
Abstract
Background
Intimate partner violence (IPV) is a significant problem; however, researchers and clinicians have not paid much attention.
Purpose
To assess the prevalence of IPV among married rural women and its correlates.
Methods
This cross-sectional study was conducted in a rural area. All the eligible females were assessed on the Intimate Partner Violence Questionnaire (IPVQ), Generalised Anxiety Disorder Questionnaire-7 (GAD-7) and Patient Health Questionnaire (PHQ)-9.
Results
169 females included with the mean age of 35.8 years. The prevalence of lifetime experience of IPV was 29.0%. Controlling behaviour was most common, followed by physical violence, threatening behaviour and sexual behaviour. About one-fourth (26%) had depres-sion, and a little less than one-third (30.8%) had an anxiety disorder. Severity of depression and anxiety had a significant posi-tive correlation with IPV and other domains of IPV. Those participants whose husbands were consuming alcohol or other illicit drugs and were from a lower socio-economic status reported a significantly higher experience of IPV.
Conclusion
The stakeholders, such as community health organisations, Ministry of Family and Healthcare organisations and others, should work in collaboration with a non-govern-mental organisation in a coordinated and planned manner and can take a pivotal role in research, prevention of IPV and other psychiatric problems among rural females.
Introduction
Intimate partner violence (IPV) is a significant public health problem that significantly impacts physical and mental health.1–3 IPV can be understood as ‘any behaviour within an intimate relationship (married, unmarried and live-in) that causes physical, psychological or sexual harm to those in that relationship’.4, 5 IPV comprises physical, sexual, threatening, controlling and psychological violence committed by the current or ex-intimate partner, including a spouse or a dating partner.
The World Health Organization surveyed 10 countries and reported a lifetime prevalence of IPV of 29.6%, which varies from 15% to 71% from country to country. 6 Up to one-third of women experienced violence perpetrated by an intimate partner worldwide.6, 7 Studies from developing countries like India started appearing, but there are inconsistencies in reporting the prevalence rate of IPV. The studies from India reported IPV in a range of 9%–40%.8, 9 National Family Health Survey (NFHS-4: 2015–2016) surveyed 29 states, including 6 union territories, and reported a prevalence rate of up to 40%, varying from 5.6% to 55.6% across different states. 10 The differences in reporting of IPV could be because of the influence of culture, attitude towards violence and societal pressure.
Among the risk factors that are associated with IPV are low household income, lower education in females or their spouses, problems of substance use like drinking alcohol by a male spouse,11, 12 wives’ lower economic status than spouses and women’s unemployment. 12 However, a few studies evaluated the antecedents or risk factors associated with IPV.
The impact of IPV on mental health has also received research attention in the last few years, but most studies are on the association between post-traumatic stress disorder (PTSD) and IPV.13–17 The studies conducted outside India reported a strong correlation between depression and IPV.18–20 Though IPV has been documented as a significant problem in India, only a few studies have explored the antecedents or consequences of IPV or its association with poor mental health. Among the psychological issues, depression, post-traumatic or exacerbation of pre-existing psychological problems were the most common consequences reported in India.3, 21, 22 The available previous studies were done either in urban settings or clinical settings.
With this background, the current study aimed to explore the prevalence of IPV among rural married women and its association with mental health-related problems. To our knowledge, this is one of the first studies from rural India.
Methods
This was a cross‑sectional descriptive study with a purposive sampling technique conducted in two different villages in northern India. The study was conducted in September–October 2021. To be included in the present study, the participants should be ≥18 years of age, female, married, staying with their spouse for at least 1 year, able to read or write Hindi or English, free from any cognitive impairment, acute debilitating physical illness, have no history of psychiatric disorders or head injury and be able to provide the written informed consent.
Procedure
In the present study, a trained female nurse, well versed in colloquial language, visited house-to-house (consecutive sequence) after obtaining permission from the village head and approached the married females. The female nurse explained the nature and the purpose of the current study. Confidentiality and privacy were assured to the participants. If the participants agreed, females were asked to provide written informed consent. In the present study, we interviewed 234 married females (agreed to the survey), of whom 169 participants were included in the present study as per the study’s inclusion criteria. The participants were assessed on the structured questionnaire in a private space. During the assessment, psychiatric treatment was offered if anyone was found to be screened positive for a psychiatric problem. Every woman was also provided with information regarding abuse prevention and its remedies.
Participants were assessed on the following questionnaires:
Sociodemographic characteristics: A semi-structured sociodemographic questionnaire included age, educational level, current employment status, religion, caste, number of children, number of abortions, spouse’s age, education, employment and substance use history. Patient Health Questionnaire (PHQ)-9: This is a brief self-administered depression scale and has nine items, with each item rated from ‘0’ (not at all) to ‘3’ (nearly every day). The scale has excellent internal consistency, validity, reliability and administration ease, making it a useful scale.
23
PHQ scores ≥10 have a sensitivity of 88% and a specificity of 88% for major depression. In the present study, we used a cut-off of a score of ≥10 as the presence of depression. The Hindi version of PHQ-9 was used in this study.
24
Generalised Anxiety Disorder Questionnaire-7 (GAD-7): The rated scale has seven items, each rated on a four-point scale (0–3) for the severity of the symptoms in the previous 2 weeks. A total of 5, 10 and 15 scores are taken as the cut-off for mild, moderate and severe anxiety, respectively. The threshold score of 10 is considered to have a sensitivity of 89% and a specificity of 82% for GAD.
25
In the present study, we used the cut-off score of 10 or more than 10 as the presence of anxiety disorder. IPV: A modified version of the domestic violence questionnaire (DVQ) by Morgan et al.
26
was used to assess IPV. DVQ has 21 items covering the three broad dimensions of IPV: physical violence, threatening behaviour and controlling behaviour.
27
In the present study, we assessed sexual violence by separating the items related to sexual violence from the physical violence domains. Each item was added to the questionnaire to evaluate violence during pregnancy and the general level of fearfulness in patients’ wives. All the items are answered as ‘yes’ or ‘no’. The scale screening was also identified with good reliability (α = 0.74). In the current study, we used the same Hindi version.
28
Those who responded yes to the item ‘ever experienced IPV’ were considered as the presence or absence of IPV; the same has been used in previous studies.
28
Statistical analysis: Frequencies and percentages were computed for categorical values, and mean and standard deviations were calculated for the continuous variable. Chi-square test and t-test were used for comparisons as per the requirement. Correlations among sociodemographic, clinical, PHQ-9, GAD-7 and IPV variables have been carried out using Pearson’s product-moment correlation.
Results
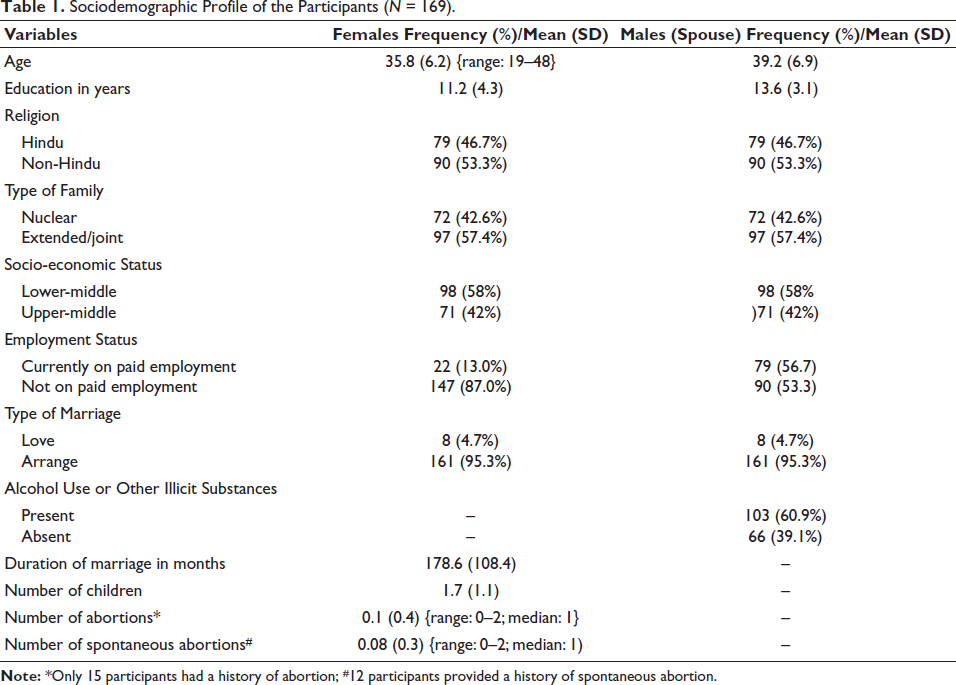
The mean age of the study’s participants was 35.8 years. The mean number of years of education was 11.2 years. More than half of the participants were from extended/joint families and belonged to non-Hindu religions from a lower-to-lower-middle socio-economic status. In total, 60.9% of the female spouses were consuming alcohol/illicit drugs. The rest of the details are given in Table 1.
Sociodemographic Profile of the Participants (N = 169).
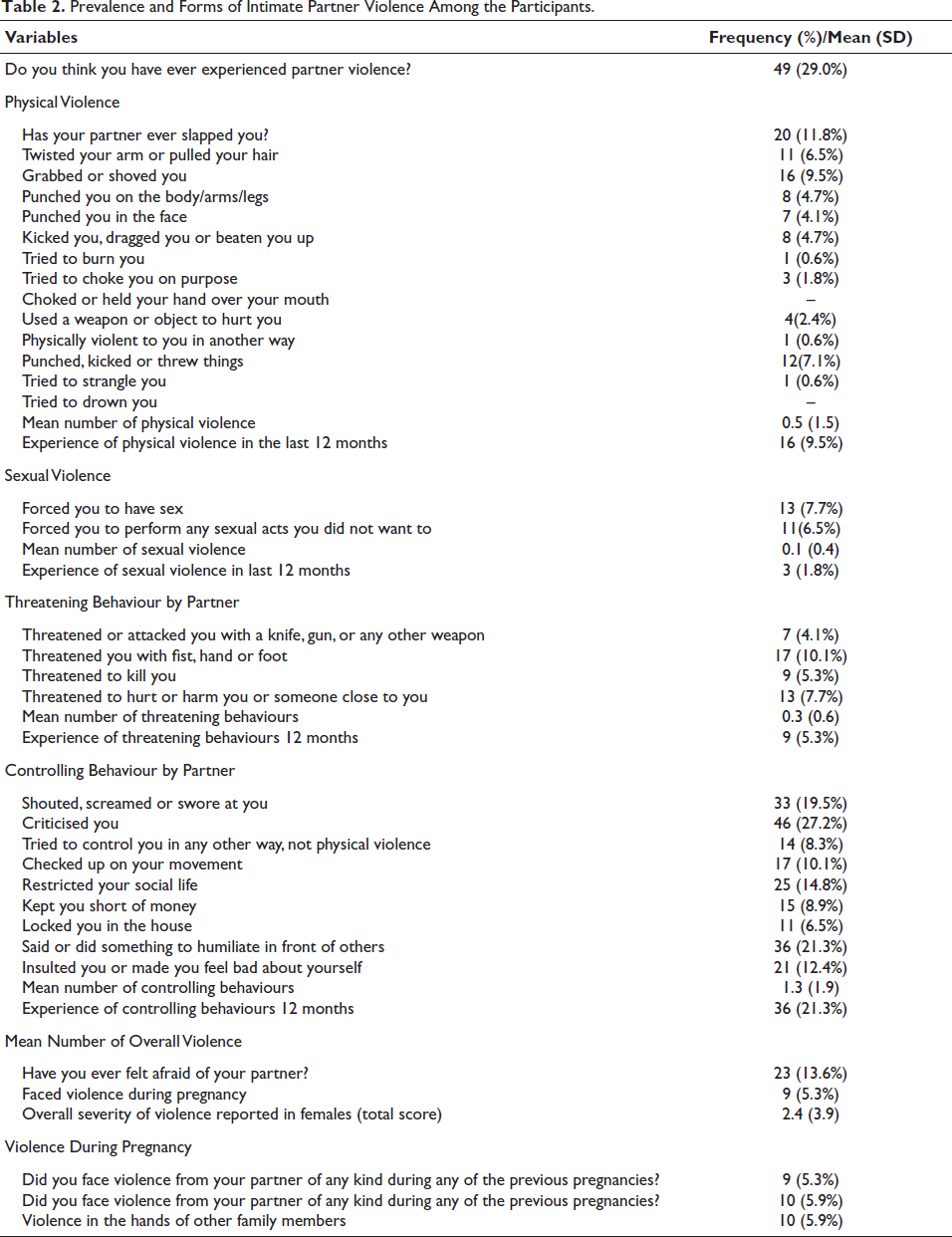
The prevalence of lifetime experience of IPV among the participants was 29.0%. Among the different types of IPV, controlling behaviour was most common, followed by physical violence and threatening behaviour, and the least common was sexual behaviour. The rest of the details are depicted in Table 2.
Prevalence and Forms of Intimate Partner Violence Among the Participants.
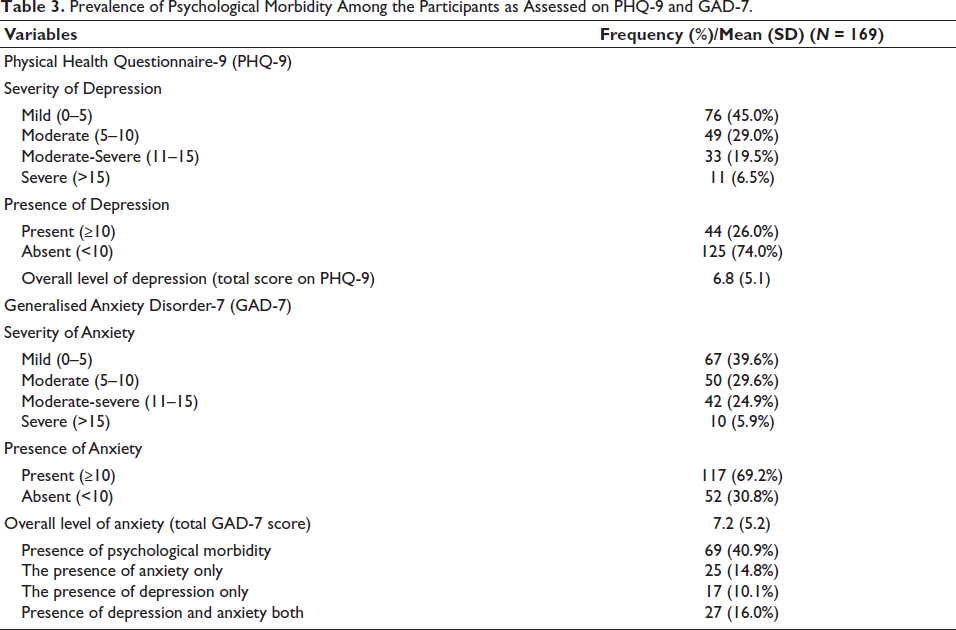
Regarding psychological morbidity, 26% had depression on PHQ-9, and 30.8% had an anxiety disorder assessed on GAD-7, as depicted in Table 3.
Prevalence of Psychological Morbidity Among the Participants as Assessed on PHQ-9 and GAD-7.
Correlation of Intimate Partner Violence (IPV) with Sociodemographic and Other Variables
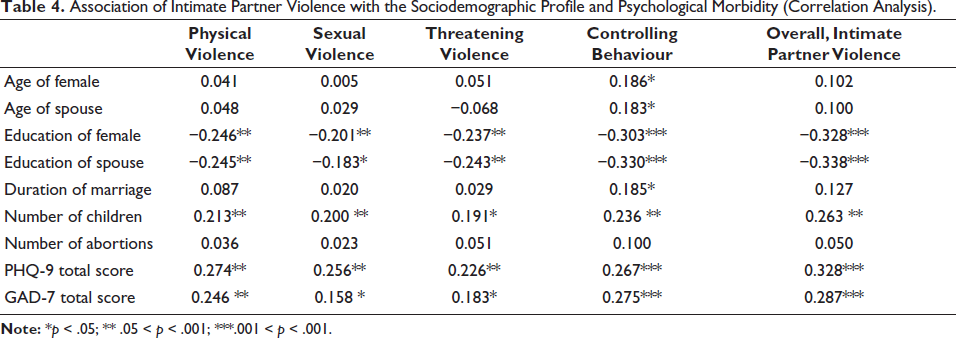
The number of years of education of the study’s participants and their spouses had a significant negative correlation with the mean of different types of IPV and total IPV, as shown in Table 3. The age of the study’s participant and their spouse and the duration of marriage had a significant positive correlation with controlling behaviour. The number of children had a significant positive correlation with the mean of different types of IPV and the total of IPV. The mean score of PHQ-9 and GAD-7 had a significant positive correlation with all the domains of IPV and the overall score. The rest of the details are depicted in Table 4.
Association of Intimate Partner Violence with the Sociodemographic Profile and Psychological Morbidity (Correlation Analysis).
Those participants whose husbands were consuming alcohol or any other illicit drugs reported a significantly higher experience of IPV (x2 = 31.441; p < .001***). Those from lower socio-economic status reported a significant level of partner violence (x2 = 25.099; p < .001***). Those who were in paid employment and their spouse who were in paid work reported a lower level of partner violence than those who were unemployed (x2 = 7.343; p = .007**) and their spouse who were unemployed (x2 = 9.156; p = .002**). The other sociodemographic factors had no association with the experience of violence.
Those females who experienced the violence were significantly more diagnosed with a depressive disorder (x2 = 26.174; p < .001***) and anxiety disorder (x2 = 10.743; p = .001**). This significant difference persisted even after controlling for factors like age, education, employment and substance use in the spouse.
Correlation
Predictors of Intimate Partner Violence (IPV)
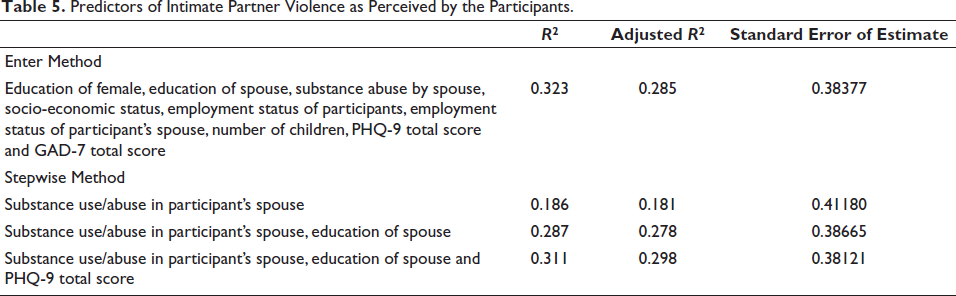
As evident from Table 5, when the enter method was used, 28.5% of the variance of IPV was explained by other variables. Among the various variables, the presence of substance use/abuse in the spouse emerged as the most important variable, followed by the spouse’s education and severity of depression. These results are depicted in Table 5.
Predictors of Intimate Partner Violence as Perceived by the Participants.
Discussion
The lifetime intimate partner prevalence in the current study was 29.0%, almost similar to the report of NFHS-4 (IIPS 2016) 10 conducted across different states of India. However, as per other studies conducted across India, the prevalence rate was reported to be 18%–70%.8,10,20,29–33 The inconsistencies in the previous studies might be because of various possible reasons, such as previous studies conducted in urban or clinical settings. The second reason could be that a majority of the studies studied IPV as part of domestic violence. The third reason could be that most studies did not use or translate the validated tool into colloquial languages. Fourth, many studies have methodological issues; untrained persons recruited patients. The advantage of the present study is that we used a validated tool, translated into colloquial language for a rural area, as per WHO guidelines and a trained health professional interviewed participants. Findings suggest that IPV is significantly high among rural married women in India. There is an unmet need to make them aware of the violence and preventive remedies. Empowerment through providing educational and employment opportunities can help women remain free from abusive relationships. Additionally, community programmes should be run through government or non-government organisations to make society aware of this evil devil. Healthcare professionals like Accredited Social Health Activists (ASHA) workers and auxiliary Nursing and Midwifery are the backbone of the community and have a strong connection with the community. These professionals should be trained to reach out to women in rural areas who are at risk of IPV. These professionals should be taught in screening for IPV and appropriate referrals to healthcare providers. Apart from the healthcare providers and healthcare settings, particularly reproductive care settings, the psychiatrist should play a significant role in reaching out to females who are at risk.
In terms of psychological morbidity, the women who had experienced IPV reported a higher level of depression and anxiety compared. The results of the present study align with those of the previous studies.1–3,22 The finding suggests that women with IPV should be screened for psychological morbidities like depression and anxiety, and vice versa, and should be provided with psychiatric health facilities in community healthcare settings. The healthcare team, researchers or the team of the NFHS should be sensitised toward the prevalence of common mental health problems among females with IPV.
In the present study, the prevalence of spousal IPV was significantly higher in wives of alcohol users or those who used other illicit drugs. Existing literature did not specifically assess spousal IPV among the wives of alcohol dependence. Hence, comparing the present study’s findings with the existing literature is tough. However, there is a general assumption that alcohol use is associated with a higher prevalence of IPV.20, 32, 34
Conclusion
It can be concluded that women from rural areas are at significant risk of IPV. This study helped us to better understand the prevalence of different types of IPV and the association of mental health with partner violence. In the present study, many women also reported depression and anxiety disorders, which have a strong association with IPV and further deserve more research, specifically longitudinal studies and clinical care. The presence of depression and anxiety disorders can be one of the presenting features of IPV. The presence of substance use/abuse spouses, low education or unemployment in females or their spouses can be other factors for the occurrence of IPV. There is a strong need to empower women by providing education and job opportunities. In addition, there is substantial demand from all the stakeholders, such as community health organisations, the NFHS, the Ministry of Family and Healthcare organisations or other government organisations, professional bodies or non-governmental organisations, to work in collaboration, which may take a pivotal role in research, prevention or early identification of IPV and identification of psychiatric problems among females with IPV.
Limitations of the Study
It was a cross-sectional study with a purposive sampling technique limited to a rural area. Hence, the study’s findings could not be generalised to other settings. Though the scale used in the current study has been validated and is reliable, it has not been validated for the rural population. The causal association between psychiatric problems and IPV could not be made, and hence, a futuristic longitudinal study is required. The other confounding variables that can affect the study’s findings, like personality traits of partners, psychiatric morbidity among the family members, financial constraints, social support, social and cultural acceptance of violence, pre- or extramarital affairs and others, were not taken into account. We did not include the severity of IPV. There is a chance that abused women could not reveal accurate information because of fear of disclosure. The confounding factors include choosing only one woman from one house, which we selected based on a lottery, which can influence the study findings. We also did not evaluate for psychiatric problems like PTSD, psychotic illness or mental retardation, which can have a strong association with IPV. Further research is needed to overcome all these limitations.
Footnotes
Acknowledgement
The authors are grateful to all the participants who contributed to the completion of the study.
Authors’ Contribution
Aseem Mehra: Conceptual designing, data analysis, framework and writing and proofing of the article.
Krishan Kumar: Conceptual designing, data analysis, writing and proofing of the article.
Sandeep Kaur and Tanvi Kiran: Data collection, data analysis, writing and proofing of the article.
Kapil Goel: Conceptual designing and data analysis.
Declaration of Conflict of Interests
The author declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article. Author Krishan Kumar is the co-Editor-in-Chief of Annals of Neurosciences. The authors did not take part in the peer review or decision-making process for this submission and have no further conflicts to declare.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Ethics
The Institute Ethics Committee approved the study.