
Abstract
Axial spondyloarthritis (axSpA) is a chronic inflammatory disease affecting the spine, peripheral joints and entheses, driven by dysregulated immune cell pathways, particularly the Janus kinase-signal transducer and activator of transcription (JAK‑STAT) pathway. While non‑steroidal anti‑inflammatory drugs and biologic disease-modifying anti-rheumatic drugs (DMARDs) (e.g., tumour necrosis factor inhibitors [TNFi] and interleukin inhibitors [IL‑17i]) are standard treatments. However, many patients show inadequate responses, necessitating alternative therapies. JAK inhibitors (JAKi), including tofacitinib, upadacitinib and filgotinib, offer targeted benefits by blocking the JAK‑STAT pathway to reduce pro-inflammatory cytokine transcription. Clinical trials have demonstrated that tofacitinib significantly improves ankylosing spondylitis outcomes, achieving superior Assessment of Spondyloarthritis International Society 20 and 40 (ASAS20 and ASAS40) responses compared to placebo. Upadacitinib has consistently shown efficacy across both radiographic and non‑radiographic axSpA in the SELECT‑AXIS trials, while the phase II TORTUGA trial reported that filgotinib significantly reduced disease activity, with greater improvements in ASDAS and Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) scores compared to placebo. Mild side effects, such as nasopharyngitis and increased creatine phosphokinase levels, have been observed without conclusive links to severe adverse events like malignancies or cardiovascular complications. Thorough screening for tuberculosis and viral hepatitis is essential before initiating JAKi therapy. Moreover, for patients with comorbid inflammatory bowel disease, where TNFi may be unsuitable, tofacitinib provides an effective alternative. Its oral formulation enhances patient compliance and, combined with favourable cost‑effectiveness data, positions JAKi as attractive alternatives to conventional biologic therapies. Current evidence suggests that JAKi are a promising option for axSpA patients unresponsive to conventional or biologic DMARDs. However, long-term studies are needed to compare their efficacy and safety with TNFi and IL-17i.
Keywords
Introduction
Spondyloarthritis (SpA) is a group of chronic inflammatory diseases with similar clinical, genetic, imaging and pathophysiological features. SpA is divided into axial and peripheral categories, according to the predominant clinical manifestation. 1 Axial SpA (axSpA) is a chronic inflammatory rheumatic condition that primarily affects the axial skeleton. 2 AxSpA is divided into two types, namely radiographic axSpA (r-axSpA) or ankylosing spondylitis (AS), and non-radiographic axSpA (nr-axSpA).1,3 In the United States, the prevalence of axSpA has been estimated to range from 0.35% to 1.4%, with approximately 0.55% reported as r-axSpA and 0.3% to 1.6% as nr-axSpA.1,4 Meanwhile, the prevalence of axSpA in Southeast Asia is estimated at 0.2%. 5
Until now, the management of SpA has faced its own challenges due to the heterogeneity of the disease and the varied therapeutic effects. As a result, the choice of treatment regimen is influenced by the dominant clinical features. 6 Non-steroidal anti-inflammatory drugs (NSAIDs) are the first line of treatment for axSpA.2,7 Biologic agents of disease-modifying anti-rheumatic drugs (bDMARDs), including anti-tumour necrosis factor (TNF) or anti-interleukin-17 (IL-17), are recommended for patients who do not respond to, or have an inadequate response to, NSAID administration.2,7 However, many patients still do not have an adequate response to bDMARD agents. 8 In recent years, targeted therapies for autoinflammatory and autoimmune diseases have been developed. On 14 December 2021, the US. Food and Drug Administration (FDA) approved tofacitinib for the treatment of AS, followed by the approval of upadacitinib (UPA) for both nr-axSpA and r-axSpA on 28 April 2023.9,10
Janus kinase-signal transducer and activator of transcription (JAK-STAT) is one of the intracellular signalling pathways. JAK-STAT has a significant role in the pathogenesis of SpA. JAK inhibitors (JAKi) will repress the intracellular processes of various inflammatory cytokines. 11 In addition, JAKi also have indirect effects on the production of cytokines that play a role in the pathogenesis of SpA. 11 Several studies have been conducted to examine the efficacy of JAKi in axSpA patients. The SELECT-AXIS 1 and SELECT-AXIS 2 bDMARD-IR studies have found the benefit of administering JAKi or UPA in axSpA patients who do not respond or are intolerant to more than one TNF inhibitors (TNFi). 12 The 2022 ASAS-European Alliance of Associations for Rheumatology (EULAR) Recommendations for the Management of Axial Spondyloarthritis suggest that JAKi may be considered, particularly for patients with persistently high disease activity despite conventional treatment. 2 Therefore, this article will discuss in depth the role of JAKi in axSpA therapy.
JAK-STAT
JAK is a type of protein tyrosine kinase (TYK) involved in the cell signalling process. The TYK protein will activate the process of intracellular protein phosphorylation as a result of receptor activation by inflammatory mediators. JAK is an intracytoplasmic TYK protein that binds to the cytoplasmic region of the transmembrane cytokine receptors. 13 JAK, which binds to a receptor (type 1 or 2), is activated after a cytokine or growth factor binds to the ligand. 14 Cytokine binding to its membrane-bound receptor triggers JAK phosphorylation and dimerisation, leading to STAT protein recruitment. STAT proteins then undergo phosphorylation and dimerisation before translocating to the nucleus, where they regulate the transcription of effector genes and promote the expression of cytokines and other pro-nociceptive factors in a positive feedback loop.13,15,16
JAK has four types of isoforms, namely JAK1, JAK2, JAK3 and TYK2. Each isoform functions to mediate certain cytokines or growth factors. JAK1 has a role in receptor signalling that is activated by IL-6, IL-10, IL-11, IL-19, IL-20, IL-22, IFN-α (interferon-α), IFN-β and IFN-γ. JAK2 is necessary for the signalling process of cytokines IL-3 and IL-5, the hormones erythropoietin, thrombopoietin, growth hormone and granulocyte–macrophage colony-stimulating factor. Additionally, JAK2 can pair with JAK1, TYK2 or other JAK molecules. JAK3 is expressed by hematopoietic cells and is activated by the cytokines IL-2, IL-4, IL-7, IL-9, IL-15 and IL-21. These cytokines play a crucial role in the activation, proliferation and function of lymphocyte cells. JAK3 only pairs with JAK1. Meanwhile, TYK2 is involved in signalling IL-12, IL-23 and type 1 INF. TYK 2 can pair with JAK1 or JAK2.17,18 There are seven types of STAT, namely STAT1, STAT2, STAT3, STAT4, STAT5a, STAT5b and STAT6. The combination of various types of STAT and JAK plays an essential role in the pathogenetic processes of autoimmune diseases.18,19
The JAK/STAT pathway plays a key role in pain modulation. Preclinical studies show that JAK/STAT3 regulates astrocyte proliferation and pain in neuropathic pain models and nerve injury.20,21 Inhibition of this pathway with JAKi like tofacitinib reduces pain and glial activation in pain-associated central nervous system regions. 22 This supports the JAK/STAT pathway as a critical target in managing pain in conditions like axSpA and complex regional pain syndrome. 23
Mechanism of JAKi
JAKi are a class of targeted synthetic disease-modifying antirheumatic drugs (tsDMARDs) that can be administered orally. Unlike bDMARDs, which inhibit cytokines, cytokine receptors or specific cell surface molecules, JAKi target intracellular signalling pathways that affect multiple cytokines and growth factors. As a result, this inhibition reduces the production of various cytokines, ultimately decreasing the inflammatory response. 18
The cytokines IL-2, IL-4, IL-7, IL-9, IL-15 and IL-21 modulate the adaptive immune system through the JAK1/JAK3 combination by regulating T-helper (Th) cell differentiation and function.13,18 IFN-γ and IL-12 signalling work through the JAK1/JAK2 and JAK2/TYK2 combinations. These signalling pathways play a crucial role in the response of Th1 cells and the production of TNF-α by macrophages, which contributes to the pathogenesis of SpA. Although TNF-α is not directly inhibited by JAKi, blocking the JAK2/TYK2 or JAK1/JAK2 pathways reduces TNF-α production by decreasing IL-12 and IFN-γ levels.13,18 Apart from the TNF-α cytokine, the IL-23/IL-17 cytokine axis mechanism plays a significant role in the pathogenesis of SpA. The cytokine IL-23, which is produced by dendritic cells, works using the JAK2/TYK2 combination. Activation of JAK2/TYK2 triggers the JAK-STAT signalling pathway, promoting the proliferation and differentiation of CD4+ cells and producing IL-17A. JAKi repress the JAK-STAT signalling pathway, thereby indirectly reducing IL-17A production by disrupting cytokine-mediated signalling, such as IL-23.18,24,25
JAKi work by inhibiting various combinations of JAK/STAT pathways to inhibit the transduction processes of different types of cytokines. This mechanism is considered effective for treating various autoimmune-related inflammatory diseases. 26 Several types of JAKi work selectively against certain JAK isoforms. However, it is still unclear whether JAK selectivity observed in laboratory experiments and experimental animals can be applied clinically in various chronic inflammatory diseases.27,28 Tofacitinib, baricitinib and peficitinib are types of JAKi that act on almost all JAK/pan-JAK isoforms. Tofacitinib works by inhibiting JAK1, JAK3 and JAK2. Baricitinib works by inhibiting JAK1 and JAK2. Peficitinib works more strongly to inhibit JAK3 than JAK1, JAK2 and TYK2. 26 Meanwhile, UPA works selectively against JAK1 but can also inhibit JAK2 and TYK2. Filgotinib works very selectively against JAK1 in laboratory experiments. 29
Effectiveness and Safety of JAKi in axSpA
NSAIDs are the first line of treatment for axSpA. They are administered up to the maximum tolerated dose, provided there are no contraindications.30,31 TNFi, IL-17 inhibitor (IL-17i) or JAKi should be considered for patients with persistently high disease activity despite conventional treatments. 2 All these drug classes have shown efficacy in axSpA trials. However, in the absence of head-to-head trials, it remains challenging to determine which treatment should be prioritised based on efficacy for axial disease. 2 The second part of the recommendation highlights current practice, which usually involves initiating treatment with either a TNFi or an IL-17i. This approach is based on a longer experience of consuming these drugs, a more extensive evidence base, their use in patients with multimorbidity (often excluded from randomised controlled trials [RCTs]) and a better understanding of their safety. 30 Response rates to TNFi and IL-17i therapies remain moderate, with only 60%-65% of patients experiencing a clinical improvement after their first bDMARD. 32
The 2019 ACR/SAA/SPARTAN guidelines recommend TNFi as the preferred first-line biologic therapy for axSpA and nr-axSpA. In cases of primary non-response to TNFi, IL-17i, such as secukinumab or ixekizumab, is recommended over switching to a second TNFi. Given the stronger evidence base, TNFi and IL-17i are favoured over JAKi, such as tofacitinib. For patients with active AS who have contraindications to TNFi, IL-17i is preferred over conventional synthetic DMARDs (csDMARDs) or tofacitinib. 33 However, in AS patients with concomitant ulcerative colitis, where TNFi use is not feasible, tofacitinib is recommended over IL-17i due to its established efficacy in inflammatory bowel disease (IBD), whereas IL-17i has not demonstrated clinical benefit in this context. 34 The 2025 Canadian Rheumatology Association and the Spondyloarthritis Research Consortium of Canada (CRA/SPARCC) guidelines align with the 2019 ACR recommendations in emphasising TNFi as the preferred first-line biologic therapy for axSpA, including AS. IL-17i is preferred over JAKi when TNFi is not an option, though the Canadian guidelines permit either IL-17i or JAKi in cases of TNFi contraindications. Both guidelines recognise JAKi as an alternative but highlight safety concerns, particularly with tofacitinib.35,36
AxSpA is a chronic condition. Although patients may initially respond to TNFi or IL-17i treatment, this response is often not sustained. Long-term effectiveness remains limited, with 50%-60% of patients discontinuing TNFi therapy within 2 years. 37 The multifaceted nature of cytokines suggests that a lack of response to a single anti-cytokine therapy does not eliminate the role of cytokines in disease pathogenesis. Targeting multiple cytokines, even those that have been ineffective individually, remains a valuable approach. This is where JAK inhibition plays a crucial role, as it blocks the receptors of various cytokines and their downstream signalling pathways. 30 Recent observational studies on JAKi have continued to emerge, showing promising results.
Tofacitinib
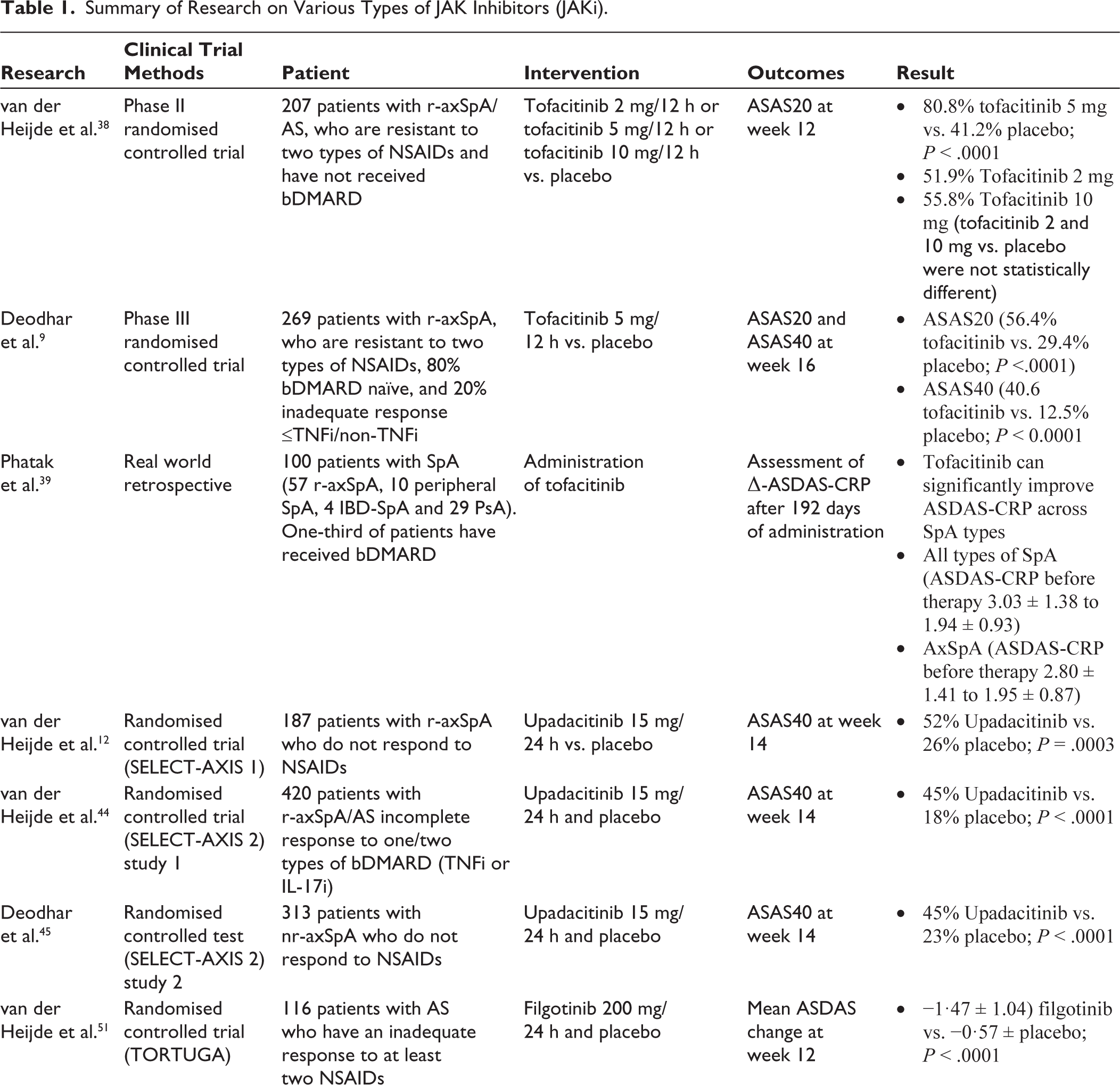
Tofacitinib is a non-selective JAKi that provides clinical benefits in AS patients. 38 The phase II tofacitinib clinical trial showed the results of administering tofacitinib (2, 5 and 10 mg every 12 h) compared to placebo in 207 AS patients who were resistant to two types of NSAIDs and had not received bDMARDs. Administration of tofacitinib 5 mg every 12 h was better than placebo, with ASAS20 response outcomes after 12 weeks of therapy (80.8% in the tofacitinib group and 41.2% in the placebo group; P < .0001). The administration of tofacitinib 2 and 10 mg was not statistically different compared to the placebo group. 38
Phase III clinical trials of tofacitinib also provided better results than placebo. This clinical trial was conducted on 269 patients with AS who did not respond to greater than or equal to two types of NSAIDs. Patients were randomly divided into two groups, namely the group given tofacitinib 5 mg/12 h and the placebo group. Research outcomes were assessed by looking at improvements in Assessment of Spondyloarthritis International Society 20 and 40 (ASAS20 and ASAS40) after 16 and 48 weeks. At week 16, tofacitinib was superior in improving ASAS20 compared to placebo (56.4% for tofacitinib and 29.4% for placebo; P < .0001) and superior in improving ASAS40 (40.6% for tofacitinib and 12.5% for placebo; P < .0001). 9 After 48 weeks of administration, side effects occurred, namely 2.3% (3 of 133 patients) had experienced liver disorders, 2.3% (3 of 133) had herpes zoster and 0.8% (1 of 133) experienced serious infections. 9
In a real-world retrospective analysis conducted in one hospital in India, tofacitinib was administered for 192 days in 100 SpA patients (57 axial SpA, 10 peripheral SpA, 4 IBD-SpA and 29 psoriatic arthritis [PsA]), one-third of whom had previously received a bDMARD. Administration of tofacitinib significantly improved ASDAS-C-reactive protein (ASDAS-CRP) in all types of SpA. 39 In addition, no serious side effects were observed during administration. Only 26 cases of mild side effects were reported, namely 19 patients experienced mild COVID-19 that did not require treatment, 3 patients had gastrointestinal side effects, 2 patients developed rash and 2 patients reported muscle pain. 39
Evaluation of seven studies (3,330 patients) of tofacitinib in patients with r-axSpA showed a significant improvement in SF-36v2 bodily pain scores and a reduction in the proportion of patients responding ‘yes’ to pain-related ASQoL questions by week 12. 40 In pooled data from two trials (370 patients), mediation analysis revealed that reduced morning stiffness accounted for ~84% of its effect on fatigue, 41 while a phase 3 post hoc analysis in 269 NSAID-IR patients demonstrated significant improvements in Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) spinal pain (−2.85 vs. −1.34), BASDAI fatigue (−2.36 vs. −1.08), ASQoL (−4.03 vs. −2.01) and work productivity impairment (−21.49 vs. −7.64) through week 48. 42 Overall, these findings support the efficacy of tofacitinib in reducing pain and enhancing quality of life in patients with r-axSpA.
Although the PASTOR study was ultimately discontinued, its design aimed to assess the efficacy of tofacitinib in reducing magnetic resonance imaging (MRI)-detected inflammation in patients with PsA presenting with axial involvement. Despite the lack of final results, the study highlighted the need for targeted treatments addressing axial inflammation in PsA. 31 In the future, studies may be needed to evaluate the role of JAKi in reducing MRI-detected inflammation in patients with nr-axSpA.
UPA
In the phase 2/3 clinical study of UPA (SELECT-AXIS 1), UPA 15 mg once daily was given to 187 patients with AS who had an inadequate response to, or were intolerant of, NSAID administration 12 Patients given UPA 15 mg/24 h were compared with placebo by assessing improvements in ASAS40 after 14 weeks. Administration of UPA was superior to placebo in improving ASAS40 (52% in the UPA group and 26% in the placebo group; P = .0003). The total reported side effects were 62% in the UPA group and 55% in the placebo group. The side effects included elevated creatine phosphokinase (9% in the UPA group and 2% in the placebo group). There were no reports of herpes zoster, infection, malignancy, venous thromboembolism (VTE) or death as side effects. 12
A follow-up study examining the results of UPA administration after 64 weeks found consistent efficacy compared to placebo. The side effects reported were nasopharyngitis (37 cases), increased creatine phosphokinase (20 cases), upper respiratory tract infections (26 cases), neutropenia (7 cases), anemia (3 cases), and lymphopenia (2 cases). 42 There were no reports of serious side effects of infection, tuberculosis, major adverse cardiovascular event (MACE), VTE, gastrointestinal perforation, IBD, kidney dysfunction or death. An adverse effect of malignant stage IVA tongue squamous cell carcinoma was reported after 20 weeks of administration, but this event was not thought to be related to the administration of. 43
The phase 3 randomised controlled study of UPA (SELECT-AXIS 2) was conducted in 420 patients with AS who did not respond completely to one or two types of bDMARD agents (TNFi or IL-17i). 44 Patients were given UPA 15 mg/24 h and then evaluated for ASAS40 improvement compared to placebo after 14 weeks. UPA was superior to placebo in improving ASAS40 (45% in the UPA group and 18% in the placebo group; P < .0001). 44 There were no reports of malignant side effects, MACE, VTE or death. Side effects were reported slightly higher in the UPA group compared to the placebo group (41% vs. 37%). One patient experienced acute cholangitis, 4 patients had COVID-19 infection and 1 patient was reported to have uveitis. 44
Apart from being used in r-axSpA patients, UPA is also effective in patients with nr-axSpA. 45 A total of 313 patients with nr-axSpA were divided into two groups: one group received UPA 15 mg/24 h, and the other received placebo. Patients were then evaluated for ASAS40 improvement after 14 weeks of therapy. UPA administration in patients with nr-axSpA was superior compared to placebo (ASIS40 improvement, namely 45% in the UPA group and 23% in the placebo group; P < .0001). 45 Both trials had similar side effects (48% in the UPA group and 46% in the placebo group). Serious side effects were reported slightly more frequently in the UPA group, namely the incidence of herpes zoster (3%), compared to placebo (1%). Five cases (3%) of neutropenia occurred in the UPA group, while there were no reports of similar cases in the placebo group. There were no incidences of opportunistic infections, malignancies, MACE or deaths when administering UPA. 45
A systematic review and meta-analysis study, involving four RCTs in 779 axSpA patients, found that JAKi administration was better than placebo in reducing disease activity, improving physical function and enhancing quality of life. 46 The incidence of side effects from administering JAKi was not significantly different from placebo. 46 Although studies of the use of JAKi in patients with axSpA did not find the incidence of MACE side effects and malignancies, patients aged ≥65 and ≥50 years with one cardiovascular risk factor should be given special attention to the risk of MACE side effects and malignancy. 2
UPA demonstrated significant and sustained improvements in pain outcomes in patients with active axSpA. In the SELECT-AXIS 1 study, UPA-treated patients showed significant improvements in global pain, back pain and nocturnal back pain as early as week 2, with the benefits continuing through week 64. 47 A post hoc analysis of SELECT-AXIS 1 confirmed that over 70% of patients had clinically meaningful improvements in back pain by week 52, which was associated with better patient-reported outcomes and reduced disease activity. 48 In the SELECT-AXIS 2 study, UPA also significantly outperformed placebo in reducing total and nocturnal back pain by week 14. 45 Another post hoc analysis of SELECT-AXIS 2 further supported rapid and clinically meaningful improvements in pain, including ≥30%, ≥50% and ≥70% reductions in patient global assessment of pain and BASDAI spinal pain question. 49 Additionally, a post hoc analysis focused on active nr-axSpA found that UPA significantly improved health-related quality of life and work productivity, with more patients achieving meaningful improvements in ASQoL, ASAS Health Index and SF-36 Physical Component Summary scores by week 14. 50
Filgotinib
The TORTUGA trial, a double-blind, placebo-controlled, phase 2 study in axSpA, evaluated filgotinib in patients with active AS who had an inadequate response to at least two NSAIDs. 51 The primary endpoint was the change in ASDAS score from baseline, with 116 patients randomised to receive either filgotinib 200 mg daily or placebo for 12 weeks. The study met its primary endpoint, showing a significantly greater improvement in ASDAS at week 12 in the filgotinib group compared to placebo (mean change ± SD: −1.47 ± 1.04 vs. −0.57 ± 0.82; P < .001). Secondary endpoints, including ASAS20, ASAS40, ASAS5/6, ASAS partial remission and Bath Ankylosing Spondylitis Functional Index (BASFI), were also significantly better in the filgotinib group. Additionally, there was a marked reduction in spinal and sacroiliac joint (SIJ) MRI inflammation scores assessed by SPARCC, with a favourable safety profile. 51
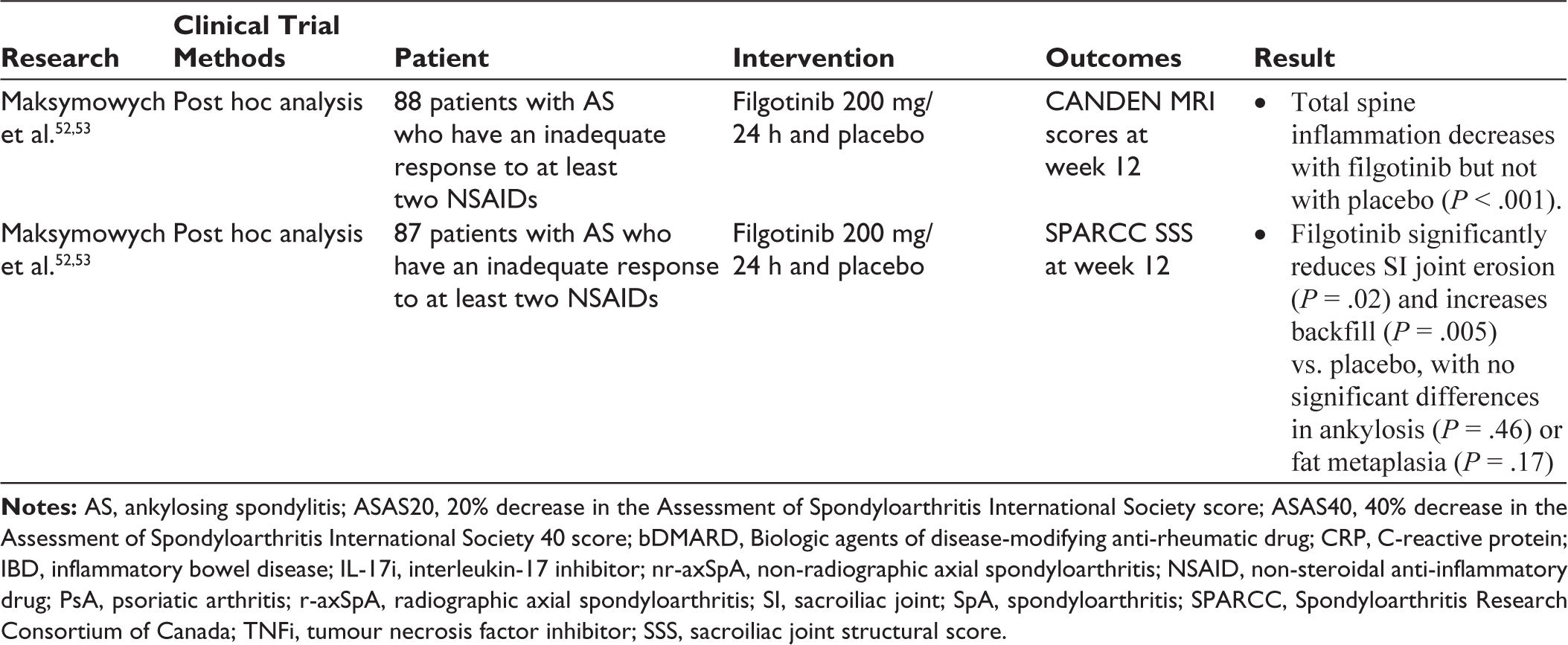
A post hoc MRI analysis further explored inflammatory and structural changes, utilising the Canada–Denmark (CANDEN) MRI scoring system for spinal inflammation and the SPARCC SIJ structural score for SIJ lesions. Filgotinib demonstrated a greater reduction in total spinal inflammation scores, including vertebral bodies, facet joints and posterolateral elements, although no significant differences were observed in vertebral body inflammation, fat lesions, bone erosion or new bone formation compared to placebo. 52 Moreover, the SIJ analysis revealed a significant reduction in erosion scores and an increase in backfill scores with filgotinib, suggesting potential tissue repair as early as 12 weeks. 53 The summary of clinical trials investigating various JAK inhibitors in axial spondyloarthritis is presented in Table 1.
Role of JAKi in Extra-articular Manifestation
The presence of extra-articular manifestations (EAMs) is a crucial factor in selecting treatment options for patients with axSpA. Monoclonal TNF antibodies, except for etanercept, have been shown to effectively prevent recurrent uveitis episodes 54 and have demonstrated superiority over etanercept and secukinumab in observational studies. 55 A similar preference for monoclonal TNF antibodies is observed in IBD, as neither etanercept nor secukinumab has shown efficacy in this condition.56–58 Due to the lack of direct comparative trials for skin psoriasis in axSpA, most of the available data come from PsA studies, which indicate that IL-17 inhibition is more effective than anti-TNF therapy in improving skin outcomes. 59
The therapeutic potential of JAK inhibition for EAMs in axSpA has been observed, though further research is needed. Its role in managing uveitis or reducing flare rates remains unclear, as no clinical trials have been conducted. Filgotinib is approved for moderately to severely active UC, 60 while UPA has shown efficacy in achieving endoscopic remission in Crohn’s disease patients who failed or were intolerant to TNFi. 61 Recent meta-analysis demonstrate the effectiveness of tofacitinib in moderate-to-severe treatment-resistant dermatoses. Although not specifically studied in axSpA, the phase 2 EQUATOR trial showed that filgotinib significantly improved psoriasis and enthesitis, with 75% of patients achieving a reduction in skin disease at week 16 compared to placebo, representing a treatment difference of 30% (P < .0001). 62
Comparative Review of JAKi and bDMARDs
Recent evidence from network meta-analyses and systematic reviews indicates that while TNF‑α inhibitors remain the benchmark for rapidly progressive AS with severe functional limitations, JAKi offer a promising alternative. In a Bayesian network meta-analysis of 937 patients with active AS, JAKi, particularly tofacitinib 5 mg, demonstrated superior ASAS20 and ASAS40 response rates compared to placebo, and ranked highest among treatments, including UPA 15 mg, filgotinib 200 mg and secukinumab 150 mg. 63 A broader review encompassing 8,937 patients further revealed that although IL‑17i produced more pronounced improvements in BASDAI50 responses and BASFI scores, the efficacy of JAKi was comparable to IL‑23i, despite TNF‑α inhibitors generally outperforming both in managing rapid disease progression. 64 In PsA, where overlapping musculoskeletal manifestations are common, JAKi exhibit similar effectiveness to TNF‑α inhibitors for joint symptoms. However, their safety profile, marked by higher risks of herpes zoster and VTE, necessitates careful patient selection. 65
In a large cohort of patients with SpA, predominantly those with PsA and axSpA, 2,849 patients initiating JAKi (mean age 51 ± 13 years) were compared with 32694 patients starting TNFi (mean age 48 ± 14 years), with post-propensity score matching yielding 2,844 patients per group and 2,792 patients per group when comparing with IL‑17i (mean age 50 ± 13 years). At 1 year, and consistently over 3 and 5 years, JAKi were not associated with an increased risk of cardiovascular disease, VTE or selected cancers compared to TNFi or IL‑17i; however, they did show a significantly higher risk of herpes zoster. 66 In a separate Korean cohort study involving patients with rheumatoid arthritis (RA), 2,963 JAKi initiators were compared with 5,169 TNFi initiators. In this study, JAKi doubled the risk of herpes zoster compared to TNFi, while the risk of serious bacterial infections was comparable, and the incidence of opportunistic infections (notably tuberculosis) was lower with JAKi. 67
JAKi offer a promising treatment option for patients with axSpA, especially those who cannot use existing biologics due to comorbidities, such as cardiac failure or IBD. While TNFi and IL-17i effectively manage axial and peripheral symptoms, TNFi benefits all EAMs, and IL-17i is particularly effective for psoriasis. Treatment selection depends on EAM presence, with TNFi often preferred as first-line therapy. However, response predictors remain unclear, and the best strategy after bDMARD failure is still debated. Limited head-to-head trial data make it challenging to prioritise treatments, and the ability to prevent structural progression remains an unmet need. As the first effective oral therapy for inflammatory spinal disease, JAKi provides a valuable alternative, particularly for patients who fail or cannot tolerate other treatments, despite current safety concerns. 68
Recent studies have evaluated the cost-effectiveness of JAKi in treating axSpA. A systematic literature review and network meta-analysis have assessed the comparative clinical and economic benefits of advanced therapies, including JAKi, for AS, a form of axSpA. The study found that UPA demonstrated numerically greater clinical efficacy and economic benefit compared to other treatments. Specifically, among biologic-naïve patients, the ASAS40 response rate for UPA-treated patients was 53.6%, with a number needed to treat of 2.8. The estimated cost per ASAS40 responder over 16 weeks for UPA was $39,500, which was lower than that of other treatments, ranging from $44,200 to $102,500. These trends were consistent among patients with prior biologic exposure. 69
In a study of 266 patients with axSpA (135 receiving tofacitinib and 131 receiving adalimumab), both treatments showed comparable improvements in BASDAI and ASDAS by month 6. Adalimumab had higher BASDAI50 and ASDAS low disease activity responses at months 2 and 4, but outcomes equalised later. The ICERdrug for adalimumab compared with tofacitinib was $188.8 per patient in the adalimumab group for each person-month with BASDAI of <4. Despite a slower early response, tofacitinib demonstrated similar long-term effectiveness with a favourable cost-effectiveness profile. 70 Cost-effectiveness analyses further support JAKi in AS treatment. In Greece, tofacitinib showed comparable quality-adjusted life-years (QALYs) to adalimumab in biologic-naïve patients, with an incremental cost-effectiveness ratio (ICER) of €41,378 per QALY. In biologic-experienced patients, tofacitinib had higher total costs than secukinumab but yielded a 0.13 QALY gain, resulting in an ICER of €42,784 per QALY. Sensitivity analyses supported these findings, reinforcing the potential value of JAKi in axSpA treatment. 71
Furthermore, retrospective and economic evaluations in diverse settings underscore the cost-saving potential of lower-cost generic JAKi like tofacitinib. In one US managed care study analysing data from 20,159 patients (aged 18–63 years with RA, PsO, PsA or AS), the average 1-year treatment cost for patients with RA taking tofacitinib was $18,769, markedly lower than the $23,682-$30,269 observed for other biologic therapies, such as adalimumab, etanercept and infliximab. 72 Another US study using a decision-tree model in 1,321 RA patients found that tofacitinib combination therapy after methotrexate failure resulted in a per-member per-month cost of $5.53, compared to $6.49 for adalimumab and $6.43 for etanercept. 73
In Japan, a cost-effectiveness analysis employing a Markov model in biologic-naïve patients with moderate-to-severe ulcerative colitis demonstrated that a treatment regimen incorporating first-line tofacitinib was more cost-effective than biologics, including vedolizumab, infliximab, adalimumab, golimumab and ustekinumab, yielding favourable ICERs. 74 Additionally, another US economic evaluation in RA confirmed that tofacitinib combination therapy maintained lower costs per responder compared with alternative regimens such as those based on adalimumab, etanercept, certolizumab and tocilizumab. 75 Collectively, these findings suggest that lower-cost generic JAKi like tofacitinib and UPA have the potential to significantly reduce treatment expenses and broaden access to effective therapy, particularly in resource-limited settings where high-cost biologic treatments may not be economically viable. JAKi may offer a cost-effective treatment option for axSpA, but it is important to note that drug costs can vary significantly based on healthcare systems, regional pricing and insurance coverage. Therefore, consulting local healthcare resources and considering individual patient factors is crucial when making treatment decisions. 69
Studies in RA demonstrate that JAKis, such as tofacitinib, baricitinib and UPA, exhibit high adherence and persistence.76–79 Their oral formulation, which provides an alternative to the injections required by many biologic therapies, may contribute to these favourable adherence outcomes. Although adherence data, specifically in axSpA, are limited, these findings suggest that the oral route may similarly benefit axSpA patients by enhancing treatment compliance and overall outcomes. Thus, based on the robust adherence observed in RA, JAKi show promise as a potential therapy for axSpA, warranting further investigation in this patient population.
Adverse Effects, Preparation and Monitoring of JAKi Therapy
Tests for active tuberculosis (TB), latent TB, hepatitis B infection and hepatitis C must be carried out on all patients before JAKi therapy.80–82 Administration of JAKi is not recommended if haemoglobin is <9 g/dl, absolute neutrophil count is <1,000/mm3 and absolute lymphocyte count is <500/mm3. 18 Concerns have been raised regarding a slight increase in the absolute risk of all-cause mortality, cardiovascular events, stroke and malignancy with tofacitinib compared to TNFi in older patients with RA. 36 In a phase 3B/4 US FDA-mandated clinical trial (ORAL Surveillance) conducted after tofacitinib approval, an imbalance was observed between tofacitinib and etanercept/adalimumab, with a higher rate of malignancies and MACE in patients with RA over 50 years of age, particularly those with cardiovascular risk factors. Furthermore, a dose-dependent increase in the risk of VTE was reported. 36
Cardiovascular Risk
Tofacitinib may be linked to an increased risk of cardiovascular events, particularly in patients with a history of atherosclerotic disease. The ORAL Surveillance trial, a large post-marketing open-label randomised study with a median follow-up of 4 years, enrolled 4,362 patients aged ≥50 years who were taking tofacitinib and had at least one risk factor for heart disease. 36 A post hoc analysis revealed an elevated risk of MACE in patients with a history of atherosclerotic disease. However, in patients without such a history, administering tofacitinib 5 mg twice daily did not show an increased risk of MACE compared to TNFi. 83 A nationwide registry from France found an increased incidence of MACE, including cardiovascular death, myocardial infarction, stroke and all-cause mortality, but the difference was not statistically significant (4.3 vs. 3.6 per 1,000 person-years, weighted hazard ratio [HR] 1.0, 95% confidence interval [CI] 0.7–1.5). 84 Similarly, the FDA reported an increase in nonfatal myocardial infarction (0.35 vs. 0.16 events per 100 person-years, HR 2.20, 95% CI 1.02–4.75) and a trend towards an increase in MACE that did not reach statistical significance (0.98 vs. 0.73 events per 100 person-years, HR 1.33, 95% CI 0.91–1.94). 36 Additionally, a large retrospective cohort study in Hong Kong found no significant difference in MACE between patients with RA taking JAKi and those taking TNFi. 85
Venous Thromboembolic
In the ORAL Surveillance trial, 4,362 patients with RA aged 50 years or older and with at least one cardiovascular risk factor were randomly assigned to receive either 5 or 10 mg of tofacitinib twice daily, or a TNFi. 36 During a median follow-up of 4 years, those receiving a higher dose of tofacitinib had a higher probability of developing venous thrombotic events and pulmonary embolism compared to those taking TNFi. 86 Risk factors for VTE included older age, a high body mass index of ≥35 kg/m² and a history of prior VTE or chronic lung disease. Several large observational studies have also suggested a possible increased risk of VTE with JAKi. A Swedish nationwide registry found more venous thrombotic events in patients taking JAKi compared to TNFi (11.3 vs. 5.2 events per 1,000 person-years). 87 A French registry also showed a higher number of venous thromboembolic events with JAKi compared to controls (6.0 vs. 3.3 events per 1,000 person-years), though the difference was not statistically significant (weighted HR 1.1, 95% CI 0.7–1.6). 84 A recent meta-analysis of 42 phase II/III double-blind RCTs, covering 6,542 patien-exposure years for JAKi and 1,578 for placebo, reported 15 VTE events with JAKi versus 4 with placebo. The pooled incidence rate ratios (IRRs) were 0.68 (95% CI 0.36–1.29) for overall VTE, 0.44 (95% CI 0.28–0.70) for pulmonary embolism and 0.59 (95% CI 0.31–1.15) for deep vein thrombosis, indicating no increased VTE risk with JAKi compared to placebo. 88 The risk of venous thromboembolic events may be higher with certain JAKi; the ORAL Surveillance trial noted an increase in dose-dependent risk with tofacitinib. 36
Malignancy
The association between JAKi and malignancy risk remains inconclusive. Clinical trials evaluating approved JAKi, including baricitinib, tofacitinib and UPA, have not shown an increased malignancy risk compared to methotrexate or adalimumab.89–91 However, findings from the ORAL Surveillance study, which included patients aged 50 and older with elevated cardiovascular risk, indicated a higher incidence of malignancy, particularly lung cancer and lymphoma, among patients receiving tofacitinib compared to those treated with TNFi (1.13 vs. 0.77 events per 100 person-years, HR 1.48, 95% CI 1.04–2.09). 36 Lung cancer was predominantly observed in current or former smokers. A post hoc analysis further suggested an increased incidence of malignancies, including non-melanoma skin cancer, in tofacitinib users, with the highest rates seen in patients with a history or elevated risk of atherosclerotic cardiovascular disease. 92 Moreover, a meta-analysis of 62 RCTs and 16 LTE studies across various diseases, covering inflammatory conditions: RA, PsA, psoriasis, axSpA, IBD and atopic dermatitis, in a total of 82,366 person-years of exposure to JAKi, reported that overall malignancy rates were similar to those with placebo or methotrexate but significantly higher than with TNFi (IRR 1.50, 95% CI 1.16–1.94). 93
Infection
Herpes zoster infections are more common with tofacitinib, occurring at a rate of 3.4 per 100 patient-years, higher than with csDMARDs or bDMARDs.89,94,95 Tuberculosis has also been reported with JAKi, with incidence rates of 0.1 to 0.22 per 100 patient-years, similar to bDMARDs, and primarily occurring in endemic regions.36,52,89,96 Opportunistic infections, including multidermatomal herpes zoster, oesophageal candidiasis, pneumocystis, cytomegalovirus and cryptococcal infections, occur at rates of 0.1 to 0.3 per 100 patient-years, comparable to bDMARDs.89,96,97
It remains uncertain whether the elevated risk of cardiovascular events and malignancies is exclusive to RA or also applies to axSpA. Additionally, it is unclear whether these risks are specific to tofacitinib or represent a broader class effect of JAKi. Until further data are available, the task force advises exercising caution when initiating JAKi, particularly in patients over 50 years old with at least one cardiovascular risk factor and those over 65 years old. 2
Pregnancy and Lactation
Tofacitinib is not recommended during pregnancy due to a lack of sufficient safety data. According to EULAR guidelines, it should be discontinued at least 2 months before conception. 98 The use of tofacitinib is also discouraged during breastfeeding, as data on its safety for infants remain limited. Given its small molecular size, it is likely to be excreted in breast milk at high concentrations. 98 A study reviewing 47 pregnancies exposed to tofacitinib reported seven spontaneous miscarriages, eight medical terminations and one congenital anomaly (pulmonic valve malformation). Among 25 live births, no anomalies were observed, while six cases were lost to follow-up. 99
Summary of Research on Various Types of JAK Inhibitors (JAKi).
Based on multiple phase II and III trials, JAKi have consistently demonstrated significant clinical benefits in patients with axSpA. These studies have shown that treatment with JAKi—most notably UPA—leads to substantial reductions in disease activity, as measured by the BASDAI, along with marked improvements in physical function (BASFI) and spinal mobility (BASMI). Patients receiving these agents experienced robust improvements in key endpoints compared to placebo, with statistically significant reductions in BASDAI scores and corresponding enhancements in quality of life. The consistent findings across various trials not only underscore the efficacy of JAKi in alleviating axial symptoms but also highlight their role in improving overall functional outcomes and patient-reported well-being. Taken together, the evidence suggests that JAKi represent an effective treatment option for axSpA, providing comprehensive therapeutic benefits by reducing disease burden and enhancing daily functioning. Detailed improvements in BASDAI, BASFI, and BASMI scores following treatment with JAK inhibitors are summarized in Table 2.
Improvements in BASDAI, BASFI and BASMI in Patients with Axial SpA Treated with JAK Inhibitors (JAKi).
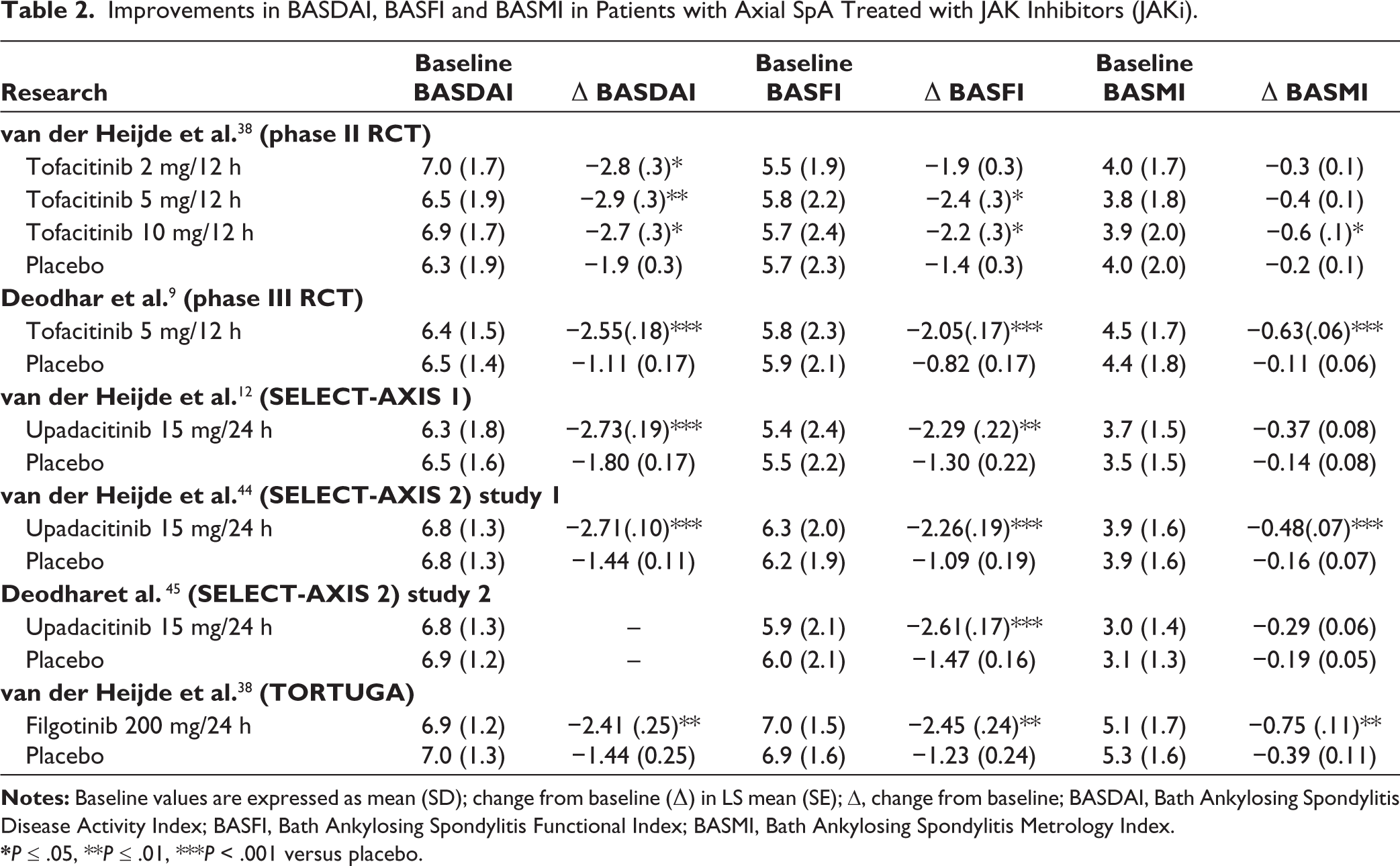
*P ≤ .05, **P ≤ .01, ***P < .001 versus placebo.
Additionally, emerging therapies for axSpA are being investigated, targeting novel pathways beyond conventional treatments. Genome-wide association studies suggest a role for TYK2 in spinal ankylosis. 100 Deucravacitinib selectively inhibits TYK2 signalling, showing efficacy and safety in psoriasis, with potential for broader immunological and inflammatory disease treatment, 101 though no TYK2 inhibitors are currently in clinical trials for axSpA.
MK2 inhibition has emerged as a potential strategy for controlling inflammation in axSpA while avoiding the toxicities associated with p38 inhibitors. CC-99677 showed promise in preclinical and phase I trials but lacked short-term efficacy in phase II.102,103 Another MK2 inhibitor, ATI-450, demonstrated a favourable safety profile in early trials. 104 MIF, a cytokine linked to inflammation and osteoblastic activity, is elevated in patients with axSpA and correlates with disease progression. 105 While MIF inhibitors have shown safety in early trials for other conditions, 106 their potential in axSpA remains unexplored. STAT3 inhibition, tested in preclinical models, improved inflammation and reduced IL-17A and TNF levels,20,107,108 suggesting a possible role in axSpA treatment. These novel targets hold promise but require further clinical validation.
Conclusion
SpA encompasses a group of chronic inflammatory diseases with a multifactorial pathogenesis involving various immune cell pathways and cytokines, particularly the JAK-STAT pathway. JAKi, such as tofacitinib, UPA and filgotinib, work by blocking this pathway and reducing the transcription of pro-inflammatory cytokines. In patients with persistently high disease activity despite conventional treatments, TNFi, IL-17i or JAKi should be considered according to current guidelines. Clinical studies have demonstrated that JAKi significantly improve disease activity and physical function in axSpA. Moreover, for patients with comorbid IBD where TNFi may not be suitable, tofacitinib offers an effective alternative due to its established efficacy in IBD. The oral administration of JAKi enhances patient compliance and, combined with favourable cost-effectiveness data, positions them as compelling alternatives to conventional biologic therapies. Although current safety profiles are encouraging, long-term studies and direct comparative trials are needed to fully establish their durability of efficacy, safety and economic benefits relative to TNFi and IL-17i. Overall, JAKi represent a promising therapeutic option for SpA patients, particularly those who are unresponsive to conventional or biologic treatments and possess additional comorbidities, such as IBD.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.