
Abstract
Long-term glucocorticoid therapy often results in a serious and common complication known as glucocorticoid-induced osteoporosis (GIOP). This condition is marked by accelerated bone degradation, reduced bone formation and a higher risk of fractures. This article delves into the fundamental mechanisms underlying GIOP, emphasising how glucocorticoids alter bone metabolism and various patient-specific risk factors. The comprehensive review covers the aetiology, consequences and current treatment strategies for GIOP, discussing established pharmacological interventions such as bisphosphonates, anti-receptor activator of NF-KB ligand (RANKL) antibodies and selective oestrogen receptor modulators (SERMs), along with promising new therapies like antisclerostin antibodies. Additionally, this article highlights the importance of nonpharmacological measures, including lifestyle changes, smoking cessation, alcohol moderation and engaging in resistance exercises, as essential components of a comprehensive treatment strategy. Evidence-based recommendations from expert guidelines aim to enhance patient care by improving bone density, preventing fractures and boosting overall health and quality of life for individuals undergoing glucocorticoid therapy. By adopting a multifaceted approach, the management of GIOP can be significantly improved, leading to better outcomes for affected patients.
Keywords
Introduction
Synthetic glucocorticoids (GCs) are artificially engineered drugs that replicate the functions of natural GC hormones produced by the adrenal cortex. These medications are extensively used to manage a diverse range of autoimmune and inflammatory diseases, including rheumatoid arthritis (RA), asthma and inflammatory bowel disease. They exert therapeutic effects by inhibiting inflammation and modulating immune responses. 1
Nevertheless, the prolonged use of synthetic GCs can precipitate several adverse effects, with corticosteroid-associated bone loss being one of the greatest significant concerns. This condition arises because of the disruption of bone remodelling processes, leading to diminished bone mineral density (BMD) and an increased likelihood of fractures, particularly in vertebral bodies, which are rich in trabecular bone. 2
Secondary osteoporosis is most commonly caused by glucocorticoid-induced osteoporosis (GIOP). Although this side effect is well-known, many patients do not receive adequate monitoring or appropriate treatment. 3 Osteoporosis is defined by changes in bone structure that lead to diminished BMD and a higher likelihood of fractures. In cases of GIOP, the increased fracture risk is not solely due to BMD changes; modifications in bone quality also contribute significantly. 4 This review focuses on GIOP, its causes, effects and management.
Prevalence and Population at Risk of GIOP
GCs continue to be extensively utilised for their anti-inflammatory, antiallergic and immunosuppressive properties in the treatment of inflammatory, chronic allergic, vasculitides and autoimmune diseases despite the advent of numerous immunosuppressive nonbiological and biological medications. 5 The link between excessive GC use and osteoporosis was first identified nearly 80 years ago; however, its clinical significance has only recently gained widespread recognition. 6 GIOP exhibits distinct characteristics, notably accelerated bone loss following the initiation of therapy, a heightened risk of fractures during this early phase and a concurrent suppression of bone formation alongside increased bone resorption in the initial stages of treatment. 7 Although awareness of GIOP among healthcare specialists has increased in recent years, multiple studies have indicated that the management of this condition remains suboptimal, highlighting ongoing challenges in clinical practice.8–10 Patients using GCs have a doubled risk of fractures, with an even greater likelihood of vertebral fractures. A comparative study involving 244,235 oral GC users and an equal number of controls identified a hip fracture risk of 1.6 and a vertebral fracture risk of 2.6, highlighting the significant impact of GC use on skeletal integrity, findings that have been consistently replicated in numerous research investigations. Among individuals receiving long-term GC therapy, the overall fracture prevalence is estimated to be 30%-50%. 11 There is a clear epidemiological association between GC therapy and fracture susceptibility. Oral GC therapy is prescribed to up to 2.5% of the older adults (70–79 years) for numerous health disorders, 12 and fractures may happen in 30%-50% of patients undergoing prolonged GC treatment. 13 Research in United Kingdom has revealed that 0.9% of adults use oral GCs, with the highest usage (2.5%) among those aged 70–79 years. 14 A recent study in the United States estimated the frequency of GC use to be 1.2%, primarily for extended periods, with infrequent concurrent use of bisphosphonates. These findings underscore the widespread use of GCs, despite their known side effects, including GIOP. 14 A retrospective United Kingdom study demonstrated that the prevalence of long-term oral GC use in the general population was estimated at 0.5%, rising to 1.7% in females aged 55 and older and reaching 2.5% in individuals over 70 years of age. 15 Importantly, only 4%-14% of patients taking oral steroids received osteoporosis treatment, suggesting that GIOP is often overlooked and untreated. 16
A comprehensive analysis of oral GC therapy demonstrated that the risk of fractures escalates rapidly within three to six months of initiating treatment with daily doses exceeding 5 mg of prednisone-equivalent, regardless of the underlying condition, patient age or gender. 17 In a research investigation of 551 long-term GC users, 37% experienced vertebral fractures and 14% had at least two clinically undetected spinal fractures. The prevalence varied by age, observed in 48% of patients aged 70 years and older and 30% of those younger than 60 years. A minimum of one VF event was observed in these age groups. The increase in prevalence with age underscores the importance of age-based preventive strategies. 18 Important relations were found between the total GC dose and BMD reduction as well as between daily dosages and fracture risk. An additional investigation revealed that higher daily doses (exceeding 10 mg/day), extended treatment duration (90 days or more) and uninterrupted GC use were associated with considerable risks of hip and vertebral fractures. 19 These findings underscore the rapid detrimental impact on trabecular bone, with vertebral fractures occurring more frequently during GC treatment than other common osteoporotic fracture sites. 20
According to previous studies, the increased risk of fractures due to GCs occurs rapidly after the initiation of treatment, particularly within the first three months, and decreases sharply after discontinuation. This is attributed to changes in bone remodelling and the induction of osteocyte apoptosis.21,22 The information also indicated a marked rise in fall frequency after the initiation of GCs. Epidemiological studies indicate that fracture risk is more strongly associated with the current daily GC dose than with cumulative exposure over time, possibly because of the difficulty in accurately calculating the cumulative dose. 23 The continuous use of GCs is related to an elevated susceptibility to hip fractures, underscoring the necessity of assessing osteoporosis and fracture risk in all patients. Loss of BMD occurs soon after the initiation of GCs and primarily affects the trabecular bone (e.g., spine). BMD loss persists in long-term GC users, albeit at a diminished rate over time. 24
Clinical Applications of Glucocorticoids
GC therapy is commonly administered via oral, intravenous or intramuscular routes, with doses typically ranging from 7.5 mg/day to 100 mg/day. An alternative approach, pulsatile administration, involves infusions of prednisone at doses between 250 mg/day and 1,000 mg/day over a duration of one to three days. 25 GCs are frequently prescribed for autoimmune diseases, including RA, systemic lupus erythematosus (SLE), severe dermatological conditions and inflammatory bowel disorders. 26 Nonetheless, prolonged systemic GC therapy, even at physiological doses, can result in substantial adverse effects, including characteristic physical changes (e.g., moon face, buffalo hump), suppression of the hypothalamic–pituitary–adrenal axis, gastrointestinal haemorrhage, glaucoma and cataract formation. 27 Short-term GC use has been linked to an elevated risk of sepsis, venous thromboembolism, decreased BMD and fractures. 28
Additional methods of GC administration, such as topical application, can also decrease BMD and increase fracture risk. These adverse effects on bone health can occur even with short-term or intermittent use of topical GCs, especially among vulnerable groups like elderly or those with preexisting osteoporosis. 28 The impact on BMD may be dose dependent and potentially reversible upon discontinuation of the medication. Regular monitoring of bone density and implementation of preventive measures, such as vitamin D and calcium supplementation, may be necessary in individuals receiving extended topical corticosteroid treatment. 29 For example, topical GCs, commonly used for psoriasis and atopic dermatitis, generally cause local complications, such as skin atrophy, 30 but a study showed that higher doses could increase the risk of major osteoporotic and osteoporosis fractures. 31 Inhaled corticosteroids (ICS) are commonly utilised in the management of obstructive airway diseases, can also have systemic adverse effects, particularly in severe cases requiring high doses and prolonged use. 32 One study found that women asthmatic patients using ICS for over six months experienced significant bone deterioration. 33 Intraarticular corticosteroid injections (IACS) used in hip and knee osteoarthritis are associated with increased risks, such as osteonecrosis and rapid joint destruction. Additionally, the prevalent adverse effects of GCs, including arterial hypertension, diabetes mellitus, immunosuppression and gastric ulceration, warrant careful consideration in treatment planning. 34
Mechanisms of Bone Loss
Bone remodelling is a dynamic and intricate procedure that involves coordinated actions of numerous cell types and signalling molecules. This physiological process plays a crucial role in preserving bone integrity, facilitating microdamage repair and adapting to mechanical loading. The quiescent state of the bone is characterised by a balance between osteoblasts and osteoclasts on the bone surface. When bone-resorbing stimuli, such as hormonal changes or mechanical stress, are present, osteoclasts are activated and begin to migrate to the targeted area. 3 These cells secrete enzymes and acids that break down both the organic matrix (primarily type I collagen) and inorganic mineral component (hydroxyapatite) of the bone, creating a resorption pit. Following the resorption phase, the formation phase begins, during which osteoblasts are recruited to the resorption pits. These cells synthesise and deposit a new bone matrix known as osteoid, which is primarily composed of type I collagen. 35 Over time, this newly formed osteoid undergoes mineralisation, incorporating phosphate ions and calcium to form hydroxyapatite minerals. This process restores the structural integrity and strength of bone. Once the remodelling cycle is complete, the bone returns to its quiescent state, with a new balance between osteoblasts and osteoclasts on the surface. GCs can significantly affect this remodelling process at various stages, affecting osteoclast and osteoblast activity, bone matrix production and mineralisation. Understanding these complex interactions is crucial for developing effective treatments for bone disorders and for managing the side effects of long-term GC therapy. 36
GIOP involves multiple mechanisms that donate to skeletal demineralisation and affect resorption and formation. On the resorption side, GCs enhance osteoclast activity by upregulating colony-stimulating factor-1 (CSF-1) and receptor activator of nuclear factor kappa B ligand (RANKL), while suppressing osteoprotegerin (OPG). This leads to increased breakdown of the bone tissue. 37 Simultaneously, GCs impair bone formation by inhibiting osteoblast generation, promoting osteoblast and osteocyte apoptosis and delaying osteoblast maturation. These effects lead to a reduction in the population of bone-forming cells and a functional impairment of mature osteoblasts. Additionally, GCs modulate mesenchymal stem cell differentiation, promoting adipogenesis at the expense of osteoblastogenesis, thereby further diminishing bone formation potential. 38 The effect of GCs on bone health extends beyond cellular mechanisms. GCs impair gastrointestinal calcium absorption, leading to a negative calcium balance, which exacerbates bone loss. This multifaceted assault on bone metabolism results in a characteristic pattern of BMD loss. Initially, there was a rapid failure in BMD through the course of treatment of GC. This is subsequently accompanied by a gradual decline in BMD over time, characterised by persistently elevated bone resorption and diminished bone formation. This ongoing imbalance in bone remodelling contributes to long-term skeletal fragility associated with GIOP, emphasising the critical role of early intervention and continuous monitoring in patients receiving GC therapy. 39
GCs exert multifaceted effects on bone health through both indirect and direct mechanisms. Their effects extend beyond bone cells and influence muscle function, calcium metabolism and overall bone mass. In terms of muscle health, GCs induce muscle atrophy by promoting protein breakdown and inhibiting protein synthesis. 37 This physiological process is influenced by the downregulation of insulin-like growth factor I (IGF-I) and the increased expression of myostatin, a growth factor known for its role in muscle catabolism. The consequent reduction in muscle mass and strength adversely affects skeletal integrity, leading to compromised bone structure, diminished bending resistance, and impaired postural stability. Collectively, these factors heighten the risk of falls, which, in turn, significantly contribute to the likelihood of fractures. 40
The result of GCs on skeletal remodelling was also significant. They interfere with calcium homeostasis by inhibiting calcium uptake in the intestine and reducing reuptake in the kidneys. This disruption results in hypocalcaemia, which, in turn, triggers hyperparathyroidism as a compensatory mechanism. Moreover, GCs directly impair bone mineralisation by suppressing the production of essential bone matrix proteins including osteocalcin and collagen. 41 These proteins are crucial for the maintenance of bone strength and integrity. The combined effects of muscle weakness, altered calcium metabolism and impaired bone mineralisation create a perfect storm for compromised bone health, making individuals undergoing long-term GC therapy particularly vulnerable to osteoporosis and fractures. 13
Glucocorticoid-induced Osteoporosis Prevention and Care
During the previous decade, numerous guidelines have been available for the prevention and treatment of GIOP. A globally recognised working group has recently established a framework aimed at standardising the care of individuals at risk for GIOP. The guidelines set forth by the American College of Rheumatology (ACR) emphasise the existing gap in knowledge regarding the long-term safety of bisphosphonates and teriparatide in patients undergoing extended GC therapy. Current expert consensus indicates a preference for short-acting agents, such as teriparatide, over bisphosphonates in premenopausal women of reproductive age, given specific therapeutic considerations. 41 Generally, the guidelines for managing GIOP follow a similar structure and can be divided into five stages (Table 1).
The Stages of GIOP Based on Guidelines.
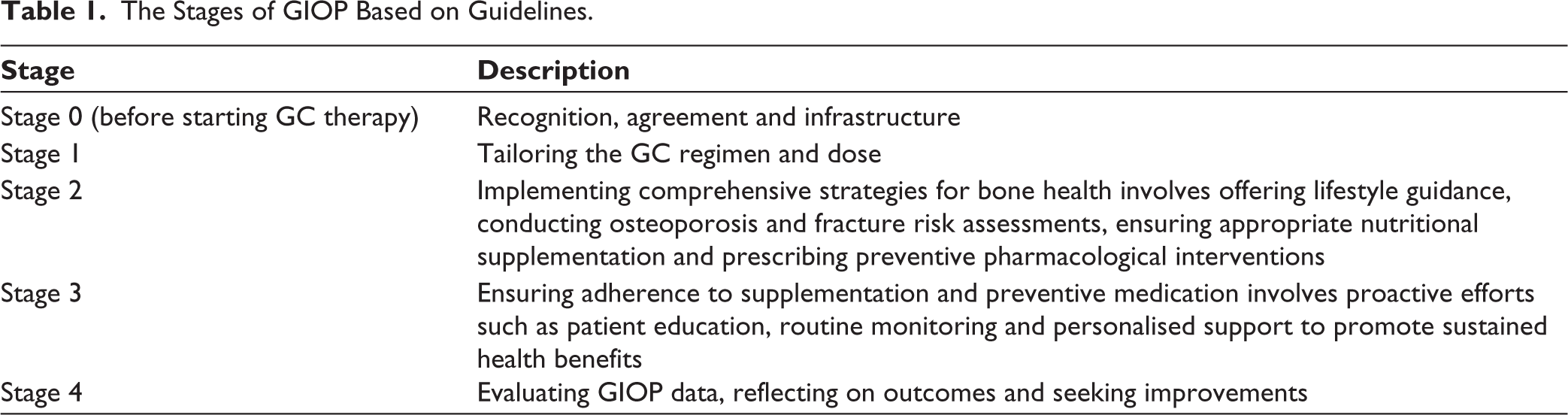
The stages of managing GIOP begin with stage 0 (awareness, agreement and infrastructure), which focuses on raising awareness about GIOP risks, establishing local protocols and ensuring consensus among healthcare professionals. Studies have indicated varying levels of treatment adherence and awareness across regions and patient groups. Menzies-Gow et al.’s findings highlight a significant gap in the implementation of bone-protective medication among individuals who require it. This underutilisation of crucial preventive treatment is a concerning issue in healthcare, as it leaves a substantial portion of the at-risk population vulnerable to bone-related complications and fractures. The reported range of 27%-40% suggests that, at best, only two out of five eligible patients receive the necessary medication, while at worst, just over one in four receive proper treatment. 15 Nevertheless, research—including studies focusing on postmenopausal women with osteoporosis—has indicated that a significant number of patients continue to go untreated. 42 Likewise, inadequate bone health management has been observed in particular patient populations, including community-based cohorts of individuals with SLE and RA undergoing GC therapy. 43
This discrepancy between recommended care and actual practice may stem from various factors, including inadequate screening protocols, lack of awareness among healthcare providers or patients, concerns about medication side effects or systemic barriers to accessing treatment. The low adherence rate also raises questions about the long-term health implications for those who do not receive bone-protective medication despite meeting the criteria for its use. Addressing this gap in care could potentially lead to significant improvements in bone health outcomes, reduced fracture rates and overall better quality of life for at-risk individuals. 44
Stage 1: Tailoring the GC regimen and dose involves evaluating and adjusting the GC regimen to minimise adverse effects including the risk of GIOP. 45
Stage 2: Lifestyle guidance, screening and supplementation strategies encompass patient education on essential health aspects, including maintaining a balanced diet, smoking cessation, fall prevention measures and the appropriate intake of vitamin D and calcium to support optimal bone health. Depending on the fracture risk, medications, such as bisphosphonates and teriparatide, may be prescribed. The need for medication, particularly bisphosphonates, should be determined based on fracture risk, teriparatide as an alternative treatment for GC-treated patients. 46 Although effective therapies for postmenopausal osteoporosis show potential for treating GIOP, their efficacy has not yet been fully established. The optimal management of GIOP in children undergoing GC therapy, young adult men and premenopausal females remains uncertain and requires further investigation. 47
Stage 3: Addressing compliance and adherence emphasises the importance of patient adherence to prescribed supplements and preventive medications, highlighting the challenges in ensuring consistent medication intake. 48
Stage 4: GIOP data evaluation, reflection and search for improvement focus on collecting data on treated patients to evaluate strategies, reflect on outcomes and seek improvements in GIOP management. It also involves assessing the cost-effectiveness and implementing programmes to enhance treatment safety. 49
The management of GIOP encompasses a multifaceted approach that addresses both the underlying causes and the potential consequences of bone loss linked to with GC therapy. A fundamental aspect of GC therapy optimisation is the strategic administration of the lowest effective dose for the shortest feasible duration while ensuring the desired therapeutic benefits. This method is essential in mitigating adverse effects on bone health and preserving skeletal integrity. 13 Vitamin D supplementation and calcium play a vital part in maintaining bone density and strength, as these nutrients are essential for proper bone metabolism. 50 Lifestyle modifications, such as smoking cessation, limiting alcohol consumption and regular weight-bearing exercises, can further support bone health and reduce fracture risk. 51
Pharmacological interventions form the cornerstone of GIOP management, with bisphosphonates being primary therapeutic approach for most patients. These pharmacological agents function by suppressing bone resorption, thereby contributing to significant improvements in BMD and a reduced risk of fractures in individuals affected by GIOP. 46 Other treatment options, such as denosumab or teriparatide, may be considered for patients with elevated health risks or those who cannot tolerate bisphosphonates. Regular monitoring of BMD through dual-energy X-ray absorptiometry (DXA) scans and assessment of fracture risk using tools like Fracture Risk Assessment Tool (FRAX) allows healthcare providers to track treatment progress and adjust management strategies as needed. Patient education is also crucial as it empowers individuals to actively participate in their care by understanding the importance of adherence to treatment plans and adopting healthy behaviors. 25
Optimising Glucocorticoid Therapy
To minimise adverse effects on bone health, the most effective approach in GC therapy is to use the smallest effective dose for the briefest period required to manage the underlying condition. This strategy helps reduce the risk of significant increased fracture and bone loss susceptibility related to long-term use of GCs. By limiting both the amount and duration of GC treatment, medical professionals can effectively balance the management of a patient’s condition while reducing potential risks to bone health. 52
In alignment with most clinical guidelines, the recommended daily dose of GCs for therapeutic intervention is generally established at 7.5 mg of prednisolone or its equivalent. In cases where a baseline evaluation is unavailable, it is advised to perform a fracture risk assessment promptly, preferably within the initial six months of GC therapy initiation. Additionally, periodic reassessment of the fracture risk is recommended. 4
The initial fracture risk assessment should incorporate a comprehensive clinical history, encompassing details such as GC therapy dosage and duration, prior low-energy fractures, fall history, alcohol consumption, smoking habits, height reduction and underlying secondary causes of bone loss. 53 In addition, history of osteoporosis and hip fractures in relatives should be considered. It is essential to assess other risk factors and comorbidities that may contribute to bone fragility. Ensuring adequate calcium intake and correcting vitamin D deficiency are critical components of this assessment. Furthermore, a comprehensive evaluation should include an analysis of physical activity status of the patient and nutritional status, as these factors have a major impact in bone health. Regular monitoring and reassessment are recommended to promptly identify any changes in fracture risk and adjust the management plan accordingly. 54
The International Society for Clinical Densitometry recommends vertebral fracture assessment (VFA) or lateral spinal radiography for patients undergoing GC therapy at a dosage equivalent to or greater than a daily dose of 5 mg of prednisone sustained for three months or longer. 55 These radiological studies are instrumental in detecting both pre-existing and new vertebral fractures, as well as additional pathologies, such as osteoarthritis. It is essential to recognise that fractures can occur in GC-treated patients, even when their BMD is higher than expected. This phenomenon is largely due to the impairment of the bone microarchitecture, which significantly contributes to an elevated likelihood of fractures. 46
The FRAX algorithm is also a computer-based tool designed to estimate decade-long risk assessment for major osteoporotic fractures (clinical spine, hip, wrist or humerus) and hip fractures by analysing individual clinical risk factors, with or without femoral neck BMD, in patients aged 40 years and above. 56 This assessment incorporates a straightforward yes/no variable to determine oral GC usage, specifically identifying patients who are either currently receiving treatment or have been exposed for over three months at a daily dosage of 5 mg of prednisolone or higher. 57 Despite its clinical utility, FRAX does not incorporate treatment duration, concurrent GC dosage or key fracture risk factors, including the severity of underlying inflammatory conditions, vertebral deformities or fall susceptibility. Furthermore, FRAX utilises femoral neck BMD as its primary assessment metric, even though GCs exert a greater adverse impact on trabecular bone within the lumbar spine. 40
Humphrey et al. provided recommendations based on an updated systematic literature review that considered nonpharmacological and pharmacological treatments, medication discontinuation and sequential therapy. They reached a consensus of over 70% on the strength and direction of these recommendations. For adults beginning or continuing GC treatment lasting more than three months, it is strongly suggested to assess fracture risk as soon as possible. This includes clinical fracture assessment, BMD evaluation with VFA or spinal radiography and FRAX for those aged ≥ 40 years. For individuals with a medium to extremely high likelihood of fractures, pharmacological treatment with oral or intravenous bisphosphonates, denosumab or parathyroid hormone analogues is strongly recommended, with the choice of treatment guided by shared decision-making. The use of anabolic agents is conditionally advised for individuals presenting with high or very high fracture risk, based on clinical recommendations. Special recommendations are provided for children, organ transplant recipients, individuals who may become pregnant and those receiving high-dose GC treatment. The guidelines also include new recommendations for the discontinuation of osteoporosis and sequential therapies. 52
Pharmacological Therapy
The complex interplay between inflammation, hormonal changes and medication side effects necessitates a multifaceted approach for managing GIO symptoms. Although oestrogen suppression has shown promise in addressing menopausal bone loss, its efficacy in GIO treatment remains poorly understood. 4 The recognition that GIO can occur due to subcutaneous inflammation, regardless of GC antidepressant use, highlights the need for targeted interventions that address both underlying inflammatory processes and bone density loss. Therefore, risk assessment and drug therapy candidates are of particular importance. 20
Multiple pharmacological agents have demonstrated efficacy in mitigating bone loss in the spine and hip among patients initiating GC therapy. These include alendronate (oral administration at a dosage of 5 or 10 mg per day or 70 mg per week), zoledronate (given as a 5 mg intravenous infusion annually) and risedronate (administered orally at 5 mg per day or 35 mg per week). Additionally, these drugs have been shown to enhance BMD in patients undergoing extended GC treatment. 58 In a subsequent investigation conducted by Laurent et al. during the following year involving 208 of the initial 477 participants, the occurrence of new vertebral fractures was markedly reduced in the cohort receiving alendronate (0.7%) compared to the placebo group (6.8%), demonstrating its efficacy in fracture prevention. 10 A study evaluating alendronate against placebo involved 477 participants over a 48-week period. The lumbar spine exhibited BMD increases of 2.1% and 2.9% in the groups receiving 5 mg and 10 mg of alendronate, respectively, whereas the placebo group experienced a 0.4% decline. Changes observed in the femoral neck were +1%, +1.2% and −1.2% across the same respective groups. Notably, in the placebo group supplemented with calcium and vitamin D, the reduction in BMD was found to be correlated with the duration of GC therapy, with values of −2.9%, −1.4% and +0.8% for patients undergoing GC treatment for less than four months, between four and twelve months, and beyond twelve months respectively. 59
All GIOP guidelines concur that in patients undergoing GCs treatment who have an intermediate to elevated fracture risk, bisphosphonates are the first-line antiosteoporotic medications for preventing new fractures. Oral bisphosphonates such as risedronate and alendronate are commonly used in clinical practice because of their antiresorptive effects on osteoclasts. 53 However, the equivalence ratio of prednisolone remains unclear. Teriparatide and bisphosphonates have been assessed for their roles in the treatment and prevention of GIOP. Nevertheless, several issues remain regarding its efficacy. Notably, fracture incidence was not designated as the primary endpoint in any of these studies; rather, the focus was placed on BMD as the key outcome measure. 60 The study duration was relatively short, averaging around one year, and included a low number of males and premenopausal females. Consequently, the effectiveness of these treatments in fracture reduction is predominantly derived from bridging data, which compares short-term variations in BMD among patients undergoing GC therapy with long-term BMD changes and fracture risk reduction observed in individuals with postmenopausal osteoporosis. 53 Additional pharmacological investigations are required to assess whether deflazacort exhibits enhanced immunosuppressive activity, potentially elevating the risk of opportunistic infections in comparison to other synthetic GCs.
A Cochrane systematic review conducted by Allen et al. examined 23 randomised trials involving over 2,000 patients with GIOP, assessing the comparative efficacy of bisphosphonates versus calcium and vitamin D supplementation alone. Findings indicated a 3.5% increase in lumbar spine BMD in the bisphosphonate-treated cohort over one year, whereas the control group exhibited an approximate 3.2% reduction in BMD. 61 In a systematic review, Messina et al. described that most investigations featured longitudinal follow-up period of less than 12 months, with only nine extending up to two years. Extended follow-up studies revealed a sustained increase in BMD of 5.5% in the BP-treated group. 7 Two studies indicated that bisphosphonates are effective in reducing fracture rates, showing significantly better outcomes when antiosteoporosis medication is initiated within the first 90 days of prolonged GC treatment. These studies documented a 48% reduction in fracture incidence, highlighting the effectiveness of the interventions in mitigating fracture risk.10,62 Bisphosphonates should be administered with caution in premenopausal females due to their ability to cross the placenta. If treatment with bisphosphonates is deemed necessary, appropriate contraceptive measures should be implemented. Additionally, it is advisable to opt for bisphosphonates with shorter bone half-lives to mitigate potential risks. 63 The effectiveness of bisphosphonates in fracture prevention rates in GIOP has been a subject of debate in the medical community. While several studies have demonstrated positive outcomes, suggesting that bisphosphonates can significantly reduce fracture occurrence in patients with GIOP, other research findings have cast doubt on these conclusions. This discrepancy in results highlights the complex nature of GIOP and the challenges in its management.64,65 The gap between GIOP management strategies and tangible improvements in patient outcomes remains a significant concern. This disconnect may be attributed to various factors, including differences in study designs, patient populations, dosing regimens and duration of treatment. Additionally, the multifaceted nature of GIOP, which involves not just bone loss, but also changes in bone quality and muscle strength, may contribute to the inconsistent results observed across studies. More studies are necessary to bridge this gap and develop more comprehensive and effective treatment approaches that can consistently translate into improved patient outcomes, such as reduced fracture rates and enhanced quality of life for individuals affected by GIOP. 20
Recent research has focused on the potential of phosphodiesterase 4 (PDE4) inhibitors in managing GIOP symptoms in immunosuppressed RA patients. These agents show promise in mitigating inflammatory cascades that contribute to collagen degradation and antigen–antibody complex infiltration, potentially offering a novel approach to GIOP treatment. 66 Additionally, GC-elimination agents and bone-forming therapies like teriparatide have demonstrated efficacy in enhancing BMD while mitigating fracture risk in both men and women with primary osteoporosis. As research progresses, the development of pharmacotherapies targeting specific molecular pathways involved in bone metabolism and inflammation may provide more impactful and personalised treatment options for RA patients experiencing GIOP. However, additional clinical trials are crucial to determine the long-term efficacy and safety of these interventions, as well as to assess their influence on patients’ quality of life and overall clinical outcomes. 67
Calcitonin
Calcitonin, a hormone with bone-protective properties, is employed as a therapeutic agent in the management of GIOP. It functions by inhibiting osteoclasts, promoting the activity of osteoblasts, and the cells responsible for bone resorption, which are bone-forming cells. This mechanism helps preserve bone mass and reduce bone loss, especially in the lumbar spine. 68 As reported by Madamsetty et al. 69 and Ukon et al. 70 the therapeutic effects of calcitonin correspond with the pathogenic pathways of steroid-induced osteoporosis, particularly in relation to the decline in endogenous calcitonin production following glucocorticoid administration. However, it is important to note that while calcitonin can help maintain bone mass, its effectiveness in preventing fractures is not well established. Additionally, calcitonin is not typically used as a first-line treatment because of the availability of more effective drugs such as bisphosphonates. Furthermore, prolonged administration of calcitonin has been linked to an elevated risk of certain malignancies, raising concerns regarding its long-term safety profile. 10
Vitamin D
Vitamin D is essential in managing GIOP by promoting intestinal calcium absorption, which is vital for bone health. Sufficient vitamin D levels correlate with higher BMD, thereby lowering fracture risk. Multiple studies have demonstrated a correlation between active vitamin D and improved BMD, alongside a decreased risk of vertebral fractures. 71 However, infrequent high-dose vitamin D supplementation (A monthly dose of 60,000 IU or an annual total of 500,000 IU) has been linked to with elevated fracture and fall risk. Consequently, the advised daily vitamin D dosage should not exceed 4,000 IU under normal circumstances. For patients undergoing long-term GC treatment, vitamin D supplementation (typically 600–800 IU daily or more in cases of deficiency) is advised to maintain adequate levels. 72 Vitamin D, when complemented by calcium, plays a vital role in preserving bone integrity, particularly in individuals with diminished bone density or a heightened susceptibility to fractures. Together, these nutrients help to maintain muscle strength and overall bone health, counteracting the negative effects of GC therapy. 50 Laurent et al. recommended that patients on GC medication maintain a serum level of 25-hydroxyvitamin D greater than 20 ng/mL to ensure sufficient vitamin D and calcium status, thereby reducing the fracture incidence risk. Their findings indicated that vitamin D plays a crucial role in regulating calcium metabolism, encompassing renal excretion, bone resorption and intestinal absorption. 10
Calcium
Calcium serves as a fundamental component in the management of GIOP, promoting bone health through its essential role in enhancing mineralisation and structural integrity. For individuals undergoing prolonged GC treatment, a daily calcium supplementation of 800–1,200 mg is recommended to mitigate the reduced calcium absorption associated with these medications. 73 However, it is important to note that excessive calcium intake exceeding 1,500 mg per day may have adverse effects, including an increased likelihood of kidney stone formation. 74
Vitamin D Supplements and Calcium
Since GIOP impairs calcium absorption in the gastrointestinal tract, supplementing with calcium and vitamin D represents a logical and clinically effective strategy to mitigate deficiency and support bone health. These supplements enhance calcium absorption, which is crucial for sustaining bone density and function. 75 Optimal vitamin D levels are linked to enhanced BMD and a lower incidence of fractures, reinforcing its essential role in skeletal health. For individuals undergoing prolonged GC therapy, supplementation with calcium (800–1,200 mg per day) and vitamin D (600–800 IU daily) is advised to maintain adequate levels and mitigate bone loss. Together, these supplements contribute to the maintenance of muscle strength and overall bone health, mitigating the adverse effects of GC treatment. 76 Adequate calcium intake, along with vitamin D intake, supports bone preservation and minimises fracture susceptibility. However, it is important to balance the calcium intake to avoid excessive consumption, which can lead to kidney stones and other health issues. 77
Denosumab
Denosumab is an effective treatment for GIOP. It is a monoclonal antibody that suppresses RANKL, a crucial regulator of bone resorption, thereby aiding in the preservation of skeletal integrity. By inhibiting RANKL, denosumab increases BMD and reduces bone turnover markers. 78 Research findings indicate that denosumab exhibits superior efficacy compared to bisphosphonates in enhancing BMD at the lumbar spine and ultra-distal radius.59,79,80 Additionally, Zhao et al. reported that denosumab effectively improves BMD and mitigates fracture risk in individuals affected by GIOP. 81 It is considered a favourable therapeutic option with a good safety profile for patients undergoing long-term GC therapy. Denosumab can be used when bisphosphonates are inappropriate or well tolerated. As the sole RANKL inhibitor approved for osteoporosis treatment, it has exhibited substantial efficacy in enhancing BMD and mitigating fracture risk.82,83
Menatetrenone
Vitamin K2 (menatetrenone) is an emerging treatment for GIOP. It plays an essential part in bone metabolism by activating osteocalcin, a protein involved in bone mineralisation. 84 Research indicates that vitamin K2 may positively influence bone turnover markers and contribute to improved BMD in individuals receiving GC therapy.85,86 Menaquinone, commonly known as vitamin K2, is believed to facilitate the gamma-carboxylation of osteocalcin, a critical process in bone matrix formation mediated by osteoblasts. Elevated serum levels of undercarboxylated osteocalcin, which may serve as an independent fracture biomarker, have been identified as a risk factor for fractures in older females. 87 However, Shikano et al. reported that the effect of vitamin K2 on likelihood of fractures reduction remains inconclusive. Vitamin K2 may be particularly beneficial for patients with systemic autoimmune diseases who are on long-term GC treatment. 88 Additionally, Kong et al. 33 and Hu et al. 89 found that menatetrenone supplementation effectively lower serum levels of undercarboxylated osteocalcin, a key marker related to with bone metabolism and fracture risk.
Teriparatide
Teriparatide, a recombinant parathyroid hormone, represents a significant advancement in GIOP treatment. Unlike antiresorptive agents, which primarily inhibit bone breakdown, teriparatide takes a unique approach by actively stimulating bone formation. 90 This anabolic effect is achieved through the direct activation of osteoblasts, which are responsible for synthesising new bone tissue. By enhancing osteoblast function, teriparatide not only increases BMD, but also improves bone microarchitecture, leading to enhanced bone strength and quality. 91
The efficacy of teriparatide in GIOP management has been exhibited in various clinical studies, which have shown significant reductions in both vertebral and nonvertebral fracture risks.92–94 This broad-spectrum fracture prevention is particularly valuable in patients, who often experience systemic bone loss. Teriparatide’s effectiveness in inducing new bone synthesis makes it an attractive option for patients who have experienced inadequate responses to other osteoporosis treatments, such as bisphosphonates. 95 Additionally, its anabolic mechanism of action may be especially beneficial in counteracting the catabolic influence of GCs on bone metabolism, potentially offering a more targeted approach for GIOP treatment. However, it is significant to note that the use of teriparatide is typically limited to a specific period owing to safety considerations, and its optimal positioning within the overall treatment strategy for GIOP continues to be an area of ongoing research and clinical discussion. 96
Other Medicines
Recent advancements in the treatment of GIOP have expanded the therapeutic options available to both patients and healthcare providers. The introduction of abaloparatide and romosozumab represents a significant step forward in addressing challenges associated with GIOP. 97 Abaloparatide, a synthetic analogue of parathyroid hormone-related protein (PTHrP), promotes osteogenesis, enhances skeletal strength and lowers the likelihood of fractures. 98 In contrast, romosozumab, a monoclonal antibody directed against sclerostin, operates via a dual mechanism, simultaneously stimulating bone formation and suppressing resorption, thereby enhancing BMD. 99 These novel therapies offer promising alternatives for patients who may not achieve optimal results with conventional treatments such as bisphosphonates or denosumab. The availability of these new options allows for more personalised treatment approaches, taking into account individual patient factors, such as disease severity, comorbidities and treatment history. 100 Furthermore, the unique mechanisms of action of abaloparatide and romosozumab may provide benefits in terms of bone microarchitecture and overall skeletal health that were previously unattainable with the existing therapies. As research in this field continues to evolve, it is likely that these new treatments will play an increasingly fundamental part in the management of GIOP, potentially improving the long-term outcomes and quality of life of affected individuals. 101
Lasofoxifene, a third-generation selective oestrogen receptor modulator (SERM), has already gained approval in Europe for osteoporosis treatment and has demonstrated remarkable efficacy in decreasing nonvertebral fractures and both vertebral. 102 Other potential treatments include cathepsin K inhibitors like odanacatib, which target osteoclast activity to support bone formation, although research on this particular drug was discontinued due to stroke risk concerns. 103 Interestingly, donepezil, an acetylcholinesterase (AChE) inhibitor primarily used for Alzheimer’s patients, has demonstrated potential in enhancing bone turnover while lowering the incidence of hip fractures in individuals with GIOP. 104
Sclerostin, a protein secreted by osteocytes and osteoclasts, suppresses osteoblast function by inhibiting the Wnt/β-catenin signalling pathway, thereby regulating bone formation. Romosozumab, an antisclerostin antibody, has shown in phase three clinical trials to increase BMD more effectively than alendronate and teriparatide. 105 Additionally, various herbal remedies have demonstrated potential in improving therapeutic effects and enhancing osseous density in GIOP individuals.60,106
To guide clinicians in managing GIOP, expert organisations have developed comprehensive guidelines. The Oxford Centre for Evidence-Based Medicine (CEBM) provides graded recommendations based on the consistency of studies, while the ACR 2017 guidelines outline appropriate prednisone dosages and treatment durations. These advancements in both pharmacological interventions and clinical guidelines collectively aim to improve the management and patient well-being suffering from GIOP. 53
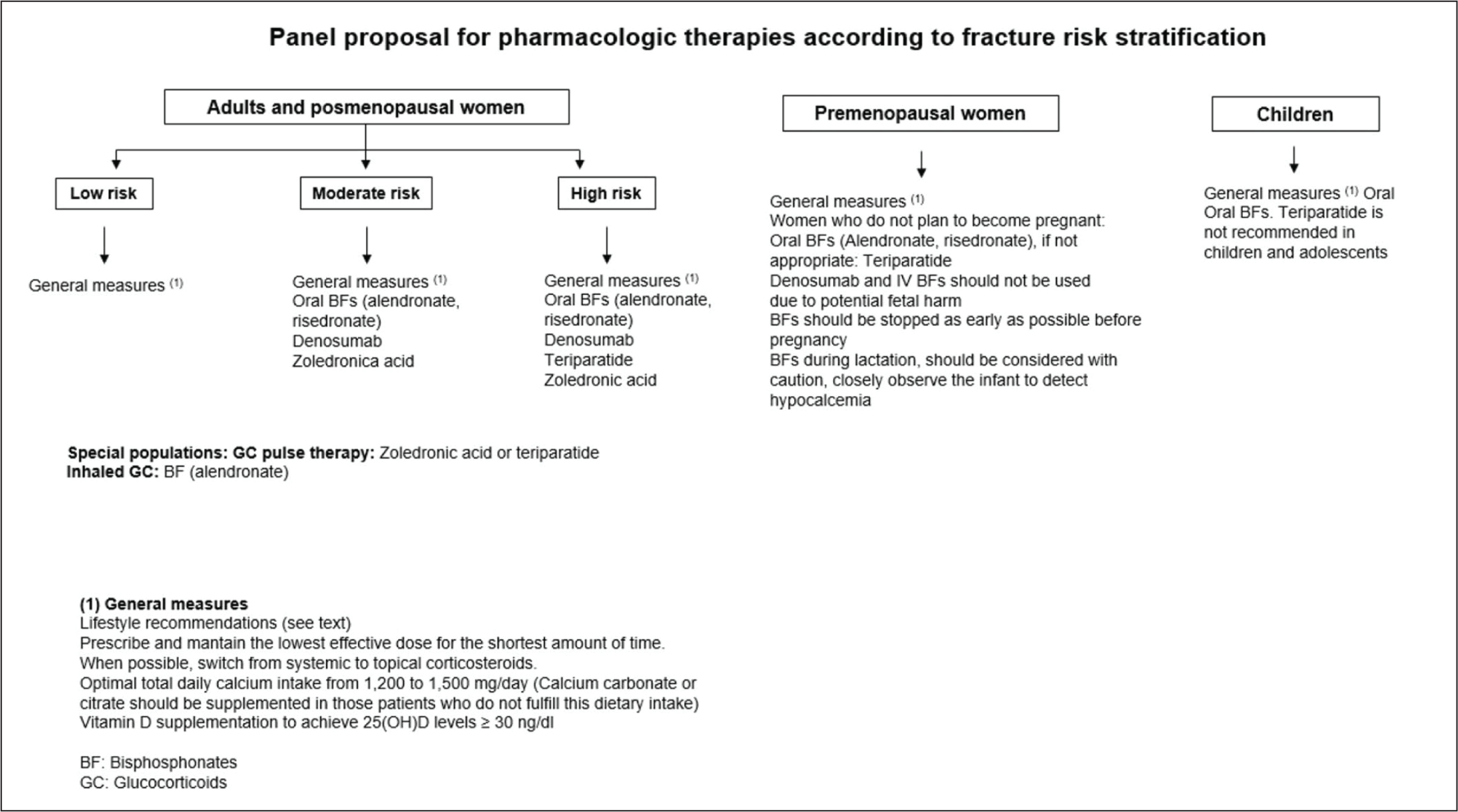
Various expert organisations have established guidelines for the prevention and management of GIOP, offering evidence-based recommendations to support healthcare professionals in clinical decision-making. The Colombian Association of Rheumatology, 2023, has played a crucial role in this process by offering graded recommendations based on the consistency of available studies. These guidelines aim to standardise care and improve patient outcomes by providing clear, actionable advice for clinicians managing GIOP (Figure 1). 51
Guidelines for GIOP by Colombian Association of Rheumatology. 51

Specific examples of such guidelines include the ACR 2017 protocols and the Brazilian Guidelines 2021, which offer detailed recommendations on GIOP management. These guidelines address critical aspects such as appropriate prednisone dosages and optimal treatment duration, taking into account factors like patient age, fracture risk and underlying conditions. By providing comprehensive guidance on prevention strategies, monitoring protocols and treatment options, these guidelines contribute to a more standardised and effective approach to GIOP management. Furthermore, the continuous development of new therapies and treatment modalities, informed by ongoing research, enhances the potential for improved clinical outcomes and patient well-being affected by GIOP (Figure 2). 107
Guidelines for the Prevention and Management of GIOP by ACR and the Brazilian Protocols. 107
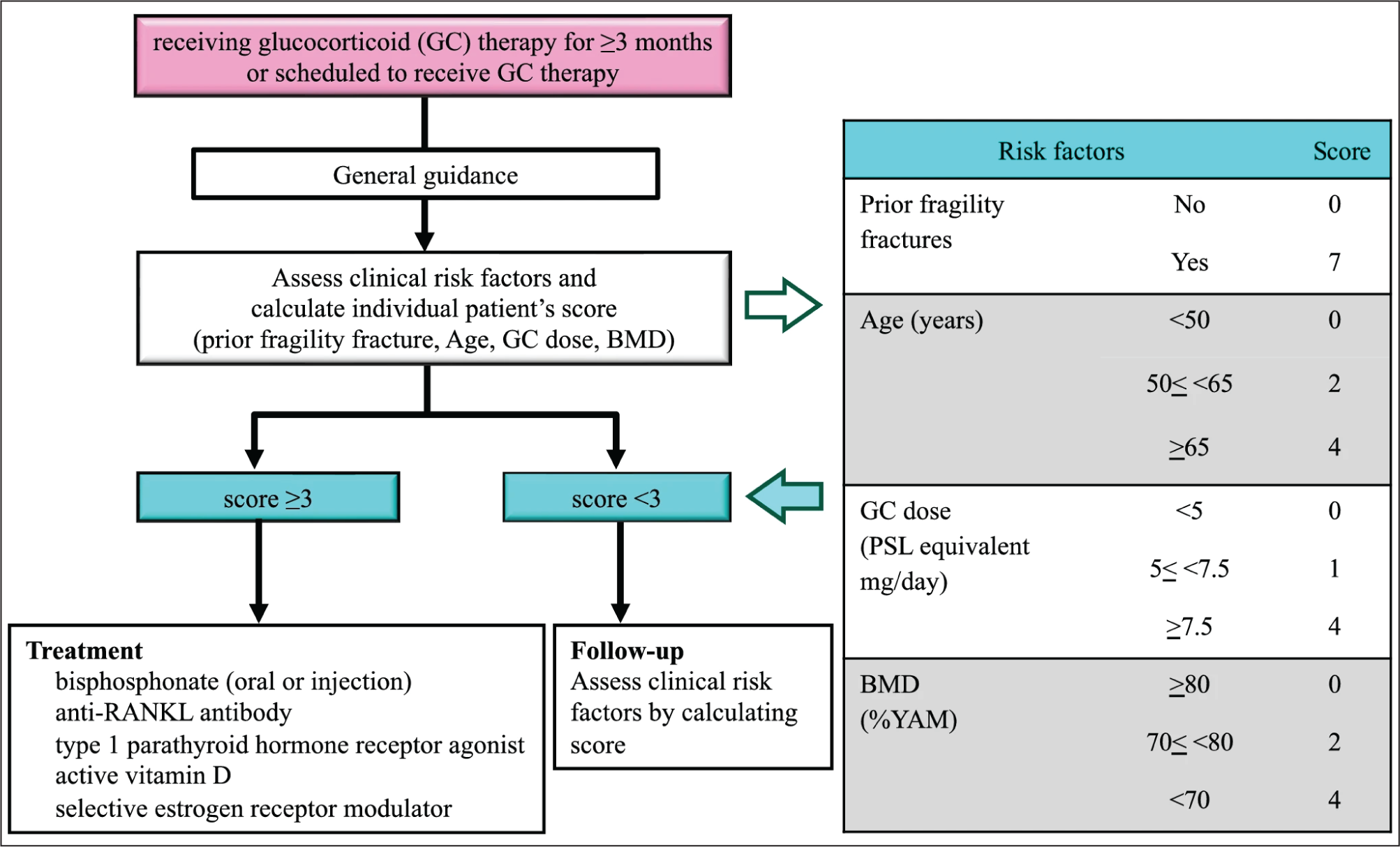
The Japanese Society for Bone and Mineral Research (JSBMR) Committee updated its guidelines for the management and treatment of GIOP by incorporating the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) framework, alongside systematic reviews and expert consensus using the Delphi method. The 2023 recommendations advocate for the administration of bisphosphonates, anti-RANKL antibodies, teriparatide, eldecalcitol or SERMs in patients with a risk factor score of three or higher, based on the criteria established in the 2014 algorithm. They also include general guidance for individuals scheduled to receiving or currently undergoing GC therapy, emphasising the concurrent use of osteoporosis medications (Figure 3). 46
Guidelines of JSBMR for GIOP. 46
Nonpharmacological Approaches to Managing GIOP
Nonpharmacological interventions for GIOP are essential to mitigate the long-term complications GC use on bone health. The initial step involves assessing the patient’s risk factors, which include the GC dosage and period of use, patient gender, age, history of previous bone fractures and any other conditions that are related to decreased bone density. This comprehensive evaluation helps healthcare providers develop personalised prevention and treatment plans. 108
Lifestyle modifications are fundamental in managing GIOP. Patients should aim to consume a diet rich in vitamin D and calcium, which are critical for bone health. Supplements can also be beneficial to ensure adequate intake, along with sufficient vitamin D obtained from sun exposure. Regular engagement in load-bearing exercises such as walking, jogging or resistance training strengthens bones and muscles, helping to counteract the bone-weakening effects of GCs.95,109
Smoking cessation and alcohol moderation are also crucial. Smoking has been shown to heighten the likelihood of osteoporosis and interfere with bone healing, while excessive alcohol consumption can weaken bones and contribute to fractures and falls. Therefore, patients should be advised to cease smoking and reduce alcohol consumption to mitigate risk factors associated with osteoporosis and enhance overall bone health. 110
Implementing fall prevention strategies is particularly important for individuals undergoing treatment for GIOP. This encompasses optimising home lighting, eliminating tripping hazards and utilising assistive devices when necessary to enhance safety and prevent falls. Such measures can significantly reduce the risk of falls, which are a major cause of fractures in osteoporotic patients.111,112
Maintaining a balanced diet and a healthy body weight is vital for overall bone health. Extreme diets or rapid weight loss can lead to a decrease in bone density, so patients should focus on consuming a variety of nutrients and maintaining a stable, healthy weight. 112
Engaging in resistance exercises is highly beneficial for bone health. These exercises encompass diverse training modalities, including free weights, medicine balls, elastic bands and weight machines. Resistance training enhances overall health, physical fitness and athletic performance by engaging the primary muscle groups associated with the spine and hip. Compound movements like squats and deadlifts are especially effective, as they involve multiple muscle groups and help enhance both bone strength and overall physical fitness.113,114
By incorporating these nonpharmacological strategies, individuals with GIOP can improve their bone health, reduce the bone fragility risk and enhance their overall quality of life.
Conclusion
GIOP represents a notable and frequently overlooked complication associated with extended GC use. Grasping its aetiology, consequences and treatment is vital for reducing its influence on patients’ well-being. GIOP stems from the intricate interaction between GC-mediated changes in bone metabolism and individual risk factors. This condition results in enhanced bone breakdown, diminished bone formation and subsequent fractures. Successful GIOP management necessitates a comprehensive strategy. Pharmaceutical interventions, including bisphosphonates, anti-RANKL antibodies and SERMs, are crucial in combating bone loss and lowering fracture risk. Novel therapies such as antisclerostin antibodies and other experimental agents present fresh opportunities for enhancing bone health. Moreover, nonpharmaceutical approaches, encompassing lifestyle adjustments, tobacco cessation, alcohol limitation and strength training, constitute essential elements of a holistic treatment plan. Protocols established by expert organisations offer evidence-based guidance for GIOP prevention and treatment, ensuring optimal patient care. By incorporating these approaches, medical professionals can effectively address GIOP, improve bone density, avert fractures and ultimately enhance the overall health and quality of life for individuals undergoing GC therapy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.