamana Dhauti in Yoga modules for depression may yield more beneficial results compared to practicing only asanas and pranayamas.
Methods
It is a prospective pilot randomised controlled trial (RCT). The primary objective was to evaluate the feasibility and tolerability of add-on Vamana Dhauti in patients with depression and changes in HRV. The secondary objective was to assess the effect of Vamana Dhauti on depression using Hamilton’s Depression Rating Scale (HAM-D). As it was a novel pilot feasibility study, a sample size of 24, twelve in each group, was chosen. 22 Consenting patients with depression from the inpatient and outpatient services of the Department of Integrative Medicine, NIMHANS, were randomly allocated to either intervention (add-on Vamana Dhauti) or control group (treatment as usual) using stratified random sampling based on age groups (18–35 and 36–50 years). The study included participants aged 18–50 years of both genders diagnosed with depressive disorders according to ICD-11/DSM V-TR criteria; patients with current gastric or duodenal ulcers, hypertension, cardiovascular disorders, alcohol-related oesophageal issues, hernia, pregnant individuals, comorbidities such as diabetes with increased intraocular pressure, those unable to understand Vamana Dhauti procedures, those practicing Yoga or similar practices in the past month, and those at risk of harm or with active suicidal ideations were excluded.
The intervention group received a single session of Vamana Dhauti (lasting 10 minutes) followed by 20 minutes of Shavasana rest on the first day. In contrast, the control group underwent 20 minutes of Shavasana rest only. In addition, both groups underwent six days of supervised group Yoga sessions using the validated Yoga therapy module for depression. 23
Feasibility outcome parameters: Acceptability and demand: If the intervention fits well in the participants’ daily lives and assess its acceptability based on retention and dropout rates. Implementation and practicality: If the intervention is completed within the designated time frame, commitment level, and with available resources. The time taken for Vamana Dhauti was calculated for each patient. Adaptation and integration: Whether any modifications were needed for the intervention to suit the given population or setting. Perceived effects and difficulty: A Visual Analogue Scale (VAS [(0-10)] to measure the ease of the practice of Vamana Dhauti.
Patients were followed up until the next day to check for any adverse events related to the procedure to ensure tolerability.
HRV was measured using Equivital Life Monitor (EQ02) in the supine position at baseline (before Vamana Dhauti or supine rest) for 10 minutes and during Shavasana rest (after Vamana Dhauti) for 20 minutes in both the intervention and control groups. The HRV recordings were taken in the morning between 7
Depression scores were measured using HAM-D at baseline and after six days of Yoga by an assessor blinded to the intervention allocation.
Statistical analysis was performed using the IBM Statistical Package for the Social Sciences (SPSS), version 24.0. The outcome variables were checked for normality using the Shapiro-Wilk test and Q-Q plots. Baseline categorical data were analysed using the Chi-square test, and the continuous data were analysed using the Independent sample t-test. The HRV data were found to be not normally distributed. So, it was converted into log values and analysed using Repeated Measures ANOVA (RM-ANOVA), where the groups were considered fixed effects. In contrast, the clinical variables (dependent variables) were considered as random effects.
Results
Screening and Baseline Characteristics
Sixty-eight participants were screened for eligibility, with 40 excluded based on predetermined inclusion and exclusion criteria. The remaining 26 eligible participants were randomly allocated into two groups of 13 each. During the study, one participant from each group withdrew (one declined to participate, and another was referred to a different hospital). Consequently, the final analysis included 12 participants per group (Tables 1 and 2).
Baseline Characteristics.
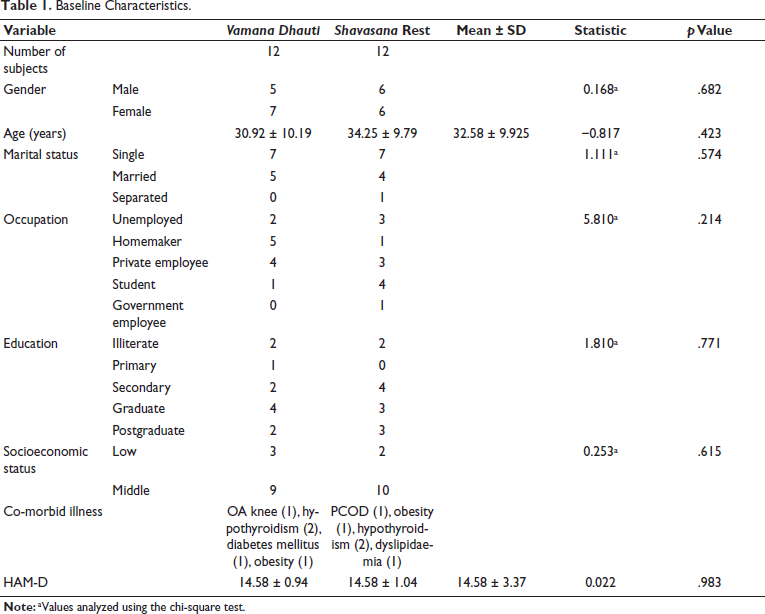
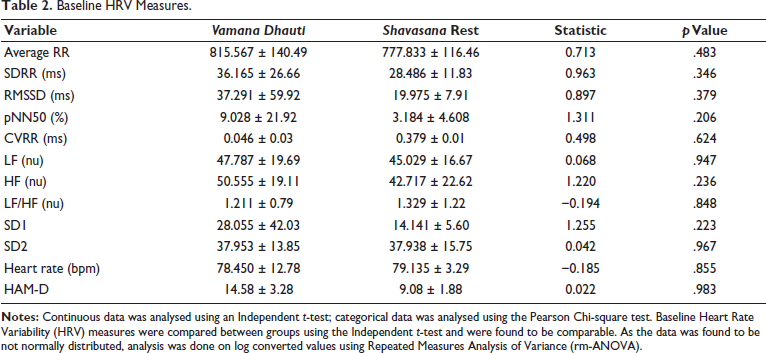
Baseline HRV Measures.
Feasibility and Tolerability
The intervention showed strong acceptance and demand, given the minimal number of dropouts (n = 2). It was effectively implemented within the specified setting, with completion time ranging from 7 to 15 minutes and an average time of 10.67 ± 2.64 minutes. Participants rated the ease of the intervention on VAS from 0 to 10 (0 representing easiest and 10 representing difficult), averaging 2 ± 1.65. The intervention was seamlessly integrated into existing treatment regimens without necessitating significant modifications or changes to the existing medications or therapies of the patient. Most of the participants (10/12) expressed their intent to continue practicing the newly taught intervention. Adverse events were diligently documented, with two participants experiencing mild adverse effects—one reported a loose stool the same day (n = 1), while another reported fatigue (n = 1). These findings suggest that Vamana Dhauti is generally well-tolerated in this context.
HRV and Clinical Outcomes
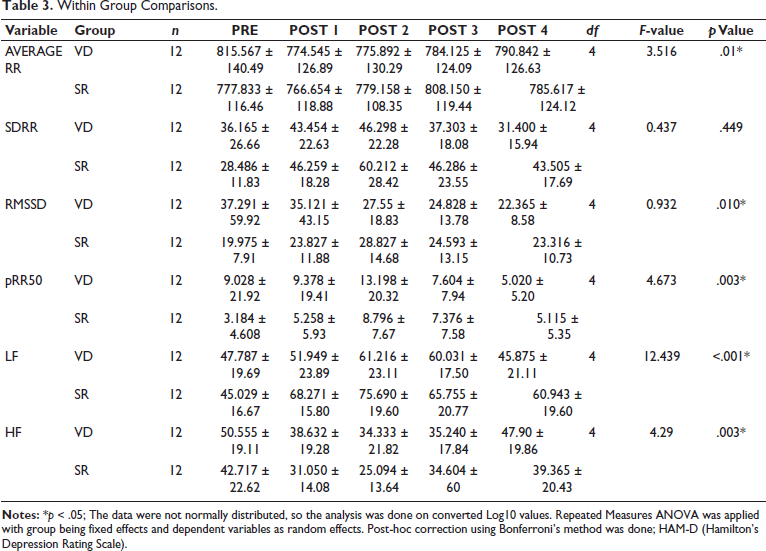
The Repeated Measures of Analysis of Variance (RM-ANOVA) showed a significant group × time interaction in low-frequency LF (nu) (df = 1,22; F-value = 8.168; p = .009), such that the LF increased in the intervention group following Vamana Dhauti, while the control group did not show any change. Other parameters of HRV analysis did not show statistically significant differences in the group × time comparisons.
Clinical outcomes measured by HDRS-17 showed a significant reduction in both groups over time (df = 1, F-value = 207.77, p = <.001) (Table 3).
Within Group Comparisons.
Discussion
The study findings show that Vamana Dhauti is feasible and well-tolerated by patients with mild to moderate depression. The dropout rate was low, suggesting high acceptance, seamless integration, and completion within the expected time. Minor adverse effects were observed, which were self-limiting and without the need for any additional medical assistance to suggest its tolerability.
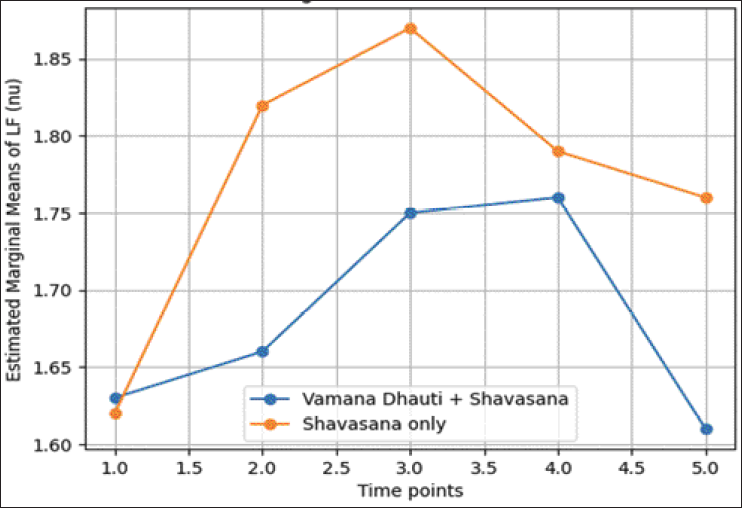
Further, changes in HRV were explored to understand the physiological mechanisms of Vamana Dhauti. We hypothesised that voluntarily induced vomiting may act through the vagal pathway, potentially enhancing vagal tone. Results show a significant change in the LF (nu) following Vamana Dhauti. Furthermore, clinical outcomes, as measured by the HAM-D, showed a significant reduction in depressive symptoms in both groups. A graphical representation of the data, comparing baseline to post-20-minute intervals divided into four time points (0–5, 5–10, 10–15, 15–20) as given in Figure 1. During the 20-minute session, participants experienced Yoga variations in LF nu, with an initial rise during muscle contraction and subsequent relaxation, leading to a decline. Notably, the control group showed a more pronounced LF nu increase than the intervention group, suggesting a potential resilience in the Vamana Dhauti group, possibly linked to an increased LF nu during Vamana Dhauti. LF nu levels decreased in the intervention group, returning to baseline by the session’s end. Similar trends were also observed in HF nu values. Thus, the changes in HRV suggested improved resilience in the intervention group as compared to the controls.
It is in line with previous studies, which showed that Hatha Yoga has significant effects on HRV, resulting in clinical improvements in depressive symptoms and cardiovascular health.11, 12, 14 High-frequency breathing and other Shatkarma practices like kapalbhati heighten sympathetic activity when done alone, whereas slow breathing techniques and meditation have the opposite effect. Thus, integrating dynamic practices like shatkarmas followed by relaxation techniques, which is a more comprehensive Yoga module, may facilitate a balanced autonomic response.11–14 Among the various types of dhauti, Vamana Dhauti or Kunjala Kriya is the easiest to learn and implement. Its simplicity in practice could make it a practical and accessible option in addition to Yoga modules aimed at managing depression. Currently, there is limited research on the physiological mechanisms of shatkarmas, with only one study invesigating their effects on pulmonary functions in healthy adults. This study revealed enhanced diaphragm function, reduced airway resistance, improved lung emptying, and vagal predominance, reflecting adaptations in the pulmonary system. 24 Although physiology involved in vomiting involves chemoreceptors and mechanoreceptors sensitive to mechanical and chemical stimuli, which transfer signals via afferent fibres of the Vagus nerve to higher centres in the medulla. Efferent fibres from the emetic centre lead to nausea, vomiting, and retching. 25
Despite being an integral aspect of Hatha Yoga, Shatkarmas are often overlooked in patient populations due to the perceived difficulties in teaching, integration, and execution within the given settings. However, this study provides valuable insights into the feasibility of incorporating shatkarmas into Yoga modules, challenging these preconceived notions.
The results showed that the intervention group had better recovery in their HRV than the control group after the relaxation session, indicating enhanced resilience. Despite the limitation of a small sample size, these results provide valuable insights into facilitators and barriers for future trials. This study lays a foundation for further exploration of Vamana Dhauti’s potential benefits in depression management through larger, more comprehensive trials.
Conclusion
This pilot RCT shows that Vamana Dhauti is feasible and tolerable in patients with depression. At the same time, its clinical efficacy requires further investigation through more rigorous RCTs in the future. The results showed that the intervention group had better recovery in their Heart Rate Variability than the control group after the relaxation session, indicating enhanced resilience. These results provide valuable insights into the methodology for conducting RCTs, highlighting facilitators and barriers for future trials. This study lays a foundation for further exploration of Vamana Dhauti’s potential benefits in depression management through larger, more comprehensive trials.
Footnotes
Authors’ Contribution
The authors alone are responsible for the content and writing the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Statement of Ethics
The study was approved by the Institute Ethics Committee (IEC), Human Ethics Committee for Research in AYUSH and Integrative Medicine (HECAIM), National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru (Reference No. NIMHANS/HECAIM/7th/MEETING/2022-23). The study was prospectively registered with the Clinical Trials Registry of India (CTRI/2023/07/054596) and conducted in accordance with ethical guidelines.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centre for Excellence in Research (CoE) grant titled ‘Yoga and Ayurveda in Neuroscience: Translational Research Accelerator Programme (YANTRA)’ [S-12011/10/2021-SCHEME (CoE)/3988] under the Ayurswasthya Yojana of Ministry of AYUSH, Government of India.
Patient Consent
Written informed consent was obtained from all participants prior to the initiation of data collection. Data were collected between August 2023 and February 2024, and the confidentiality of all participant information was assured and maintained throughout the study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.