
Abstract
Background:
YouTube, the second most visited website globally, is a major source of health information. While it holds educational potential, the prevalence of misleading medical content is concerning. This study evaluated the content, reliability and quality of YouTube videos on Ankylosing spondylitis (AS).
Methods:
In October 2024, a YouTube search using the keyword ‘Ankylosing spondylitis’ and the default ‘Relevance’ filter was conducted. The top 100 eligible English-language videos were included. Exclusion criteria were duplicates, non-English videos, irrelevant content, and YouTube Shorts. Reliability and quality were assessed using the modified DISCERN (mDISCERN) and Global Quality Scale (GQS) scores.
Results:
Of 120 videos screened, 20 were excluded (12 duplicates, 8 non-English). Among the 100 included, 89% were useful and 11% misleading. Useful videos had higher mDISCERN scores (median 3; range 2–3) than misleading ones (median 2; range 2–2) (P = .002) and higher GQS scores (median 4; range 3–4) compared to misleading ones (median 2; range 1.5–2.5) (P < .001). All videos by academic institutions, professional organisations and rheumatologists were useful. Misleading videos originated mainly from alternative system professionals, non-rheumatologist doctors and independent users. Despite lower quality, misleading videos had higher engagement. The median number of comments was significantly greater for misleading videos (161, range 53–306) than for useful ones (26.5, range 5.8–89.5) (P = .019), and they received more likes on average.
Conclusion:
YouTube is a valuable source of health information, but it lacks regulation of medical accuracy. Rheumatologists should collaborate with content creators to produce engaging, evidence-based videos. YouTube must prioritise reliable health content.
Introduction
In today’s world, the internet serves as one of the most widely used platforms for accessing health information. Online resources and social media are becoming increasingly significant in healthcare, with numerous patients relying on them for information. 1 YouTube is the world’s largest video-sharing platform and is also the second most visited website globally, following Google Search. 2 On average, more than one billion hours of YouTube content are seen by viewers every day. Given its reach, YouTube is a valuable educational tool that rheumatologists can utilise to inform patients about rheumatic conditions. It has been studied for this role in rheumatic conditions such as Sjogren’s syndrome, 3 Rheumatoid Arthritis (RA) 4 and Systemic Lupus Erythematosus (SLE). 5 While YouTube has tremendous potential as an educational tool, it also poses significant risks due to the prevalence of misleading information.4,6 Anyone can post a video about a medical condition, and YouTube lacks a system to check the source or content or filter the videos prior to publication. Concerns persist about the accuracy and quality of health information provided on YouTube. A study by Singh et al. found 30.4% of analysed videos about RA misleading and 73.9% of for-profit content inaccurate—highlighting the prevalence of misinformation and the need to address it in rheumatic diseases. 4 Ankylosing spondylitis (AS) is a chronic autoimmune inflammatory arthritis. It is a disabling form of spinal arthritis that typically begins before the age of 40 and occurs more frequently in males. Indian prevalence is estimated to be about 0.07%–0.1%. 7 YouTube features numerous videos about AS. Very few global studies have assessed the content, reliability or quality of YouTube videos related to AS, and none have focused on content presented to viewers in India. 8 YouTube is known to present different videos in different countries as per its algorithm based on demographics. Given YouTube’s region-specific algorithm and India’s diverse population, this study was undertaken to investigate the content, reliability and quality of health information pertaining to AS videos presented by YouTube to viewers in India.
Materials and Methods
This descriptive study was conducted from October 2024 to December 2024. A qualitative content analysis of YouTube videos on AS was performed using the Microsoft Edge web browser, without any prior login or search history.
Inclusion and Exclusion Criteria
Videos on AS presented in English were included in the study. Duplicate videos, irrelevant videos, videos in languages other than English and YouTube Shorts were excluded.
Sample Size
The sample size was the top 100 YouTube videos listed when searched for ‘Ankylosing spondylitis’.
YouTube Search
The keyword ‘Ankylosing spondylitis’ was searched on YouTube (
Data Analysis
Prior to video evaluation, all four rheumatologists (DM, DL, VB, AZ) underwent a calibration exercise to standardise the interpretation of the modified DISCERN (mDISCERN) and GQS tools. This process involved discussion of scoring criteria, review of sample videos and clarification of definitions for ‘useful’ and ‘misleading’ content to ensure consistency in assessment. Videos meeting the inclusion criteria were then independently and blindly evaluated by the four rheumatologists using the mDISCERN and GQS scores. Any discrepancies in scoring or classification were resolved through reassessment and consensus discussion. As individual reviewer scores were not retained as separate datasets, formal inter-rater reliability statistics such as Cohen’s or Fleiss’ kappa could not be calculated.
Data Collection
Data were extracted from each video, including the title, source, type of source, upload date, duration, number of views, number of likes, total subscribers and total comments. Additionally, days since upload, views per like and daily views were calculated.
The video sources were classified into seven categories, including academic institutions, professional organisations, rheumatologists, non-rheumatologist doctors, healthcare professionals (HCPs) other than physicians (such as dietitians, nurses and physical therapists), health information websites, alternative system professionals and independent users. The videos were also grouped according to the target audience, which included patients, HCPs and those unspecified.
Evaluation of Usefulness
Videos were classified as useful or misleading based on content accuracy. Videos containing scientifically accurate information regarding any aspect of AS were classified as useful, whereas videos containing at least one scientifically unproven or inaccurate claim were classified as misleading. This conservative classification strategy was adopted to reflect a patient-safety-oriented approach, as even a single misleading statement—particularly related to diagnosis or treatment—may influence patient understanding and health-related decisions.
Evaluation of Reliability and Quality
A modified five-point DISCERN tool, adapted from the original DISCERN tool, 9 was used to evaluate the reliability of the videos. 4 This tool consists of five questions, each answered with ‘yes’ or ‘no’, scored as 1 or 0 points, respectively (Supplementary Table S1), with higher scores representing greater reliability. Overall video quality was assessed using the five-point Global Quality Scale (GQS) (Supplementary Table S2), with higher scores indicating better video quality. 10 Videos were grouped into groups according to their mDISCERN score (good reliability, score >3; moderate reliability, score = 3; poor reliability, score <3). Videos were grouped into three groups according to their GQS score (high quality, score 4–5; intermediate quality, score = 3; low quality, score 1–2).
Ethical Approval
This article does not contain any studies with human or animal participants; informed consent from participants was not relevant to the study, and no ethical approval from a research ethics committee was necessary.
Statistical Analysis
Data were analysed using the Statistical Package for the Social Sciences (SPSS), version 29.0. Descriptive analysis was used to present the study outcomes. Continuous variables were described as mean and standard deviation (SD) or median (IQR = inter-quartile range), whereas categorical variables were described as numbers and percentages. The Kolmogorov-Smirnov test was used to assess the normality of the data. Non-normally distributed continuous variables were expressed as median (range). Pairwise comparisons between the ‘useful’ and ‘misleading’ videos were performed using the Mann-Whitney U test. The reliability and quality scores according to video scores were compared using the Kruskal-Wallis test, with pairwise comparisons evaluated using the Mann-Whitney U test. A P value of <.05 was considered statistically significant.
Results
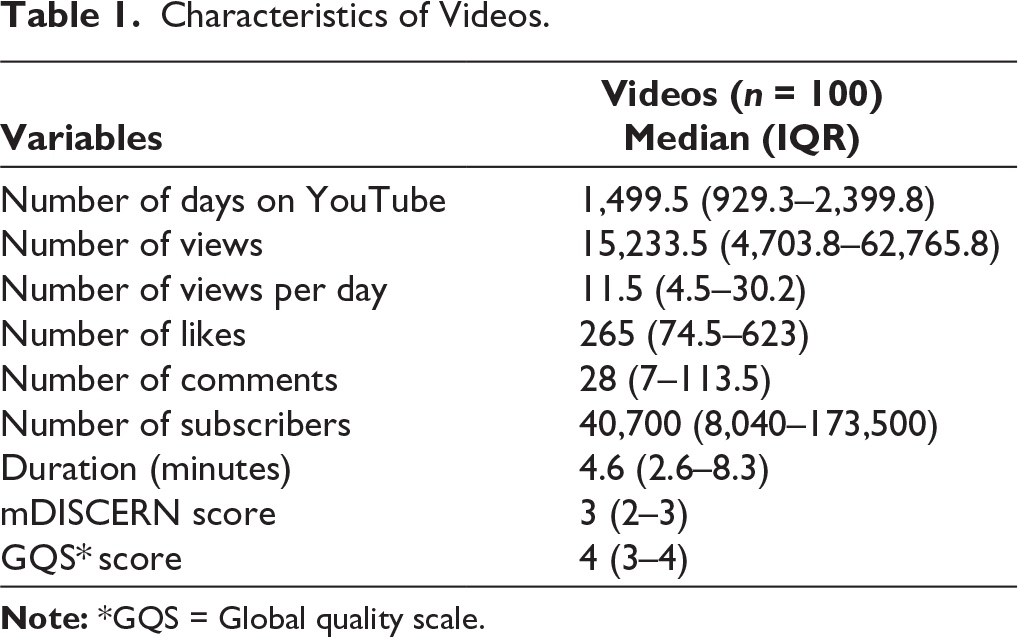
A total of 120 videos were screened, of which 12 duplicates and eight videos presented in languages other than English were excluded. Overall, 100 videos were included and analysed in the study. The median (range) number of views was 15,233.50 (4,703.75–62,765.75), with a median (range) number of daily views of 11.49 (4.48–30.24). The median (range) duration of the videos was 4.59 minutes (2.57–8.26) (Table 1).
Characteristics of Videos.
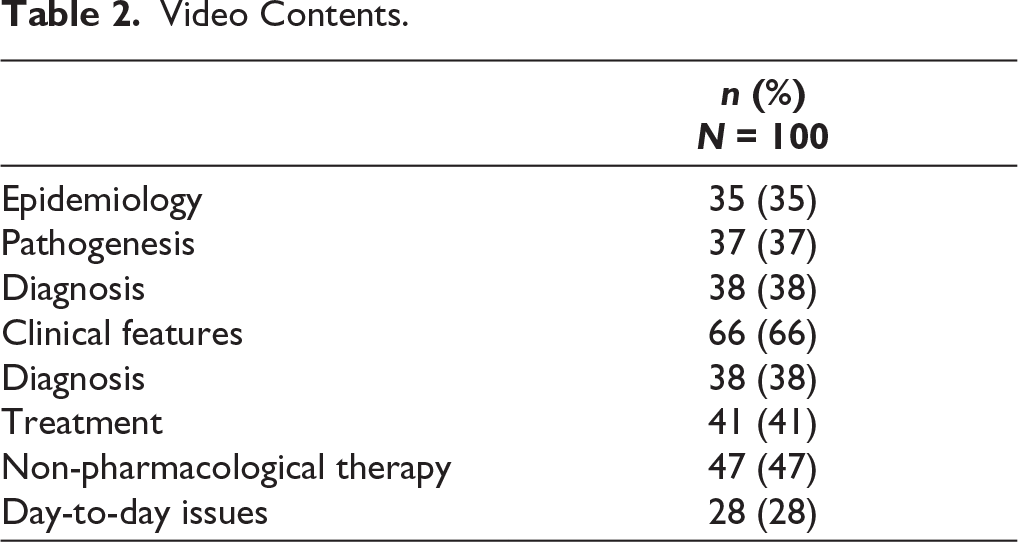
Among the analysed videos, 66.0% included information on clinical features, while 47.0% covered non-pharmacological therapy and 41.0% addressed pharmacological therapy. The epidemiology of AS was discussed in 35.0% of the videos and pathogenesis in 37.0%. Additionally, 38.0% of the videos addressed disease diagnosis, and 28.0% focused on day-to-day challenges (Table 2).
Video Contents.
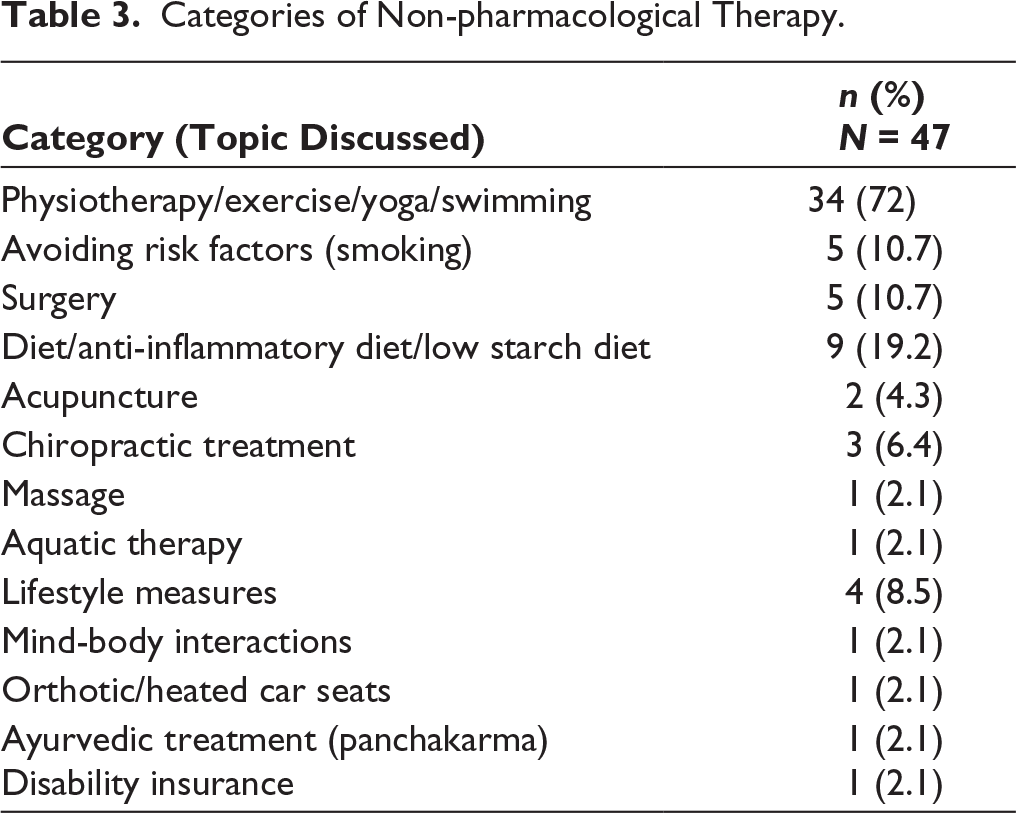
Among the videos discussing non-pharmacological treatment options, information related to physiotherapy/exercise/yoga/swimming was discussed in 72% of the videos, followed by 19.2% on diet, 10.7% on smoking and surgery and 8.5% on lifestyle measures (Table 3).
Categories of Non-pharmacological Therapy.
Of the analysed videos, 89% provided useful information, while 11% provided misleading information. Examples of misleading information included therapies which do not have any scientific evidence (Laser therapy); information unrelated to AS, such as Lyme disease, fungal infection (under the title AS); dietary claims with no proven scientific evidence (keto diet) and therapies with limited scientific data (Immunoglobulin therapy).
Misleading videos had a significantly longer median duration (7.0, range 5.3–12.3 minutes) compared to useful videos (4.4, range 2.3–8.2) (P = .040). Additionally, the median number of comments was significantly higher for misleading videos (161, range 53–306) than for useful videos (26.5, range 5.8–89.5) (P = .019) (Table 4).
Descriptive Statistics.

Comparisons between the ‘useful’ and ‘misleading’ videos were performed using the Mann-Whitney U test.
*GQS = Global quality scale, N/A = Not applicable, †HCPs = Healthcare professionals.
Values of P < .05 were accepted as significant and marked in bold and red.
Of 100 videos, 22% had high reliability (mDISCERN score >3), 40% had moderate reliability (mDISCERN score = 3), and 38% had poor reliability (mDISCERN score <3).
Of 100 videos, 60% had high quality (GQS 4–5), 27% had intermediate quality (GQS = 3), and 13% had low quality (GQS 1–2).
All the videos created by the academic institutions, professional organisations and rheumatologists were useful (100%). The majority of videos produced by health information websites (95.7%) and HCPs other than physicians (83.3%) were useful.
Target Audience and Video Source
In all the videos, the majority of the target audience consisted of patients (90%), followed by HCPs (9%), with 1% being unspecified. Most videos posted on YouTube were uploaded by independent users (26%), followed by academic institutions or professional organisations (23%) and health information websites (23%). The remaining videos were posted by rheumatologists (14%), HCPs other than physicians (6%), non-rheumatologist doctors (4%) and alternative system professionals (4%).
Reliability and Quality of Videos
The majority of videos posted by rheumatologists (42.9%), HCPs other than physicians (33.3%) and health information websites (30%) had a higher mDISCERN score (>3). In contrast, videos posted by independent users, alternative system professionals and non-rheumatologist doctors had significantly low mDISCERN score (< 3) (P = .006).
The quality of videos was high (GQS score = 4–5) for videos posted by rheumatologists (92.9%), HCPs other than physicians (83.3%), academic institutions and professional organisations (82.6%) and health information websites (65.2%). Video quality was intermediate to low (GQS score = 1–3) for videos posted by independent users, alternative system professionals and non-rheumatologist doctors (P < .001).
Discussion
The internet has been regarded as the third most trusted source of health information, ranking behind physicians and government healthcare institutions and is now considered more reliable than traditional mass media. 11 Research showed that 80% of internet users search for health information online. 1 Hay et al. reported that 62.5% of rheumatology patients used the internet to gather information about their condition before their first consultation with a rheumatologist. 12 YouTube, with its vast reach, free and easily accessible videos, has huge potential to provide reliable information to patients, but it lacks a quality control system to regulate the accuracy, content or reliability of the videos. Therefore, this study evaluated the content, reliability and quality of health information pertaining to AS on YouTube.
Overall, our study found the quality of English videos about AS presented to Indian viewers to be useful and of good quality and reliability. The proportion of useful videos (89%) was notably higher compared to prior research, which reported 51.4% useful videos for Sjogren’s syndrome 3 ; 54.9% for RA. 4
Despite this encouraging finding, the median number of views and daily view counts were significantly greater for misleading videos compared to useful ones. This concerning trend aligns with the observations made in two other studies by Onder ME et al. 6 and Garg et al. 13 These findings emphasise that, while the medical content on YouTube demonstrates substantial usefulness, viewer engagement—measured by metrics such as views—continues to favour misleading videos over accurate and reliable ones. It would also suggest that engagement metrics such as views and comments may be influenced by multiple factors unrelated to content accuracy, including presentation style and emotional appeal, limiting their interpretation as indicators of informational quality.
Although misleading videos demonstrated higher engagement metrics, including views and comments, these findings should be interpreted cautiously. The observed association does not imply causation or confirm algorithmic prioritisation by YouTube, as the platform’s recommendation mechanisms are proprietary and not directly accessible. Higher engagement with misleading content may reflect factors such as emotional appeal, simplified narratives or controversial messaging rather than informational accuracy or credibility. Therefore, these observations should be regarded as associative and hypothesis-generating rather than evidence of preferential algorithmic promotion of misleading medical content.
Videos created by rheumatologists were found to be significantly more useful, reliable and of higher quality. However, only 14% of the analysed videos were uploaded by rheumatologists, making them a minor contributor to the dissemination of awareness and information. This highlights the need for rheumatologists to play a more active role by creating and sharing more video content.
YouTube’s stated content creation strategy explains that: ‘Our algorithm doesn’t pay attention to videos, it pays attention to viewers. So, rather than trying to make videos that’ll make an algorithm happy, focus on making videos that make your viewers happy’. 14 However, this approach fails to address the importance of the usefulness, quality and reliability of the content. As a result, it suggests that content’s scientific accuracy alone does not influence the algorithm’s promotion of videos to viewers. To bridge this gap, rheumatologists should consider collaborating with content creation professionals to optimise their videos for greater engagement while maintaining scientific accuracy and relevance.
YouTube’s content recommendation strategy emphasises viewer engagement; however, the extent to which medical accuracy influences content visibility remains unclear. While recent algorithmic updates are reported to address misinformation, 15 it is not known whether non-evidence-based medical claims are consistently identified or deprioritised. Further platform-level research is required to better understand how health-related content is ranked and recommended.
Limitations
This study has several limitations. YouTube is a dynamic platform with continuously changing content, and search results are influenced by algorithmic and regional factors; therefore, the selection of the top 100 videos based on a single search term, default relevance filter and a single search date represents only a snapshot in time and may limit reproducibility and generalizability. The analysis was restricted to English-language videos, which may reduce applicability to non-English-speaking and rural populations in India, where regional language content is frequently accessed. Consequently, the findings may not fully reflect the overall quality and nature of AS-related information available to all population groups. The evaluation of video reliability and quality was performed by HCPs, and patient perceptions may differ from expert assessments. In addition, formal inter-rater reliability statistics could not be calculated, as individual reviewer scores were not retained separately, and final assessments were based on consensus among four rheumatologists. Finally, the binary classification of videos as misleading based on the presence of at least one unproven claim does not account for the clinical relevance or potential harm of individual inaccuracies and may overestimate the proportion of misleading content. To address language-related limitations, a complementary analysis of Hindi-language YouTube videos on AS has been conducted and is currently being finalised.
Conclusion
This study highlights YouTube’s potential as an important platform for accessing high-quality videos about AS, with nearly half of the reviewed content meeting high-quality standards. To improve patient engagement and broaden the dissemination of credible information, rheumatologists should actively contribute by creating and sharing more video content. Collaborations with social media experts can further help enhance the appeal and reach of these videos without compromising their scientific integrity. Moreover, it is essential for YouTube to integrate metrics for evaluating the accuracy and reliability of scientific content into its algorithm to promote trustworthy medical information.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors thank Dr Srivallabh Sane (Statistician), StandForAS Foundation, for statistical support.
Authors’ Contribution
All listed authors have met the following criteria: (a) Made a significant contribution to the concept, design, acquisition, analysis or interpretation of data. (b) Approved the final version of the article for publication. (c) Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity. (d) Drafted the article or revised it critically for important intellectual content.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This article does not contain any studies with human or animal participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by StandForAS Foundation.
Patient Consent
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.