
Abstract
Objectives
Linagliptin reduces blood glucose levels, but its efficacy in brittle diabetes mellitus with early diabetic nephropathy (BDM-EDN) remains unclear. Therefore, this study investigated the efficacy and safety of linagliptin in BDM-EDN treated with Dendrobium polysaccharide extract.
Materials and Methods
From January 2020 to December 2022, 90 BDM-EDN patients admitted to the endocrinology department of our hospital were selected and equally divided into a control group, a Dendrobium polysaccharide (10 mg/d) group, and a Dendrobium polysaccharide (10 mg/d) + linagliptin (5 mg/d) group using a random number table method. After 12 weeks of continuous treatment, serum indicators were measured, and an enzyme-linked immunosorbent assay (ELISA) was used to examine the levels of inflammatory factors. Polymerase chain reaction (PCR) detected HMGN1 and toll-like receptor 4 (TLR4) expressions. Fifteen BDM-EDN model mice were constructed and equally divided into Dendrobium polysaccharide (10 mg/d) + CRX-527 (an agonist of the HMGN1/TLR4 pathway, 0.1 mg) group and Dendrobium polysaccharide (10 mg/d) + TAK-242 (inhibitor of HMGN1/TLR4 pathway) group. The expression differences of the HMGN1/TLR4 pathway in mice were observed in the 0.1 mg group and the Dendrobium polysaccharide (10 mg/d) + linagliptin (5 mg/d) + TAK-242 (0.1 mg) group.
Results
Compared with the control group, the biochemical indexes were significantly reduced in the Dendrobium polysaccharide group, while the anti-inflammatory factor interleukin (IL)-10 was elevated (p < .05). Compared with the Dendrobium polysaccharide group, biochemical indexes, renal function indexes, and inflammatory factors were all reduced in the Dendrobium polysaccharide + linagliptin group (p < .05). Both Dendrobium polysaccharide and linagliptin had inhibitory effects on HMGN1/TLR4 levels. In comparison with the Dendrobium polysaccharide group, FPG and 2hPBG decreased; urinary albumin excretion rate (UAER), Cys-C, and C-reactive protein (CRP) decreased; and IL-10 increased in the Dendrobium polysaccharide + TAK-242 group (p < .05).
Conclusion
Linagliptin combined with Dendrobium polysaccharide extract can modulate the blood glucose level of BDM-EDN patients, improve UAER by decreasing inflammatory response, and protect renal function.
Introduction
The number of global diabetic patients reached 250 million in 2010, and the incidence of diabetes mellitus is still increasing year by year. With the development of the disease, it may also lead to a variety of complications, among which diabetic nephropathy is one of the most common chronic complications and is also the cause of end-stage renal disease (ESRD). Diabetes mellitus is also one of the main causes of death in patients (Dai et al., 2018; Ding & Wong, 2012; Srinivasan et al., 2017; Williams et al., 2004). Brittle diabetes mellitus is a special type of diabetes mellitus with characteristics including proneness to hypoglycemia and ketoacidosis, bipolarity, large fluctuations of blood glucose, and also proneness to short-term diabetic microvascular complications (Ling et al., 2012; Mattila & de Boer, 2010). Therefore, the treatment and management of brittle diabetes mellitus with early diabetic nephropathy (BDM-EDN) patients is more difficult. Currently, many hypoglycemic agents have certain adverse effects and limitations, so there is a need to find safer and more effective treatments.
Recent studies have shown that Dendrobium polysaccharide (DOP) is one of the main bioactive components of Dendrobium, possessing several activities such as anti-oxidant, hepatoprotective, immunomodulatory, gastrointestinal protection, hypoglycemic, and anti-tumor properties (Figure 1; Liu et al., 2019). Dendrobium officinale leaf polysaccharides ameliorated type 2 diabetes mellitus in mice (Jia et al., 2017) and, at the same time, had a strong anti-oxidant effect on pancreatic islet cells, which not only reduces the damage of free radicals on pancreatic islet function but also promotes the release of pancreatic islet B cells and increases insulin synthesis, and also has an extra-pancreatic hypoglycemic effect (Cao et al., 2013, 2019). In addition, a randomized, double-blind, placebo-controlled clinical study showed anti-aging effects of D. officinale and its fermented version on human skin, highlighting a notable contribution to dermatological research (Na et al., 2024). Moreover, DOPs can regulate TET2 function and protect against neuronal apoptosis (Wu et al., 2018). Therefore, it is important to study the therapeutic mechanism of DOPs in diabetes.
Diagram of the Dendrobium Polysaccharide Extraction Process.
Linagliptin tablets are a novel hypoglycemic agent that can improve glycemic control in type 2 diabetes patients. It is a novel oral glucose-lowering drug based on enteroglucagon, which is currently attracting much attention (Forst et al., 2010) as it can reduce the level of glucagon-like peptide-1 (GLP-1) in the body by inhibiting DPP-4, thus elevating the level of endogenous GLP-1, increasing insulin secretion, and inhibiting glucagon secretion, thereby achieving glycemic control (Morales, 2011). DPP-4 inhibitors are utilized for hypoglycemic treatment of type 2 diabetes (Deacon & Lebovitz, 2016; Loh et al., 2016). Some studies have shown that DPP-4 inhibitors may have a renoprotective effect through a GLP-1 non-dependent pathway (Abe & Okada, 2015).
Several studies have confirmed that DPP-4 inhibitors have a protective effect on diabetic nephropathy, which can stabilize a patient’s blood glucose, reduce the incidence of glucose fluctuation and hypoglycemia, improve the patient’s body weight, and protect pancreatic function. However, there are still fewer studies on brittle diabetes mellitus combined with early-stage nephropathy. The islet function of this kind of patient is poorer, and their complications appear earlier. Whether the application of DPP-4 inhibitors is effective needs to be clinically verified. Meanwhile, high-mobility group nucleosome-binding protein 1 (HMGN1) is a nuclear non-histone protein that modulates chromatin structure to regulate inflammatory gene expression. Toll-like receptor 4 (TLR4), a key receptor in innate immunity, promotes NF-κB pathway activation upon stimulation, leading to the release of inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin (IL)-6. Recent studies have demonstrated that the HMGN1/TLR4 pathway is hyperactivated in diabetic nephropathy and closely associated with glomerular fibrosis and podocyte injury (Abe & Okada, 2015). Furthermore, in brittle diabetes, glycemic variability exacerbates oxidative stress and inflammatory responses, resulting in dysregulated energy homeostasis in adipose tissue. This metabolic disturbance causes abnormal activation of the HMGN1/TLR4 pathway and accelerates renal damage (Abe & Okada, 2015). Therefore, this study investigated the efficacy and safety of linagliptin versus DOP extract in BDM-EDN treatment and analyzed the mechanistic role of the HMGN1/TLR4 pathway in this process, providing new insights about targeted therapy in such patients.
Materials and Methods
Experimental Materials
The following apparatus and reagents were used in this study: Linagliptin (Shanghai Boehringer Ingelheim Pharmaceuticals Co., Ltd, batch no. 462469H); DOP extract (Shaanxi Snout Bio, CAS: 2115-91-5), a dendrobium extract known for its efficacy in improving human metabolism, lowering blood sugar, and anti-tumor effects; HMGN1 (Phosphorylated S20/S24, Shanghai Chunmai Biotechnology Co., Ltd); polyclonal antibody (HMGN1 antibody, Eimage Technology, CAS: PAB10016); EPR2078Y (TLR4 antibody, Eimage Technology; CAS: ABP57210); CRX-527 (HMGN1/TLR4 pathway agonist, Shenzhen Xinbosheng Biological, CAS: tlrl-crx527); TAK-242 (HMGN1/TLR4 pathway inhibitor); HMGN1/S24 (phosphorylated S20/S24, Shanghai Chunmai Biological Technology Co., TLR4 pathway inhibitor, Shanghai Weihuan Biological, 243984-11-4); blood glucose meter (Guangdong Goukang Biotechnology Co., Ltd); RNA extraction kit (Shanghai Yuduo Biological); reverse transcription kit (GeneCopoeia, USA); and enzyme-linked immunosorbent assay (ELISA) kit (Jingle Biological). The plant diagram and molecular formula of DOP are shown in Figure 2.
Dendrobium Plant Map.

In this study, the clinical research was approved by the Hospital Ethics Committee (HEA-20210206E) and registered with the Chinese Clinical Trial Registry. Animal experiments were conducted in accordance with SPF-level animal ethics norms (Ethics number: LGD20250201).
General Data
A total of 90 BDM-EDN patients admitted to the Department of Endocrinology of our hospital from January 2020 to December 2022 were selected, including 53 males and 37 females (average age: 50.67 ± 10.28 years). Inclusion criteria included (a) meeting diagnostic criteria; (b) not having cardiac insufficiency, hypertension, or primary renal disease; (c) maintaining normal blood urea (BUN) and creatinine (SCr) levels in compliance with diagnostic criteria for early DN by WHO in 2006; (d) not being affected by diabetic nephropathy. Patients with acute complications such as ketoacidosis and hyperosmolar coma were excluded. Exclusion criteria involved (a) heart disease, renal failure, and patients with malignant tumors or malignant disease and (b) long-term use of glucocorticosteroids and other patients affecting glucose metabolism, and recent use of angiotensin-converting enzyme inhibitor (ACEI) or ARB affecting urinary albumin excretion rate (UAER).
The patients were then divided into a control group, DOP group, and DOP + linagliptin group by using the randomized numerical table method. The basic data showed no differences among the three groups (p > .05).
Intervention Method
After admission to the hospital, all enrolled patients stopped using the original glucose-lowering program and switched to insulin (recombinant glucagon insulin combined with menthyl insulin) and Benadryl in order to improve renal artery pressure treatment. They also followed a strict diet and did appropriate exercise. After achieving stable blood glucose levels, the DOP group received oral DOP (10 mg/day) as an add-on therapy. The combination group received DOP (10 mg/day) + linagliptin (5 mg/day) for 12 weeks.
The index levels of fasting blood glucose (FPG), 2 h postprandial blood glucose (2hPBG), glycosylated hemoglobin (HbA1c), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), triglyceride (TG), UAER, and Cys-C were detected.
The capillary blood of patients was collected from the fingertips to check FPG and 2hPBG: blood glucose test by glucometer; HbA1c: ion exchange chromatography method; TC, TG: enzyme method; LDL-C: direct measurement method; UAER, Cys-C: immunoturbidimetric method.
ELISA
A 100 µL of antigen solution was added and each sample corresponded to a blank well, followed by the addition of 200 µL of blocking solution to block the unbound sites. The plate was then washed to remove unbound blocking solution and antigen. Next, 100 µL of the sample to be tested was added to each well, followed by the addition of standard and quality control samples at the same time, and the setting up of blank wells. The plate was incubated after sealing for 1 h, followed by washing the plate to remove unbound samples and quality control samples. A 100 µL of development solution was then added for 30 min, followed by the addition of 50 µL of termination solution to each well and mixing well. The optical density was then measured using an ELISA reader.
Western Blot Detection of HMGN1, TLR4 Protein Expression
Peripheral blood single-nucleated cells were isolated using human peripheral blood cell isolation solution, and the cells were lysed using cell lysis solution to obtain protein samples that were quantified using a protein quantification kit. Protein samples were electrophoresed and transferred to nitrocellulose membranes. The nitrocellulose membrane was blocked and incubated with primary antibody (EPR26772-17, 1:200 dilution, EPR2078Y, 1:150 dilution). The next day, the cells were incubated, and the membrane was washed three times, followed by the addition of rabbit secondary antibody (1:10,000) and incubation for 1 h (37°C), washing with phosphate-buffered saline (PBS) three times, and observation of ImageJ images.
Polymerase Chain Reaction (PCR) Detection
Human peripheral blood cell isolation was used to isolate peripheral blood single-nucleated cells, followed by fluorescence quantitative PCR detection of HMGN1 and TLR4 mRNA (QIAGEN), including mRNA extraction, reverse transcription to cDNA, and fluorescence quantitative PCR. The specific sequences of primers are shown in Table 1.
Primer Sequences.

Mouse Model Construction and Grouping
SPF grade, male, C57BL/6J mice (15 in number) were selected for the study. A high-fat/sugar diet was given to them and before the experiment, FBG was measured in all mice, and the mice were required to have an FBG <7 mmol/L to exclude the mice with congenital blood glucose abnormality. The model group was fed with a high-fat/sugar diet for 8 weeks, and their body weight was measured regularly to exclude mice with substandard body weight. Mice with body weight greater than or equal to that of the control group were screened, while those with substandard body weight were eliminated, suggesting that they were tolerant to or insensitive to the induction of obesity. After 8 weeks of high-fat and high-sugar diet feeding, mice were weighed and eliminated from the obesity-induced tolerant mice, FBG was measured, and an oral glucose tolerance test (OGTT) was performed. Model mice were made to fast for 16 h after 1 d of resumption of a high-fat/sugar diet. They were injected with STZ at 50 mg/kg per day, and the STZ was 0.1% and citric acid was 0.5%. The STZ injection solution was prepared with 0.1% citrate buffer (pH 4–5). The mice were fasted during the day and injected at night for 5 days. FBG >16 mmol/L was regarded as the success of the construction of the medium-term diabetes model. The mice were reared for 8 weeks, and blood from the tail vein was collected for the detection of various indices.
Mice were grouped as follows: DOP + CRX-527 group: DOP 10 mg, CRX-527 0.1 mg; DOP + TAK-242 group: DOP 10 mg and TAK-242 0.1 mg; DOP + linagliptin + TAK-242 group: DOP 10 mg, linagliptin 5 mg, and TAK-242 0.1 mg.
Statistical Methods
All data were processed by SPSS 25.0 and GraphPad Prism 8.0 software. Measurement data were expressed as mean ± standard deviation (mean ± SD). The comparison between the two groups was performed using the independent sample t-test (normal distribution) or the Mann–Whitney U-test (non-normal distribution). The homogeneity of variance least significant difference (LSD) t-test was performed after the one-way analysis of variance for multi-group comparisons. All statistical tests were two-sided tests. A p value < .05 was considered statistically significant.
Results
Clinical Observation of Linagliptin Promotes the Ameliorative Effect of DOP Extract on BDM-EDN
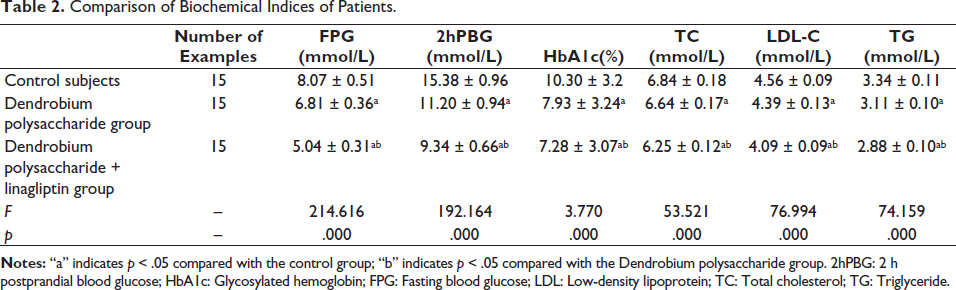
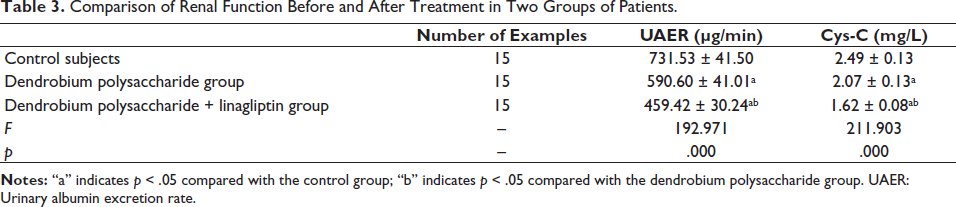
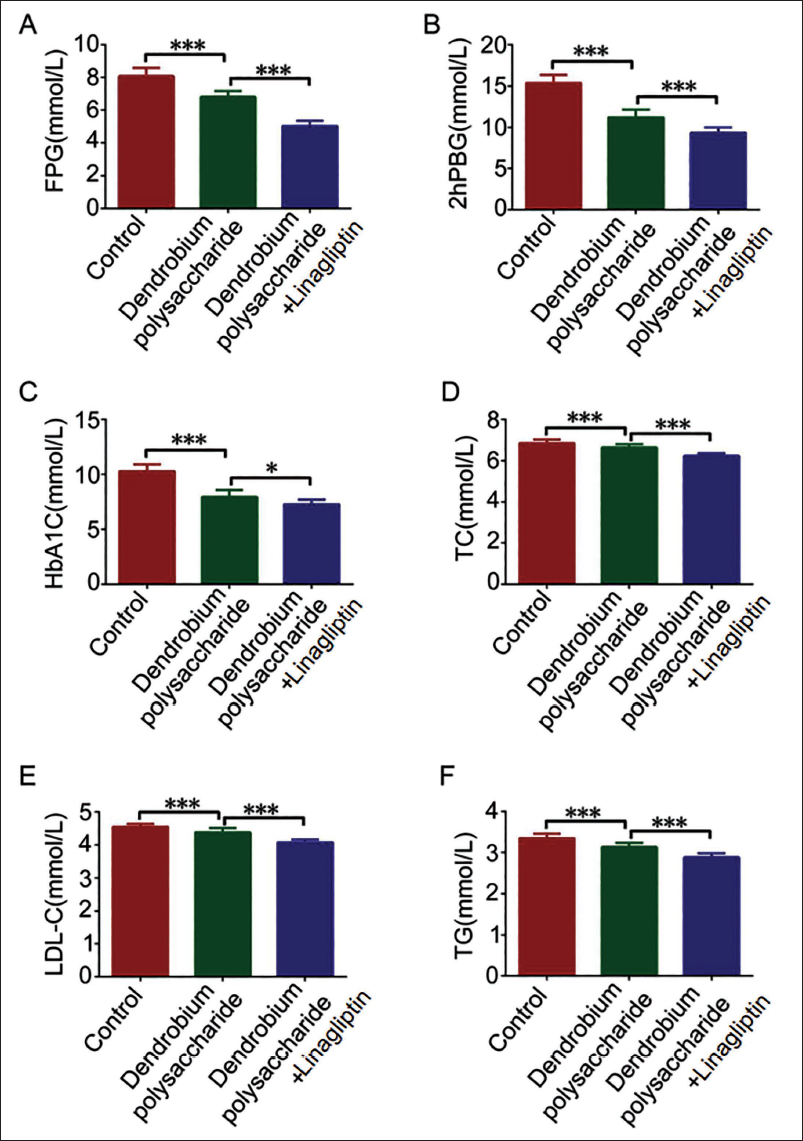
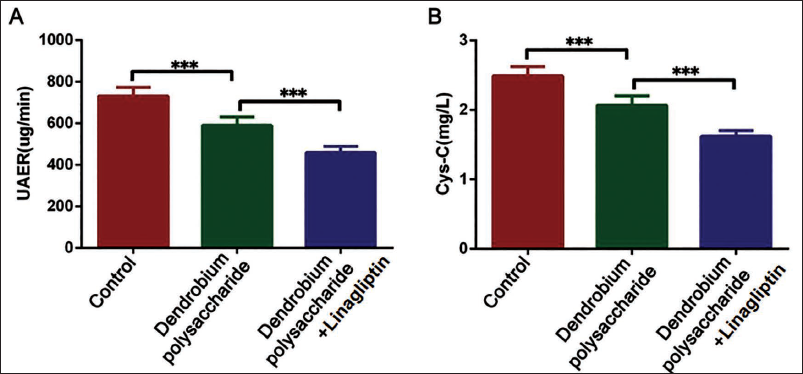
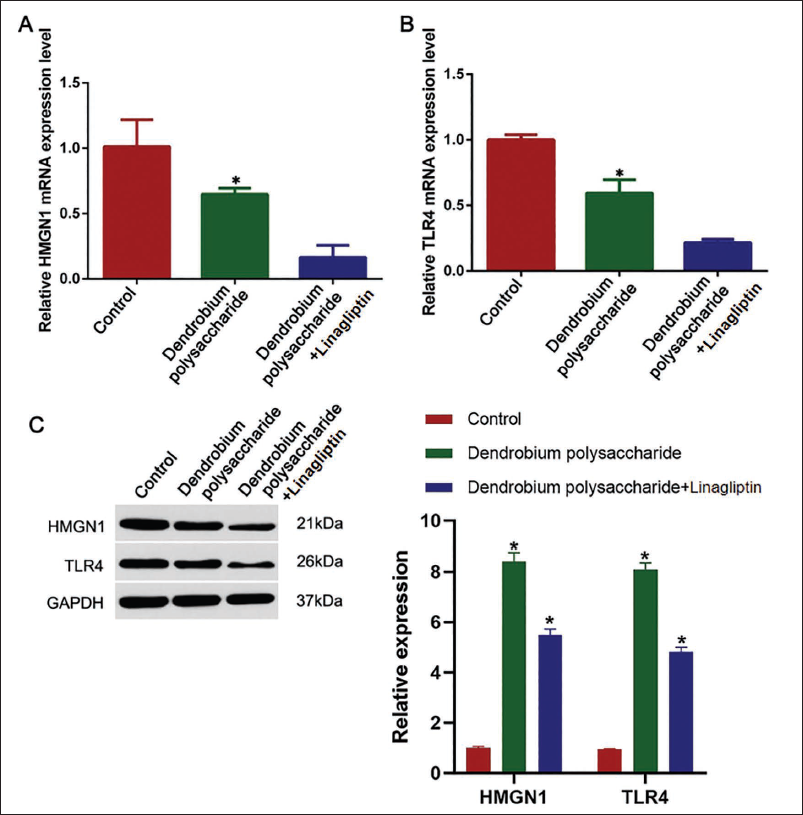
In order to investigate the effects of linagliptin and DOP extract on diabetic nephropathy, we found that patients’ biochemical indexes showed a significant trend of decreased FPG, 2hPBG, and HbA1c blood glucose, and the patients’ lipid index levels showed the same changes (Table 2, Figure 3A–3F). Further investigation found that the levels of UAER, Cys-C, and two renal function indexes showed a decreased trend (vs. other groups, p < .05, Table 3, Figure 3A–F) in BDM-EDN patients under DOP + linagliptin intervention. It was further found that the levels of UAER and Cys-C in patients showed a decreased trend under DOP + linagliptin intervention (vs. other groups, p < .05, Table 3, Figure 4A–B), and the levels of CRP, IL-6, and TNF-α were reduced significantly, whereas IL-10 increased (vs. DOP group, p < .05, Table 4, Figure 5A–5D). The levels of UAER and Cys-C in patients with early diabetic nephropathy showed similar changes in this case (5A–5D). We found that the HMGN1/TLR4 pathway gene expression was significantly reduced in this process (Figure 6A–6B), and protein expression also showed consistent changes (Figure 6C).
Comparison of Biochemical Indices of Patients.
Comparison of Renal Function Before and After Treatment in Two Groups of Patients.
Changes in Levels of Inflammatory Factors in Patients.

Comparison of Biochemical Indexes of Patients (A, B: Fasting Blood Glucose (FPG) and 2 h Postprandial Blood Glucose (2hPBG) Index Levels Detected by Blood Glucose Meter; C: Glycosylated Hemoglobin (HbA1c) Levels Detected by Ion-Exchange Chromatography; D, F: Total Cholesterol (TC) and Triglyceride (TG) Levels Detected by Enzyme Assay; E: Low-density Lipoprotein (LDL)-C Levels Detected by Direct Assay; Compared with Control Group, *p < .05; n = 15).
Comparison of Renal Function in Patients (A, B: Immunoturbidimetric Detection of Urinary Albumin Excretion Rate (UAER), Cys-C Index Levels; Compared with Control Group, *p < .05; n = 15).
Changes in the Levels of Inflammatory Factors in Patients (A, B, C, D: Serum C-reactive Protein (CRP), Interleukin (IL)-6, IL-10, and Tumor Necrosis Factor (TNF)-α Expression Levels by Enzyme-linked Immunosorbent Assay (ELISA); Compared with Control Group, *p < .05; n = 15).

HMGN1/TLR4 Pathway Protein Expression (A, B: Polymerase Chain Reaction (PCR) for HMGN1, TLR4 Gene Expression; C: Western Blot for HMGN1, TLR4 Protein Expression; Compared with Control Group, *p < .05, n = 15).
DOP Combined with Linagliptin Slows Down Disease Progression in Mice by Inhibiting HMGN1/TLR4. Mechanism Verification of the Pathway
On the basis of the above research, this project deeply investigated the mechanism of DOP on the HMGN1/TLR4 pathway. We successfully constructed the in vitro experimental mouse model, and the success rate for mouse construction was 100%. Through further research, we used CRX-527 and TAK-242 to agonize and inhibit the HMGN1/TLR4 pathway, and results showed that FPG and 2hPBG decreased with the DOP group when compared with the DOP + TAK-242 group. Moreover, UAER, Cys-C, and CRP decreased, and IL-10 was elevated in the DOP + TAK-242 group (p < .05, Figure 7A–7F). HMGN1 and TLR4 gene expression was reduced significantly (vs. DOP group, p < .05, Figure 7G–7H) in which the results for the DOP + linagliptin + TAK-242 group showed more obvious and consistent change, while the DOP + CRX-527 group had opposite results, which indicated that DOP had a significant inhibitory effect on the HMGN1/TLR4 pathway.
Changes in Blood Glucose, Renal Function, and Inflammatory Factors (A, B: Fasting Blood Glucose (FPG) and 2 h Postprandial Blood Glucose (2hPBG) Index Levels Detected by Glucometer; C, E: Urinary Albumin Excretion Rate (UAER) and Cys-C Index Levels Detected by Immunoturbidimetric Assay; D: Glycosylated Hemoglobin (HbA1c) Levels Detected by Ion-exchange Chromatography; F: Serum Interleukin (IL)-10 Expression Levels Detected by Enzyme-linked Immunosorbent Assay (ELISA); G, H: HMGN1 and TLR4 Gene Expression Detected by Polymerase Chain Reaction (PCR); Compared with Control Group, *p < .05; n = 5).

Discussion
DOPs have beneficial effects on anti-oxidants, immunostimulant (Liu et al., 2011), as well as dermatological disorders (Yang et al., 2020). DOP treatment attenuated hepatic lipid metabolism disorders in type 2 diabetic rats and alleviated symptoms of hepatic lipid accumulation (Meloni et al., 2013).
Linagliptin reduces glucagon levels in a glucose-dependent manner (Burcelin et al., 2006; Lee et al., 2018; Nadkarni et al., 2014; Sandoval, 2008). Current studies have confirmed the therapeutic effect of linagliptin on diabetic nephropathy. Experiments on a diabetic rat model (Katsuno et al., 2021) demonstrated that linagliptin can reduce oxidative stress and effectively improve diabetic nephropathy and that it is effective in ameliorate pathological changes. In addition, some studies have confirmed a better effect of DPP-4 inhibitors on brittle diabetes (Kanasaki, 2018).
UAER and Cys-C are diagnostic indicators of EDN (Javanmardi et al., 2015), and it is believed that diabetic nephropathy is related to inflammation and renal fibrosis (Duran-Salgado & Rubio-Guerra, 2014). CRP is correlated with DN severity (Sinha et al., 2019). In this study, we found that biochemical indexes FPG, 2hPBG, HbA1c, TC, LDL-C, and TG, and renal function indexes UAER, Cys-C, and also CRP, IL-6, and TNF-α inflammatory factors were reduced under intervention by DOP, while the IL-10 anti-inflammatory factor was elevated. Moreover, the biochemical indexes in the DOP + linagliptin group, renal function indexes, and inflammatory factors were further reduced. It shows that DOP can significantly improve diabetic nephropathy and that linagliptin has an inhibiting effect on it. In addition, we also observed that the intervention by DOPs led to a significant reduction of HMGN1 and TLR4 proteins, and the inhibitory effect of DOPs + linagliptin was more significant. It was thus suggested that the effect of DOP on diabetes was related to the HMGN1/TLR4 signaling pathway.
HMGN1/TLR4 signaling regulates immune response. The inflammatory response is exacerbated in diabetic nephropathy because of immune imbalance. Activation of the HMGN1/TLR4 signaling pathway can affect the activation and function of immune cells, thereby influencing the immune response process (Imig & Ryan, 2013). This study found that the combination of DOPs and linagliptin significantly reduced the expression of HMGN1 and TLR4, which was accompanied by decreased levels of inflammatory factors (such as CRP and IL-6) and improved renal function markers (UAER and Cys-C). These results suggest that the therapeutic effects may be achieved through the suppression of the HMGN1/TLR4 pathway. This mechanism is consistent with the findings of Yu et al. (2018) in a BDM-EDN model.
To investigate the role of the HMGN1/TLR4 signaling pathway, we used CRX-527 and TAK-242 to activate and inhibit it, and found that patients’ FPG, 2hPBG, UAER, Cys-C, and CRP were all reduced, while IL-10 was increased. Moreover, results for the intervention effect of DOP + linagliptin + TAK-242 were more obvious, and the effect of DOP + CRX-527 was opposite to that effect.
Conclusion
In conclusion, DOP extract can control blood glucose levels in BDM-EDN patients and improve UAER by decreasing inflammation, which has the effect of protecting renal function, and linagliptin can further amplify the effect. This provides new treatment options for the treatment of this disease and helps to provide a theoretical basis for future drug development. However, the small sample size in this study was a shortcoming of the experimental design of this study, and it is thus necessary to expand the sample size for in-depth research to confirm.
Footnotes
Acknowledgments
This work was supported by the Medical Science Research Project of Hebei Provincial Health Commission (Project 20210231) and Hebei Provincial Administration of Traditional Chinese Medicine Research Program(Progect 2021216 and Project 2022441).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the ethics committee of Bethune International Peace Hospital.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The patients gave informed consent to the study and signed informed consent forms.