
Abstract
Background
Borderline personality disorder (BPD) is a complex condition in which individuals often face significant challenges with low motivation and high ambivalence in treatment. The present study aimed to qualitatively explore the predictors of motivation to change in females with BPD through motivational interviewing (MI) as an adjunctive, pre-therapy intervention.
Purpose
In patients with BPD due to sudden shifts in mood there is lack of motivation and poor treatment adherence, resulting in poor prognosis. To enhance the treatment compliance and motivation in BPD patients the present study was designed to explore the predictors of motivation to change in patients with BPD with the help of Motivational Interview as an adjunctive therapy.
Methods
A qualitative design was employed, utilising Braun and Clarke’s (2006, Qual Res Psychol, 3, 2, 77–101) Thematic Analysis. A purposive sample of five BPD-diagnosed female participants, aged 20–35, was recruited from the Hospital for Mental Health, Ahmedabad, Gujarat. Participants underwent six to eight sessions of MI, followed by semi-structured interviews. Data were transcribed and analysed using an inductive thematic approach.
Results and Discussion
The analysis yielded a thematic framework of six interconnected themes, with participants moving ‘From Emotional Turmoil to Meaning-Making’, navigating the central conflict of ‘Struggling Between Hope and Helplessness’ (the nature of ambivalence) and contending with ‘Working Through the Wall’ (barriers to change). Forward momentum was driven by ‘Seeds of Motivation’ (internal and external factors) and facilitated by ‘Catalysts of Change’ (supports and small steps). ‘The MI Experience’ was identified as a primary predictor of change.
Conclusion
MI as a ‘therapeutic bridge’ for individuals with BPD may help them transition from self-blame to self-reflection and from ambivalence to action. It appears to be a valuable adjunct to enhance the effectiveness of intensive therapies.
Keywords
Introduction
Borderline personality disorder (BPD) is a complex mental health condition with a global prevalence of 1.8% in the general population. 1 The disorder is characterised by instability in affect, self-image issues and poor interpersonal relationships. BPD is theorised to result from a combination of early traumatic experiences, such as childhood abuse or neglect, and biological vulnerabilities, particularly in emotional regulation. This personality disorder is considered hereditary, as the genes run in families, with first-degree relatives showing a higher risk. It typically manifests in adolescence or early adulthood with a continuous course. 2 Both pharmacological and non-pharmacological treatment modalities are applied, but due to a lack of motivation, poor treatment adherence is present, and prognosis is generally poor. Dialectical Behaviour Therapy (DBT), 3 Mentalisation-based Therapy 4 and Schema Therapy 5 are the widely used psychotherapeutic models for managing the disorder. Despite overall promising outcomes, psychotherapy for BPD has notable limitations. Non-response rates remain high, ranging from 42% to 48% in specialised treatments to 64% in treatment-as-usual. 6 BPD-specific features, such as attention-seeking or relational indifference, higher baseline anger/hostility and impulsivity, high baseline depression, paranoia, preoccupied attachment style, and dismissive attachment, function as barriers to treatment engagement and continuation.7–9 Previous research on factors influencing treatment engagement and success in BPD has found that early therapeutic alliance in DBT significantly predicts dropout rate. 10 Literature has shown that higher pre-treatment symptom severity predicts greater symptom improvement, while stronger patient-rated therapeutic alliance predicts better outcomes. 11 Active engagement and participation in therapy require intrinsic motivation to learn skills and the application of learned skills, respectively. 12 In females, higher readiness to change suggests a greater willingness to engage in treatment processes. 13 Higher client commitment and perceived ability to work in DBT have been linked to fewer suicide attempts. 14 For bringing change through therapy, patients’ intrinsic motivation and commitment to change are required, so motivational interviews may be the cornerstones for the better outcome of any therapy. The essence or ‘spirit’ of motivational interviewing (MI) has been explained by Miller et al.15, 16 based on the intentionality of three therapeutic behaviours: ‘actively collaborating with clients, eliciting from clients their strengths and resources, and honouring client autonomy or decision-making’. 17 Four guiding principles lead this method: express empathy, develop discrepancy, roll with resistance and support self-efficacy. Five ‘early’ methods are used in the practice of MI: OARS (Open questions, Affirming, Reflecting and Summarising) techniques and Eliciting Change Talk. The first four methods (OARS) are a set of client-centred counselling skills that are used right from the start. The therapist elicits change talk by encouraging clients to state both sides of ambivalence and highlight discrepancies between current behaviour and personal values or goals. Strategies to elicit change talk include decisional balance, double-sided reflections, querying extremes, contemplating past and future, importance and confidence rulers, and exploring values. 15 While Phase 1 of MI involves building intrinsic motivation for change, Phase 2 transitions the client into strengthening their commitment to change. The therapist ensures the adoption of a balanced approach by avoiding the prescription of a rigid plan that the client is not ready for, or being passive by withholding guidance. 15 Keeping this in view, the present study was conducted with the aim of exploring the predictors of motivation to change with the help of MI as an adjunctive pre-therapy intervention.
Methods
The study was conducted at the National Forensic Sciences University, Gandhinagar, Gujarat, with data collection occurring at the Hospital for Mental Health, Ahmedabad. It took place between March and July 2024, with a 5-month data collection period. Through the purposive sampling method, a total of five female participants between 20 and 35 years, fulfilling the International Classification of Diseases-10, Diagnostic Criteria for Research (ICD-10, DCR) 18 and the International Personality Disorder Examination (IPDE) 19 cut-off score for BPD were taken for the study. Written informed consent was received from all the participants. A qualitative approach was selected to capture in-depth, nuanced insights into the participants’ lived experiences.
Procedure
The objective of the study was to explore the predictors of motivation to change in individuals with BPD through motivational interviews. To execute the study, first, a semi-structured interview schedule was prepared. Further, this schedule was reviewed by the subject experts, co-authors and supervisor of the present study. The interview schedule was assessed on the parameters related to comprehension, relatedness as per the study objectives, as well as the nature of the questions (open-ended questions were framed). Then, it was finalised for the present study. Following screening, participants underwent an MI intervention, spanning six to eight sessions from building rapport to working through ambivalence to facilitate change. For the motivational interview, a manual for MI was used. 16 Semi-structured interviews were then conducted, guided by an interview protocol designed to explore themes relevant to the research objectives. Interviews were audio-recorded with participants’ consent.
Data Analysis
An inductive approach using thematic analysis was employed to identify and analyse emergent themes from the interview data. 20 This process began with the verbatim transcription of all audio-recorded interviews. Following transcription, each transcript was translated into English language for efficient understanding and analysis of the content. The initial phase involved familiarisation with the depth of the participants’ experiences before the formal process of coding began. Descriptive codes were generated from the data set, which were further manually screened to organise the large list into smaller chunks relevant to the research questions. Codes that appeared to share a unifying construct or addressed a similar aspect of the data were organised into potential themes. The iterative process of reviewing themes, defining and naming themes, and producing the final report was conducted to ensure contextual sensitivity and accurate reflection of the participants’ experiences.
Results
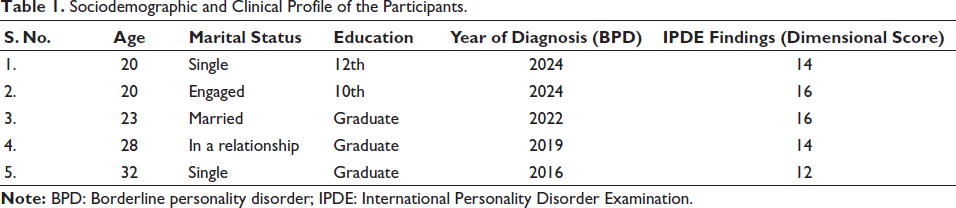
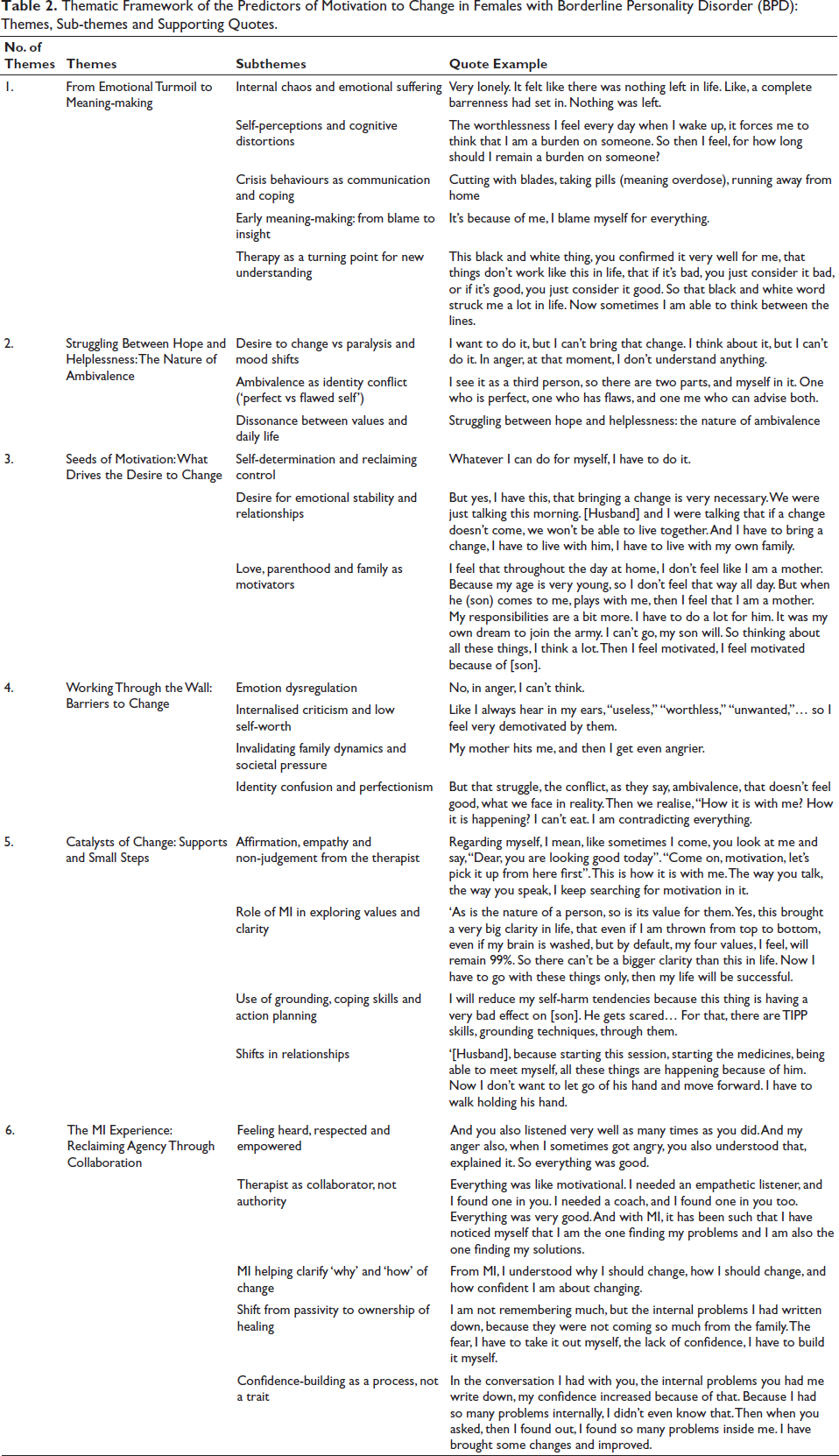
Description of the sociodemographic and clinical variables of the participants, such as age, gender, education, marital status, year of diagnosis and IPDE scores, is depicted in Table 1. After six to eight sessions of MI, a semi-structured interview was conducted through the interview schedule, which was prepared to explore the predictors of motivation to change in patients with BPD. Six themes resulted from this process, with 24 subthemes. Table 2 exemplifies the overarching themes, constituent subthemes and a representative verbatim quote example. This illustration provides a comprehensive summary of the thematic framework developed from the analysis of the data to understand the participants’ experiences with MI and the resulting predictors of motivation to change.
Sociodemographic and Clinical Profile of the Participants.
Thematic Framework of the Predictors of Motivation to Change in Females with Borderline Personality Disorder (BPD): Themes, Sub-themes and Supporting Quotes.
Discussion
The current study utilised MI as an adjunctive treatment modality to understand its experiential effect on individuals diagnosed with BPD. The research sought to streamline its focus on how the client-centred counselling approach influenced motivation, ambivalence, values clarity and therapeutic engagement. Using a qualitative, thematic analysis of semi-structured interviews, six overarching themes emerged: (a) From Emotional Turmoil to Meaning-Making, (b) Struggling Between Hope and Helplessness: The Nature of Ambivalence, (c) Seeds of Motivation: What Drives the Desire to Change, (d) Working Through the Wall: Barriers to Change, (e) Catalysts of Change: Supports and Small Steps and (f) The MI Experience: Reclaiming Agency through Collaboration.
From Emotional Turmoil to Meaning-making
The first theme illustrates the transformation from initial emotional chaos to eventual steps towards psychological insight. Participants described overwhelming internal distress, including feelings of emptiness, abandonment and intense emotional pain, consistent with established symptom profiles of BPD.2, 21 Unhealthy, high-risk behaviours such as self-harm and suicidal ideation were mostly described as strategies to communicate distress, regulate emotion or exert control—findings echoed in prior literature emphasising affective dysregulation and maladaptive coping in BPD.22, 23
The subtheme ‘Crisis behaviours as communication and coping’ reflects the complex relationship between self-harm and emotional regulation documented in BPD literature. Recent ecological momentary assessment studies have shown that non-suicidal self-injury contributes to short-term affect stabilisation in people with BPD. 24 The MI approach appeared to help participants reframe these behaviours as adaptive attempts at coping rather than pathological acts deserving of shame, facilitating the meaning-making process.
The subtheme ‘Therapy as a turning point for new understanding’ emphasised how participants began to reconceptualise their suffering through therapy. The MI process, with its emphasis on client autonomy and empathy, facilitated psychological shifts in self-perception. 15 For example, participants described moments when the therapist’s reframing of blame and responsibility allowed them to develop insight without triggering self-blame, criticism and negative self-evaluation. These findings align with prior studies showing that acknowledgement of internal experience, when met with validation, can initiate cognitive restructuring and reduce internalised stigma. 25
Struggling Between Hope and Helplessness: The Nature of Ambivalence
The second theme explores the push–pull between wanting to change and feeling stuck due to internal conflict, mood instability, and fear. This duality aligns with the paradoxical nature of motivation in BPD, where emotional volatility and fear of abandonment coexist with a deep yearning for stability and growth. 26 The theme’s title captures what might be considered the hallmark experience of BPD—simultaneous hope and despair that creates a paralysing ambivalence about change.
The subtheme ‘Ambivalence as identity conflict (Perfect vs Flawed Self)’ reflects what Kernberg 27 termed identity diffusion and is supported by work showing that resolving internal splits is fundamental to therapeutic progress in individuals with BPD.28, 29 Participants described experiencing multiple, contradictory selves that seemed to be in constant conflict. This internal dialogue was not merely cognitive but deeply emotional, involving competing value systems and behavioural impulses. One participant’s description of having ‘a perfect self, a flawed self, and an advising self’ illustrates the complex internal negotiations that characterise the emotionally unstable disorder.
This finding is particularly relevant to MI practice, as traditional approaches to ambivalence resolution may be insufficient for the level of identity fragmentation present in BPD. This suggests that MI techniques, like decisional balance and exploring consequences of change/non-change, helped clarify these conflicting positions by providing structure for what was otherwise a chaotic internal experience.
Seeds of Motivation: What Drives the Desire to Change
The third theme captures what internally and externally motivates change: relationships, self-worth, purpose and reclaiming agency. Many participants described a transition from externalised distress to a more reflective stance on change. MI’s strategic use of change talk, personalised goal setting and reflective listening seemed to activate intrinsic motivation, aligning with Self-determination Theory, which posits that autonomy, relatedness and competence are foundational for internal motivation.15, 30, 31
The subtheme ‘Self-determination and reclaiming control’ reflects the profound impact of supporting autonomy in individuals who often feel powerless. Research has consistently shown that autonomous motivation for treatment is associated with better outcomes. 31 For BPD specifically, where individuals often feel controlled by their emotions, impulses and interpersonal dynamics, the experience of making autonomous choices in therapy can be transformative.
Van der Kaap-Deeder 32 proposed that emotion regulation difficulties in BPD can engender feelings of helplessness, failure, and social isolation, which increase borderline features. The current study’s findings suggest that MI’s support for autonomy may help interrupt this cycle by restoring a sense of agency and self-efficacy.
The subtheme ‘Love, parenthood and family as motivators’ emerged as particularly powerful for several participants. The desire to be a good parent or partner provided concrete, meaningful goals that could sustain motivation through turbulent phases of life. This finding aligns with research on values-based interventions, which show that connecting behaviours to deeply held values increases motivation and persistence. 33
Working Through the Wall: Barriers to Change
The fourth theme describes the psychological and environmental barriers to change: emotional overwhelm, perfectionism, invalidation and stuck patterns. The subtheme ‘Emotion dysregulation’ captures what many consider the core feature of BPD. Participants’ descriptions of being unable to access skills when angry align with research on emotional hijacking and the neurobiological basis of BPD. 23
Importantly, participants did not just describe emotional intensity but the way emotions seemed to disable their capacity for reflection and choice—a finding that has significant implications for treatment timing and pacing. Traditional MI approaches may need modification for individuals whose emotional states can completely overwhelm cognitive functioning.
The subtheme ‘Internalised criticism and low self-worth’ reflects the shame-based core beliefs that often drive BPD symptoms. Research consistently shows that shame is particularly problematic in BPD, associated with self-harm, interpersonal difficulties and treatment dropout. 22 However, the same research suggests that adaptive guilt—which focuses on specific behaviours rather than global self-condemnation—may actually be protective. 34 MI’s emphasis on separating the person from the problem may help foster this more adaptive form of self-evaluation.
The subtheme ‘Invalidating family dynamics and societal pressure’ highlights the environmental factors that maintain BPD symptoms. Linehan’s 4 biosocial theory emphasises the role of invalidating environments in BPD development, and the current findings show how these dynamics continue to impact change efforts in adulthood. Family members’ lack of understanding, criticism and even well-meaning pressure appeared to derail motivation for change.
Research on adolescent BPD has shown that family engagement significantly impacts treatment outcomes, and similar dynamics may persist into adulthood. 35 This finding has important implications for MI practice with BPD, suggesting that family involvement, or at least environmental assessment, may be crucial.
Catalysts of Change: Supports and Small Steps
The fifth theme highlights the emotional and practical supports that help initiate change: empathy, MI, small wins and new patterns. The subtheme ‘Affirmation, empathy and non-judgement from the therapist’ aligns with extensive research on therapeutic alliance in BPD treatment. Studies consistently show that therapist warmth, empathy and validation are crucial for engaging individuals with BPD.10, 14
What emerged as particularly important in this study was the timing and specificity of affirmations. Participants described how even small compliments from the therapist could serve as ‘motivational anchors’ during difficult periods. This finding suggests that MI’s emphasis on affirmations may be especially powerful for individuals with BPD, who often struggle with self-worth and may be hypersensitive to interpersonal cues.
The subtheme ‘Role of MI in exploring values and clarity’ captured participants’ experience of the MI process as uniquely clarifying. Unlike previous therapy experiences that participants described as confusing or overwhelming, MI seemed to provide structure for exploring internal experience without imposing external goals. The collaborative nature of MI appeared to address the autonomy needs that are often threatened in BPD treatment.12, 25
The subtheme ‘Small behavioural steps and new goal pursuit’ reflects the importance of achievable goals in maintaining motivation. Participants described how small changes—like improving appearance or leaving the house more often—could create positive feedback loops that sustained larger change efforts. This finding aligns with behavioural activation principles and supports the MI emphasis on change talk and commitment to small, specific steps.
The Motivational Interviewing Experience: Reclaiming Agency Through Collaboration
The sixth theme describes MI as a transformative relational experience that fosters agency, clarity and a sense of being truly heard. The subtheme ‘Feeling heard, respected and empowered’ captures what participants described as a fundamentally different therapeutic experience. Unlike previous treatments that felt authoritarian or invalidating, MI was experienced as collaborative and respectful.
This finding is particularly significant given research showing that individuals with BPD are often stigmatised in healthcare settings and may have histories of invalidating therapeutic relationships, as cited in van Beek and Verheul’s study. 13 The MI emphasis on partnership and respect for client autonomy appeared to provide a corrective experience that itself became therapeutic.
The subtheme ‘Therapist as collaborator, not authority’ reflects a shift in the power dynamic that participants found empowering. Rather than feeling like passive recipients of expert intervention, participants described feeling like active partners in their own healing. This shift appeared crucial for individuals whose sense of autonomy may have been repeatedly violated in relationships.
The subtheme ‘Shift from passivity to ownership of healing’ captures what may be the most significant outcome of the MI process—a fundamental change in how participants understood their role in recovery. The quote ‘I am not remembering much, but the internal problems I had written down, because they were not coming so much from the family. The fear, I have to take it out myself, the lack of confidence, I have to build it myself’, exemplifies this shift towards self-efficacy and personal agency.
Conclusion
The findings suggest that autonomous motivation is associated with better treatment outcomes. It also resonates with recovery-oriented approaches that emphasise personal empowerment and self-direction. This study offers first-person accounts of how individuals with BPD experience MI and its impact on motivation, ambivalence, values clarity and steps towards change. By validating client experiences, supporting autonomy and facilitating values clarification, MI appears to help clients develop the internal resources necessary for sustained change. They suggest that addressing motivational barriers may be as important as teaching coping skills or processing trauma in BPD treatment. For practitioners working with individuals with BPD, even brief MI interventions may help establish a therapeutic alliance, clarify treatment goals and enhance motivation for change. Most importantly, they demonstrate that individuals with BPD are not inherently unmotivated or untreatable, but rather may require approaches that honour their complexity, validate their experiences, and support their inherent capacity for growth and healing. Future research should aim to validate these findings in larger, more diverse samples and employ mixed-methods designs to triangulate qualitative insights with quantitative measures.
Footnotes
Authors’ Contribution
Shrawasti Lavanya contributed to the concept of study, data collection, evaluation and interpretation and write up of the study.
Soniya Vats contributed in designing and supervising the study, Allocation of the patients, Structure, organization and review of the study and proceedings for the publication.
Vinod Sanwal has given his expert input to finalize the study.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Ethics
Not applicable.