
Abstract
Background
Psychiatric comorbidities are among the most disabling non-seizure manifestations of epilepsy yet remain underrecognised in routine care, particularly in low- and middle-income settings. Understanding their clinical spectrum and correlates is vital for comprehensive epilepsy management.
Purpose
To determine the prevalence and spectrum of psychiatric disorders in adults with epilepsy and evaluate their associations with seizure characteristics and antiseizure medication (ASM) use.
Methods
A cross-sectional study was conducted on 98 adults (aged 18–65 years) attending a tertiary epilepsy clinic between January 2024 and February 2025. Psychiatric evaluation was performed using the Patient Health Questionnaire (PHQ-SADS), PHQ-9, the Generalised Anxiety Disorder-7 (GAD-7), the Yale–Brown Obsessive–Compulsive Scale (Y-BOCS), the Brief Psychiatric Rating Scale (BPRS), PHQ-15 and the Columbia Suicide Severity Rating Scale (C-SSRS). Associations between psychiatric symptoms and seizure-related variables (frequency, duration, aura, injury) and the ASM profile were analysed using Pearson correlation and ANOVA.
Results
Overall, 59.2% of patients exhibited at least one psychiatric disorder. Depression (38.1%) and anxiety (19.1%) were the most common, followed by somatic symptom disorder (10.2%), suicidal ideation/behaviour (8.1%), obsessive–compulsive disorder (OCD) (7.2%) and psychosis (6.1%). Higher seizure frequency and longer epilepsy duration correlated significantly with depressive and anxiety symptom severity (p < .05). Aura and seizure-related injuries were associated with elevated affective scores. Polytherapy and older ASMs (phenytoin, carbamazepine) increased depressive risk, whereas newer agents showed better tolerability.
Conclusion
Psychiatric comorbidities are highly prevalent among adults with epilepsy, strongly influenced by seizure burden rather than demographic variables. Routine mental health screening and integrated neuropsychiatric care should be integral to epilepsy management, particularly in resource-limited settings.
Introduction
Epilepsy is a chronic neurological disorder characterised by recurrent, unprovoked seizures caused by abnormal neuronal discharges in the brain. It affects more than 50 million people worldwide and continues to impose a considerable medical, psychological and social burden.1, 2 Beyond seizure control, epilepsy greatly influences mental health, with psychiatric comorbidities emerging as among the most frequent and disabling non-seizure manifestations.3, 4
Individuals with epilepsy are two to five times more likely to experience psychiatric disorders than the general population.5–7 These comorbidities negatively affect seizure control, medication adherence, cognitive performance and quality of life, often contributing more to long-term disability than the seizures themselves. 8
The pathophysiology of psychiatric disturbances in epilepsy is multifactorial, involving both neurobiological and psychosocial mechanisms. Recurrent epileptic activity and network hyperexcitability may disrupt the limbic circuits, particularly the hippocampus and amygdala-responsible for emotional regulation. 9 Monoaminergic dysregulation, hypothalamic–pituitary–adrenal (HPA) axis overactivity, neuroinflammatory processes and altered connectivity between cortical and subcortical regions further contribute to vulnerability for depression, anxiety and psychosis.10, 11 Psychosocial factors such as stigma, social isolation, economic stress and fear of seizure recurrence amplify this risk. 12
Despite increasing global awareness, psychiatric comorbidities remain underrecognised and undertreated in routine epilepsy practice. Most studies have focused primarily on depression and anxiety, while other disorders—including psychosis, obsessive–compulsive disorder (OCD), somatic symptom disorder and suicidal ideation or behaviour—have received less attention, particularly in clinical settings of low- and middle-income countries. Furthermore, the potential influence of seizure-related variables (frequency, duration and aura) and antiseizure medication (ASM) therapy, including polytherapy, on psychiatric symptomatology is incompletely understood. 13
The present study was conducted to assess the prevalence and spectrum of psychiatric comorbidities among adults with epilepsy and to explore their associations with seizure characteristics and antiepileptic drug (AED) usage patterns. Specifically, patients were evaluated for major depressive disorder, generalised anxiety disorder (GAD), psychosis, OCD, somatic symptom disorder and suicidal ideation or behaviour using standardised diagnostic instruments. By identifying clinical and pharmacological predictors, this study aims to strengthen the evidence base for integrated neuropsychiatric assessment and management in adult epilepsy care.
Methods
Aim of the Study
To determine the prevalence and pattern of psychiatric manifestations in patients with epilepsy and to examine their association with demographic and clinical variables associated with seizures and ASMs.
Study Design and Setting
This was a cross-sectional, observational study conducted at the epilepsy clinic of a tertiary care academic hospital. Data were collected prospectively from adult patients attending the clinic over a defined period (January 2024–February 2025).
Participants
A total of 98 adults (≥18 years-65 years) with a confirmed diagnosis of epilepsy, as per the 2017 criteria of the International League Against Epilepsy.
Inclusion Criteria
Established diagnosis of epilepsy.
Regular follow-up in the epilepsy clinic.
Ability to provide informed consent and participate in clinical interviews.
Exclusion Criteria
Any psychiatric disorder diagnosed before the onset of seizures.
Severe cognitive impairment or intellectual disability interfering with a valid psychiatric assessment.
Postictal confusion at the time of evaluation or unstable medical condition.
Progressive neurological diseases (e.g., neurodegen-erative disorders).
Clinical and Demographic Assessment
Demographic variables included age, sex, education level, marital status and occupation.
Epilepsy-related Variables Recorded Were
Seizure type (focal, generalised or combined/unknown),
Seizure frequency during the preceding one year:
Low frequency: ≤1 seizure/month.
Moderate frequency: 2–4 seizures/month.
High frequency: ≥5 seizures/month.
Duration of epilepsy (years).
Presence of aura.
Epilepsy-related injuries within the preceding year (falls, burns, fractures or head trauma).
Antiseizure Medication Profile
Medication details were obtained from clinical records and patient interviews. Variables included:
Type of ASM (monotherapy vs. polytherapy).
Specific drug names (e.g., levetiracetam, valproate, carbamazepine, clobazam, phenytoin, lamotrigine).
Dosages (mg/day) standardised to therapeutic equivalents.
Duration of current ASM exposure (years) and total treatment duration.
Dosages were verified against standard therapeutic ranges (e.g., levetiracetam 500–1,500 mg twice daily (BD; Bis in Die); valproate 200–1,000 mg BD) to capture dose variability.
Drug load (monotherapy = 1, polytherapy = ≥2) was used as an indirect marker of seizure refractoriness.
Psychiatric Evaluation
All participants underwent a structured psychiatric assessment conducted by a neurologist. Psychiatric diagnoses were established in accordance with Diagnostic and Statistical Manual of Mental Disorders (DSM)-5 criteria, using the Patient Health Questionnaire-Somatic, Anxiety and Depressive Symptoms (PHQ-SADS) as the diagnostic tool.
Symptom severity was quantified using standardised rating instruments:
PHQ-9 for depressive symptoms GAD-7 for anxiety Yale–Brown Obsessive–Compulsive Scale (Y-BOCS) for obsessive–compulsive symptoms The Brief Psychiatric Rating Scale (BPRS) for psychotic symptoms, where indicated PHQ-15 for somatic symptom severity Suicidal ideation or behaviour, assessed using the Columbia Suicide Severity Rating Scale (C-SSRS) Psychiatric diagnoses were clinically confirmed based on standardised diagnostic criteria following structured clinical evaluation and all diagnoses were validated by a consultant psychiatrist. Screening scales, when used, served as adjuncts and were not the sole basis for diagnosis.
Statistical Analysis
Descriptive statistics were used to summarise demographic, clinical and psychiatric characteristics. Continuous variables were presented as means with standard deviations and categorical variables as frequencies and percentages. The prevalence of depression and anxiety was determined using PHQ-9 and GAD-7 thresholds (>5), representing mild or greater symptom severity. Additional psychiatric comorbidities—psychosis, OCD, somatic symptom disorder and suicidal ideation or behaviour—were diagnosed using the PHQ-SADS and quantified using the BPRS, Y-BOCS, PHQ-15 and C-SSRS, respectively.
Pearson correlation coefficients were computed to assess linear relationships between seizure-related variables (frequency, duration, presence of aura) and psychiatric symptom severity scores (PHQ-9, GAD-7, Y-BOCS, BPRS, PHQ-15). One-way Analysis of Variance (ANOVA) was applied to compare mean psychiatric scale scores across categories of seizure frequency and epilepsy duration, with post hoc analyses following significant results.
Associations between psychiatric disorders and demographic or clinical factors (age, gender, marital status, education, occupation and antiepileptic drug use) were also examined. Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) version 25.0 (IBM Corp., Armonk, NY, USA), with p < .05 considered statistically significant.
Results
Demographic Characteristics
Demographic and Clinical Characteristics.
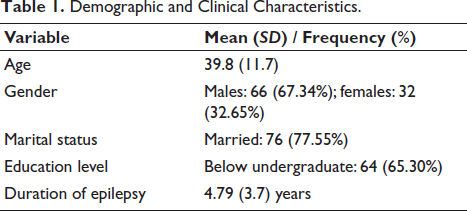
Univariate analysis showed no significant effect of gender, marital status, education or occupation on the presence of psychiatric comorbidities (p > .05), indicating that sociodemographic factors were not independent predictors of psychiatric morbidity. However, Pearson correlation analysis revealed a modest positive association between age and depressive symptom severity (r = 0.336, p < .05), suggesting that older participants had slightly higher PHQ-9 scores. In contrast, anxiety severity correlated weakly and negatively with age (r = −0.134, NS), indicating a mild decline in anxiety with increasing age. Together, these findings imply that while age and other demographic variables did not influence the presence of psychiatric disorders, subtle age-related variations in symptom intensity, particularly for depression, were observed.
Prevalence of Psychiatric Disorders
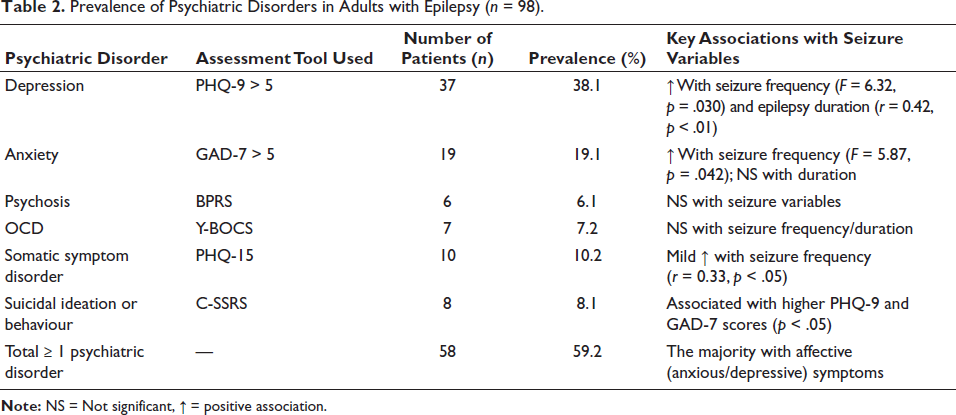
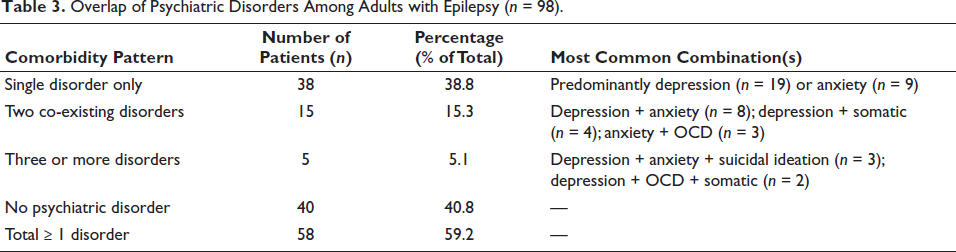
Among 98 adults with epilepsy, psychiatric comorbidities were identified in 58 patients (59.2%) (Table 2). Depression was the most common disorder (38.1%), followed by anxiety (19.1%), somatic symptom disorder (10.2%), suicidal ideation or behaviour (8.1%), OCD (7.2%) and psychosis (6.1%). Comorbidity was frequent, with 20 patients (20.4%) meeting criteria for more than one disorder, most commonly the depression–anxiety combination (8.2%) (Table 3). Multimorbidity was associated with higher seizure frequency and longer epilepsy duration (p < .05). Although eight patients (8.2%) exhibited both depression and anxiety, the Pearson correlation between PHQ-9 and GAD-7 scores was minimal (r = 0.042*), implying their severity levels did not vary linearly in this cohort.
Seizure Characteristics Associated with Psychiatric Comorbidities (Table 4)
Patients were grouped by seizure frequency:
Low (≤ 1/month): 34 patients Moderate (2–4/month): 33 patients High (≥ 5/month): 31 patients
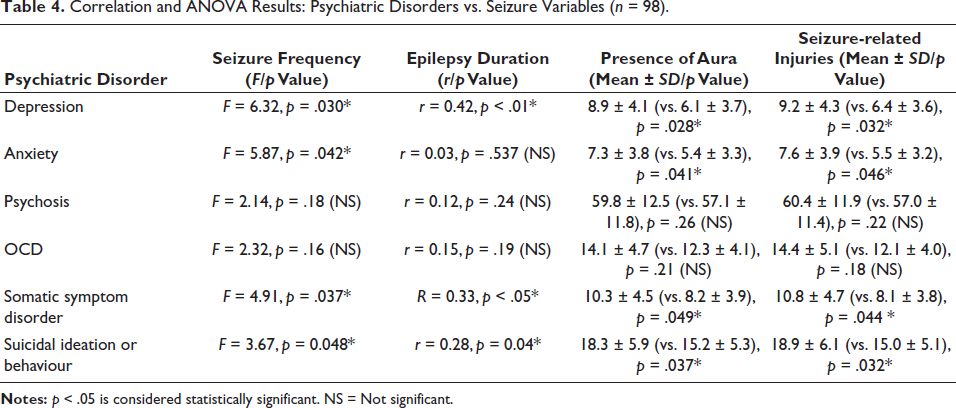
ANOVA revealed that seizure frequency and duration had significant associations with affective and somatic symptoms. Patients with moderate (2–4/month) and high seizure frequency (≥5/month) exhibited higher PHQ-9 and GAD-7 scores compared with those with infrequent seizures (F = 6.32, p = .030 and F = 5.87, p = .042, respectively). Epilepsy duration was positively correlated with depression severity (F = 6.45, p = .019; r = 0.42, p < .01), while anxiety showed a weaker, nonsignificant association (p = .537). Somatic symptom scores (PHQ-15) were modestly related to seizure frequency (r = 0.33, p < .05*).
The presence of aura was associated with higher mean PHQ-9 and GAD-7 scores compared to patients without aura (p < .05*). Additionally, patients reporting seizure-related injuries (n = 24) had significantly elevated depression and anxiety scores compared to those without injuries (p = .032 and p = .041, respectively), indicating that physical harm and loss of control contribute to psychological morbidity.
In contrast, psychosis and OCD showed no significant relationships with seizure frequency, duration, aura or injury, suggesting that these disorders may arise from distinct neurobiological or medication-related mechanisms rather than seizure burden itself.
Antiseizure Medication Profile and Psychiatric Associations
Prevalence of Psychiatric Disorders in Adults with Epilepsy (n = 98).
Overlap of Psychiatric Disorders Among Adults with Epilepsy (n = 98).
Correlation and ANOVA Results: Psychiatric Disorders vs. Seizure Variables (n = 98).
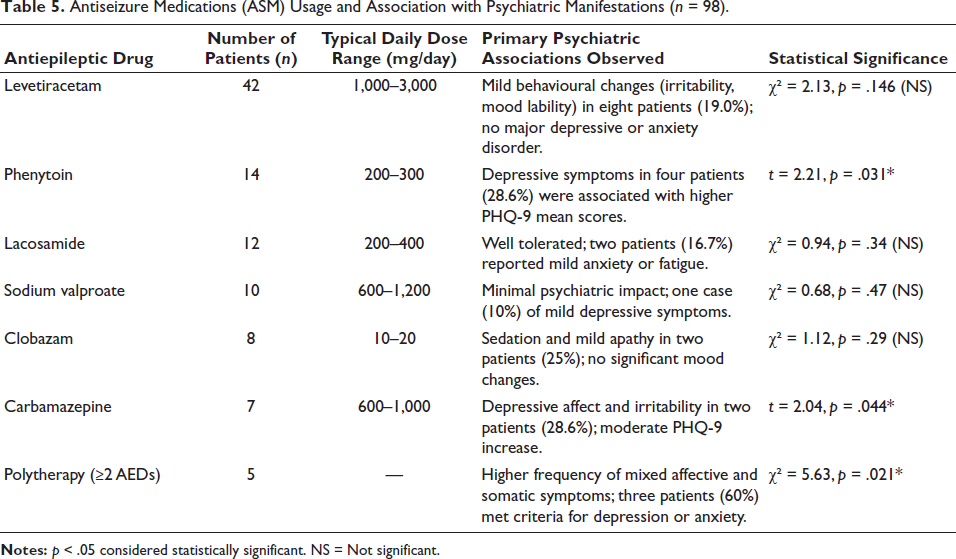
Antiseizure Medications (ASM) Usage and Association with Psychiatric Manifestations (n = 98).
Discussion
This cross-sectional study highlights the substantial psychiatric burden among adults with epilepsy, with 59.2% of participants exhibiting at least one psychiatric disorder. The predominance of depression (38.1%) and anxiety (19.1%) mirrors earlier observations from both Indian and international cohorts, which have reported rates ranging from 30% to 50% for depression and 15%–25% for anxiety.3, 14, 15 These findings reinforce that psychiatric comorbidities represent a major determinant of disease complexity and quality of life in epilepsy.
The strong association between seizure frequency, duration and depressive symptom severity in this cohort supports the theory of shared neurobiological pathways between epilepsy and mood disorders. Chronic epileptic discharges may induce limbic network dysfunction, particularly in the amygdala and hippocampus, leading to disturbances in serotonergic and gamma-aminobutyric acid (GABA) ergic transmission. These limbic alterations, coupled with HPA axis dysregulation, may explain the progressive emergence of depression with increasing seizure chronicity.
In contrast, the modest relationship between anxiety and seizure duration suggests that anxiety symptoms may be more reactive or anticipatory, often related to fear of recurrence, unpredictability of seizures or situational avoidance, rather than cumulative neuronal injury. The significant association of aura presence with higher PHQ-9 and GAD-7 scores implicates that the auras, particularly from temporal or insular foci, may heighten autonomic and limbic activation, reinforcing both physiological arousal and conscious fear of impending seizure.
Patients reporting seizure-related injuries also showed elevated affective scores, likely reflecting post-event anxiety. These findings together suggest that seizure burden influences emotional distress both through biological vulnerability and psychological reinforcement mechanisms.
No significant association was found between psychiatric symptoms and demographic factors (age, gender, marital status, education or occupation). This supports prior meta-analyses 5 suggesting that psychosocial stress and neurobiological pathology, rather than demographic background, drive psychiatric morbidity in epilepsy.
Similarly, ASM usage overall did not predict depression or anxiety severity, possibly because most patients were on levetiracetam or modern agents with minimal psychotropic interference. Although some prior studies have associated levetiracetam with irritability, our cohort demonstrated only mild behavioural changes without statistical significance, likely due to standardised dosing and short exposure duration.
The significant association of phenytoin and carbamazepine with higher PHQ-9 scores may relate to enzyme induction–mediated folate depletion or direct effects on serotonergic tone, consistent with previous pharmacovigilance reports. 4 The absence of correlation for valproate, lacosamide and clobazam aligns with their known mood-stabilising or neutral profiles. These findings highlight that drug-related mood changes are heterogeneous and often masked by seizure control benefits or interindividual tolerance differences.
Individuals on polytherapy (≥2 AEDs) exhibited the highest prevalence of depressive and anxiety symptoms (60%, p = .021). This finding aligns with evidence that polytherapy increases neuropsychiatric vulnerability through several converging mechanisms.
First, the combined use of multiple AEDs can cause additive central nervous system (CNS) depressant effects, leading to fatigue, apathy or mood blunting. Second, pharmacokinetic interactions between enzyme-inducing drugs. Third, the psychological burden of chronic illness requiring multiple medications may heighten perceived disease severity and health anxiety.
Our data echo findings that polytherapy, even when clinically necessary for seizure control, may independently worsen affective outcomes.4, 16 Clinicians should therefore balance seizure control with mental health screening, gradually simplifying regimens where feasible and integrating psychiatric monitoring into long-term epilepsy management.
Our results are in close agreement with recent multicentric studies such as the standard and new antiepileptic drugs trial (SANAD)-II trial,16, 17 which identified seizure frequency as the most robust predictor of affective symptoms. The inclusion of somatic symptom disorder (10.2%) and suicidal ideation (8.1%) expands the conventional focus beyond depression and anxiety, illustrating the multi-dimensional psychiatric spectrum of epilepsy. The relatively low rate of psychosis (6.1%) and OCD (7.2%) is consistent with interictal psychosis patterns and selective cortical involvement rather than seizure load, reflecting distinct neurochemical origins.
This study contributes new evidence from a resource-limited tertiary care setting, emphasising that psychiatric morbidity is not merely reactive but integral to the epileptic disease process. The use of a structured diagnostic interview (PHQ-SADS) alongside validated severity scales (PHQ-9, GAD-7, Y-BOCS, BPRS, PHQ-15, C-SSRS) ensured diagnostic rigour. Importantly, the identification of aura-related distress and injury-linked affective symptoms as independent correlates adds a novel clinical dimension not systematically captured in earlier Indian studies.
The absence of demographic influence and the weak correlation between PHQ-9 and GAD-7 scores despite comorbidity further suggest that depression and anxiety in epilepsy, though often co-existing, are phenotypically distinct—possibly mediated by different neural networks (amygdala–hippocampal vs. orbitofrontal circuits).
The limitation of this study is that, being a cross-sectional hospital-based study, causality cannot be inferred. The overall sample size was modest, which may have limited the power to detect subtle associations. In addition, several diagnostic and treatment subgroups had small numbers, reducing the precision and stability of subgroup estimates. The lack of detailed epilepsy classification (e.g., temporal vs. extratemporal), type of aura, electroencephalography (EEG) lateralisation and neuroimaging correlates restricts the precise localisation of psychiatric associations. Moreover, potential confounders such as socioeconomic stress, cognitive impairment and ASM’s blood levels were not analysed. Longitudinal designs and multimodal neuroimaging could clarify causal pathways and temporal dynamics of psychiatric comorbidity.
Conclusion
Psychiatric disorders are highly prevalent among adults with epilepsy, with depression and anxiety being the most common and clinically significant. The study demonstrates that seizure burden, including frequency, duration, aura and seizure-related injuries, is the strongest determinant of psychiatric morbidity, surpassing demographic or pharmacologic influences. While affective and somatic symptoms are tightly linked to seizure activity, psychotic and obsessive–compulsive phenomena likely arise from distinct neurobiological mechanisms.
Older ASMs (phenytoin, carbamazepine) and polytherapy modestly increased depressive risk, whereas levetiracetam and modern agents were generally well tolerated. These findings underscore the necessity of routine mental health screening within epilepsy clinics and advocate for integrated neuropsychiatric care models. Future longitudinal studies combining neuroimaging, neuroendocrine profiling and cognitive-affective mapping could further elucidate the bidirectional brain–behaviour interface underlying epilepsy and psychiatric comorbidity.
Footnotes
Acknowledgement
The authors express sincere gratitude to the faculty and staff of the Department of Neurology, MS Ramaiah Medical College and Hospitals, Bengaluru, for their valuable support during data collection and patient evaluation. The authors also thank all study participants for their cooperation and consent to participate in this research.
Authors’ Contribution
Dr Shalini Shanthi: Conceptualisation, data collection, psychiatric evaluation, statistical analysis and manuscript drafting.
Dr R. Pradeep: Study design, supervision, data validation, manuscript review and corresponding author responsibilities.
Dr Mahendra Javali: Overall scientific guidance, clinical expertise and critical revision of the manuscript for intellectual content.
Dr Chandrashekar Enuguri, Dr Chintalapati Ashrith, Dr Immani Soma Mani Giridhar: Patient recruitment, clinical data verification, literature review and editing.
Dr Anish Mehta, Dr Purushottam Acharya: Methodological inputs, manuscript review and approval of the final version.
Each author made substantial contributions to the conception, design, acquisition, analysis and interpretation of data, participated in drafting or revising the article and approved the final version to be published.
Data Availability Statement
The data supporting the findings of this study are derived from patient medical records and structured interviews conducted at the Department of Neurology, MS Ramaiah Medical College Hospital, Bengaluru. In accordance with Institutional Ethics Committee policy and to protect patient confidentiality, these data are not publicly available. De-identified data may be obtained from the corresponding author upon reasonable request and with prior approval from the Institutional Ethics Committee.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
ICMJE Statement
This manuscript has been prepared in accordance with the International Committee of Medical Journal Editors (ICMJE) recommendations. All authors meet the ICMJE authorship criteria, have substantially contributed to the conception, design, data acquisition, analysis or interpretation of data, drafted or critically revised the article for important intellectual content and approved the final version for publication.
Informed Consent
Written informed consent was obtained from all participants prior to their inclusion in the study. All assessments were conducted in accordance with the ethical standards of the Institutional Ethics Committee of MS Ramaiah Medical College, Bengaluru.
Statement of Ethics
This study was approved by the Institutional Ethics Committee of MS Ramaiah Medical College, Bengaluru (Approval No. MSRMC/EC/AP-11/09-2024). Written informed consent was obtained from all participants before inclusion. Confidentiality and ethical standards were maintained throughout the study.