
Abstract
Introduction:
The COVID-19 pandemic led to increased risk of mental ill-health as well as new challenges in the implementation of community-based interventions. This study aimed to evaluate the implementation of a resilience and mental health intervention among young people in disadvantaged urban communities in Uttarakhand, India, during the COVID-19 pandemic.
Material and Methods:
Participants in this study included 426 school-going adolescents who lived in low-income neighborhoods in Dehradun, North India. They joined weekly peer-facilitated group sessions of 90 minutes and followed a structured intervention, Nae Disha. Qualitative interviews and focus group discussions with 79 people assessed implementation processes. We analyzed these using reflexive thematic analysis (inductive) and then fitted the categories that emerged into an adapted framework for the evaluation of complex health interventions.
Results:
In a context of emerging from a pandemic lockdown in disadvantaged, informal urban settlements, participants (facilitators and youth) reported improved coping, mental well-being, and hope for the future as well as improved relationships with household members and peers. Implementation factors that supported outcomes included contextually adapted innovations, use of WhatsApp for coaching and monitoring. Implementation measures taken to reduce COVID-19 transmission included small group sizes, responsiveness to community concerns, and smartphone use to coach facilitators.
Discussion:
This study found improved measures of mental health and resilience for young people participating in this group intervention set in low-income communities in North India, which are correlative, not causative. Key mechanisms that supported outcomes included recognizing concepts by using local dialects, feeling safe to participate, forming new peer friendships, and feeling safe and belonging. This group intervention was socially feasible, acceptable and cost-effective in a pandemic context and merits further research using a control group in other settings in South Asia.
List of Abbreviation
FGDs: Focus group discussions
Background
The increases in mental distress in the global COVID pandemic were linked to both social restrictions to limit viral spread, as well as to the infection itself. 1 There is clear evidence that the COVID-19 pandemic and associated public health measures significantly increased mental distress among young people through increased social isolation and fewer opportunities for peer contact. Groups at higher risk included groups who already experience structural disadvantages, such as those who are poor, women, and young people.2,3 Young people confined to their households were at greater risk of mental ill-health due to increased violence in families, loss of routine, and lack of access to peers, schooling, and physical activity.3,4 Further, they were at risk because of the reduced opportunity to attend school, which limited opportunities for cognitive and social development. There is also evidence of increased mental distress with greater anxiety and depression for young people globally in both low and high-resource settings. 5 This was likely linked to fewer mental health-promoting and protecting activities such as exercise, peer contact, and school activities.6,7 These increases in mental distress were particularly noted among young people facing structural disadvantage, such as those in low- and middle-income countries and living in disadvantaged neighborhoods.5,7
Mental illness contributes at least 4.7% to disability-affected life years in India. 8 In India, access to mental health services is poor 9 and studies following the COVID pandemic in India showed significantly higher prevalence of common and severe mental health problems even among those with higher education and socio-economic status. 1 Yet a growing body of research explores how interventions can reduce the negative impacts of childhood adversity and also improve mental health and resilience for young people.10–12
During the COVID pandemic and in the following years, there were significant physical social distancing restrictions, meaning interventions needed to build on local resources and use local people.7,13 Yet few studies have evaluated implementation of mental health interventions among youth in low- and middle-income countries in pandemic conditions, and a recent systematic review found no publications or studies set in South Asia among young people during the COVID pandemic. 7 Nae Disha (New Pathways) is a four-month-long youth resilience and mental health intervention developed by Burans, Herbertpur Christian Hospital. Pilot implementation studies among 106 young women who had dropped out of school and 142 young people impacted by mental health problems demonstrated that young people participating showed increases in resilience, social inclusion, and mental health in pre-post studies which endured up to nine months.14,15 This intervention demonstrated mechanisms such as new peer friendships, higher levels of community participation, and greater self-efficacy in a realist evaluation. 16
Recognizing the likelihood of further respiratory transmitted pandemics in the years ahead, 7 this study aimed to evaluate the implementation processes in conducting the Nae Disha resilience intervention in disadvantaged urban communities in North India.
Methods
The Conceptual Framework
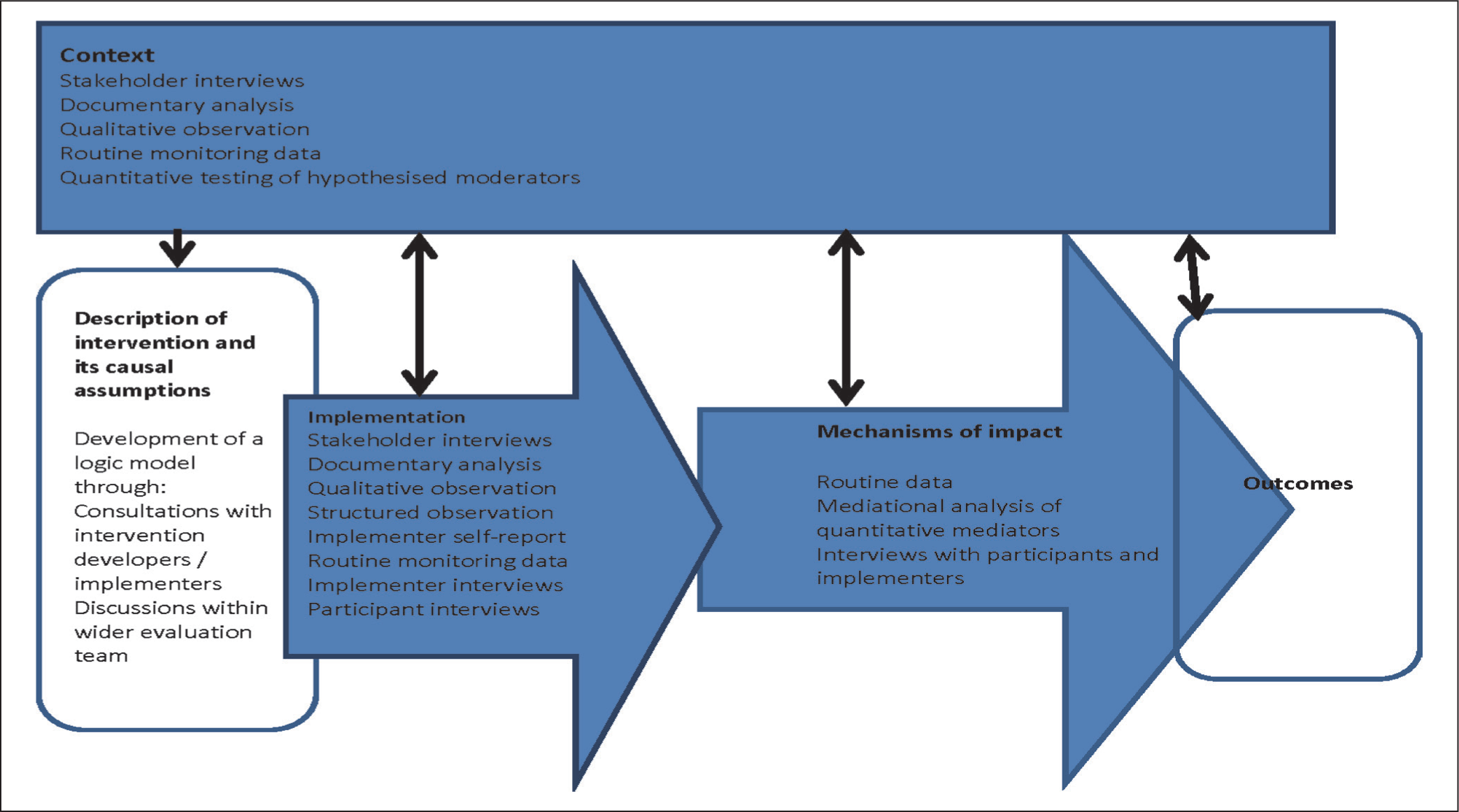
We examined the process of how Nae Disha was delivered during the COVID-19 pandemic, focusing on the context, implementation, and mechanisms of impact, adapting the MRC framework for process evaluations of complex interventions depicted in Figure 1. 17 Greater detail on the intervention and the theory of change has been described elsewhere.14,16 In this study, an “intervention” refers to the specific action or program being implemented, while a “mechanism” is the underlying process or reasoning through which that intervention produces change within a particular context, essentially explaining how the intervention works at a deeper level by focusing on the cognitive and behavioral responses of individuals affected by it. 18
Setting
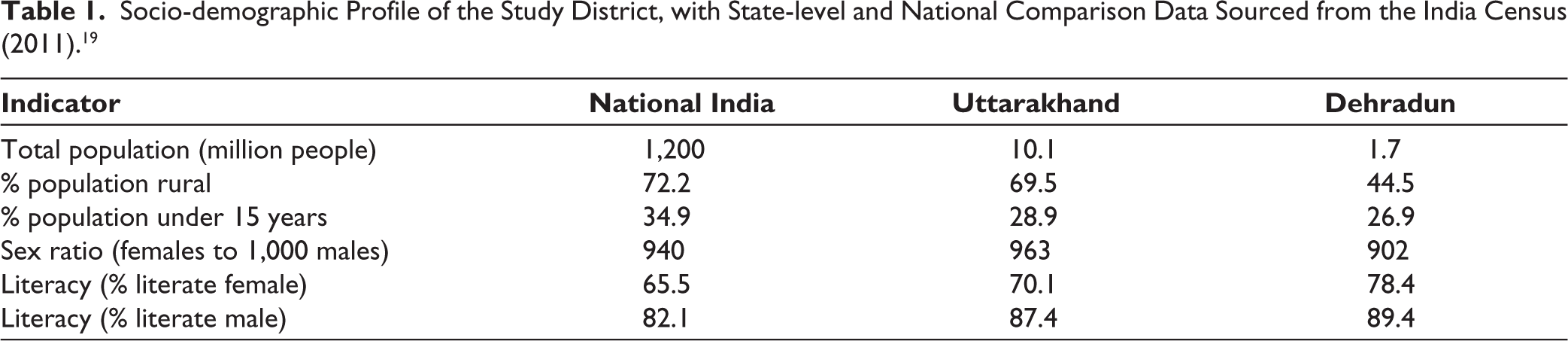
Nae Disha was implemented from September to December 2020, among 426 school-going adolescents, after the first Indian COVID-19 wave during the easing conditions of lockdown. We selected three urban and peri-urban sites in low-income urban communities in Uttarakhand, North India. We have outlined the socio-demographic profile of Dehradun district compared with Uttarakhand state and the national data in Table 1 to provide context for the gender disparities and demographics of the study area. It shows Dehradun’s population is youthful and predominantly urban, with a high level of gender disadvantage demonstrated by skewed sex ratios advantaging men, and also greater literacy for men than women.
Socio-demographic Profile of the Study District, with State-level and National Comparison Data Sourced from the India Census (2011). 19
Participants
Facilitators recruited the 426 participants aged 13–18 years using a pragmatic real-world approach that could be generalized in other settings and did not include statistical sample size calculation. Based on several years of work in the project areas, they selected gullies in informal urban areas where they planned to work. Our inclusion criteria approach was to invite 100% the young people enrolled at the same government school in classes 7–9 in the identified gullies (lanes) by door-knocking at each house in adjacent gullies. We excluded young people attending private schools. This approach did mean that those attending private schools were systematically excluded, and the bias favored participation of government school students who are typically more disadvantaged.
This approach allowed participants to meet without violating travel restrictions and allowed the formation of peer friendships with neighbors. Sample size was pragmatically chosen to meet the maximum capacity of implementation teams. Groups were formed with 8–10 adolescents of the same gender. We took signed consent for participation of all young people from parents and took verbal assent for participation for all youth participants.
Intervention
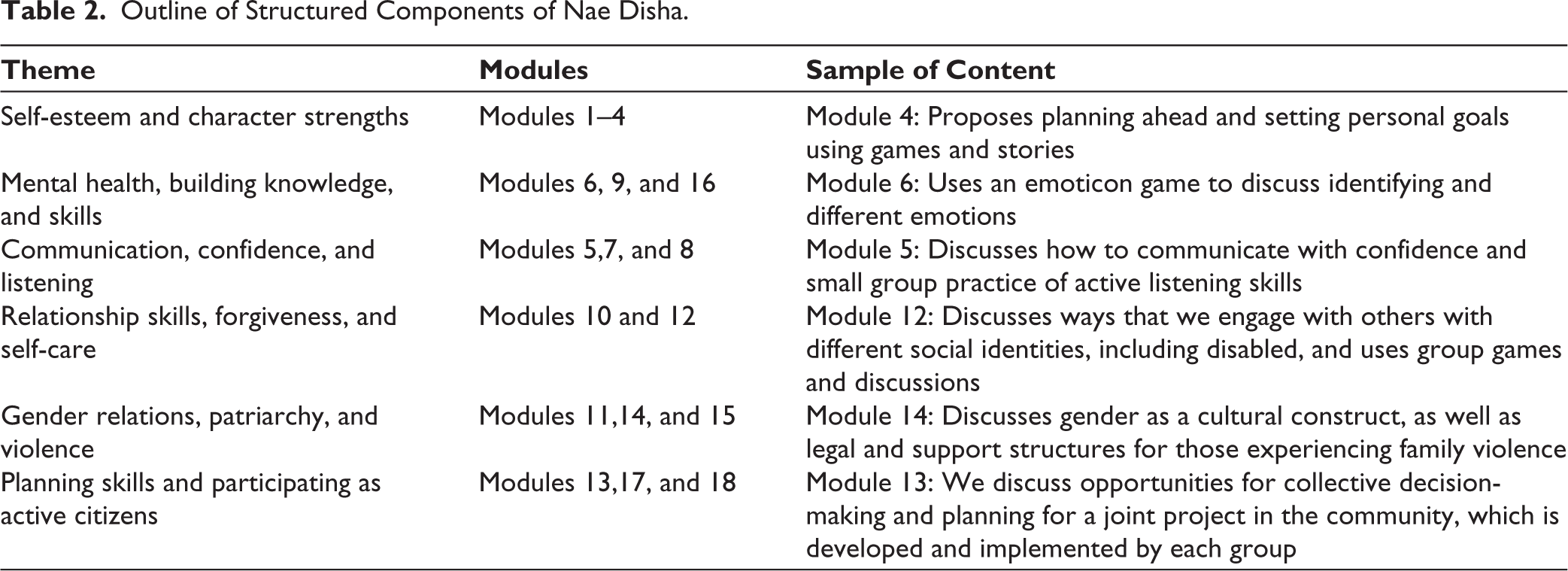
The Nae Disha intervention is available from First connecting relationally with the community, which includes meeting parents, young people, and building relationships over several weeks before formal meetings. Second, young people are formed and meet in groups and are facilitated to follow a structured curriculum that builds on youth development and positive psychology precepts, described below in Table 2. Eight community-based volunteers aged 25–35 years were trained both in person and via WhatsApp over six full days by a coach. The training focused on skill-building for group facilitation. The training also sought to de-establish hierarchy and promote critical reflection between coaches and facilitators. Facilitators were trained to promote experiential learning, such as running scenarios with role plays to model more equal gender relations. Table 2 provides an overview of the intervention content.
Adaptations were made to the intervention to engage with the pandemic context and included measures such as:
Training of facilitators using WhatsApp group calls Revising the location of meetings to ensure a high level of ventilation Ensuring the use of masks by all participants in group meetings Substitution of contact activities or those requiring close proximity with alternate non-contact games The content engaged with current pandemic-linked events, such as in the modules around mental health and anxiety, facilitators gave examples of the lockdown and invited sharing about the emotions experienced at that time
We measured intervention fidelity with the following registers:
An intervention fidelity checklist (adherence to curriculum and intervention) Coach-led discussions with facilitators on challenges and highlights fortnightly A register noting attendance of facilitators and adolescents A register noting completion of assigned home activities.
We calculated the total budget by including facilitator costs, community volunteer honorarium, refreshments, and room hire costs over the entire program, which was divided among the total number of participants to arrive at the cost per participant.
Data Collection
SP collected qualitative data using semi-structured interviews and focus group discussions with implementers, group leaders, young people, and parents (total n = 79 participants). These explored the contexts that supported outcomes, as well as mechanisms, enablers, and barriers to participation. We also discussed sessions with young people to identify preferred modules and activities, and those that worked less well. Supplementary Table 1 provides an overview of the types of qualitative data collected and the participants in data collection.
Quantitative Data
Youth filled the paper-based forms and were supported by data collectors. Socio-demographic data were adapted from the Indian demographic and health surveys. 20
Data Analysis
SP transcribed and analyzed using the framework in Figure 1 and analyzed inductively, using thematic analysis. JL and SP coded the same three transcripts, and then a broad coding framework was agreed upon with KM. JL and SP then coded the remaining transcripts in discussion with KM. Coding generated seven categories and four themes. We provide an example of the coding process in Table 2 in the Supplementary Materials. We then grouped findings by the adapted framework for the process evaluation for complex health interventions. 17
Outline of Structured Components of Nae Disha.
Ethical approval for this study was granted by the Emmanuel Hospital Association IEC in Delhi. All participants provided informed written consent for their participation in the study. This community study was registered with the Clinical Trials Registry of India.
Results
Results are presented here as a socio-demographic profile, outcomes (both quantitative and qualitative), and key meta-themes (qualitative) emergent from the data, under the headings: Context, implementation, and mechanisms that supported the outcomes.
Socio-demographic Profile
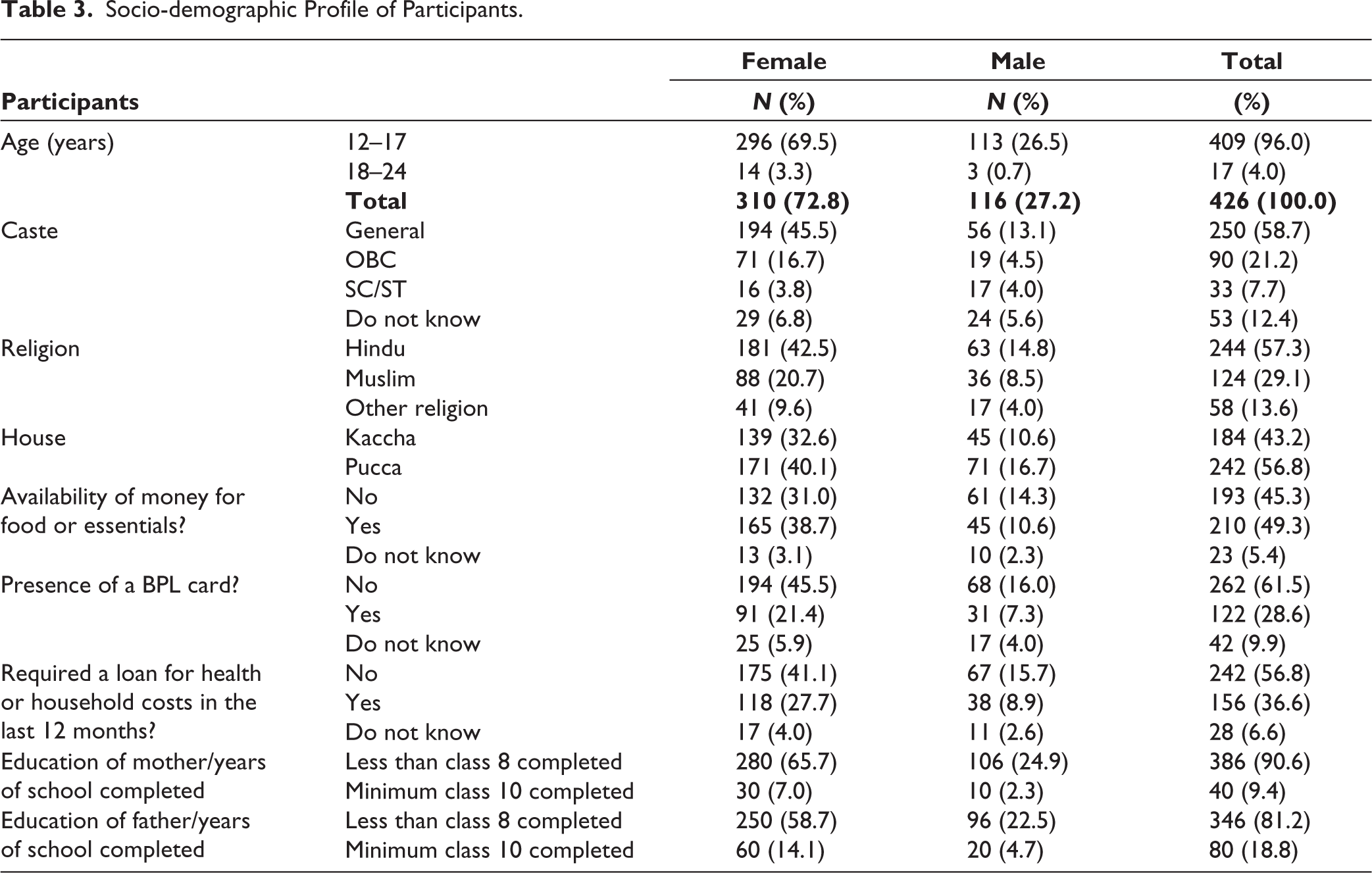
The socio-demographic profile of participants in Table 3 shows that the young people were extremely disadvantaged economically. For example, half of the participants described running out of money for basic needs such as food, and over half of the young people lived in a “kaccha” house, denoting housing made of temporary materials such as a tarpaulin roof or a dirt floor. Also of note is the low education status of parents, with 80% of fathers and 90% of mothers reported as not having completed eight years of schooling.
Socio-demographic Profile of Participants.
Qualitative Findings
Supplementary Table A summarizes key findings from the qualitative data, and themes are presented below.
Outcomes: A Better Understanding of Sexual and Reproductive Health (SRH) and Gender Equality
Outcomes linked to gender transformation and SRH included increased knowledge and skills in gender relations, while girls in particular described new attitudes supporting gender equality.
I used to hesitate a lot to play with boys….“playing with boys will make you (girls) like them.” Now, without any hesitation, I play with boys and defeat them. So playing is fun for me now. I was not interested in studying, but after joining Nae Disha, I understood that I need to study to become something in life.
Young woman, Nae Disha
Some mothers also described that through their daughters, they had greater knowledge around SRH. A handful of students, including young men and women, described increased understanding of gender equality and being more engaged in understanding hierarchies linked to non-binary and heteronormative identities, caste, and religion.
Outcomes: B Improved Coping and Relational Skills
Young people and their parents reported that after completing the Nae Disha intervention, they felt more confident and that they had greater self-esteem and acceptance of self and others. Facilitators also reported that “shy” participants were eventually able to make friends and interact with others in the group, becoming more confident and open to conversation.
I never liked to make new friends. I just had one friend with whom I used to share all my feelings. But now I know the importance of friends and friendship. I made new friends here and liked to meet new teachers here.
Young woman, Nae Disha
Parents described their children as becoming more compliant and, in terms of how they themselves accrued benefit, for example, describing their children as more helpful with household chores, obedient and respectful, and saying that they “talk better.” Other changes described included anger management, increased focus, and increased setting and working toward goals, as well as being able to deal with stress and problem-solving capabilities.
Context: A Response to Socio-economic and Pandemic-induced Conditions in the Community
Lockdowns in India were imposed from March 2020, with gradually easing restrictions from September 2020. In some cases, although enrolled in schools, adolescents described that they could not access online classes as they did not have access to mobile phones or reliable internet connectivity. Additionally, they explained that there were no other resources or opportunities for meeting peers due to the lack of smartphone ownership and data among young people. Facilitators noted that this intervention primarily engaged with young people by visiting door to door to communicate the intervention and meeting details, which recognized the limited connectivity for low-income families. They also described that COVID-19 restrictions had some positive influences on Nae Disha implementation. For example, because schools were closed and casual employment was limited, this increased attendance and participation with Nae Disha groups, which provided an opportunity to socialize with peers.
Context: B Family and Gender Relations Influences on Attendance
There was a range of factors linked to family and gender relations that influenced attendance. Facilitators and young people described parents as key influencers of attendance. Most parents supported their children participating, perceiving Nae Disha as educational and even a substitute for classes missed due to the lockdowns.
Geographic factors, such as travel distances for those in more remote areas, reduced attendance. Gender relations were a further key factor influencing attendance and participation, and young women reported limited freedom of movement and could only attend Nae Disha sessions if accompanied when walking to and from group meetings. Young men described that gender relations impacted their attendance after the lockdown because, as workplaces started opening, they were required and expected to generate income, being male members of the family.
Implementation: An Adaptation of the Intervention to A Pandemic Setting by Reducing the Risk of Infection
Nae Disha’s COVID-19 infection control measures included physical spacing between people, questions on household pre-attendance COVID-19 exposure, and measures such as ventilation, mask use, and cleaning surfaces.
To respond to the pandemic setting, we made substantial changes to the Nae Disha implementation, such as changes in group size, group meeting rules, coaching, documentation, and keeping all implementation plans fluid. We reduced group size from 15 to 10 young people, to limit risk of exposure to infection, and for the same reason, we also moved group venues from private homes to rooms hired in the community, used masks and spaced physically, used ventilation in rooms, and collectively agreed that any group members with respiratory symptoms would stay home. There were also increased documentation requirements, such as maintenance of registers and meeting observations, as the number of groups also increased, repeated schedule changes based on the many moving variables, such as lockdown status changes, online classes, exams, school reopening, and household chores of participants. Because of absences, facilitators summarized the previous session before each new module and gave catch-up sessions with individual participants where possible, which increased the facilitator workload and fatigue.
Recognizing higher rates of anxiety and depression among young people, we also supported those who were more severely affected in seeking formal help. To facilitate movement, while there were some travel restrictions, a facilitator would accompany young people to the government hospital using a hired Vikram (open-sided three-wheeled vehicle).
There were also increased pragmatic barriers to implementation in a pandemic setting, such as finding rooms large enough for a group of 10–12 people with spacing between them as outlined below:
I faced a space issue. Many times, we had to change the location and one of the reasons was to maintain social distancing. The room where we conducted Nae Disha was also used for a business selling momos, and was too crowded. Then I made them sit at another place, but it was a makeshift arrangement, so the students did not concentrate properly. Facilitator, HOPE
Eventually, the implementers rented three rooms in the community, which were easy to access for the majority of the participants, and these allowed adherence to COVID-19 safety protocols.
Implementation: B Responding to Community Concerns
Additionally, many families from the community mistrusted outsiders and were reluctant to provide phone numbers and/or other identifying information due to a sense of growing government surveillance. Further, in urban slum communities, there was minimal compliance with COVID-19 control guidelines, such as wearing masks and regularly washing hands. To mitigate mistrust and non-compliance, facilitators spent time talking and meeting with community members and reported that the field presence of BBBS’s general mental health work increased the credibility of facilitators in the community. This community relationship building supported recruitment and engagement with participants. Facilitators described that it would be challenging to conduct Nae Disha as a stand-alone community-based intervention, explaining that relationships between facilitators and parents were more fragile in locations where no other buttressing BBBS mental health program was delivered.
In that colony, people do not know us. Parents do not understand what it is that we do and therefore do not trust us.
Coach, HOPE
Implementation: C Using Smart Phones and Social Media Groups Optimized Implementation
Facilitators from different communities were asked to reduce face-to-face interactions with each other in closed spaces to reduce the risk of transmission of COVID-19 between communities. The limited spaces where groups were conducted also posed a challenge for coaches to visit each session while maintaining social distancing and transmission prevention protocols. Additionally, teams were also reducing transmission risk in public transportation by limiting travel to places outside their communities.
Smartphones and WhatsApp were useful in communicating with coaches and facilitators to discuss key learnings and challenges online, plan training sessions, and share photos of group sessions without having to meet face-to-face. For example, facilitators facing challenges with seating a group could take photos or use a video call to engage and problem-solve with a coach who could see the setting remotely using phone technology.
Mechanisms: A Framing of Concepts in Local Common-use Language Triggered Greater Participation by Youth
Facilitators were all local residents of Dehradun, trained as community workers of BBBS and coached on facilitation, relationship building, and problem-solving skills throughout Nae Disha implementation. They were fluent in local idiomatic terms for confronting topics, such as SRH. A facilitator explains how he did this by using scientific Hindi terms for genitalia below:
With boys, I start by asking them to make a diagram of the whole body, but they do not draw the private parts on it. I explain that God has made our body for a purpose, and so if you have all these body parts, then you must feel free to draw and label them too. Coach, HOPE
The facilitator’s fluency and contextual familiarity facilitated more difficult conversations. Facilitators were given the space to innovate as well as adapt sessions to cultural contexts and prepare for sessions by catering to requests for pick up and drop off of young people (especially young women), follow-up sessions, and adjusting timings to suit family needs. The horizontal relationship between the young people and facilitators was described as important by both groups.
Facilitators shared examples from their own lives with the groups, which created connection and a safe space for youth to name their emotions. The facilitators described a sense of being alongside by joining young people sitting on the ground in a circle, as well as the use of and encouraging informal titles such as “didi” (older sister), rather than terms used frequently to denote hierarchy, such as “ma’am.”
Young people, on the other hand, described facilitators admitting to not knowing answers to some questions as making them more approachable.
Mechanisms B: Feeling Safe and Willing to Share in Group Situations, Which Was Triggered by Careful Sequencing of Structured Intervention Components
Modules moved from “easy” to “hard,” starting with knowledge about self to interpersonal communication skills to more confronting topics such as SRH. This sequence encouraged young people to participate, and young people and parents described the SRH and gender-based violence sessions as challenging but providing important new learning.
I think the boys are very excited too, because there is no conversation at all on this topic (SRH), and there is no information, so they find themselves on the wrong path. Actually, the environment is not very friendly even at home for such conversations.
Coach, HOPE
Recognizing the cultural taboos in these conversations, facilitators communicated with parents before SRH sessions to explain the need for knowledge and understanding of our bodies. While a few parents did not permit young people to attend these sessions, they were appreciative of the transparency shown by facilitators and continued to engage with the remaining modules.
Mechanisms: C Forming New Peer Friendships Was Triggered by the Safe Space Provided by the Group Meeting Platform
Young people described forming new friendships with each other and meeting up outside of Nae Disha group sessions to do things together. Relationship building was supported by activities and games that required sharing of experiences, and cooperative decision-making, and the youth described peer interaction as highly appreciated after a lengthy lockdown period. These connections, buttressed by connections with facilitators, supported the group as a safe space to rehearse speaking in a group or holding an opinion as described below:
Here, we do not hesitate to talk, but in school, we still hesitate. In school, there are boys as well, and we feel shy asking anything to our schoolteachers, but here at Nae Disha, we ask questions related to our bodies to understand the reason behind things, like why we menstruate, and what is to be done at that time. Young woman, Nae Disha
Cost of Implementation
The overall cost of implementation (excluding research costs) was calculated to be INR 10.65 lakh or INR 1.065 million rupees. This sum was divided by the number of participants, yielding a cost of INR 2500 per young person, which translates to less than USD 30 per young person.
Discussion
This study describes a feasible and acceptable process to implement a group-based intervention during a pandemic that supported improved mental health and resilience. The key strategies that emerged as supporting effective implementation were using local facilitators, appropriate sequencing of modules, adapting the intervention content and process to the local context and pandemic, and use of an engaging session delivery format that responded to emerging concerns of young people.
Infection prevention and control measures aligned with WHO advice, though challenges arose due to the urban slum setting. Indoor sessions allowed for social distancing. Low compliance with safety protocols was mitigated through collaborative guideline development. We used a collaborative process to develop prevention and control guidelines suitable for the context of the group sessions. 21
Although the implementation of groups was conducted face-to-face, the implementation was strengthened by mobile phones to connect with facilitators. This enabled frequent communication and capacity building when there was a limited opportunity for travel. India has more than a billion users of mobile phones, and more than 487 million WhatsApp application users. 22 In this context, challenges to virtual sessions with young people included the lower availability of devices and internet connectivity for young people who still do not typically own phones, and challenges in maintaining confidentiality when using shared devices in a household.
The intervention targeted adolescents in a context of a prevalent patriarchy that privileged men and disadvantaged women.16,23 Poorer young women in this setting are more likely to be expected to leave school in their early or mid-teens and to marry in their late teens and have limited freedom of movement, while poorer young men are expected to generate income from their early teens.23,24
The Nae Disha intervention’s gender-transformative aspirations were limited by entrenched cultural norms. Balancing progressive SRH education with parental trust proved challenging.10,23 Yet the implementing team built trust through dialogue and relationship between the implementers (facilitators and coaches) and parents, which others also report as key to increased civic engagement and community change.10,25
Implementing an intervention that challenges social norms and patterns requires close attention to the formats of implementation to ensure they are culturally acceptable.10,26–28 “Complex interventions may work best if tailored to local circumstances rather than being completely standardized.” 29 Approaches included iterative implementation, community trust-building, and evidence of facilitators applying learnings in their own lives and use of technology.
This intervention represents a low-cost and scalable intervention. While we could not easily locate comparable community-based studies with a cost analysis, a school-based intervention conducted in India estimated a cost per participant of USD 158 during a trial, which they suggest would be USD 123 per participant in a scaled and non-trial setting. 30 Our cost per participant of USD 30 compares very favorably, suggesting this is low-cost and scalable as an intervention. We note that a systematic review identifies mental health promotion and prevention group interventions as broadly cost-effective. 31 The costs of this participant (less than USD 30 per person) are low considering the opportunity for small group connections and an intervention with five months of relationship building. This intervention can be seen as cost-effective and sustainable
Strengths and Limitations of Study
There were some important limitations in this study, which include the risk of participants being non-representative of their neighborhoods. As participants were only selected if they attended a local government school, they were likely to have been more disadvantaged than others nearby (as many families with resources prefer to enroll children in private schools). Conducting the study during the pandemic posed many changes in both the implementation and research of this study. It meant the context was changing constantly during implementation, which led to challenges in needing to iteratively adapt the intervention and to keep changing processes of documentation for this implementation research study. These findings are useful to inform community program delivery in future pandemics, but this may make the findings less generalizable to non-pandemic settings. We note that the core context of the need to support youth mental health in low-income urban communities during a respiratory transmitted epidemic is likely to be relevant in the years ahead.
There were important strengths in the study design: First, it was conducted in a low-income “real-life” setting, and groups were facilitated by community members who understood the local contexts well, thus likely delivering the intervention in ways that were relevant and acceptable. The implementation was relatively low-cost because it was facilitated by local community members who received modest remuneration and used local resources (such as holding meetings in local houses), which increased generalisability and minimized costs. Thus, strengths included the real-world setting, data that provide an in-depth understanding of the context, pandemic implementation, and inclusion of disadvantaged participants, which addresses ethical equity concerns.
Implications
This study illustrates the value of psychosocial groups as a socially feasible and acceptable platform to address anxiety, build peer connections, and improve mental health outcomes for young people in a pandemic context. This study is low-cost, and our cost analysis suggests that this intervention can be scaled even in settings of limited resources. Notably, the costs may be even less in an institutional setting such as a school, where there are greater opportunities for assembling young people and using existing infrastructure for meetings. 30 Psychosocial groups interventions such as this have the potential to influence both the demand and supply side of poor mental health in communities in South Asia, both during and outside of pandemic periods.32,33 Importantly, a group intervention such as this can act as a platform for the delivery of mental health promotion and even care, in times of crisis.32,34 We recommend implementation research of this and similar interventions in other complex settings (such as prisons, conflict, and pandemics) to further understand effective iterative adaptations and mechanisms that will trigger outcomes to strengthen mental health and resilience in diverse contexts.
Conclusions
This youth mental health and resilience intervention was feasible and acceptable when implemented among disadvantaged young people living in informal urban communities in the context of the post-lockdown period of the first wave of the COVID-19 pandemic in North India.
Qualitative data revealed outcomes of greater knowledge in SRH and improved relational and coping skills. Key mechanisms that supported these outcomes included recognizing concepts using local dialects and examples, feeling safe to participate, forming new peer friendships, and feeling safe and belonging in groups. Key to implementation was the responsiveness of facilitators to community concerns, iterative micro-adaptations to the changing local context, and use of digital platforms to support implementation (particularly WhatsApp). This group intervention was socially feasible, acceptable, and cost-effective in a complex context and merits further research using a control group in other settings in South Asia.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Thanks to Laxman Balan, Pooja Bhatt, Atul Goodwin Singh, Jeet Bahadur and the entire Burans team and partners for the implementation and data collection of Nae Disha programme and all the young people who participated in this Nae Disha programme. Thanks to Sanjaya Mark and Craig Cook from Woodstock School, Lawrence Singh & Stephen Masih from Agnes Kunze Society, Ronjoy Rao and Rita Rao from Sneha School, Leena Aparajit, who were part of the advisory body that supported pragmatic changes to the implementation during the pandemic.
Data Availability Statement
The quantitative data from this study is available from authors on request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study (Protocol 224) was granted by the Emmanuel Hospital Association Institutional Ethics Committee in August 2020. The study was retrospectively registered with the Australian New Zealand Clinical Trials Registry on June 17, 2022, and was assigned registration number ACTRN12622000858796.
All procedures performed in this study were conducted in accordance with the ethical standards of the responsible institutional and national committees on human experimentation and with the 1975 Helsinki Declaration, as revised in 2000.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The University of Melbourne Chancellory Grant supported costs for the implementation of the intervention, and the research costs were covered by in-kind time of Herbertpur Christian Hospital staff using local funding sources.
Statement of Informed Consent
Consent was taken by all participants as per ethics protocol but further was not required for this paper.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.